
Abstract
Background
Mobile health technologies have shown promise as delivery platforms for digital health coaching for chronic conditions. However, the impacts of such strategies on users’ health beliefs, intentions and ultimately clinical outcomes are understudied.
Objective
This study sought (1) to evaluate the effects of a digital health coaching intervention on participants’ belief constructs; and (2) to assess relationships between these belief constructs and intentions to utilize the technological intervention, actual adherence metrics and clinical outcomes related to hypertension.
Methods
Thirty-four participants with hypertension were recruited from a university community from January to May 2021. They self-measured weight and blood pressure (BP) for 30 days followed by digital coaching delivered via a mobile application for 30 days. Surveys assessed constructs from the Health Belief Model and Technology Acceptance Model, compared to intention, health belief, BP self-monitoring adherence and BP outcomes. A path analysis model was used to assess the relationships between constructs and intention, adherence metrics and clinical outcomes. A Kruskal–Wallis test was used to identify changes in beliefs.
Results
Participant health beliefs significantly improved after coaching, including self-efficacy (H(1) = 15.12, p < 0.001), cues to action (H(1) = 5.33, p = 0.02), attitude (H(1) = 10.35, p = 0.002), perceived usefulness (H(1) = 15.02, p < 0.001) and decreased resistance to change (H(1) = 4.05, p = 0.04). Adherence to BP measurements positively correlated with perceived health threat (β = .033, p = 0.007) and perceived ease of use (β = .0277, p < 0.001). Self-efficacy (β = −2.92, p = 0.02) and perceived usefulness (β = −3.75, p = 0.01) were linked with a decrease in diastolic BP.
Conclusions
A mobile health coaching intervention may help participants improve beliefs regarding hypertension self-management.
Introduction
In the United States alone, more than 100 million adults were reported last year to suffer from hypertension, a chronic condition characterized by having a systolic blood pressure (SBP) ≥ 130 mmHg or a diastolic blood pressure (DBP) ≥ 80 mmHg. 1 When uncontrolled, hypertension can cause complications such as kidney disease, stroke and heart disease. 2 The U.S. Department of Health and Human Services estimated that annual medical costs associated with hypertension care are approaching $200 billion domestically. 2
Hypertension is associated with unhealthy lifestyle choices, such as a sedentary lifestyle and a poor diet, and the presence of comorbidities such as diabetes and obesity. 3 Adopting healthy habits is key to the effective management of hypertension; however, sustainable behavior change has shown to be a major challenge. 4 Health coaching, which focuses on encouraging health-related behaviors via goal-setting and education, 5 has shown promise in improving hypertension and other chronic disease outcomes. 6 We have previously highlighted the need for more research on the efficacy of behavior coaching to improve the self-management of hypertension due to several limitations in the literature such as the absence of significant improvements in clinical outcomes, 6 or the need for a human coach to provide the coaching.7,8
The emerging mobile health (mHealth) technologies can serve as reliable platforms to deliver automated digital health coaching while facilitating continuous data collection and communication between patients and providers.9–11 While mHealth interventions have grown in popularity over the past decade, there is limited evidence of their efficacy mainly due to a lack of longitudinal methods. 12 In addition, despite the promise shown by these technologies, adoption, adherence and user satisfaction have been documented as relatively low. 13
Previous research has investigated behavioral constructs and beliefs to understand their predictive utility for adherence to technological interventions. 14 While these efforts have shown promise in identifying links between health beliefs and intentions to use mHealth interventions, studies have generally focused on investigating beliefs at a single point in time.10,15 To our knowledge, Dou et al. 16 is the only study that investigated the health beliefs as predictors of intention to use a Self-Measured Blood Pressure (SMBP) monitoring intervention that included a blood pressure (BP) cuff device and an associated mHealth tool for daily self-measurements and then compared the intentions to actual usage. While Dou et al.'s study provides evidence for the efficacy of using health belief constructs in predicting intentions to use a technological intervention for hypertension, more research is warranted to validate such findings and better understand the relationship between beliefs and actual behaviors performed.
