
Abstract
Objective
The aim of this pilot study is to identify the main predictors and barriers that influence user intention to adopt teledentistry services among the Saudi population.
Methods
A total of 426 respondents completed a questionnaire. Our study used the technology acceptance model to predict how users will adopt teledentistry. An analysis of the factors that influence patient users’ intention to utilize teledentistry was conducted using partial least square structural equation modeling.
Results
Among the factors that influenced the intention to use teledentistry services, social influence positively affected the intention (β = 0.18, t = 2.19, p-value = 0.03), whereas perceived risk negatively affected it (β = −0.21, t = 2.69, p-value =0.01).
Conclusion
The perception of risk was a major barrier to the adoption of teledentistry services, while social influence was a significant positive predictor. Using the findings of the study, policymakers and health service providers can gain a better understanding of the factors influencing the implementation of teledentistry.
Introduction
During the past few years, information and communication technologies have revolutionized the delivery of health care.1,2 Telemedicine refers to the use of computer technology, telecommunications, and clinical expertise to provide services such as diagnostics, consultations, and treatment remotely.3,4 Teledentistry is the application of telemedicine in the field of dentistry. 3 A variety of modalities can be used to deliver teledentistry services, such as synchronous (live video), asynchronous (store and forward), remote patient monitoring, or mobile health (mHealth). 5 With teledentistry, oral health care can be more readily accessible and delivered more efficiently at a lower cost. 6 Additionally, it might reduce rural and urban oral health care disparities. 6
In 1994, a large teledentistry project was implemented to serve U.S. soldiers and their dependents worldwide. 7 Teledentistry has been shown to reduce overall costs, improve patient care, and provide more complete data analyses than traditional referral processes. 7 Teledentistry has been adopted somewhat slowly; however, many dental practices and hospitals have been encouraging teledentistry since the start of the coronavirus disease 2019 (COVID-19) pandemic.8,9 As dental procedures significantly increase the risk of transmission, face-to-face consultations have been severely restricted. 10 Risk assessment, triage, and the management of emergency dental care have frequently been accomplished remotely by telephone or video link as the first step in the urgent dental care system. 9
In the sight of the American Dental Association, with the help of teledentistry dental practitioners can now reach a greater number of patients, thus enabling greater access to dental care. 5 A high level of patient satisfaction has generally been documented with telemedicine consultations.11–13 For example, the majority of patients at Massachusetts General Hospital rated telemedicine follow-up visits as more convenient than in-person appointments. 14 According to a recent survey of private U.S. health plan members, the majority of those who participate in U.S. private health plans will use video or online services if they are available. 14
Previous studies have examined the acceptance of teledentistry among dental professionals and dental students in Saudi Arabia.15–20 However, there is a lack of published evidence showing that patients are ready to accept teledentistry.21,22 The aim of this pilot study was to determine the perceptions of the Saudi population regarding teledentistry and to identify any existing gaps in terms of patient preferences.
Methods
This study was reviewed and approved by the Institutional Review Board at King Abdulaziz University Faculty of Dentistry (#286-09-21). The survey was distributed from December 2021 to March 2022. Participant eligibility criteria included living in Saudi Arabia and being 18 or older. All participants provided informed consent. The main outcome of this study is the intention to use teledentistry.
In this study, we used the technology acceptance model (TAM) to predict how users will adopt teledentistry and to identify any design flaws in the information system before it is widely used. 23 The TAM theory was developed in the 1980s as an information system model that describes how users accept and use technology over time. 24 It was thought that the key to increasing the adoption of information technology (IT) was to increase acceptance, which could be measured by asking individuals about their future intentions to use it. 25 It is possible to increase the adoption and use of IT by understanding the factors that shape one's intentions. 25 The questionnaire used was adopted from previous studies.23,25–29 To fit the goal of the study, minor adjustments to the questionnaire were made. The questionnaire consists of two parts. The first part concerns the demographic characteristics of the participants—gender, age, marital status, nationality, education, employment status, income, region, living area, study/work in the dental field, dental insurance, chronic disease, and last dental visit. The second part deals with eight constructs of TAM adopted from previous studies—facilitating conditions, perceived ease of use, perceived risk, perceived usefulness, resistance to use, social influence, technological anxiety, and trust.23,25,29 All constructs and their definitions are shown in Table 1.
