
Abstract
This study aimed to explore the adoption of person-generated health data in clinical settings and discern the factors influencing clinicians’ willingness to use it. A web-based survey containing 48 questions was developed based on prior research and the Unified Theory of Acceptance and Use of Technology 2 model. The survey was administered to a convenience sample of 486 nurses and physicians in South Korea recruited through an online community and snowball sampling. Of these, 70.7% were physicians. While 65% had used mobile health apps and devices, only 12.8% were familiar with person-generated health data. Still, a promising 73.3% expressed interest in incorporating person-generated health data into patient care, particularly data on blood glucose and vital signs. The findings of the study also indicated that clinicians specializing in internal medicine (OR: 1.9, CI: 1.16–3.19), familiar with person-generated health data (OR: 2.6, CI: 1.58–4.29), with a positive view of information and communication technology adoption (OR: 2.6, CI: 1.65–4.13), and who see the value in person-generated health data (OR: 3.9, CI: 2.55–6.09) showed higher inclination to utilize it. However, those in outpatient settings (OR: 0.4, CI: 0.19–0.73) showed less enthusiasm. The findings of this study suggest that despite the willingness of clinicians to use person-generated health data, various barriers must be addressed first, including a lack of knowledge regarding its use, concerns about data reliability and quality, and a lack of provider incentives. Overcoming these challenges demands concerted organizational or policy support. This research underscores person-generated health data's untapped potential in healthcare and the pressing need for strategies that facilitate its clinical integration.
Keywords
Introduction
The adoption of mobile apps and wearable devices with sensor technologies has rapidly increased in the healthcare field.1,2 Health apps provide patients with a streamlined means of collecting their health data outside the clinical environment and enable the collection of large amounts of person-generated health data (PGHD) through the activities of daily living.3,4 As reported by Research2Guidance, more than 259,000 mobile health apps are available in online app stores. 5
PGHD, as defined by the Office of the National Coordinator for Health Information Technology (ONC), is produced and documented by patients or their families outside the clinical setting to assist in managing their health issues. 6 The proliferation of PGHD has enabled clinicians to understand patients’ health status outside the hospital better and improve the continuity of care. 7 Findings from numerous studies have demonstrated that improved patient outcomes can be achieved with the use of PGHD. For example, patients with chronic illnesses, including diabetes and stroke, and patients requiring rehabilitation were able to manage their health effectively with the help of PGHD.8–10 In addition, the patient–provider relationship was enhanced by using PGHD, which was regarded as an effective tool for communication.11–13
Despite the benefits of incorporating PGHD in patient care, various issues regarding the use of PGHD, including data reliability, data interoperability, and clinical workflow integration, have hindered the broad adoption of PGHD in clinical settings.14–16 Understanding the healthcare providers’ perceptions and expectations regarding the use of PGHD in the patient care setting is crucial to addressing the various challenges associated with the use of PGHD. Previous studies examining healthcare providers’ experiences with using PGHD in patient care reported that multiple issues need to be resolved to facilitate the clinical use of PGHD.17–21 An association of healthcare providers’ attitudes toward and experience with the use of PGHD with the actual use of PGHD in patient care was also reported.17,18
Previous research indicates that the successful integration of PGHD in clinical settings hinges on clinicians harboring positive expectations. These expectations encompass enhancements to clinical care, improved patient outcomes, and a more streamlined utilization of PGHD in clinical processes. 22 The preconditions for embracing PGHD align with the Unified Theory of Acceptance and Use of Technology 2 (UTAUT2), which delves into crucial factors influencing the acceptance and use of technology. A few examples of these factors are effort expectancy (ease of use) and performance expectancy (the perceived contribution of technology to job performance). 23