To address this gap, this research focused on documenting a longitudinal study investigating two main objectives: (1) to evaluate the effects of a digital health coaching intervention on participants’ belief constructs and (2) to assess the relationships between these belief constructs and intentions to utilize the technological intervention, actual adherence metrics and clinical outcomes related to hypertension. The intervention used was an SMBP plus weight kit that included a weight scale and a BP cuff device as well as mHealth coaching.
Belief constructs and hypotheses
To quantify the relationship between behavioral constructs and intention or actual use, we utilized several constructs from the Health Belief Model (HBM). Health Belief Model has been commonly used to investigate the relationship between health beliefs and individuals’ intention to perform a health-related behavior. 17 In addition, the widely used Technology Acceptance Model (TAM) 18 was utilized to assess use-related constructs such as perceived ease of use and perceived usefulness. Finally, in line with Dou et al., 16 the resistance to change construct which assessed the willingness to try new interventions and perform new behaviors was added. A total of 24 questions were elicited from the participants to create nine constructs. These constructs were used to define several hypotheses that are detailed below.
The HBM posits that behavioral intention is influenced by several constructs. In this study, intention is operationalized as the intention to complete the tasks assigned to improve one's hypertension self-management while the actual behavior or adherence was measured as the number of assigned tasks completed.
First, perceived health threat from HBM assesses the degree to which an individual may perceive their condition as threatening to their health, 17 which has been found to influence intention to manage hypertension. 16 Therefore, we hypothesized that perceived health threat from hypertension is positively associated with the intention to use the intervention (H1a). Accordingly, we hypothesized that perceived health threat is positively associated with participant adherence to the required tasks (H1b). Additionally, previous research has shown that education about the risks of unhealthy behavior increases perceived health threat. 19 Therefore, we hypothesized that educating participants about the risks of hypertension using American Heart Association (AHA) content increases their perceived health threat (H1c).
Self-efficacy refers to how confident the individual is in their ability to manage their condition. Dou et al. 16 found that self-efficacy had a significant relationship with the intention to adhere to an SMBP regimen. Therefore, we hypothesized that high self-efficacy positively impacts the intention to use a hypertension coaching intervention (H2a). In addition, given the evidence of low self-efficacy among patients with hypertension, 20 we hypothesized that health coaching increases self-efficacy (H2b) since participants would have access to educational resources and may be more motivated to adopt a healthy lifestyle. Finally, in previous research, participants with hypertension who had high self-efficacy showed higher adherence to self-management routine, 21 so we hypothesized that higher self-efficacy is positively associated with adherence to required tasks (H2c) and with significant improvement in their clinical outcomes (H2d).
Perceived barriers, which relate to the perception of the potential negative aspects of performing a certain health behavior, 17 have been found to negatively influence intentions to perform that behavior. 22 Therefore, we hypothesized that perceived barriers is negatively associated with intention to use the intervention (H3a) and adherence to the required tasks (H3b). Also, it is expected that perceived barriers to managing hypertension would decrease through the course of the intervention since participants are provided with the motivation and devices needed to better self-manage their condition. Therefore, we hypothesized that the hypertension coaching intervention lowers participants’ perceived barriers (H3c).
Cues to action reflects individuals’ internal ability to remember to perform certain tasks or behaviors. It has been shown that stronger cues to action influence the intention to perform behaviors. 17 Therefore, we hypothesized that cues to action are positively associated with the intention to manage hypertension (H4a). Similarly, it was expected that our digital coaching intervention which includes goal setting and reminders would support such prospective memory to perform the required tasks regularly (e.g., BP measurements). 23 Therefore, we hypothesized that higher cues to action is positively associated with participants’ adherence to performing required tasks (H4b), and that cues to action would increase significantly as a result of the intervention (H4c).
