
Abstract
This paper builds on thematic findings from a larger study that explored how digital technologies (e.g. smartphones, apps, search engines) shape expectant and new mothers’ early parenting practices. An overarching theme that arose across these mothers’ experiences which deserved deeper exploration was relational digital surveillance. In the context of this paper, relational digital surveillance describes how mothers evaluate their sense of preparedness, goodness or suitability for motherhood as they transition into parenting in relation to: their own use of digital technologies when caring for their pregnant bodies (self-surveillance), partners’ and family members’ commentary and/or judgement regarding their use of digital technologies to support their parenting and decision-making (familial surveillance) in addition to service/health care providers’ commentary and/or judgement concerning their technology use (systemic surveillance). Mothers’ use of digital technologies in this study not only provided others (partners, family members, health care providers) with means to watch over their actions and bodies as they transitioned into motherhood but offered a new evaluative dimension for others to scrutinize their behaviour as a new mother. Such understandings of relational digital surveillance within the transition to parenting context raise critical questions concerning the promotion and commercialization of digital self-surveillance technologies among expectant/new parents given the ways these technologies can further push the boundaries of hegemonic mothering practices and contribute to feelings of inadequacy and self-doubt. Alternatively, these insights offer avenues where health care providers can intervene to facilitate activities that enhance digital health literacy skills and mitigate parents’ exposure to platforms that amplify anxieties.
Keywords
Introduction
Mothers are charged with the societal expectation that they will make the most ‘responsible’ decisions for themselves, and their families based on health information they encounter and increasingly this information is offered in digitized formats. A co-parent or family member may take an interest in the decisions being made during the transition to parenting; however, primarily it is mothers who are expected to retrieve, understand and act upon increasingly sophisticated information about health issues and health care.1,2 In digital spaces, this undertaking for mothers takes place within a landscape of intensifying surveillance of the self and others. 3
Surveillance is an established practice within public health, and in recent years, there has been an upsurge in digital surveillance technology development designed to support health promotion practices, such as recording and tracking prenatal vitamin intake.4,6 The study of surveillance is most notably tied to Jeremy Bentham and Michel Foucault's writings on the Panopticon. 7 Briefly, the Panopticon describes a structure in which a single individual or entity monitors an individual or groups of people simultaneously without them knowing whether they are or are not being directly monitored at any given moment. A classic example of the Panopticon in practice is a prison with a single guard tower equipped with mirrored glass situated within a ring of prison cells; those incarcerated behind bars will never know if they are or are not being observed by the guards in the tower, which gives the structure its power to passively control the behaviours of incarcerated people. Although there is agreement among some scholars that the Panopticon is no longer a useful metaphor to understand contemporary forms of surveillance in our digital age, others suggest that the Panopticon is perhaps even more relevant now given the pervasiveness of modern surveillance technologies (e.g. social media platforms) and their ability to shape how individuals self-govern and exercise power over themselves (e.g. behave according to social media feedback of likes or dislikes from others) without any coercion required.7,8
As such, bodies under contemporary forms of capitalism can be understood to be self-governed according to the logic of individual responsibility and risk calculation; in other words, individuals must rely on their own self-management strategies to mitigate social and health risks, rather than relying on state or institutional bodies. 9 In particular, the pregnant body falls under an intense network of increasingly digitalized self-management strategies given that it is solely responsible for nurturing a foetus and its potentiality as a healthy and productive future citizen. Thus, during the transition to parenting, women are subjected to normative pressures to mitigate their own and their developing foetus’ health risk by constantly engaging in self-surveillance activities using digital technologies regardless of their socio-economic situation.9,12
This paper reports findings from a larger study exploring the ways digital technologies contribute to the experience of the transition to parenting; particularly, the role these technologies played in organizing and structuring emerging pregnancy and early parenting practices. Within that larger study, surveillance was identified as a pervasive element of the experience of transitioning to parenting within a digital context. As such, this manuscript contributes to the literature on digital media and motherhood by highlighting the potential for harm and further disenfranchisement among mothers who experience oppression (e.g. housing precarity, limited education), and who may not have the financial means, privacy or personal safety to utilize digital technologies in ways that support their well-being during the transition to parenting.
Methods
A qualitative descriptive study by the research team 13 was conducted to understand new parents’ experiences with and uses of digital technology across four stages – prenatal, pregnancy, labour and postpartum – of their transition to becoming a new parent. Qualitative description research studies are appropriate for understanding a phenomenon, process or the perspectives of participants where time and resources are limited, and information is needed directly from those experiencing the phenomenon under investigation. 14 As a methodology, this approach represents the characteristics of qualitative research and has gained traction within nursing research 14 – a discipline in which the majority of this study's research team members have significant expertise. Regarding methods, semi-structured in-depth interviews and focus groups are appropriate for qualitative descriptive studies as they allow researchers to explore concerns with participants through encouraging means that consequently facilitates the emergence of new concerns related to the phenomenon or process in question. 14 Within this study interested persons were eligible to participate if they met the following inclusion criteria: (1) became a parent within the last 24 months, (2) were between the ages of 16 and 35 years old, and (3) identified as a fluent English speaker; technology use was not part of the study's inclusion criteria.