List of the proposed constructs.

FC: facilitating conditions; PEOU: perceived ease of use; PR: perceived risk; PU: perceived usefulness; RC: resistance to use; SI: social influence; TA: technology anxiety; T: trust; UI: usage intention.
The questionnaire was developed in English. It was translated into Arabic using the forward and backward translation method. The questionnaire was provided in English and Arabic via the QuestionPro platform. 30 Participants were recruited using a non-probability snowball sampling method. The questionnaire was distributed through social media platforms (WhatsApp, Twitter, Instagram, and Snapchat). Pre-testing was conducted to ensure the validity and effectiveness of the questionnaire. All participants were required to sign a consent form.
Sample size calculation
The sample size was calculated using the online Raosoft sample size calculator. 31 It was calculated using a 35 million population size, 32 50% response distribution, a 95% confidence level, and a 5% margin of error. This study required a minimum sample size of 385 participants. A total of 770 participants will be recruited to account for any missing data or non-response rate.
Statistical analysis
Univariate analysis was conducted to calculate the frequencies and percentage of the participants’ characteristics. Partial least square structural equation modeling was used to examine the factors that affect users’ intention to use teledentistry. 33 The standardized path coefficient, t-statistics, and the bootstrapping method were used to test the structural model. The significance level was set at a p-value of < 0.05. Data was analyzed using IBM-SPSS (version 20; Armonk, NY, USA) and SmartPLS 3.3.5 software.
Results
