
Abstract
Objective
The research aimed to study digital divide by determining the usage of digital technology among older adults with cognitive frailty (CF) in Malaysia.
Methods
The dataset was obtained from the AGELESS trial screening phase conducted from October 2021 to March 2022, involving 476 community-dwelling Malaysian older adults (67.7 years old ± 6.1). Digital technology usage was assessed and CF was determined using Fried's criteria and Clinical Dementia Rating. A binary logistic regression was used to determine the sociodemographic factors associated with digital technology use among older adults with CF.
Results
The findings suggest a digital divide between older adults with CF and robust in Malaysia. CF individuals (72.1%) were less likely to utilise digital technology, mainly smartphone than robust older adults (89.6%). More than 70% of older people owned social media on their smartphones, namely, WhatsApp. The most frequent online activities in both groups were family interaction and obtaining current news. CF older adults were less likely to play games on their smart devices. Usage of digital technology was more common among male, younger age, attained formal education more than 6 years, had a higher monthly household income, and robust participants.
Conclusions
The usage of digital technology was inversely related to CF status. CF older adults were less likely to integrate digital technology into their daily living compared to robust even though they were familiar with it. The use of digital technology should be reinforced among female, advanced age, widowers/divorcees without formal education and those from lower- or middle-income statuses, and cognitively frail older people.
Introduction
Digital technology is any electronic equipment, systems, devices and resources that induce and cache data from management or education. 1 It is beneficial in promoting and facilitating healthy aging and combating loneliness in older adults.2,3 During the COVID-19 pandemic, digital technology was the primary tool used in various daily routines to comply with physical distancing. 4 According to the Internet Users Survey in Malaysia, the percentage of older adults utilising the Internet daily is merely 6.5% compared to their younger counterparts. 5 However, the usage of the latest digital technology, for example, smartphone and the Internet, has significantly increased among this population, accelerated by the COVID-19 pandemic restrictions.6,7 This is supported by a recent study conducted in Singapore where one-third of older people seemed to adopt digital technology and increase computer use. 6 Information and communications technology (ICT) has emerged as a need that allows people to accomplish job responsibilities, access online services, communicate and participate in leisure and religious activities including older people. 6
Cognitive frailty (CF) is described as a pre-dementia risk involving the presence of mild cognitive impairment and physical frailty simultaneously. 8 The prevalence of CF among older adults varies across countries, ranging from 1.0% to 12.0%.9–11 Evidence showed that individuals who experienced inadequate vitamin D intake, decreased social interaction, depression and advanced age had a risk of CF.12,13 While the shift of increasing usage of digital technology certainly contributed to numerous benefits, older people with cognitive decline face significant hindrances in keeping pace with rapid technological advancement. 14 This growing gap in access to and adopt digital technology among this population, commonly known as the ‘digital divide’, has become a problem about the potential exclusion of this vulnerable group from the various benefits of the digital age. 15 Previous evidence indicated that older adults with lower cognitive ability, mild cognitive impairment and dementia negatively impacted the accessibility of the Internet, adoption and utilisation.16–18 In fact, the usage of digital technology among CF older people was still limited. 19
The World Health Organization (WHO) has mentioned digital health as an alternative platform to improve quality health service by providing an efficient and sustainable healthcare system. 20 Telehealth and telemedicine are part of the broad spectrum of eHealth. 21 Web-based health information service is a practical way to educate and deliver knowledge to the public, including the older population.22,23 Digital technology with Internet, email and text messaging might be a viable platform for health promotion and interaction specifically for younger-age older people and individuals with a particular group of impairment and a lesser degree of disabilities. 24 Adoption of digital technology among the older population was influenced by various aspects such as individual, technology, social and delivery. 25 A review indicated that telerehabilitation might be acceptable among older adults with CF or mild cognitive impairment (MCI) but need to explore further investigation. 7 Understanding and addressing the digital divide gap among older people with CF is essential, given the potential impact on their well-being and social inclusion. This issue, however, still needs to be explored. Many digital divide study among older people focused on gender, age, income and strata, yet to our knowledge, there were limited studies that discussed this issue in the health context.15,26,27
Thus, this research aims to thoroughly explore the digital divide by determining their digital technology usage among a novel population of older adults with CF and its association with sociodemographic characteristics from middle-income countries such as Malaysia during the pandemic.