Participant recruitment
This study took place during winter 2019 in an urban setting in Southwestern Ontario, Canada, and used a purposive convenience sampling strategy commensurate with a qualitative descriptive methodology to recruit participants who met the study's inclusion criteria. Print flyers were circulated in spaces that parents tended to frequent with their young children in the community which included local public health units, daycare centers, family health clinics and early year play centers. Digital flyers were circulated within buy-and-sell websites and social media platforms such as Facebook. These flyers used inclusive language to welcome individuals of any gender given that not all people who become pregnant or a partner of someone who becomes pregnant fit the categories of ‘woman’/ ‘mother’ or ‘man’/ ‘father’. Each participant provided written informed consent prior to participating in a focus group and/or interview and was compensated for their time with a CAD $15 honorarium.
Data collection and analysis
Data collection and thematic analysis occurred concurrently through in-person focus groups and individual follow-up interviews at locations that were mutually agreed upon between the participants and researchers. Small focus group sessions, with 2–3 participants in each, were held to ensure participants would be engaged and participate to the best of their ability. 15 In addition to maximizing engagement, a small focus group size proved easier to coordinate with this demographic given their caregiving demands; to facilitate involvement in the focus groups, participants’ infants and children were welcomed. Similar methodological approaches have been used when conducting research among parents of young infants to mitigate barriers to participation and make the research environment as comfortable and inclusive as possible. 16 Overall, the locations for the focus groups included public libraries, a shelter and a children's center as some participants did opt to bring their children along and preferred a child-friendly setting. The focus groups were moderated by members of the research team. At the time of data collection, all but one member of the research team identified as a parent with child/ren ranging in age from 7 to 30 years of age. As such, the research team members had diverse levels of parenting experience and engagement with digital technology within the context of parenting which offered dynamic avenues to probe participants when moderating the focus groups to delve deeper into their accounts and experiences.
Researchers followed a semi-structured interview guide throughout the focus groups and follow-up interviews to facilitate conversation between participants. The nature of inquiry within the focus groups related to participants’ use of digital technologies within the context of the transition to parenting (i.e. social media, use of pregnancy/parenting apps, participation in online pregnancy/parenting support groups). If a focus group participant spoke of a topic that required additional time or consideration to explore, the researchers moderating the focus group offered them an individual follow-up interview; such topics for individual interviews included in vitro fertilization and egg donation. All the focus groups and interviews were digitally recorded and transcribed verbatim.
An iterative, inductive thematic analysis approach 14 was used to co-construct findings; all members of the research team analyzed each interview transcript before cross-comparing insights with one another to negotiate emerging themes within subsequent in-person team meetings. Codes were tracked in a tabular matrix using exemplar quotes from interview transcripts to demonstrate the meaning of the code. 14 Throughout data collection and analysis, reflexive dialogue amongst the research team offered space to question how reflections of positionality, power and social locations shaped each research team member's tacit assumptions about digital technology and parenting.
Recruitment of focus group participants continued until data saturation was met through participant discussions and team analysis when no new themes, patterns or codes emerged and categories became repetitive in nature.14,17 Trustworthiness of the data was optimized through measures of credibility (verbatim transcription and multidisciplinary analysis), transferability (descriptive details included to facilitate readers decisions about transferability of findings), conformability (researchers use of an audit trail and reflexivity throughout the analysis process) and dependability (detailed description of the methodological process).16,17
Findings
Descriptive findings
A total of 10 focus groups consisting of 2–5 participants in each (as well as their infants) and three individual follow-up interviews were completed with 26 participants. Although recruitment efforts targeted parents of all genders and sexual orientations, all participants who contributed to this study identified as cis-gendered, heterosexual women between the ages of 17 and 35 years old. There was a range of formal educational attainment; seven women with some secondary school education, one woman who had completed high school, one who had completed community college or apprenticeship, ten who had completed a university undergraduate degree and two who had completed a graduate degree (see Figure 1).