One of the constructs in TAM is attitude which refers to how favorable a behavior may be to the individual. 18 Attitude has been found to positively influence the intention to use technology. 24 Therefore, we hypothesized that a positive attitude towards managing hypertension is positively associated with the intention to do so (H5a) and with adherence to performing required tasks (H5b). In addition, since our intervention includes coaching content from a credible source such as the AHA, then we hypothesized that participants would have a significant improvement in their attitude towards hypertension self-management (H5c). 25
Next, perceived usefulness, a core construct of TAM, has been shown to positively influence the use of technology. 18 Perceived usefulness indicates how useful and beneficial a system is perceived by an individual to help achieve a specific purpose. Therefore, we hypothesized that perceived usefulness is positively associated with participants’ intention (H6a) and adherence to the required tasks (H6b). We also hypothesized that participants’ perceived usefulness of the hypertension coaching tool will increase after exposure to the intervention (H6c).
Additionally, perceived ease of use from TAM has been used to show that technologies that are easier to use positively influence intentions to use them 26 ; therefore, we hypothesized that stronger perceived ease of use is positively associated with intention (H7a) and user adherence to required tasks (H7b). We also anticipated that given the user-centered design approach used to design and evaluate the intervention, our participants would have an increase in the perceived ease of use after exposure to the hypertension digital coaching intervention. Therefore, we hypothesized that perceived ease of use will significantly increase after exposure to the intervention (H7c).
Resistance to change, originally from the Dual Factor Model, 27 is based on the claim that there are inhibiting beliefs that prevent individuals from trying new behaviors that could help them with their condition. Resistance to change has been found to negatively influence intention in various studies.16,28 Therefore, we hypothesized that resistance to change is negatively associated with intention (H8a) and user adherence to required tasks (H8b). Finally, interventions that successfully change behavior or improve outcomes may mitigate participants’ resistance to change as per the Dual Factor Model. 27 Therefore, we hypothesized that the hypertension coaching intervention will lower the participants’ resistance to change (H8c).
Methods
Study design
A longitudinal study was conducted which required participants to use a custom-designed mHealth app called HyperCoach along with Bluetooth-enabled BP cuff and weight scale devices for 60 days. The first 30 days of the study were labeled as a health awareness phase while the next 30 days were labeled as the health coaching phase. The study was conducted between January and May 2021.
Intervention components
In the health awareness phase, participants were reminded to self-measure their BP and weight once every day shortly after they woke up in the morning while seated but did not receive any additional health coaching content. The devices used were the upper arm BP monitor and weight scale by Indie Health (Del Mar, CA). The health coaching phase involved completing daily health coaching tasks in addition to the self-measurements following an AHA-endorsed 30-day plan. The HyperCoach app included a 30-day calendar and a list of daily tasks with visual indicators for complete or incomplete tasks (Figure 1). The daily tasks consisted of daily self-measurement of weight and BP during the health awareness phase and reviewing educational material (short 1–2-page articles and short 2–3 min videos) on self-management of hypertension as well as weekly self-assessment quizzes during the health coaching phase. For tasks to be marked by the app as completed, at least 2 min of videos must have been watched by the participant, and the written articles required a minimum of 1 min of reading (operationalized as having the article open without switching to another app/screen). Participants were able to view visualizations showing their BP and weight trends as well as daily and weekly averages and received automated reminders to complete the daily measurements in both phases. However, participants did not receive tailored feedback regarding their outcomes and were only contacted via email in case of missing measurements for more than two days. A more detailed description of the health coaching tasks, the HyperCoach mHealth app, and the general impact on outcomes are discussed in Markert et al. 29

Preview of the HyperCoach app.