Materials and methods
Study design
The present evidence utilised data from the AGELESS trial screening phase conducted from October 2011 to March 2022 during the movement control order due to the COVID-19 pandemic. The AGELESS trial is a multi-centre, longitudinal, randomised controlled trial (RCT) recruiting participants from an urban and rural area that aims to reverse CF among the ageing population residing in the community. 28 This study was also a part of developing multi-domain telehealth intervention among cognitively frail older adults in Malaysia. Ethical approval was obtained from the Universiti Kebangsaan Malaysia Medical Research Ethics Committee (UKM PPI/111/8/JEP-2020-347). The sample size calculation for this study used the Cochran, W.G. (1963) formulae. The prevalence of Malaysian older adults using the Internet is 6.5%, 95% confidence interval, statistic for the level of confidence 1.96 (Z value) and 0.05 precision level, and the sample size was 93 older adults. Considering the 10% drop-out rate, thus the total number of participants was 103 older adults.
Scouting was conducted at several places by sharing a poster in the form of PDF via social media platforms such as WhatsApp and Facebook, inviting participants to attend the research centre as well as meeting with persons in charge for further discussions and screening place arrangements such as meeting rooms, halls, mosques and community centres. During the screening phase, the inclusion criteria were older adults aged 60 years and above, living in an urban or rural community and able to communicate in Malay or English. Using purposive sampling, the study location included both an urban (Klang Valley) and a rural area (Rembau, Negeri Sembilan) in Malaysia. Since the screening phase was conducted during the COVID-19 pandemic, strict safety precautions such as wearing face masks, sanitising hands and keeping physical distance from each other were practised during the sessions. Out of 1059 screened older people, a sample of 476 participants was included in this study consisting of CF and non-CF criteria. All participants provided informed written consent to indicate they agreed to participate in the research before completing the questionnaire and receiving an honorarium after the screening.
Materials
Sociodemographic characteristics of the participants include gender (male, female), age, race (Malay, Chinese, Indian), marital status (married, single, widow), living situation (alone, along partners, along family relatives), duration of formal education (less than 6 years and more than 6 years) and level of formal education (not attend, primary education, secondary education, tertiary education), employment status (housewife/not working, retired, employed), household income (US$), strata (urban, rural), family history of dementia, history of traumatic brain injury (TBI), smoking status, alcohol consumption and medical history were obtained.
Since this study was a part of the AGELESS trial, CF status classification followed the published protocol paper by Ponvel et al. (2021) that utilised Clinical Dementia Rating and Fried's criteria. Digital technology assessments were adapted from previous studies by Gordon and Hornbrook (2018) with cultural adaptations which consist of 10 items (see Supplementary material). Among the items are usage of digital technology, how frequent and what type of digital technology, any household using digital technology and the intention of using it, and participants were asked whether they played any games. Content and face validity was conducted among expert panels and older adults. A pilot study was also conducted among this population, and its reliability was tested. Cronbach's alpha reliability coefficient was acceptable (0.72). 29 The higher value of Cronbach's alpha depicts good internal consistency of items in the scale. 29
Statistical analysis
All analyses were conducted using IBM SPSS version 26. Descriptive statistics analysed the age and duration of formal education. Percentage, total number, mean and standard deviation were reported in each row. At the same time, the chi-square test and Fisher exact test tested the association for categorical data. All comparisons between the usage of digital technology groups mentioned in the text are statistically significant, with a value of at least p < 0.05.
A hierarchical binary logistic regression (BLR) analysis was conducted to examine the factors associated with the usage of digital technology. In this analysis, all the significant variables in the univariate analysis were categorised as (1) Model 1, demographic; (2) Model 2, socioeconomic; and (3) Model 3, health. Then, a hierarchical BLR following a stepwise approach was performed. Parameters with significant values in each model were selected in the binary logistic analysis. The results are reported as crude and adjusted odd ratios (ORs) with a 95% confidence interval. Data was statistically significant when the p-value was p < 0.05.