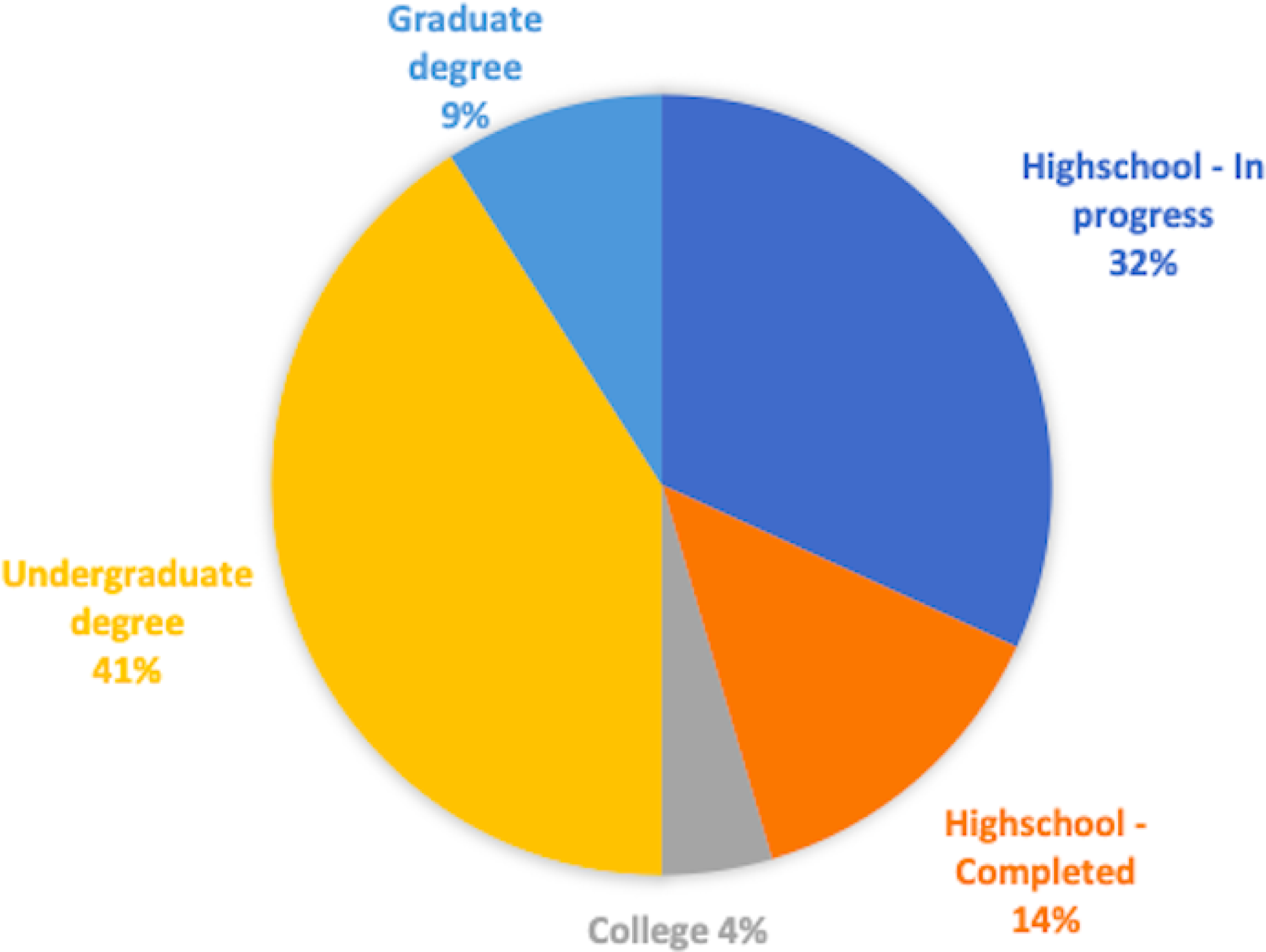
Participants educational attainment.
Twenty women reported their employment status, of which nine women were unemployed, three were employed part-time and seven were employed full time. Their household income also varied: four reported a yearly household income of less than $20,000, three reported between $20,000 and $50,000, four reported between $50,000 and $99,999 and five reported household income over $100,000 per year (see Table 1). Half of the women (N = 13) were married, seven were single and had never been married and one reported being separated from her partner. Three women identified as racialized, five did not disclose, and most (N = 18) identified as white.
Participants gender, age and household income.