Sample characteristics
Of the 966 people who received the questionnaire, 426 completed it; 89 were ineligible (younger than 18) and were excluded from the study. Table 2 shows the study sample's characteristics. The study sample tended to be Saudi women who are married, hold a bachelor's degree, and are employed in the governmental sector. Approximately 45% of the study sample fell in the age range of 30–49, and more than one-third have a monthly income of >10,000–20,000 SAR. The majority live in urban areas, with 47% living in the Western region. About 38% have dental insurance, and more than two-thirds have had a dental visit in the past year.
Characteristics of the study population (n = 426).
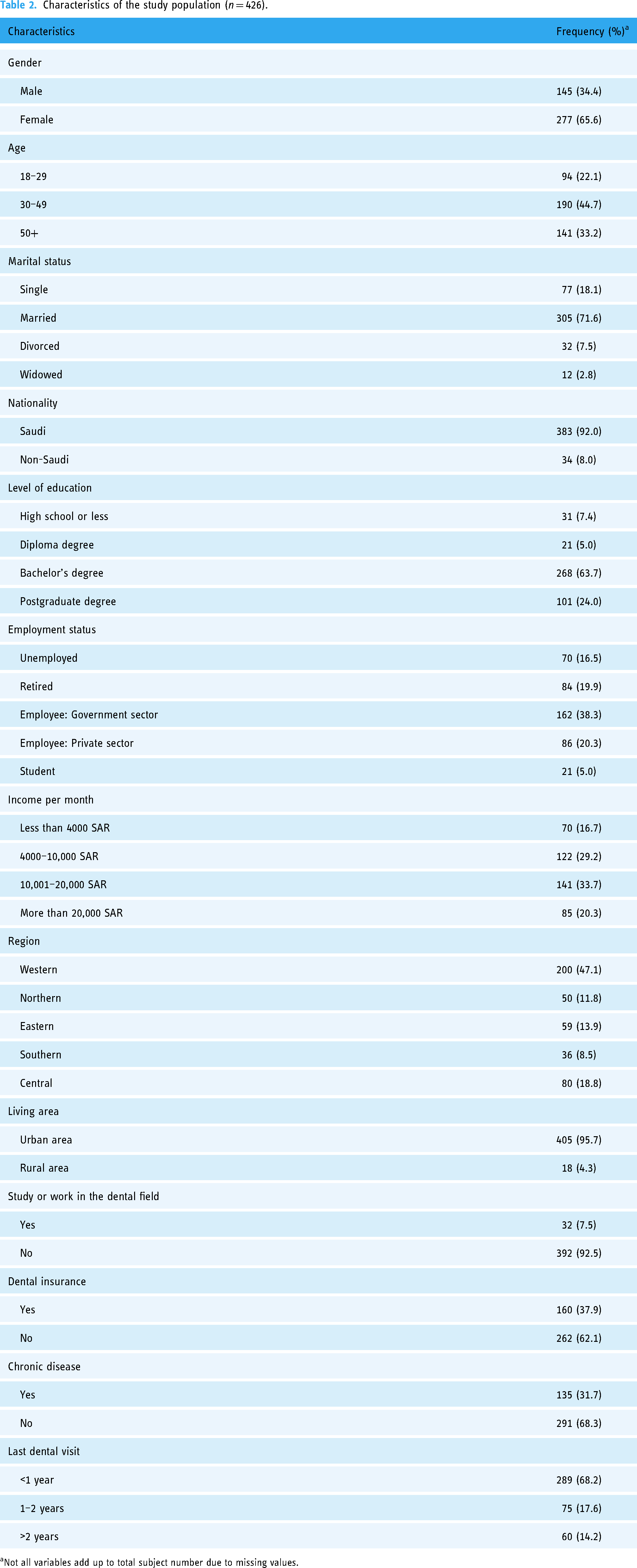
Not all variables add up to total subject number due to missing values.
The measurement model
Exploratory factor analysis revealed that T2 (Teledentistry systems will require me to be cautious with this technology) and T3 (I feel satisfied and confident that I will be able to rely on the benefits of teledentistry) had an Eigenvalue of less than 1. Therefore, they were not retained in the analysis. 34
To assess the construct validity of the variables, a confirmatory factor analysis was conducted (Table 2). All items had factor loadings greater than 0.5 in relation to their constructs, indicating construct validity. 35 A Cronbach's alpha was calculated for all constructs to ensure internal consistency, with all scales exceeding the recommended value of 0.7. 36 A composite reliability of 0.80 and an average variance extracted (AVE) of over 0.5 were met for all constructs to ensure convergent validity (Table 3). 37
The measurement model.
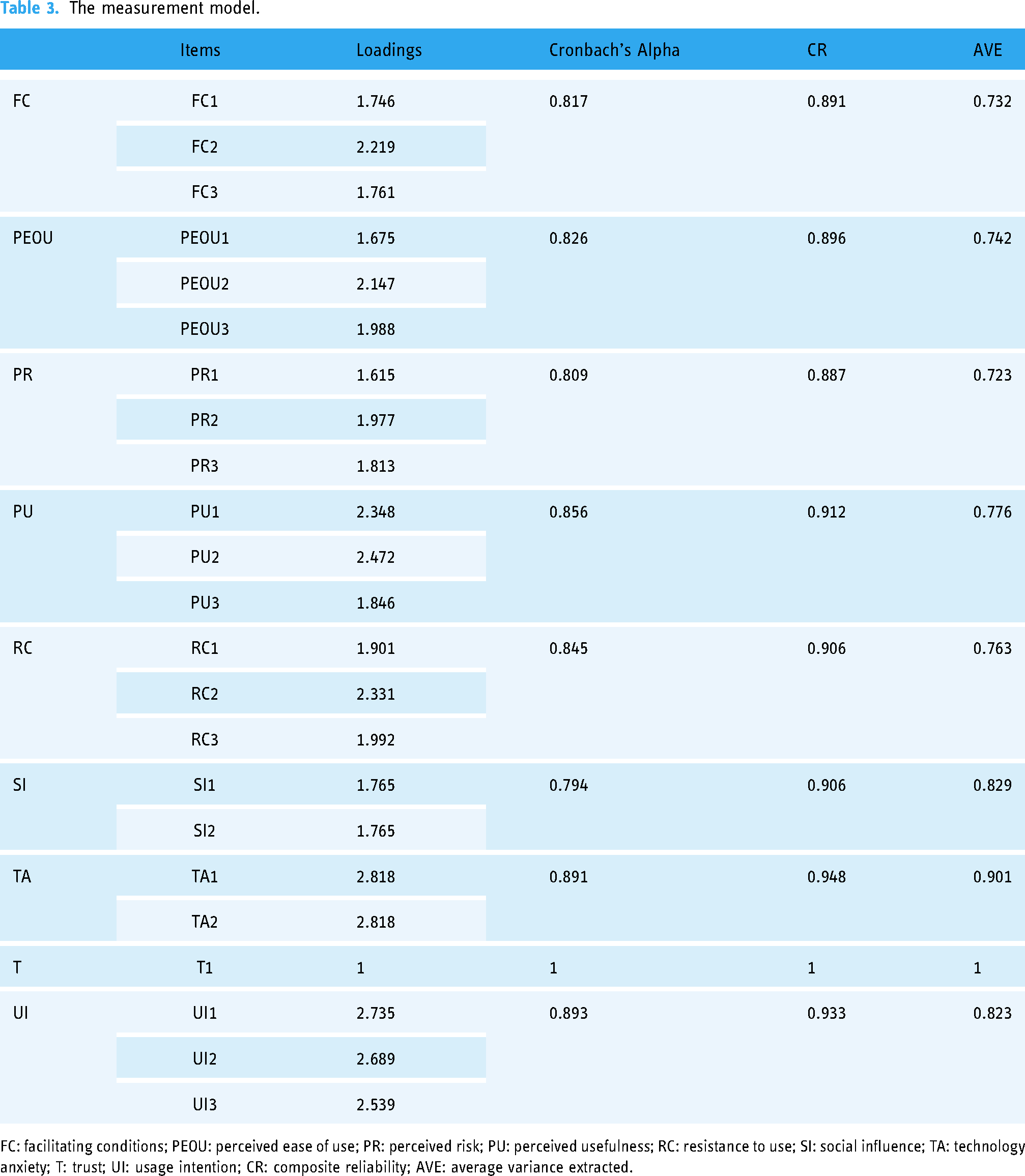