Results
Participants’ sociodemographic
Table 1 shows the sociodemographic information between digital and non-digital technology users. The sample consisted of 476 Malaysian older population aged 60 to 89 years old, with an average age of 67.7 years old ± 6.2 residing in the community. The sample comprised a gender-balance population (46% male and 54% female). More than 80% of the participants were from the Malay ethnic group, 66% were married and most stayed with family members. The mean duration of formal education was 9.0 years ± 4.0, with the majority receiving secondary education. Almost 50% of participants were retired, lived in the urban area and had a mean total household income of 363.91 USD ± 2058.3. Regarding medical history, most participants had no any family history related to dementia or a history of TBI. However, most of them experienced hypertension, high cholesterol and diabetes mellitus. Almost 56% of the older people were classified as CF, yet more than 80% of robust participants were likely to use digital technology.
Descriptive information of the sample and the study variable.
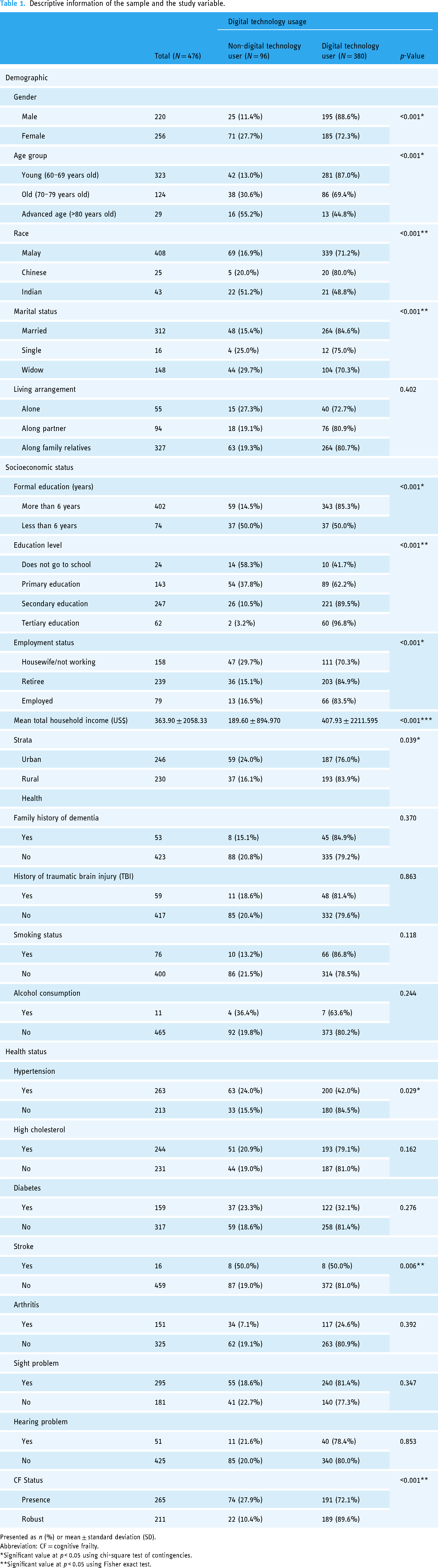
Presented as n (%) or mean ± standard deviation (SD).
Abbreviation: CF = cognitive frailty.
*Significant value at p < 0.05 using chi-square test of contingencies.
**Significant value at p < 0.05 using Fisher exact test.
A substantial mean difference was noted in comparing digital and non-digital technology users. Those using digital technology were more likely to be male, from the Chinese ethnicity group, younger age, married, obtained secondary or tertiary education and retired (p < 0.05). A significantly lower number of older adults with CF (72.1%) used digital technology as compared to robust (89.6%) (p < 0.05).