Globally, there is a growing trend towards systematically managing PGHD to facilitate its effective utilization in clinical practice and health promotion efforts. Notably, Accenture and the ONC in the United States have jointly published a white paper offering comprehensive guidelines for leveraging PGHD in both healthcare practice and research. 24 Finland's MyKanta is a prime example of a national health data platform that incorporates Personal Health Records (PHRs) housing individuals’ health and welfare data, including data generated by individuals to gauge their well-being. 25 The “My Healthway” initiative, which was recently launched by the Korean government, was established in part to facilitate the use of various types of health data, including PGHD and environmental, clinical, and genomic data, in order to reach the most appropriate decisions regarding prevention and treatment of disease for an individual.26–28 The pivotal elements of the My Healthway initiative involve the identification and standardization of a core data set for PHRs, the development of a secure and robust data infrastructure, the facilitation of health data utilization by patients through the My Healthway app and connected health services, and the refinement of data governance policies and structures. 29
However, few studies have been reported examining the views of clinicians in South Korea regarding the use of PGHD in patient care. Therefore, this study conducted a survey of nurses and physicians in South Korea to assess their experience and expectations regarding using PGHD in patient care. Specifically, this study aimed to understand (1) the current use of PGHD in clinical practice, (2) the attitudes of registered nurses and physicians toward the use of PGHD in patient care, and (3) the factors affecting the willingness to use PGHD in patient care.
Methods
Study design
In order to examine clinicians’ experiences and views on the clinical use of PGHD and identify the factors influencing their intention to use PGHD in patient care, the authors formulated a questionnaire by adapting questions from previous surveys and grounding them in the UTAUT2 model.19,20,22,23,28,30 The survey questionnaire was designed to investigate various dimensions, including participants’ performance expectancy, effort expectancy, facilitating conditions, experience, behavioral intention of using PGHD in clinical care, and demographic details. The final questionnaire comprised 48 questions: eight items focusing on demographics, five items gauging perspectives on information and communication technology (ICT) (performance expectancy), five items assessing experience with the use of wearable devices and mobile health apps (experience), nine items on the experience with the use of PGHD for patient care (experience), 12 items gauging the perceived usefulness of PGHD (performance expectancy), and nine items addressing challenges in use of PGHD that need attention (effort expectancy and facilitating conditions). The survey underwent testing with ten clinicians to ensure clarity and logical flow. The survey was implemented through a Health Insurance Portability and Accountability Act-compliant online survey platform. 31
Data collection
Survey participants were recruited through a South Korean online community for clinicians. 32 In addition, recruitment emails were sent to the clinicians at the institutions affiliated with the authors. Only those without difficulties reading and writing Korean and with more than one year of direct patient care experience were invited to participate in the survey. Given that there were ∼ 1.2 million registered nurses and physicians in South Korea, 385 participants were required with a confidence level of 95% and a 5% margin of error in response. Considering the dropout rate of ∼ 30%, our target enrollment was 500 participants. The survey was conducted between 1 and 7 July 2022. All participants electronically submitted their consent through a digital informed consent form integrated with the survey. After excluding incomplete or unreliable responses, 486 responses were included in the analysis. The participants received coffee vouchers valued at $4 for completing the survey.
Statistical analysis
Data analysis was performed using R 4.1.2. 33 The responses were analyzed using descriptive statistics to assess patterns and trends. Using the Mann-Whitney U-test, the responses in the 5-point Likert scale were compared according to the participants’ characteristics. To determine the factors affecting clinicians’ willingness to use PGHD in patient care, the responses on the 5-point Likert scale were dichotomized into willing (strongly willing to and willing to) and unwilling (strongly unwilling to, unwilling to, and neutral); logistic regression models were then developed for prediction of the dichotomized willingness to utilize PGHD in patient care. The predictors used in the model included the participants’ demographics, clinical practice setting, experience with the use of PGHD and mobile health technologies, and attitude toward using ICT in the healthcare field.
Ethical consideration
This study was approved by the Institutional Review Board (IRB) of Seoul National University (IRB No. 2206/004-011).