Participants
Participants were recruited through a bulk mail sent out to a large university community in the southern United States. Participants were included in the study on a rolling basis. Power analysis showed that at least 30 participants are needed to achieve a medium Cohen's effect size of 0.5, a significance level of (α = 0.05), and a power of 80%. To account for attrition, we aimed to recruit 36 participants. The inclusion criteria only allowed participants who were at least 18 years of age or older, spoke English and whose primary diagnosis was hypertension. Additionally, participants had to take medication to control their hypertension and use an iOS smartphone with continuous internet access. Participants were excluded if they had resistant hypertension, or more than two comorbidities based on the Charlson Index to limit the effect of confounding variables and complications from other diseases. 30
Study procedure
During an onboarding video call which lasted around 20 min, participants were instructed on how to utilize the app, BP Cuff and weight scale and practiced using the devices on camera. Behavioral constructs mentioned earlier were measured using questionnaires administered electronically through the app before the health awareness phase, before transition to health coaching phase and end of the study (Figure 2). Ten constructs were measured with at least two questions for each construct (Table 1) to assess reliability. The questions for each construct were adapted from another study 16 and were rated on a 1–7 Likert scale ranging from Strongly Disagree to Strongly Agree. A quality of life (SF-36) 31 questionnaire was also administered electronically before and after the health awareness phase and at the end of the study. Measures of clinical outcomes, namely SBP, DBP and weight were self-measured daily. Adherence metrics were also assessed including total time spent on educational material, total educational content completed, BP and weight readings taken, and assessments and quizzes completed.

Study timeline.
Questions and constructs used in the study as well as the reliability measures.

TAM: Technology Acceptance Model; HBM: Health Belief Model.
Analysis
Reliability
Constructs that included more than two questions were tested using Cronbach's alpha for reliability while questions that only included two questions were assessed via a Spearman's correlation to assess reliability. The first three constructs had more than two questions, so Cronbach's alpha test was performed. Results for attitude (α = .93), intention (α = .74) and perceived health threat (α = .87) indicate high reliability. Spearman's correlation analysis showed adequate reliability for the other variables (p < 0.001 for all variables) (Table 1).
Changes in beliefs
To test for significant changes in the behavioral constructs over time, a Kruskal–Wallis test was performed since the Likert scale data are considered to be nonparametric.
Belief constructs, adherence metrics and clinical outcomes
A Partial Least Square (PLS) regression analysis was conducted to assess the relationships between the dependent variable (DV) and the independent variables that may have influenced it. The first test considered the DV to be intention and assessed its relationship with other belief constructs. This was followed by assigning adherence to BP measurements as the DV and comparing adherence to the belief constructs. Lastly, changes in clinical outcomes such as DBP were compared to the belief constructs. RStudio was used for all analyses and utilized the packages “lavaan” and “QuantPsyc”.
Results
Out of 36 participants who initially signed up, 35 enrolled and commenced the study. However, 34 participants completed the study since one participant dropped out of the study due to personal obligations and other health issues. Participants had a mean age of 44.8 years (SD = 14.1; range 19–79). Out of the 34 participants, 25 identified as female and nine as male. Participants had a mean baseline SBP of 136.3 mmHg (SD = 18.4), a mean baseline DBP of 84.2 mmHg (SD = 11.4) and a mean baseline BMI of 32.0 (SD = 6.9). Full demographic information can be found tabulated in our other article on the general outcomes of the study. 29
Changes in beliefs
The means of belief constructs and Kruskal–Wallis analysis for change in respective beliefs can be found in Table 2. Only one construct, namely perceived ease of use significantly increased (H(1) = 17.87, p < 0.001) in the health awareness phase from (Mdn = 4) to (Mdn = 6) just before coaching began and then to (Mdn = 7) after coaching was complete. Therefore, H7c was supported. However, by the end of the study, six additional constructs had improved due to coaching. Self-efficacy increased as well (H(1) = 15.12, p < 0.001) from (Mdn = 4.75) to (Mdn = 6.5); therefore, H2b was supported. Cues to action increased (H(1) = 5.33, P = .02) from (Mdn = 5.25) to (Mdn = 6), so H4c was supported. Attitude increased (H(1) = 10.35, p = 0.002) from (Mdn = 5.95) to (Mdn = 6.5); therefore, hypothesis H5c was supported. Perceived usefulness increased (H(1) = 15.02, p < 0.001) from (Mdn = 6) to (Mdn = 6.5); therefore, H6c was supported. Resistance to change decreased significantly (H(1) = 4.05, p = 0.04) from (Mdn = 2) to (Mdn = 1.25), so H8c was supported. Perceived health threat decreased from the beginning of the study to the end of the study; however, this change was not statistically significant. Therefore, H1c was not supported. Similarly, while perceived barriers decreased over time, this change was not significant. Therefore, H3c was not supported. A full list of hypotheses and whether they were supported or not is included in Table 3.