Prior to conducting regression analyses, bivariate correlations among study variables were determined (not shown in tabular format). All correlation coefficients were in the expected direction, and no concern collinearity was detected. There was a negative relationship between the usage of digital technology and CF status among older adults (r = −0.217, p < 0.01). The hypothesis made was the higher usage of digital technology, the lower status of CF among older adults. The findings from the bivariate correlation analysis validated the proposed hypothesis of treating digital technology usage and CF status as separate outcome variables.
We further examine the COVID-19 sociodemographic parameters predicting daily digital technology. Table 2 summarises the results of the predictors on usage of the digital technology among older adults. In this analysis, digital technology users were more likely to be male, younger older adults, attained more than 6 years of formal education and had higher monthly household income. The likelihood of robust older people using digital technology was two times higher than CF older adults. Ethnicity, living arrangement, employment status, marital status, strata, family history of dementia and TBI, smoking status and other health parameters were not associated with digital technology use.
Hierarchical binary logistic regression (BLR) to predict usage of digital technology.

Dependent variable (DV): usage of digital technology among older adults with CF.
*Significant value at p > 0.05 using hierarchical binary logistic regression (BLR).
Digital technology usage among older adults with CF status
In contingent to the type of digital technology used by older adults with CF and robust, more than 80% of them significantly utilised smartphones daily. Based on Figure 1, usage of smartphones, laptops or computers was considerably lower among older adults with CF (81.5% and 6.5%, respectively) than robust participants (88.0% and 12.1%, respectively). In comparison, tablet usage was almost similar in both groups (5.6% for CF and 6.5% for robust).

Comparison of digital technology devices between CF and robust older adults (N = 476).
Table 3 depicts the usage of digital technology among CF and robust by reporting their use frequency, presence of household digital technology usage and its type, social media account, the function of digital technology and play game on the phone status. Both groups in robust and CF older adults showed significantly utilised digital technology daily. Meanwhile, in this study, household digital technology was referred to any informal caregivers living with participants that used digital technology such as a spouse, children, grandchildren, family relatives or friends. 30 When differentiating these results in accordance with CF status, household digital technology usage among CF older adults showed significant data in utilising digital technology (53.8%) compared to the robust group (46.2%) (p < 0.05). They frequently utilised smartphone (53.5%), followed by laptop or computer (51.4%) and tablet (37.3%) (p < 0.05).
Usage of digital technology among CF and robust participants.

Presented as mean ± standard deviation or n (%).
*Significant value at p > 0.05 using chi-square test of contingencies; **Significant value at p > 0.05 using Fisher exact test.
In terms of social media, more than 70% of participants in both groups notably owned social media on their smartphones. The most common social media platform used in this study was WhatsApp (63.24%), followed by Facebook (37.82%), Instagram (21.42%), Telegram (19.32%) and Twitter (15.76%). According to CF status, a remarkable data of having social media platform was indicated by robust participants than CF participants such as WhatsApp (56.7% and 43.4%, respectively), Facebook (56.7% and 43.3%, respectively), Instagram (61.8% and 38.2%, respectively), Telegram (63.0% and 37.0%, respectively) and Twitter (32.0% and 68.0%, respectively).
Interestingly, 73% of older adults have been accessing the Internet for their daily activities, such as family interaction (63.4%), reading online news (33.6%), online shopping (27.7%) and website exploration (30.7%). In this data, all activities carried out by the subjects seemed higher among robust than CF older people. The most activities accomplished by participants were interaction with family members (52.6% and 47.4%, respectively) and reading online news (59.4% and 40.6%, respectively). In comparison, the least preferred activities were website exploration (50.8% and 49.2%, respectively) and online shopping (56.2% and 43.8%, respectively). With all activities that can be fulfilled, the majority agreed that the Internet could improve their quality of life (80.5%) yet did not keen to play games on their device (12.8%).