FC: facilitating conditions; PEOU: perceived ease of use; PR: perceived risk; PU: perceived usefulness; RC: resistance to use; SI: social influence; TA: technology anxiety; T: trust; UI: usage intention; CR: composite reliability; AVE: average variance extracted.
The correlation matrix
The square root of the AVE was compared with correlations between the constructs under study to ensure discriminant validity. 37 For each construct, the square root of AVE was larger than correlations with other factors 37 (Table 4).
The correlation matrix.

FC: facilitating conditions; PEOU: perceived ease of use; PR: perceived risk; PU: perceived usefulness; RC: resistance to use; SI: social influence; TA: technology anxiety; T: trust; UI: usage intention; AVE: average variance extracted
Square root of AVE for each latent variable.
The structural model testing
To verify the model fit, the normed fit index (NFI) and standardized root mean square residual (SRMR) were calculated. The NFI was 0.815, and it has been suggested that a value higher than 0.8 is considered a good fit. 38 The SRMR was 0.051, which is considered a good fit according to Hu and Bentler. 39
Table 5 presents the relationship between the independent variables and the dependent variable (usage intention). Hypothesis testing demonstrated the positive effects of facilitating conditions, perceived ease of use, perceived usefulness, social influence, and trust, although the only significant factor was social influence (β = 0.18, t = 2.19, p-value = 0.03). The factors that had negative influence were perceived risk, resistance to use, and technology anxiety, with perceived risk being the only significant factor (β = −0.21, t = 2.69, p-value = 0.01).
The structural model.