Belief means and significant changes over two months.
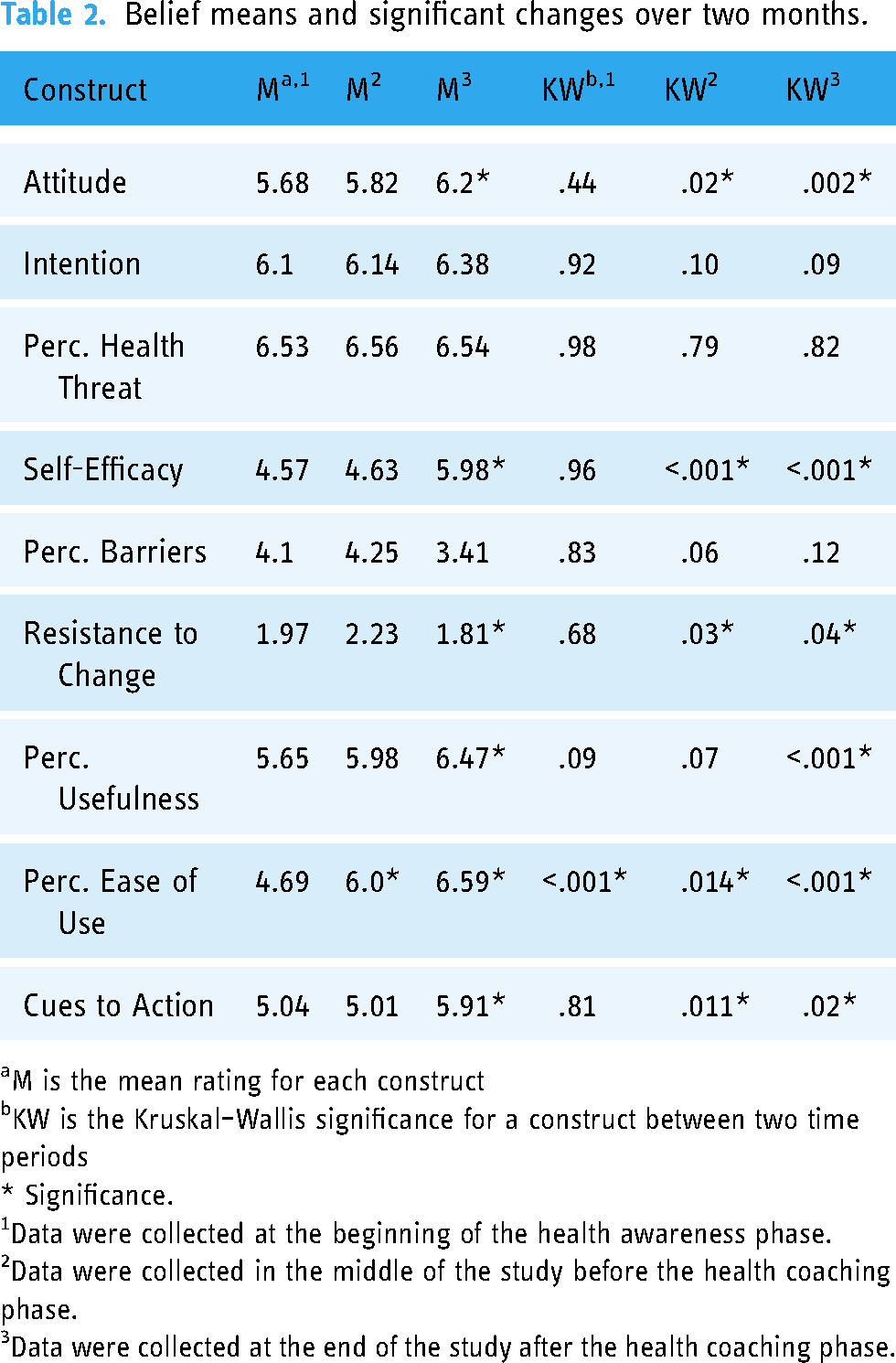
M is the mean rating for each construct
KW is the Kruskal–Wallis significance for a construct between two time periods
* Significance.