Discussion
In line with limited evidence on digital technology use among older adults with CF, we aimed to investigate the digital divide by determining the influence of sociodemographic variables on digital technology usage among 476 Malaysian older adults with CF. Overall, the majority of our robust older adults were using digital technology during the COVID-19 pandemic which is higher than CF participants. Similarly, recent research indicates that more than 70% of older adults were utilising digital technology every day.19,31,32 ICT devices and applications engage people of all ages in experiencing a healthier, safer and enjoyable life.33,34 Evidence on the usage of Internet among the older population during pandemic is still limited. 35 Yet, previous literature indicated that the older population was increasingly implementing digital technology in recent years. 36 The digital divide among older people with CF has appeared as an issue in today's technologically advanced society as they might experience challenges to access and use digital technology. People with cognitive impairment might have difficulty learning new things and perceive digital technology as complex devices. 37 A recent study showed that other obstacles that might influence them to adopt digital technology were financial constraints, lack of vision, limited interest and knowledge. 38
Further analysis also showed a higher likelihood of digital technology use among male of younger age, formal education attainment (more than 6 years), having higher monthly household income and robust (non-CF) participants. In our study, male older adults were likely to implement digital technology in order to keep in touch with the existing relationships compared to female participants. This is congruent with another study where male elders are more likely to utilise digital technology than women depending on their purpose in personal tasks or health-related status.24,39 As expected, younger-age older adults had a higher rate of Internet access and greater Internet skills than older age. 40 In our study, advanced-age older people were less likely to implement digital technology due to hearing or vision impairments and having difficulty using and comprehending current digital technology. This is supported by the latest study that indicated as individuals get older, they are less likely to implement health-related online services such as eHealth literacy, receiving online test results, renewing prescriptions and scheduling appointments.41,42 Widowed elders in this study perceived digital technology as an interactive platform to reduce loneliness, social isolation and enhance social networking. 43 In addition, in our findings, those with higher formal education backgrounds were associated with the usage of digital technology. These older adults might be interested in keeping updated with recent digital technology to interact with their family members and friends. Indeed, education level and previous working experience were associated with the use of information technology among older adults.44,45 However, we found that this evidence contradicted other evidence that reported education level was not linked to digital technology usage, probably due to mediators, for example, an individual's experience and skills in using digital technology. 46 Our study showed that digital technology had become an alternative platform for interacting with people, including older people. Some older adults owned their digital technology devices owing to children bought them and taught them how to use them.
Our findings demonstrated that the most familiar devices among older adults were the smartphone, followed by laptop or computer and tablets. This is parallel to previous findings that showed that older adults were likely to integrate smartphones into their daily life.47,48 Smartphones were the most preferred as they might be perceived as feasible and enjoyable and include multiple features such as Internet access, mobile telecommunications, sensors, location, notifications and the ability to install applications. 49 Cognitive aid features, for example, alarms, calendars, reminders and navigation aids, encourage older adults to use digital technology.50–52 During the COVID-19 pandemic, smartphone usage was increasing as a supportive tool to improve their quality of life, emotion, wellness and communication needs.53–55 This is supported by a recent study indicating a surge increase in using digital technology with Internet for communication purposes that include voice or video calls and engagement with government services but remarkably lessened in searching health-related information during the COVID-19 pandemic. 56 However, the digital divide limits social engagement and increases social isolation among CF older people. Cognitive impairments reduce their capability for online communication and participation with family and friends as they might experience problems in navigating social platforms, interacting effectively and adapting to the latest evolving technologies. Consequently, this may lead to a reduction in quality of life.
In addition, our data indicated that older people with CF was less likely to play games on their phone compared to robust older adults. A probable reason for this could be people with cognitive impairment were comfortable with less complex digital technology. 57 Older people are likely to play games when the technology device is user-friendly, easy to use and suitable for the needs of older demographics. 58 The design of online games must include interactive video games that involve visual and auditory cues.59,60 Research stated that game intervention could delay cognitive decline among advanced-age people, and their compliance with activity could be improved as long as they were willing to participate and enjoy the activities. 61 Cognitive training games can potentially improve global cognitive abilities among older people with cognitive impairment.62,63
Our evidence also align with other research suggesting socioeconomic status was an independent predictor of using digital technology with the Internet for health purposes.64,65 Yet, globally, poverty could lead to a digital divide especially among older people which tend to be less likely to use Internet compared to younger people, and those who have access to the Internet are still low in number. 66 In tandem with the household arrangement aspect, these factors need to be more carefully considered in relation to cultural diversity particularly in terms of digital technology usage such as contact and communication. In developing countries, the gap in digital technology usage across the countries was different. 45 Low Internet accessibility and use of digital technology were associated with income status due to limited exposure to technology devices, financial problems obtaining devices, disabilities and related illnesses that restrict utilisation. 67 Nevertheless, we observed that there is no significant mean difference between urban and rural. This could be due to the migration of individuals from urban to rural after retirement.