Results
Participant characteristics
The majority of the 486 participants were physicians (N = 344, 70.7%). More than half of the participants were males (N = 258, 53.1%), and aged between 30 and 39 (N = 268, 55.1%). Almost half of the participating physicians were from clinics or small hospitals with less than 100 beds (165, 48%) and working in an outpatient setting (N = 275, 79.9%). By contrast, most nurses (N = 103, 72.5%) were from a large hospital with more than 800 beds and working in an inpatient setting (N = 84, 59.2%). Internal medicine was the most commonly reported specialty for both physicians (N = 139, 40.4%) and nurses (N = 58, 40.8%). A summary of the participants’ characteristics is shown in Table 1.
Characteristics of the participants.

ICU: intensive care unit; ER: emergency room; OR: operation room.
Multiple responses were allowed; thus, the sum of column % exceeds 100.
Participants’ attitudes towards the use of ICT in patient care
Participants expressed highly positive attitudes towards the adoption of ICT in patient care. While the overall rating remained high, their responses regarding the role of ICT in enhancing patient–provider relationships were relatively reserved (Figure 1).

Clinicians’ perspectives regarding the adoption of information and communication technology (ICT) in healthcare.
Experience with mobile health devices, apps, and PGHD
Results regarding the participants’ familiarity with mobile health devices, apps, and PGHD are shown in Table 2. Among 486 participants, 316 responded that they were current or previous users of wearable devices and mobile health apps. However, regarding PGHD, a considerable majority of the participants answered that they had never heard of it (N = 206, 42.4%) or that they had heard of it but never used it for patient care (N = 218, 44.9%). Only a small fraction of participants (N = 62, 12.8%) were current (N = 44, 9.1%) or previous (N = 18, 3.7%) users of PGHD. The reasons given by respondents who had heard of PGHD but never used it (N = 218) and those who had used PGHD before but were not currently using it in patient care (N = 18) are shown in Figure 2. The most common reason was a lack of organizational support. Patients’ lack of familiarity with mobile health devices, data reliability issues, clinicians’ lack of knowledge regarding the utilization of PGHD, and the burden of data processing were also highly ranked reasons. The responses showed no significant variations between nurses and physicians (Supplemental Figure A).

The reasons for not using person-generated health data (PGHD) in patient care.
Experience using mobile health devices, apps, and person-generated health data (PGHD).

Multiple responses were allowed; thus, the sum of the column % exceeds 100.
Current or previous PGHD users utilized it primarily to check patients’ status at home (N = 34, 54.8%) and to encourage patient engagement in the treatment process (N = 29, 46.8%). The most common method of accessing PGHD was through the patient's smartphone app (N = 31, 50%), followed by electronic health records (EHRs) (N = 26, 41.9%). The most common response to the ideal period requiring PGHD review was the entire period between hospital visits (N = 48, 77.4%).
Perceived usefulness of PGHD according to data types
Twelve types of data that can be obtained as PGHD were presented and participants were asked to indicate their usefulness in patient care. The 12 data types include physical activity, eating habits, sleep patterns, stress and mood status, alcohol or recreational drug use, smoking, vital signs, blood glucose, body weight, skin condition with a picture, menstrual cycle, and medication adherence. The responses took a 5-point Likert scale (1 = not useful at all, 2 = slightly useful, 3 = moderately useful, 4 = very useful, 5 = extremely useful).
The average ratings for usefulness are shown in Figure 3. Detailed frequency distributions are provided in Supplemental Table B. Nurses tended to rate the usefulness of the presented PGHD types higher than physicians, except for physical activity, smoking, and eating habits. Blood glucose and vital signs received the highest rating from both physicians and nurses. However, both of them rated alcohol or drug use, smoking, and eating habits relatively low. Skin condition and stress/mood state also received a low rating, particularly by the physicians. Statistically significant differences in the average usefulness scores for vital signs, blood glucose, and skin/wound pictures were observed between nurses and physicians when tested using the Mann-Whitney U-test.