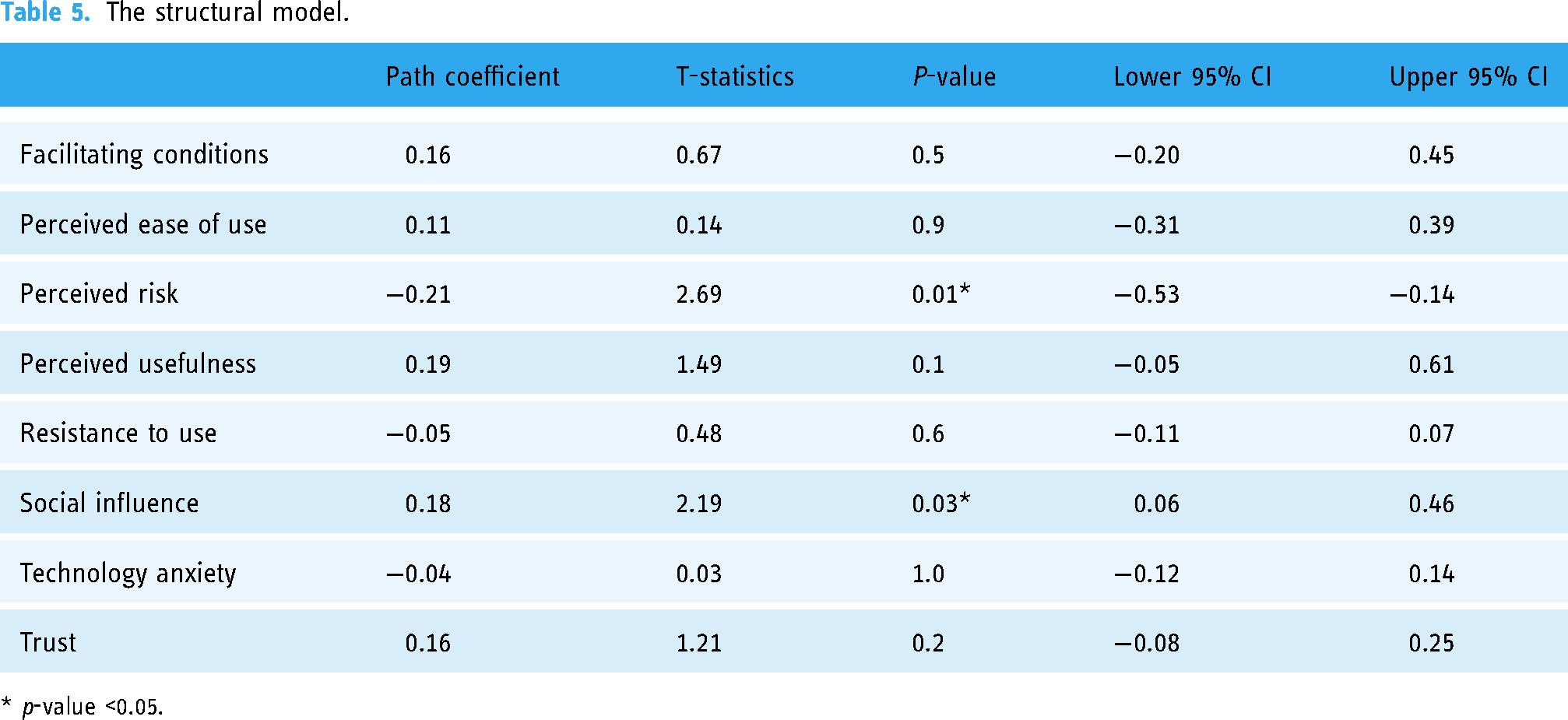
* p-value <0.05.
Discussion
The World Health Organization has published a set of guiding principles for the implementation of telemedicine services during the COVID-19 pandemic, and the differences in accepting teledentistry across countries is expected to vary. Therefore, this pilot study used TAM to predict the acceptance and use of teledentistry among the general population in Saudi Arabia. This model is used to identify the main predictors and barriers that influence the user intension to adopt teledentistry services.