In order to fill the gap in the digital divide among CF older adults, it is imperative to design personalised interventions and implement supportive policies. Technological interventions should comprehend improving usability, incorporating interactive design features and providing personalised support from family or peers to overcome cognitive challenges. Training session to enhance digital literacy in targeted individuals could enhance their adoption and navigation toward digital platforms more efficiently. Besides, collaboration from multiple stakeholders such as professional healthcare providers, systems developers and the community is vital to ensure holistic support for this population as well as during the development and testing phase.
The strength of this study was that researchers could address the digital divide's current gap in the health context which is essential to develop telehealth, telemedicine, eHealth or mHealth systems. On the other hand, the limitation of this research was that researchers could not reach individuals from the upper socioeconomic status as they were reluctant to join the collection due to the pandemic. Future studies may explore digital technology usage among older adults with CF longitudinally over the years. The association between digital technology use and health purposes such as telehealth, telerehabilitation, mobile health and eHealth among older adults with CF still need to be studied. It could be beneficial to imply qualitative or mixed-methods design to obtain a deeper understanding of these issues in this population. Next, since this research was conducted during the COVID-19 pandemic, researchers were required to limit physical meetings and practice social distancing. Thus, the pilot-tested questionnaire used needs to be brief but comprehensive.
Conclusion
In summary, older adults with CF integrate digital technology lesser compared to robust older adults into their daily function life mainly smartphones, tablets, computers or laptops in order to stay connected with their surroundings and update online news through WhatsApp social media and are less likely use their devices for game purposes. Male, younger individuals, who obtained formal education level and higher monthly household income status, and robust (non-CF) participants were the predictors of using digital technology. A better understanding of the implementation of digital technology may assist in direct future digital interventions aimed at enhancing cognitive function and quality of life especially in lower-middle socioeconomic countries. Adopting digital technology among older adults, especially with CF, requires collaboration from multiple stakeholders, including professional healthcare providers, caregivers and peers because they may be intimately engaged with patient's health care. We could enhance their well-being and fair participation in the digital era by bridging the digital divide.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231207594 - Supplemental material for Digital technology usage among older adults with cognitive frailty: A survey during COVID-19 pandemic
Supplemental material, sj-docx-1-dhj-10.1177_20552076231207594 for Digital technology usage among older adults with cognitive frailty: A survey during COVID-19 pandemic by Nurul Hidayah Md Fadzil, Suzana Shahar, Devinder Kaur Ajit Singh, Roslee Rajikan, Divya Vanoh, Nazlena Mohamad Ali and Shahrul Azman Mohd Noah in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank all researchers, participants and others who were involved directly or indirectly during data collection and reviewed this manuscript.
Contributorship
All authors made substantial contributions to the study design. NHMF was responsible for the data analysis and writing of the original draft of the manuscript. SS, DKAS, RR, DV, NMA and SAMN were involved in the supervision of the study and writing—review and editing of the manuscript. SS and DKAS contributed to the data interpretation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research is funded by the Ministry of Higher Education of Malaysia under the Long Term Research Grant Scheme (LRGS) (LRGS/1/2019/UM-UKM/1/4).
Ethical approval
This research is approved by Medical Research Ethics Committee of the National University of Malaysia (UKM/PPI/111/8/JEP-2020-34).
Guarantor
SS will serve as the Guarantor for the described research activities.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.