Thematic findings
There was no aspect of the transition to parenting where discussions of surveillance had not shaped these participants’ sense of preparedness, goodness or being suitable for motherhood. Universally, participants expressed a near-compulsive need to simultaneously utilize and restrict their use of digital technologies to inform their parenting behaviour. This internal tension among participants regarding digital technology use was exacerbated by their awareness of others’ (e.g. strangers to family members) judgements of if, when, how often, for how long and for what purpose their time online was deemed productive. Although the concept of surveillance was not a sensitizing concept at the outset of the study, it was a theme that underpinned the majority of the participants’ accounts of how they used digital technology in the context of the transition to parenting. We report one overarching theme of ‘relational surveillance’ with the associated subthemes of: (1) Self-surveillance: ‘This app is telling me I’m ovulating’, (2) Other/interpersonal surveillance: ‘They were judging me’ and (3) Systemic/societal surveillance: ‘On Instagram, it looks like people have their shit together’. Given our sub-thematic analysis, we align our understanding of relational surveillance to be inclusive of how individuals move through interconnected networks of varying contexts (e.g. people, environments, processes) that continually shape one's behaviour and understanding of self. 18
Self-surveillance: ‘This app is telling me I’m ovulating’
Behaviours of self-surveillance threaded throughout the entire transition to parenting, from pre-conception, prenatal to the postnatal period. As an extension of their developing maternal identities, participants adopted a range of self-surveillance strategies that were prompted, mitigated and directed by digital technologies, which began during pre-conception. Immediately following the focus group moderator's question regarding potential app use during the pre-conception period, participants spontaneously started to compare their platform choice(s) among one another within the group. This generated a lively dialogue about the benefits of some over others, as well as personal preferences depending on reproductive information needs at any given stage: As one participant shared: ‘I used a fertility app to know when I was ovulating. And then when I got pregnant, I used another app to show like what the baby was’. [T1] In contrast, another participant explained how using digital self-surveillance influenced a range of health-related behaviours, including her dietary choices and decisions to engage or not in intercourse with her partner: ‘I was not eating like certain things. I wasn't drinking. I, you know, you can only have sex on like these two days. don't come near me before that. Like save it all up and we weren't getting pregnant. So, like one month I didn't do any ovulation tests, I didn't follow the app. Actually, when I got pregnant, I wasn't even supposed to be ovulating’. [T2]
Participants frequently described how the pervasiveness of digital self-surveillance technologies caused them to question their own intuitive sense of their bodies. One participant described themself as deferring to the apparent authority of the technology over their health and well-being, a sentiment that resonated with other mothers in this study: ‘… [ovulation tracking] became consuming for me because it took us about a year to get pregnant the second time… But I couldn't, even though I would try not to track… and then I felt like I started doubting my body because it’d be like “well this app is telling me I’m ovulating.”’ [T12]
As participants described, such digital self-surveillance extended over significant periods of time and intensity; as one woman noted: ‘My periods were four or five a year, so I needed to make sure I knew when they were due to know if I was late or, you know, if I was ovulating at the time. I’ve used that app for probably five years’ [T2]. Trailing from this reflection, was the sentiment expressed by another participant: ‘it [ovulation tracking] was a job’ [T11]. Another participant extended the concept of self-surveillance with their app ovulation tracking usage being akin to a job, onboarding an obsessive use of the technology: ‘… I found that when I was, like, following it [ovulation tracking] so stringently that I was almost, like, obsessing over it. Like, it's gotta be this day, like, and then it didn't, for my body, it didn't really work that way’. [T3]
Interestingly, one participant noted that it was her non-use of a tracking app that was responsible for an unintended pregnancy: ‘I did not use an app. That's why [child's name] got her - he was a surprise. I’m a single mother’. [T1]
Once pregnant, digital self-surveillance practices pivoted to the growth and well-being of the fetus and self. Participants described an unrelenting drive to search for reassurance regarding the health of their fetus, and digital technologies were central to their self-surveillance at this stage of their transition to parenting: ‘So, for me, like YouTubing the sound of the placenta blood flow versus a baby's heartbeat… I mean, I feel like it [personal doppler use] did put me at ease for the most part, maybe when I was having difficulty finding it [fetal heartbeat], then it was, like, more stressful. And I know my husband had to hide it from me from time to time because I was using it too much and then I was, like, Googling ‘is a sound wave safe?’ Like, should I like not be using it?’ [T11]
Additionally, some participants described how using digital technologies to access information about ‘appropriate’ body changes (e.g. weight gain) during pregnancy led to negative feelings about oneself: ‘I always felt like I was way bigger than other people and always became paranoid … I felt …big and ugly and but, like, it's because you’re comparing. You see these photos, picture perfect pictures that are like set up and the perfect angle and stuff’. [T12]
Digital technologies continued as surveillance devices during labour. In this case, apps were commandeered as digital birthing coaches: ‘So, when my contractions were like two to three, four minutes apart, it was kind of like, well my pain is not an eight yet. Which she told me once your pain is at like a seven or eight, then call me. So, I was like, okay I’m listening to my app, but I’m also, like so I was also doing a lot of both instead of just sort of putting all my eggs into the app’. [T12]
During the postpartum period of the transition to parenting, the participants often described how digital technology use facilitated self-surveillance to selectively curate their online presence as a new mother. These participants were self-critical of their pregnancy-related physical changes, which limited their willingness to post about themselves online: ‘After I had her, I dropped every single inch – I went right back to my pre-birth weight and then slowly, I gained it back. So, like I’m more self-conscious about it now. So, I don't really post like in terms of myself’. [T2]
Once their infants were born, participants yielded to digital technology and online resources to ensure correctness of their parenting practices inclusive of infant feeding, hygiene, sleep and safety. Additionally, some commented on deferring to others online, often strangers, for reassurance: ‘Validation, like searching for, like, validation in order to, like, get that positive energy from somewhere else versus like, you know, how you have to, like, get it from within’. [T12]
Once participants had transitioned into the role of new parenting, digital surveillance technologies continued to serve as instruments of tracking, recording, cuing and cataloguing: ‘There is another app…basically, you go in and you can like, you can track like, the feeding, the changing, like when did you feed, when did you change. Like, if you’re breastfeeding; left breast or right breast how long. and then they updated it to like, bath time, playtimes…and then medicine you can put in what medicine, how much they get it, how often. And then it would like keep it tracked on a chart so you can go see it on a chart and you can like, see the patterns and everything’. [T3]
To this end, some participants undertook the role of analyst, piecemealing together data stored within various apps to aid in parental decision-making.