Data were collected at the beginning of the health awareness phase.
Data were collected in the middle of the study before the health coaching phase.
Data were collected at the end of the study after the health coaching phase.
Hypotheses status.

Belief constructs and intention
At the beginning of the coaching phase, intention was significantly predicted (R2 = .79, F(10,23) = 8.49, p < 0.001) by four constructs as represented in Figure 3. Perceived health threat had a significant positive effect (β = .32, P = .017). Perceived barriers had a mild effect (β = .12, P = .016). Attitude had a significant positive impact (β = .29, P = .006) and resistance to change had a negative effect on intention (β = −.18, P = .006). Therefore, H1a, H5a and H8a were all supported. Higher perceived barriers had a mild positive effect on intention contrary to the original hypothesis so H3a was not supported. The other behavioral constructs did not have an impact on intention, so H2a, H4a, H6a and H7a were also not supported.

Significant constructs impacting intention.
Belief constructs and adherence metrics
A t-test for participant adherence with completing BP and weight measurements was performed and indicated a significant increase in measurements taken (t (44.63) = −2.66, p = 0.011) during the second phase of the study which included coaching. Specifically, the adherence of participants to perform their recommended measurements of BP and weight increased from an average of 26.5 measurements out of 30 (SD = 4.47, range: 15–30) during the health awareness phase, to 28.74 out of 30 (SD = 1.92, range: 21–30) during the health coaching phase. All health coaching tasks were completed comprehensively by the participants during the health coaching phase.
The PLS regression conducted showed no relationship between adherence to BP measurements and beliefs during the health awareness phase. As for the coaching phase (Figure 4), adherence to measurements was influenced by several behavioral constructs (R2 = .79, F(11,22) = 7.78, p < 0.001) including perceived health threat (β = .033, p = 0.007), intention (β = −.060, p = 0.001), self-efficacy (β = −.014, p = 0.044), cues to action (β = .019, p = 0.001) and perceived ease of use (β = .0277, p < 0.001). Therefore, H1b, H4b and H7b were all supported. Self-efficacy had a contrary effect on BP measurements compared to the hypothesis so H2c was not supported. No other variable had a significant impact on BP measurement adherence; therefore, H3b, H5b, H6b and H8b were not supported. No other significant relationship was found between any of the belief constructs and the weight measurements performed, assessments completed or educational material completed.

Relation between constructs and blood pressure (BP) measurements and diastolic BP.
Belief constructs and clinical outcomes
The impact of the intervention on clinical outcomes is out of the scope of this paper and is reported in more detail elsewhere. 29 In brief, during the health coaching phase participants’ mean SBP significantly decreased from 136.3 (SD = 15.6) to 130.8 (SD = 13.5), as well as mean DBP which significantly decreased from 85.1 (SD = 9.5) to 81.2 (SD = 9.5). Quality of life also improved significantly during the health-coaching phase. 29 On the other hand, the decrease in weight was not significant; therefore, a longer study may be required to report a more noticeable improvement.
An assessment of the relationship between change in health outcomes and behavioral constructs during coaching revealed that only change in DBP (R2 = .56, F(11,22) = 2.53, p < 0.001) had a significant relationship with self-efficacy (β = −2.92, p = 0.02) and Perceived usefulness (β = −3.75, p = 0.01). Therefore, H2c was supported. No significant relationships were found between the belief constructs and SBP, weight change or quality of life during coaching (Figure 4).