Perceived usefulness of different types of person-generated health data (PGHD).
The intention to use PGHD in patient care
The majority of the participants (N = 356, 73.3%) responded that they were likely (N = 249, 51.2%) or highly likely (N = 107, 22%) to use PGHD in patient care in the future. Approximately 21% (N = 102) responded with a neutral stance, and the remaining 28 (5.7%) were unwilling. The reasons for reluctance to use PGHD in patient care are shown in Figure 4. The most common reasons for the unwillingness were not knowing how to use PGHD in patient care (N = 9, 32.1%), concerns regarding data reliability (N = 8, 28.6%), and lack of provider incentives for using PGHD (N = 8, 28.6%).

The reasons for unwillingness to use person-generated health data (PGHD) in patient care (multiple responses allowed).
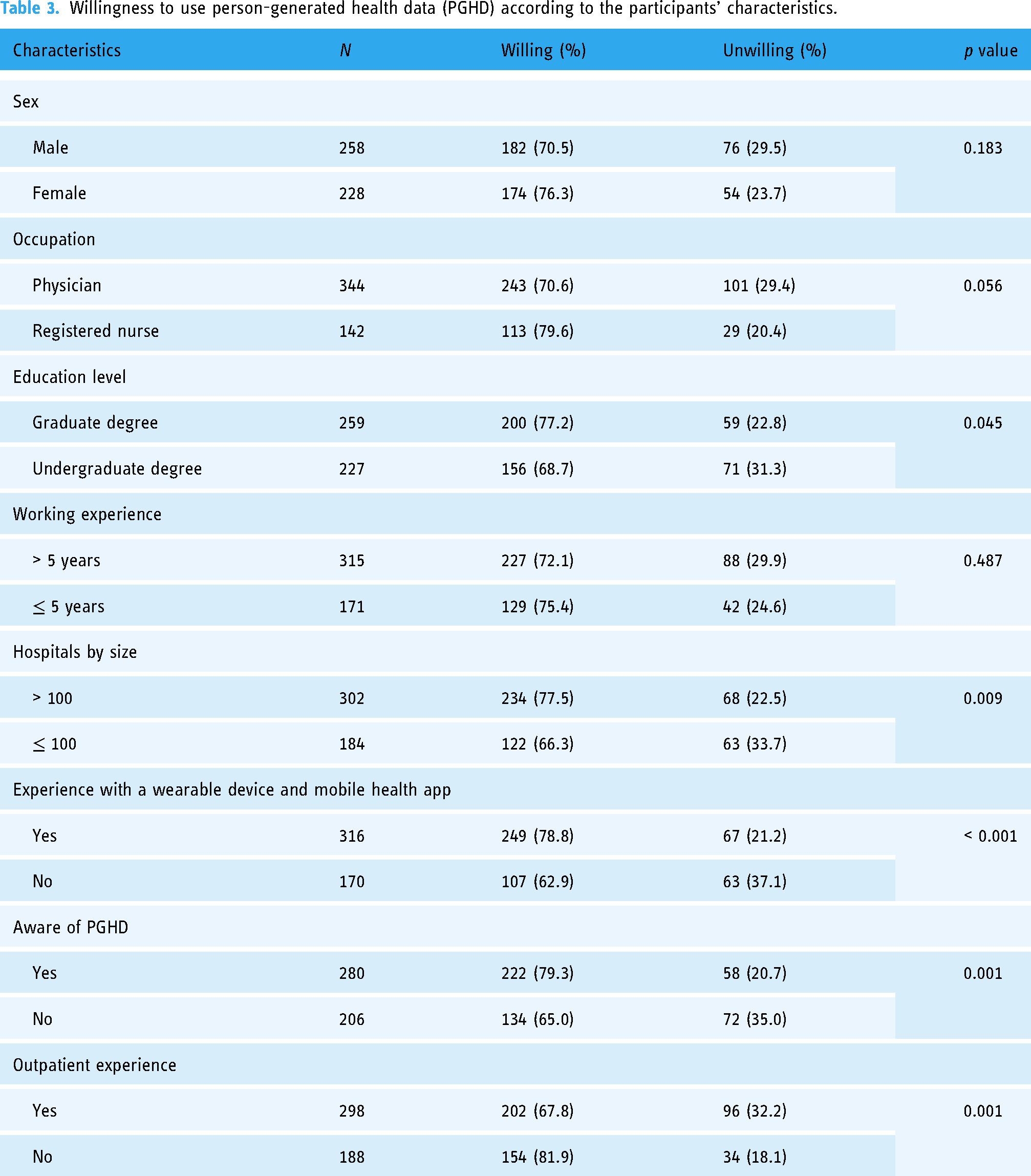
The intention toward the use of PGHD was dichotomized by combining neutral, somewhat unlikely, and highly unlikely responses as unwilling to use PGHD, and likely and highly likely responses as willing to use PGHD. A comparison of the dichotomized intention for the use of PGHD was performed according to participants’ characteristics using the proportion test (Table 3). Participants with graduate-level education, a smaller institution, experience using wearable devices or apps, awareness of PGHD, and who did not have experience working in outpatient settings showed a significantly higher level of willingness to use PGHD in patient care settings.
Willingness to use person-generated health data (PGHD) according to the participants’ characteristics.
The factors affecting the willingness to use PGHD in patient care
A logistic regression model was constructed to examine the factors affecting clinicians’ willingness to use PGHD in patient care settings. Figure 5 illustrates both adjusted and unadjusted odds ratios (OR). In a univariate logistic regression model, all factors, except for age (OR: 1.31, 95% CI: 0.85–2.00), gender (OR: 1.35, 95% CI: 0.90–2.03), and specialization in internal medicine (OR: 1.44, 95% CI: 0.95–2.02), demonstrated statistical significance. Notably, being a physician (OR: 0.62, 95% CI: 0.38–0.98), working in outpatient settings (OR: 0.46, 95% CI: 0.29–0.72), and being employed in smaller hospitals (OR: 0.57, 95% CI: 0.38–0.86) emerged as prominent risk factors associated with a willingness to use PGHD in patient care.