Even when outside the home, participants spoke of an incessant need to monitor their infants, and could do so with the use of digital technologies: ‘I just look to see if he's still sleeping and I find that, like, when we’re out for dinner, like you’re out, I find I can't completely let that go. Oh, is he still sleeping? Rather than just trusting that [babysitter] will call me and message me if I’m needed. It's, like, okay [just] let me watch him’. [T12]
Participants in this study were not passive consumers of online health information, and within the focus group discussions, several questioned the accuracy of the information they were being supplied and shared with the group the strategies they employed to mitigate potential backlash from others online (e.g. posting comments anonymously or lurking only to obtain information without asking specifically for feedback). Others also attempted, with varying success, to self-restrict their personal use of digital technologies: ‘I had to delete some of the apps from my phone for the longest time, so I wasn't getting that trigger, like that immediate, like, you don't need to respond to every notification as soon as it pops up. It's like that, I don't know, that dopamine rush. You hear a ‘bing’. But even if you silence it, then I found okay, I’ll just silence it. And then it's well, did I miss something? I’m going to check to see. And it's like, okay, that's not working either. Just remove from my phone for a while, and then I got it back’. [T12]
As the aforementioned quotes exemplify, despite their attempts to cut the digital umbilical cord, some felt an irresistible tug to get back online. For other participants, app usage decreased after the birth of their babies: ‘I don't really use any apps now’ [T2]. One participant stood in contrast to other group members, reflecting on the motivations for avoiding social media: ‘I’m just a very abnormally private person and so is my husband when it comes to social media. I don't know if that's like nerves. I don't know if that's like I’m afraid of judgment’. [T1]
Other/interpersonal surveillance: ‘They were judging me’
Surveillance in the transition to parenting extended broadly beyond the self, to include intensive surveillance within their familial (as defined by the participant to include family and/or friends) relationships with others. They discussed the judgements they faced from other family members and partners about their technology use, while also participating in surveilling the appropriate use of others’ technology. Participants surveilled within the context of their relationships were highly scrutinized about their use of technologies in the transition to parenting. Relational surveillance by partners and family members contributed to self-judgement, doubt and lack of privacy. For example, one participant described how her family monitored their digital technology use and intervened when they disagreed with the participant's parenting approach: ‘Like I would be feeding her, and I would be looking at these chat groups or scrolling Facebook or whatever. My mom was, like, you’re not bonding with your daughter…stop that. She's like give me your phone, and she’d like literally take it away from me when I was with her, and I’m like, you know, you’re right’. [T11]
Other participants described how their families’ surveillance of their digital selves impacted their sense of personal privacy. As one participant stated: ‘My mom for example, she was constantly going through my Facebook and stuff like that where I would have no privacy as in now’ [T5]
Participants also described how being the subject of familial surveillance fostered self-judgement of their own parenting activities: ‘My boyfriend comes over a lot and he like complains and I’m like always on my phone now. I tried, like I said, I tried not to be but if I’m not playing with my son or whatever, like he – and my daughter, she's on like technology too. So, if I’m not playing with my son, like I’ll be on my phone or like I think that he just catches me at bad times where I’m checking my phone or if I’m bored you know, I’ll be on phone. But I don't feel like I’m on it like constantly because I have to clean, I have to cook. Like I have to bathe the kids and so, yeah’. [T5]
As these quotes demonstrate, the surveillance of participants’ behaviour that was undertaken by family members often served as a ‘corrective’ moment wherein participants’ behaviour was shifted or promoted self-judgement because of this feedback.
