
Abstract
Background
Cognitive decline significantly affects the functional and intrinsic capacities of older adults, highlighting the need for effective interventions. Evidence suggests that mentally stimulating activities, particularly those supported by digital technologies, can promote cognitive health and quality of life in aging populations.
Objective
This pilot trial examined the feasibility and preliminary effectiveness of GameAAL, a multidomain Cognitive Training programme delivered via tablet and television, in older adults with cognitive impairment or dementia.
Methods
The intervention targeted key cognitive domains including attention, reaction time, memory, language, and executive functioning. Forty-one older adults (aged 60–93), living in nursing homes, participated in a 6-month programme. The tablet intervention group (n = 10) completed 30 sessions using a tablet device, while the TV intervention group (n = 31) completed nine sessions using a TV interface. All participants engaged with six serious games designed around cognitive tasks related to activities of daily living.
Results
Pre- and post-intervention assessments included the Montreal Cognitive Assessment (MoCA) and the Hospital Anxiety and Depression Scale (HADS). The Tablet group showed a trend towards improved MoCA scores following the intervention, whereas the TV group did not show significant changes. At the post-intervention, the Tablet group demonstrated significantly better cognitive performance compared to the TV group (p = 0.044). No significant between-group differences were observed in HADS scores.
Conclusion
The findings suggest that the GameAAL Cognitive Training programme may help improve cognitive function in older adults with cognitive impairment by combining computer-based exercises with ecologically valid tasks.
The rapid aging of the global population and its consequences are a growing concern. According to projections by the World Health Organization, 1 the proportion of people aged over 60 is expected to nearly double between 2015 and 2050, reaching approximately 22% of the world’s population, or around two billion individuals. Coupled with increasing life expectancy, this trend highlights the rising prevalence of neurodegenerative dementias, particularly Alzheimer's disease and related disorders. 2 The growing burden of dementia poses significant social and economic challenges for healthcare systems, care providers, and families, with notable disparities in access to care and resources among older adults. 3 Beyond dementia, diabetes, falls, and depression are also major causes of disability in this population. 1
Cognitive decline reduces the intrinsic capacity of older adults and is associated with higher risks of functional impairment and mortality. 4 Although physiological and structural changes are inherent to aging, research indicates that regular participation in physical exercise and mentally stimulating activities, such as reading, puzzles, and social engagement, is linked to better cognitive performance, greater functional independence, improved emotional well-being, and reduced mortality risk.5,6 While healthy aging involves preserving functional capacity and adapting to psychological, physical, and social changes, age-related cognitive decline is often associated with reduced in activities of daily living and overall functional ability.7–9 Recent studies emphasize that advancements in cognitive interventions, particularly those supported by digital technologies, can enhance cognitive functioning 10 and positively influence quality of life and well-being in older adults. 11
Cognitive training for the elderly delivered through information and communication technology
Cognitive interventions for older adults, with or without cognitive impairment, encompass seven main approaches: Compensatory Cognitive Training, Cognitive Stimulation, Enrichment, Cognitive Rehabilitation, Cognitive Training, and Cognitive Remediation and Brain Training. 12 Although grounded in distinct theoretical models, these methods share the goal of preventing cognitive decline, sustaining cognitive abilities, or enhancing specific domains, 13 and can be delivered via traditional or digital formats. In our previous review, we use the term computerized cognitive training (CCT) to refer to structured, goal-oriented cognitive exercises delivered through digital platforms. This construct encompasses interventions described in the literature ICT-based cognitive programmes, digital brain training tools, or technology-supported enrichment activities, provided they involve targeted practice of specific cognitive functions.
In this study, we employed a multidomain CCT programme targeting language, memory, attention, and executive functioning in older adults with cognitive impairment or dementia. The programme integrated guided practice, repetitive training, and individualized feedback to support skill acquisition and monitor progress.10,14–22 Evidence from recent meta-analyses indicates that technology-based interventions can yield improvements in global cognition, attention, processing speed, executive function, immediate recall, and working memory, with stronger effects in individuals with cognitive impairment and when programmes include structured tasks, professional supervision, and extended training schedules (exceeding 24 sessions of at least 30 min each). 23 Collectively, findings suggest that multidomain, supervised, and adequately dosed cognitive programmes tend to produce the most robust effects.
Prior research using CCT in older adults with mild cognitive impairment (MCI) has reported gains in verbal learning and memory24,25 processing speed and attention, 26 and working memory, functional outcomes, and subjective memory perception. 27 Additional trials have shown improvements in attention, working memory, verbal fluency, and cognitive flexibility among individuals with MCI or mild dementia, 28 as well as moderate gains in global cognition maintained over 6 months in older adults at risk of dementia. 29 Meta-analytic evidence further supports enhancements in memory domains, particularly when training is supervised, 30 and highlights the importance of frequency and duration for optimal effects. 31 Despite promising results, long-term follow-up studies remain needed to determine sustainability and refine implementations for clinical settings.