Factors affecting the willingness to use person-generated health data (PGHD) for patient care.
However, in a multivariate model, the effects of hospital size and education level no longer held significance. Instead, the specialization in internal medicine (OR: 1.9, 95% CI: 1.16–3.19) became a significant facilitator, along with factors such as awareness of PGHD (OR: 2.6, 95% CI: 1.58–4.29), experience with wearable devices and apps (OR: 1.9, 95% CI: 1.15–3.11), positive attitudes toward ICT in healthcare settings (OR: 2.6, 95% CI: 1.65–4.13), and the perception of PGHD as useful (OR: 3.9, 95% CI: 2.55–6.09). Furthermore, working in outpatient settings (OR: 0.4, 95% CI: 0.19–0.73) remained a significant risk factor in the multivariate model, while age and gender continued to be statistically insignificant. Multivariate logistic regression models constructed separately for nurses and physicians were presented in Supplemental Figure C. The specialty of internal medicine, experience with wearable devices and apps, and positive views on using ICT in healthcare did not significantly influence nurses’ willingness to utilize PGHD in patient care.
The barriers to using PGHD in patient care
The participants indicated the importance of resolving the known barriers associated with PGHD in order to be able to utilize PGHD in patient care. The participants were presented with five well-known barriers reported in previous studies12,20,21,34 and asked to indicate their significance using a 5-point Likert scale. According to the participants’ responses, improving the overall accuracy and reliability of PGHD data was the most important, followed by data quality assurance with effective data cleaning and workflow support through EHR integration. Improving the efficiency of data use, such as extracting only useful information and data visualization, was also considered important (Figure 6). The responses aggregated separately for nurses and physicians were provided in Supplemental Figure D.