In addition to being the subject of familial surveillance, participants also described how they engaged in surveillance of friends’ and family members’ inclusion of digital technology use in their parenting approaches. Recounts of such surveillance were often judgemental and included assessments of how digital devices were being used by the parents to calm their children. For example, one participant used her own parenting approach as a comparator when assessing their friend's use of digital technologies during car rides: ‘I have friends who started this where their kid will not get in the car unless they have an iPad or a phone and I’m like, how did that start. Like you obviously started that and then they liked it and then they got upset when you didn't do it. Whereas I’ve only ever given my kids like a toy or a book to play with in the back. But I see a lot of kids that wont, like actually have full on meltdowns if the iPad is not playing on the back of the seat’.[T11]
Another participant described the prevalence of digital device use among other parents’ children at meal time as impacting social interactions between the family: You see it at restaurants now where like no one talks….And my niece she won’t eat unless she has, she’s watching Sesame Street on the iPad or on the cell phone. [T11]
Systemic/societal surveillance: ‘On Instagram, it looks like people have their shit together’
Self and familial surveillance were interconnected with systemic surveillance in the transition to parenting. Systemic/societal surveillance included the ways in which participants perceived or feared the judgement of members of the wider community (online or in person) and those who held formalized positions of power. For instance, as one participant explained, she was hesitant to provide updates online about her pregnancy based on earlier experiences because she had not disclosed paternity online: ‘They were judging me because they didn't know who the baby daddy was. I knew who it was, but it's just they don't know because they’d never seen me with a guy more than a month. So, it's like they probably thought, oh, I don't know who the dad is. So, me thinking that that's what they’re thinking and they’re judging me, and I got asked that a couple times, do you know who the father is and it's like people I don't even talk to’. [T9]
Participants frequently reported how their digital activities were surveilled systemically (and in some cases enacted systematically) when accessing a range of social services. For example, one participant who resided in a shelter for single mothers described how ubiquitous systemic surveillance of her digital technology use was used to influence both her parenting behaviours and future access to social supports: ‘Like the group home wouldn't allow us [residents] to allow [infant] to watch TV…they [the workers] write notes on about you and then they get back to CAS [child protection services]…you obviously wanna like do what they’re telling you to do so then it doesn't look bad on you…it's funny because when we [residents] were there, we kept asking them if we could have like internet access and stuff. I had no phone when I got there [group home], like I was ready to leave. I had no contact with anybody…it's like a maternity home where like, you know, like kids are there. They’re like ‘you shouldn't be on your phones while you’re playing with your kids’ and technically that's what you’re supposed to be doing all the time. So, unless you were taking pictures, you weren't allowed to be on your phone unless your kid was sleeping’. [T5]
Within the health care system, entrenched normative understandings about the appropriate use of technology among early childhood were pervasively negative. One participant described her interaction with a health care provider as follows: ‘I remember like the first doctor's appointment or one of the first I had after she was born, the first thing my doctor said was ‘no screen time before two’, and I was like, ‘screen time? What is screen time? I had never heard that’ and she [physician] goes, ‘you’d be surprised how many parents will pop their baby in front of an iPad or a TV as young as a couple months old and they just sit there like watching it’, and I was horrified. I was like ‘I never even thought of that’, but she says it to every new parent, “No screen time.”’ [T2]
Online or digitally derived expectations of parenting were used by the participants as the standard for their own mothering: ‘I have a seven-month-old at home and a three-year old and trying to do all this stuff and just like watching other nutritionists doing this and watching other people do this and thinking, okay, well maybe I should do that or maybe, you know, I’m not doing enough or I’m not living up to like those expectations. So, I was putting on like unsolicited expectations on myself that weren't even coming from me, what I wanted and I started kind of like spiraling. Just kinda comparing and thinking, second guessing myself and just, yeah. It just wasn't feeling good anymore’. [T12]
Although they were aware of the fabricated nature of online presentations of the self, some participants also felt compelled to participate in these illusions. In doing so they reified the very normative representations and expectations of a narrowly prescribed and unrealistically attainable hegemonic image of ‘good mothering’19,20 they were problematizing: ‘We [partner and participant] almost didn't make it, like, you know. And I didn't tell that story, I only showed the great story, so social media can be really negative in that sense and I think especially in that fragile postpartum period, we’re so vulnerable and we’re so out there, like, not feeling good really about where we are…On Instagram, it looks like people have their shit together’. [T12]
Discussion
Within this study relational digital surveillance accounted for individuals’ lived context, exerting a powerful influence on these women's experiences, perspectives and behaviours in relation to the self and others during the transition to parenting. 21 Participants described their relationships with technologies within and across the blurred domains of the self, other/interpersonal and systemic/societal. The ‘self’ was rooted within various technological communities; whereas other/interpersonal relationships functioned within a network comprised of partners, parents and friends and systemic surveillance was informed by the voices of those who acted with authority via positional power, in participants’ lives. As demonstrated by many participants in this study, digital technologies enabled and facilitated mothers’ incessant engagement in behaviours of self-surveillance (‘am I too big for being only 12 weeks pregnant?’); however, surveillance did not end with self-appraisal of their personal fittingness when compared to the digitally curated self of another online image. Surveillance by others prompted recursive thinking, looping almost unabated, on their correctness of their actions – to do, not do, do better, do differently, in the face of online information. Participants shared multiple examples of basing their behaviours and decision-making off information they gathered online, and on the reactions of others to their use of digital technologies. In effect, they ‘outsourced’ their agency, which speaks to the vulnerability women in our study experienced in relation to doing ‘good mothering’. With this in mind, we draw on the concept of ‘societies of control’ 22 to theorize the role of digital technologies in the transition to parenting as a broadening from surveillance, to one of control. Surveillance societies as characterized by Foucault 23 rely on specific architectural arrangements to produce the desired outcome among individuals, rendered into ‘docile bodies’. People become visible to others in these bounded spaces, while mechanisms of control are at least partially obscured, thus one never knows when they are or are not being watched (e.g. hospitals, jails, classrooms). 23 Consequently, people take up the role of state surveillance to police their own behaviours, and self-correct according to the normative ways of being, thinking and doing within a given sociopolitical–historical context.