Social influence is defined as factors that motivate or inhibit people, including the extent to which individuals consider their peers’ opinions, particularly those of friends and acquaintances, regarding how they should behave. 28 Our findings reveal that social influence is a positive significant predictor for the acceptance of teledentistry services by the general population. It is consistent with previous studies that social influence is found to be a positive determinant of users’ intension to use teledentisty.23,40,41 It is likely that an individual's willingness to use teledentistry services will increase if their family members or peers consider these services to be effective in improving their oral health. It is possible that uncertainty created by newly introduced innovations makes potential adopters seek the opinions of their peers and local social circle. 42 Furthermore, most respondents in this study were aged 30–49 (generation Y), and social networks account for a larger share of sources of information about dental and health care. 43
Evidence has shown that social influence is a potentially important determinant of users’ willingness to adopt new technologies.44,45 Additionally, studies on technology acceptance in health care often apply Rogers’ diffusion of innovation theory. According to this theory, apparent elements of innovation, dissemination through social channels, and time are key factors influencing the spread and success of the innovations. 46 It is therefore important to incorporate social influence into major technological acceptance models for both scholars and health care organizations to gain a better understanding of the issue. Consequently, health care policymakers need to engage well-known and trusted community members and local public figures when introducing new technology-based health services so they can facilitate the diffusion of these services among the general population and facilitate the acceptance of these services. As technology use will continue to be driven by social influence, future multi-theoretical studies are needed to better understand how social networks influence behavior and referent effects, so that the subjective norm can be enhanced and users’ adoption of teledentistry services can be predicted. 47
Perceived risk is an individual's perception of uncertainty when deciding to take a particular action or engage in a particular activity. 48 Our findings revealed that perceived risk was a major barrier to users’ intention to use teledentistry. The effect of perceived risk on users’ adoption of technology-based health care services has also been observed in other studies.23,49 Technology-based services are associated with uncertainties and risks that are distinct to patients and health care providers, and perceived risk plays a significant role in the decision to use them.50,51 Previous studies have identified several aspects of perceived risk, such as psychological risk caused by reduced mental satisfaction, the financial risk caused by cost barriers, and performance risk associated with a probabilistic perception of insufficient health information when using online services. 23 Perceived risk has been shown to contribute to the expectation of destructive consequences, which then negatively influences usage intentions. 52 The respondents’ insecurity and perceived sense of risk regarding teledentistry services may be reasonable, as the impersonal nature of these services is the main barrier when seeking online oral health care. 53
The use of teledentistry is becoming increasingly popular in order to manage patients more effectively. Teledentistry can be particularly useful in remote areas that are difficult to reach. Patients were able to learn about their treatment and diagnosis through teledentistry, as well as educational programs that raised awareness about oral health. 54
This study has a few limitations. First, it used an online questionnaire that was completed exclusively by individuals who are computer literate and who have Internet access. Therefore, the results cannot be generalized, as the bias towards interest in this subject could not be avoided, and the opinions of individuals in resource-constrained places were not explored. Furthermore, the responses were collected during the COVID-19 pandemic, which may have influenced the respondents’ acceptance decisions. Last, due to the cross-sectional nature of this study, causality cannot be determined. However, this was the first study to utilize a theoretical framework to assess the facilitators of and the barriers to predicting the Saudi population's future intention to adopt teledentistry services. In addition, the results of this study suggest that policymakers and health care authorities should formulate strategic plans by identifying the key aspects in adopting teledentistry services from the patient perspective to ensure effective diffusion.
Conclusion
Social influence was found to be a significant positive predictor of the adoption of teledentistry services, whereas perceived risk was found to be a major barrier. These empirically based insights are important to help policymakers implement effective strategies to ensure the large-scale successful acceptance of teledentistry services.
Footnotes
Acknowledgments
The authors acknowledge Omar Khalid Abdulwassi and Youssef Ghassan Ajab Noor who participated in the data collection.
Author contributions
LB and MA researched literature and conceived the study. OA and YA collected the data. LB analyzed the data. The manuscript was drafted and critically reviewed by LB and MA. LB and MA approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was reviewed and approved by the Institutional Review Board at King Abdulaziz University Faculty of Dentistry, Jeddah, Saudi Arabia (#286-09-21). All methods were performed in accordance with the principles of the Declaration of Helsinki.
Informed consent
All participants provided informed consent.
Guarantor
LB