The barriers to overcome in order to facilitate the use of person-generated health data (PGHD) in patient care.
The participants were asked to freely submit comments regarding the use of PGHD at the end of the survey. Eighty participants provided additional opinions on the use of PGHD, mainly re-emphasizing the importance of addressing issues related to integrating PGHD with clinical workflow and a healthcare service model (N = 40) and data quality (N = 28). Other notable comments included concerns regarding data privacy and the digital divide, the importance of user training, gathering evidence regarding the effects of using PGHD, and improving data interoperability.
Discussion
This study analyzed the experiences and perspectives of clinicians in South Korea regarding the use of PGHD in patient care, using a convenience sample. We further investigated the factors influencing their intention to employ PGHD in patient care, drawing on the UTAUT2 model. Although not all aspects of the UTAUT2 model were reflected in the survey questionnaire, it provided a useful framework for interpreting the survey results. While the research was centered in South Korea, its findings provide meaningful insights applicable to similar endeavors in other countries aiming to incorporate PGHD into clinical care.
The majority of the participants (N = 356, 73.3%) expressed a willingness to use PGHD in patient care. Although nurses (79.6%) showed a higher degree of willingness than physicians (70.6%), the difference was not statistically significant.
Both physicians and nurses who participated in the survey perceived blood glucose, vital signs, and body weight, which are measured objectively using a device, as very useful in clinical practice, whereas they considered wound pictures, mental health status, and alcohol or drug use, which are dependent on patient's self-report, less useful. As reported in previous studies, self-reported data were regarded as less useful by the participants in this study due to reliability concerns.30,35,36 Of note, the perceived usefulness of wound pictures was significantly lower for physicians than nurses, possibly due to their different roles and interests in assessing skin conditions within close proximity to patients. 30 For example, nurses routinely assess patients’ skin conditions to prevent pressure injuries or evaluate wound status. These findings are consistent with those reported in previous studies, which suggested that perceptions regarding the usefulness of different types of PGHD could be influenced by their relevance to a particular clinical field. 19
According to the results of logistic regression, clinical setting, specialty, and personal experience with mHealth devices, apps, and PGHD were factors significantly affecting the participants’ willingness to use PGHD. Participants’ positive perspectives on the adoption of ICT in healthcare and the clinical usefulness of PGHD were also significant predictors of their willingness to use PGHD in patient care. The findings of this study also indicated that experience using PGHD and wearable health technologies could have a positive impact on the intention to adopt PGHD in patient care. This finding agrees with those of previous studies on the acceptance of health ICT, which reported that the digital readiness of clinicians had an impact on their acceptance of new medical technologies.28,37–41 Also, this result confirms that positive experience and performance expectancy of technology affect users’ intention to adopt PGHD. 23
Of note, experience working in an outpatient setting was identified as a significant risk factor for the intention to use PGHD in clinical practice. According to the results of the additional analysis provided in Supplemental Tables and Figures E, participants with outpatient experience had more experience with the use of PGHD than their counterparts. They also showed a slightly lower rating on their perspectives regarding the adoption of ICT in healthcare settings and the clinical usefulness of PGHD than their counterparts. These findings suggest that practitioners’ negative experiences with PGHD may directly impact their resistance to incorporating it into clinical practice. Moreover, the utility of PGHD for patient care might be perceived as less compelling, particularly in outpatient settings where patients typically present with less acute conditions. Consequently, the immediate necessity to integrate PGHD into these clinical practices may not be readily apparent. This situation could be interpreted as having a comparatively diminished performance expectancy regarding PGHD.