With the advancement of digital technologies, control societies are increasingly present as individuals’ data-producing behaviours, and overall acceptance of the omnipresence of digital technology becomes normalized. Consequently, power is diffused and embedded into a matrix of technologies that track, prompt and codify granting access to the minutiae of humans’ every movement. 24 In the context of the transition to parenting, this increasing ‘dataveillance’ capitalizes on maternal anxieties produced through the downloading of systemic accountabilities into the hands of mothers. Uptake of these digital technologies has been folded into the normative discourse that drives the way we think about the performance of good mothering, characterized as intensive, self-sacrificing and all-consuming. 10 Such intensive mothering has long required of women professional-level skills, high levels of physical, psychological and emotional energy as well as money. 25 However, in the context of the existing digital technologies landscape, women in our study demonstrated how this intensification of mothering no longer has any material boundaries and are so pervasive they have become normalized as a crucial element of what is understood to be responsible, good mothering.
The pregnant body has long been medically surveilled and socio-culturally re-positioned according to technological advancements of the day 12 and the commercialization of digital technologies once reserved for clinical settings (e.g. fetal dopplers and oxygen saturation monitoring for infants) reflects some of the more recent tools commodified to enlist parental labour in service of surveillance. In effect, these commercialized and increasingly accessible technologies promise expectant mothers that motherhood is nothing more than a practice of data management. 10 Historically, the emergence of the fetal sonogram marked a pivotal evolution in mechanisms of surveillance of the fetal environment, a ‘womb with a view’ 26 that would extend its gaze beyond its intended clinical significance. To this day, the digital image of the fetal environment is highly politicalized, weaponized to repeal abortion access, criminalize individuals seeking to end a pregnancy and used to perpetuate stigma of ‘good’ motherhood. 10 As scholars note, digitalization of maternal responsibilities was aided by the technological developments in reproductive visualizing technologies. 9 This form of individual responsibility and self-governance relates to a new mother's burden of caring for, and ensuring their child's health, beginning during pre-conception.
This one technological innovation alone, set the stage for the intensification and diversification of surveillance (and later control) technologies to come, and serves as a powerful exemplar of what can happen when these technologies generate information that lands in the hands of those without medical authority to accurately interpret the data. The availability of these digital technologies has recruited everyday citizens to become pseudo experts in the (digital) management of pregnancy and parenting outcomes.
Our findings further demonstrate that digital technologies facilitate surveillance behaviours to operate beyond the individual person and extend to the realm of relationships. Participants were subjected to commentary and judgements from others about their digital technology usage as a dimension of their evaluation as mothers. The use of digital technologies among participants in our study extended the ‘gaze’ or oversight to others – family members, friends, their health care providers and virtual actors – to scrutinize their motherhood. Our findings indicate that digital technologies and online platforms reinscribe what good mothering looks like, how good mothering is performed, the types of interactions, where these interactions happened and when these interactions happened among pregnant/new mothers, to curtail or mitigate harmful responses.
Systemically/societally, participants faced judgement from those who held positional, authoritative power relative to themselves. These authority figures (e.g. physicians, social workers) wielded their position to discourage their clients from what they perceived to be inappropriate use of digital technologies but without the benefit of longitudinal research evidence to support their claims. Tan and Goonawargene 27 conducted a systematic review of the influence of patients’ Internet health information seeking on the patient–provider relationship. From their analysis, the risk of judgement or avoidance of the topic altogether, from their care providers, contributed significantly to patients’ reluctance to disclose their online information-seeking behaviour and the information they found during searches. Additional study findings report that some physicians’ reactions appeared to discredit the patients’ capacity to appropriately use the Internet to become more informed about their health. 28 Findings from Sjöström et al., 29 demonstrated that health care providers’ unwillingness or inability to engage in dialogue with Internet-informed patients about the digital technologies they utilize misses a critically important avenue to promote equitable care, enhance health literacy and counter potential misinformation. Findings from our study demonstrate that mothers are indeed looking online for health information, and most critically, they are using this information to digitally surveil the health of their pregnancies and newborns. Participants in this study not only accessed health information from recognized research and clinical experts through their clinical encounters but also accessed through social media platforms and online apps. 1 They also appreciated and sought information created by other parents and especially mothers’ groups who shared their pragmatic expertise on many of the issues and challenges that are part of the transition to parenting journey. The diversity of content and content contributors to health and health-related online social media platforms and apps opens up important conversations related to our understanding of health information experts and evidence.30,31 This is an area of future research given the importance of online information access juxtaposed to the proliferation of online health misinformation and disinformation.