Discussion
This study showed that several constructs related to health beliefs have improved because of a technological intervention to improve hypertension outcomes. In addition, we found interesting relationships between some of these constructs and intentions, adherence and clinical outcomes.
Changes in beliefs
Although we did not expect a change in beliefs during the health awareness phase, our findings showed that perceived ease of use improved significantly. This is in line with the interviews conducted at the end of the study where participants reported that the app was easy to use. 29 However, limited functionality was operational during this phase which could explain the lack of significant improvement in the perceived usefulness of the app or any other beliefs. When the coaching features were introduced, several beliefs significantly improved. First, perceived usefulness, attitude and resistance to change significantly improved indicating the participants benefitted from the app features. We believe this is mostly due to improvements in health outcomes which have positively affected the perception of the intervention. Second, self-efficacy improved significantly during the coaching phase. Setting goals for the intervention, empowering participants to achieve those goals, and a positive trend in health outcomes might have helped participants feel more confident in their routine as suggested by Direito et al. 25 Third, daily reminders to perform measurements may have helped participants form a habit of recalling to perform behaviors related to hypertension self-management. In turn, this led participants to perceive a significant increase in their cues to action. Finally, perceived health threat is believed to be impacted by training and education. 32 In fact, our previous study evaluating an educational intervention to mitigate drowsy driving among nurses showed a similar impact of education on perceived health threat. 19 However, we did not witness any improvement in perceived health threat in this study. A possible explanation for this finding might be the scope of the educational and coaching content that focused more on mitigation methods and healthy behaviors compared to making the consequences of hypertension tangible.
Belief constructs and adherence metrics
As expected, during the health awareness phase, no significant relationships between adherence measures and beliefs were detected. Similarly, as hypothesized, during the coaching phase, we found a positive correlation between perceived ease of use of the app, perceived health threat and stronger cues to action and adherence to BP measurements. However, in contrast to previous research (e.g., Tan et al. 21 ) a negative relationship between adherence and two health beliefs, namely self-efficacy and intention was found. This counterintuitive relationship can be explained by the intention-behavior gap 33 which posits that even with strong intentions, inaction may happen due to forgetfulness, willpower or complacency. Such complacency might have been the case in our study due to significant positive progress and may describe the counterintuitive findings related to self-efficacy. Indeed, in our study, those with higher self-efficacy had a stronger decrease in their DBP which might have led to complacency. It is notable that participants with hypertension have generally been found to have lower self-efficacy than participants of other chronic conditions 20 which necessitates interventions to improve participants’ perception of their abilities to self-manage their condition. However, our results may suggest that the benefits of increased self-efficacy may diminish if not managed properly. Similar effects have been widely documented in the literature where upon accomplishing personal goals, individuals become complacent which results in a worse subsequent performance (e.g., Vancouver et al. 34 ).
Belief constructs and clinical outcomes
In addition to the significant improvement in SBP and DBP mentioned briefly in the results above and reported in Markert et al., 29 we attempted to test the relationship between beliefs and changes in clinical outcomes. We found a linear relationship between self-efficacy and perceived usefulness and DBP. In other words, the more confident the participants felt in managing their condition and the more useful they perceived the intervention to be, the more improvements they have seen in terms of lower DBP. This finding reaffirms the strong relationship between self-efficacy and participant progress in managing hypertension seen in the literature. 35 However, no linear relationship was found between any beliefs and the decrease that occurred in SBP even though (as reported elsewhere 29 ) mean SBP and DBP both significantly decreased after the coaching phase. The probable reason for this could be that SBP has been reported to have a greater variation coefficient than DBP, 36 making a linear relationship between SBP and beliefs more difficult to detect.