While the clinicians who participated in this study expressed a high level of willingness to utilize PGHD in patient care, they also asked for the resolution of various issues hindering the use of PGHD. As reported in previous studies, the participants in this study identified data reliability as a very significant issue. 40 An efficient method for processing noisy data is vital to extract valuable insights. Equally crucial is the integration of PGHD into clinical workflows, accompanied by suitable incentives for the additional effort required in reviewing PGHD. The most common barriers to using PGHD in patient care are concerns about data quality and a lack of understanding of its application. This study underscores the need to address these data quality challenges and to develop effective techniques for extracting meaningful information from PGHD, paving the way for its wider adoption in clinical practice. These issues should be considered critical facilitating conditions for the clinical adoption of PGHD.
The responses from the participants provided a consistent indication that systematic efforts at the organization or policy level, such as the development of a data processing pipeline for PGHD, including PGHD in routine clinical workflow, providing incentives for incorporating PGHD in patient care and offering opportunities for training on the use of PGHD to clinicians, are required in order to facilitate the use of PGHD. In addition, gathering evidence of the impact of PGHD on patient outcomes is crucial in the effort to encourage clinicians to incorporate it into patient care.
This study has several limitations. First, the use of convenience samples recruited through closed online communities and snowball sampling may limit the generalizability of the findings. Second, recall bias may have influenced the results, a common issue in survey studies. Third, many of the participating clinicians had overlapping and varied clinical specialties and settings. Thus, interpretations of the effects of clinical experience on clinicians’ attitudes toward using PGHD were not fully explored in this study. Fourth, 90% of the participants were relatively young, aged less than 50. Thus, the results did not adequately reflect the perspectives of more experienced clinicians on using PGHD in patient care.
Conclusion
Although numerous studies have highlighted the benefits of incorporating PGHD in the patient care setting, its adoption remains slow, as evidenced by the fact that only 9.1% of the participants in this study had experience with using PGHD in a clinical setting. However, the majority (73%) of the clinicians who participated in the study expressed their willingness to use PGHD in patient care despite identifying various challenges, including data reliability, workflow disruption, lack of incentive models, and inadequate training on the use of PGHD, which have also been reported in previous studies conducted in other countries. Organizational or policy-level support is essential to facilitating the use of PGHD in patient care by streamlining the data handling process in clinical settings and providing clinicians with the necessary incentives and training to use PGHD effectively.
Supplemental Material
sj-png-1-dhj-10.1177_20552076231218133 - Supplemental material for Attitudes and perspectives of nurses and physicians in South Korea towards the clinical use of person-generated health data
Supplemental material, sj-png-1-dhj-10.1177_20552076231218133 for Attitudes and perspectives of nurses and physicians in South Korea towards the clinical use of person-generated health data by Hyeoneui Kim, Boseul Cho, Jinsun Jung and Jinsol Kim in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231218133 - Supplemental material for Attitudes and perspectives of nurses and physicians in South Korea towards the clinical use of person-generated health data
Supplemental material, sj-docx-2-dhj-10.1177_20552076231218133 for Attitudes and perspectives of nurses and physicians in South Korea towards the clinical use of person-generated health data by Hyeoneui Kim, Boseul Cho, Jinsun Jung and Jinsol Kim in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors express their sincere appreciation to all people who contributed directly or indirectly at every stage of this study.
Contributorship
HK conceived the research idea, analyzed the data, wrote the manuscript, and supervised the study. BC designed the survey, analyzed the data, and wrote the manuscript. JJ analyzed the data and conducted a literature review. JK designed the survey and edited the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable; no human subjects involvement.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by a grant from the National Research Foundation of Korea (grant number: 2022R1A2C201136011) and the BK21 four project (Center for Human-Caring Nurse Leaders for the Future) funded by the Ministry of Education and National Research Foundation of Korea.
Guarantor
Hyeoneui Kim.
Supplemental material
Supplementary material for this article is available online. The survey questionnaire, along with the de-identified survey data, is accessible upon submission of a reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.