Patient/family-focused models of care offer a more proactive and collaborative approach to determine how to best support families with their online activities, taking the broader context in which each family navigates these decisions.32,33 Rather than avoiding altogether or completely dismissing parents’ usage of technology to aid in health information seeking, professionals would benefit from the invitation to challenge their assumptions of parental device use, and the presumed ill health and social outcomes for children. It would be beneficial for care providers to move beyond a ‘just don't search’ approach, to activities that enhance health literacy/digital health literacy 34 and decrease parents’ exposure to platforms that amplify anxieties and self-doubt. In the context of highly prolific online health (mis)information, this research raises critical questions about how care providers hold positions of influence (or not) pertaining to digital surveillance technologies.
Participants in our study felt they were often caught in a double bind of being expected to utilize whatever digital tools were available at their disposal for the sake of their families’ well-being, while simultaneously being highly scrutinized by others about whether their digital activities were appropriate, or potentially damaging to their families’ well-being by being distracted and ‘too connected’. Paradoxically, increasing amounts of information, services and support once available to pregnant and parenting women in person (such as prenatal classes and lactation support), have now moved almost exclusively online. 35 Given the continued ravaging impacts of the COVID-19 pandemic at the time of this article's writing and online information curation (e.g. online misinformation and disinformation), mothers are increasingly faced with little to no choice but to accept (albeit with hesitation), uncertainty regarding the credibility and reliability of their sources as they search online for health information, peer support and social connections during the temporally bound transition to parenting. Findings from our study highlight the potential for harm and further disenfranchisement among mothers who experience oppression (e.g. housing precarity, limited formal education), and who may not have the financial means, privacy or personal safety to utilize digital technologies in ways that support their well-being during the transition to parenting.
Limitations
Data were collected prior to the COVID-19 global pandemic. There can be no doubt about the pandemic's influence on patterns of digital technology usage during pregnancy and parenting; a great many of the very services people depended upon (prenatal appointments), went virtual. Therefore, study findings must be contextualized to the time preceding the pandemic. Additionally, all participants in this study spoke English as their first language. Future research should consider the intensification of surveillance practices deployed in service of the state directly or indirectly, among populations who are racialized, and for whom surveillance of their mothering behaviours carries with it the added fear of anti-Black racism, stigmatization, discrimination and criminalization. 36 As most participants within this study identified as white, middle-class, cis heteronormative, it is important that future research consider the experiences of LGBTQ2+ parents negotiating the transition to parenting in a digital context. Furthermore, future research should also explore the role digital technologies play in the lives of disabled parents during the transition to parenting, and how surveillance may serve an added health-enhancing role in supporting the tracking and monitoring of their health and the health of their infants.
Conclusion
Relational digital surveillance calls attention to the unrelenting desire for those who are pregnant and parenting to find meaningful use of digital technologies in service of optimizing health outcomes for themselves and their families. The role of relationships (self, other/interpersonal and systemic/societal) and the interplay between them, as an added layer of surveillance, has not to our knowledge previously been explored in the research literature. This broadened understanding of how surveillance operates within and across relationships demonstrates the web of impossibilities and uncertainties mothers traverse in relation to their own relationship with digital technologies. Furthermore, attention should be paid to the commercialization and sources of promotion of digital self-surveillance technologies during the transition to parenting, and the potential undesirable outcomes on maternal and infant well-being. In doing so, critical questions should be raised to uncover the underlying interests and biases of the designers of the algorithms that power the digital surveillance technology, as well as those who may profit, monetarily or otherwise, from the peddling of these digital wares to new and expectant parents. Awareness that parents are being shaped into clinical care providers because of the commodification of the transition to parenting further pushes the boundaries of hegemonic mothering practices and can be used to inform the development of new digital health-promoting resources by appropriate health authorities. Ultimately, accounting for such social factors may promote the development of digital health resources that support the health and well-being of women and their infants within the omnipotent environment of digital surveillance technologies.
Footnotes
Acknowledgements
The authors would like to thank the participants for their contributions to this research.
Author note
Lorie Donelle is currently affiliated with College of Nursing, University of South Carolina, Columbia, SC, USA.
Contributorship
All authors contributed equally to the development of this manuscript.
Conflict of Interests
The authors declare that this is no conflict of interest.
Ethical approval
The Research Ethics Board at Western University approved this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fanshawe College Research Fund, (grant number #2019-08-FRF).
Guarantor
LD.