Limitations and future work
This study had some limitations that could impact the generalizability of findings. First, the sample size is relatively small, and the population used was from a large university community in Texas. Indeed, this is reflected in our sample's demographics which show homogeneity in education levels. 29 Demographic factors have been previously reported to impact participants’ understanding of hypertension which may affect beliefs as in our study. 37 Additionally, our population consisted of either students or working-age adults, thus our findings may not be generalizable to an elderly or retired population that may have difficulty utilizing the app and devices. More work may help validate our findings with smaller and more stratified samples across education, geographical location, age and other variables. Second, despite our promising results, it is not clear if the benefits and beliefs changes observed are sustainable. Work is in progress in collaboration with the AHA to address these gaps in a follow-up study that evaluates the efficacy of a 90-day hypertension coaching plan in well-served and underserved areas to gather a larger more diverse sample and assess aforementioned metrics over a longer period of time. Third, a repeated measures design was used where the same group participated in both the health awareness phase and the health coaching phase given the pilot nature of the study and small sample size. Future work should aim to include a control group with no exposure to the either phase of intervention. Fourth, while the belief questions were adapted from a similar study within the hypertension context, some questions were generalized to the overall intervention while the others (e.g., ease of use) focused on the app not the devices. More work is warranted to include additional questions per construct to account for all components of the intervention. Finally, since this at-home study was naturalistic in nature, then we did not have control over some confounding variables that may have influenced the participants’ change in beliefs, behaviors or clinical outcomes.
Conclusions
There is a general gap in understanding the utility of using participants’ beliefs to predict behaviors and clinical outcomes when exposed to technological interventions. The results from this study showed that some health beliefs such as attitude, resistance to change and perceived health threat were key predictors of intention to use a mHealth coaching plan for self-management of hypertension. We also found that utilizing this intervention was effective at helping participants with hypertension improve beliefs such as self-efficacy, internal cues to action, attitude and perceived usefulness regarding the self-management of hypertension. Consequently, this may have led to improvements in their adherence to daily measurements and a significant decrease in BP. More work is warranted to monitor these changes over a longer study period and across a more diverse population.
Findings from the study primarily show the efficacy of using health beliefs and technology acceptance constructs to predict intentions and actual behavior when exposed to mHealth coaching interventions. Given the nonintrusive and cost-efficient nature of these methods, even modest predictive utility may provide valuable input during front-end analyses. The findings also show that mHealth digital coaching interventions may provide participants with hypertension the training, resources and motivation needed to improve their attitudes and beliefs toward managing their condition, may increase their adherence to a new self-management regimen which may improve clinical outcomes, lower risk of cardiovascular disease and increase life expectancy. 38 Moreover, since intention alone may not be sufficient in predicting action, 16 accounting for belief constructs such as perceived health threats, cues to action and perceived ease of use may help in capturing more of the variance of the actual behavior as seen in this study. Given the evidence presented in this paper, interventions focused on these three variables may potentially prove effective in positive changes in behavior. For example, coaching content can educate the participants about the long-term effects of unhealthy behaviors and habits to increase the perceived health threat or integrated targeted reminders may increase participants’ cues to action and support the prospective memory to perform a particular behavior. Future work should consider incorporating behavior change techniques explicitly aimed at targeting specific constructs based on the impact they have on specific beliefs. 25
Footnotes
Acknowledgments
The study was developed in conjunction with the American Heart Association Center for Health Technology & Innovation and utilizing coaching material developed as part of the American Heart Association's 12-week hypertension CarePlan. The authors would also like to thank Jacob M. Kolman, MA, ISMPP CMPP, of Houston Methodist and Texas A&M University, for his critical review, editing and formatting assistance.
Contributorship
KZ, CM and FS conceived and designed the study, oversaw the study's progress and wrote the first draft. KZ and CM reviewed the literature, gained ethical approval and collected and analyzed the data. All authors reviewed and edited the manuscript and approved the final version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The study was approved by the Institutional Review Board of Texas A&M University (IRB2019-1070), and informed consent was obtained electronically from all participants.
Funding
This work was sponsored by the National Science Foundation Engineering Research Center: Precise Advanced Technologies and Health Systems focused on Underserved Communities (PATHS-UP).
Guarantor
FS.