Evidence from cognitively healthy older adults also supports structured CCT. The Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE) trials remain the most influential in this field, examining multi-session programmes delivered to community-dwelling older adults over 5–6 weeks, typically comprising 10 training sessions focused on memory, processing speed, and reasoning.32–37 Some protocols included booster sessions.33,35–37 These interventions consistently produced domain-specific improvements, with reasoning and processing speed gains observed across cohorts32,33 and comparable benefits from memory-focused training.34,35,37 Effects were maintained for up to 5 years, 37 and some outcomes, including preserved IADL (instrumental activities of daily living) functioning, remained detectable 10 years later. 36 Booster training strengthened long-term maintenance, particularly for reasoning and processing speed.35,36 Additionally, long-term analyses linking ACTIVE data with mortality records indicated that higher baseline cognitive scores were associated with reduced mortality risk over a 20-year follow-up period, whereas the type of cognitive training received did not significantly influence survival outcomes. 38 The subsequent study from Chen and colleagues seems to have found results in the same line. 39 Interestingly, another ACTIVE follow-up study showed that participants enrolled in the cognitive training had a low risk for Alzheimer's disease and other related dementias associated to higher health care and education access indicators, over a 20-year follow-up period. 40 Furthermore, the follow-up study of Zahodne et al. 41 raised the attention to the role of perceived control. Although no moderation effects were found between intervention group and time to diagnosis, participants with greater levels of perceived control at baseline, evidenced lower dementias incidence.
Online-delivered programmes have yielded similar cognitive benefits. Gigler et al. 42 reported enhanced working memory and processing speed following a ten-week, 17-session programme in adults with and without MCI. Similarly, Vermeij et al. 43 observed improvements in digit and spatial span after a 5-week, 25-session intervention, with gains sustained at 3 months and modest enhancements in figural fluency.
Multidomain interventions, including CCT, have also demonstrated positive outcomes in dementia populations, with improvements reported in global cognition,44–46 physical functioning, 44 mood, 46 IADL performance, and reductions in anxiety and depressive symptoms.44,46
Tablet-based programmes represent another accessible delivery modality. Saluvich et al. 47 found improvements in episodic memory, potential gains in visuospatial ability, and increased motivation and memory confidence in individuals with a-MCI after an eight-session intervention. Shamir et al. 48 similarly reported reduced cognitive complaints following five group-based tablet sessions in older adults with MCI. Positive effects have also been observed in cognitively healthy older adults, including improved episodic memory, processing speed,49,50 and attentional control. 51 Finally, Fong and colleagues 52 also found favourable results with a 5-month CCT in a group with and without risk of MCI, prolonged even after a 3-month follow-up period.
Recent systematic reviews and meta-analyses reinforce the potential of ICT-based cognitive interventions for individuals with MCI or early dementia. Chae and Lee 53 reported cognitive improvements, reduced depressive symptoms, and enhanced quality of life, particularly in programmes lasting at least 6 weeks, with sessions longer than 30 min and multidomain content. Jung et al. 54 similarly observed statistically significant, albeit modest, cognitive gains with ICT-based interventions in MCI populations.
Although research on television-based Cognitive Training in older adults remains limited, findings from two randomized controlled trials (RCTs) are promising. Shatil et al. 55 evaluated an interactive TV programme in 119 cognitively healthy older adults and found significant gains in working memory and executive function. Similarly, Nouchi et al. 56 tested TV-based Cognitive Training games designed to enhance driving-related skills in 55 older drivers; over 6 weeks, adaptive training led to superior improvements in driving performance, processing speed, and inhibitory control, compared with non-adaptive games. These findings indicate that interactive TV platforms may provide an accessible and effective alternative for older adults, particularly those with limited computer access.
A summary of the main intervention characteristics, study populations, delivery modalities, and cognitive outcomes is provided in Table 1 to facilitate synthesis of the reviewed evidence.
Summary of studies on cognitive training interventions, including interventions, study populations, delivery modality, and cognitive outcomes.

Note: MCI: Mild Cognitive Impairment; CCT: Computerized Cognitive Training; IADL: Instrumental Activities of Daily Living; Online-BCP: Online-Based Cognitive Programmes; a-MCI: Amnestic Mild Cognitive Impairment; TV-BCT: TV-Based Cognitive Training.
A pilot trial was conducted to evaluate the feasibility and preliminary effectiveness of the ‘GameAAL—Gamification Supporting Active and Assisted Living’ programme, a tablet and TV-Based Cognitive Training intervention targeting attention, reaction time, memory, language and executive functioning, which incorporate ecological tasks to promote the transfer to participants’ everyday life.
To date, studies are still scarce in examining the application of two simultaneous types of intervention, tablet and TV-Based Cognitive Training, in older adults with cognitive impairment or dementia, and reflect their performance in parallel based on the same interface, from the Neurohab platform, 57 previously tested in a pilot study with a population of heterogeneous cognitive impairment and dementia, using the tablet modality. 58 This software platform provides several features, including real-time feedback and personalized learning (for more details see 57 ). This underscore the importance of this pilot study for assessing feasibility, adherence, user-friendliness, the level of acceptance and attendance in this population and, ultimately, the potential cognitive benefits from these paralleled interventions (tablet and TV modalities), before progressing to a definitive trial, serving as a final proof of concept. We hypothesized that participation in this intervention would result in improvements in overall cognitive functioning.
Method
Participants
A convenience sample was recruited through contact with nursing homes in the Coimbra district. Three institutions were selected, whose residents presented varying levels of cognitive impairment. The study was approved by the Ethics Committee of the Faculty of Medicine of the University of Coimbra (CE-077/2018), and written informed consent was obtained from all participants or their legal representatives. All procedures were conducted in accordance with the Declaration of Helsinki.
Eligibility criteria were verified, and informed consent was obtained from all participants or their legal representatives (see Figure 1). This pilot study was initially designed as a parallel-group RCT with a 1:1 allocation ratio. However, practical constraints during implementation meant that a true randomization procedure could not be applied. Consequently, participants were allocated manually in the order of their enrollment and according to their availability for scheduled sessions. The allocation was carried out by administrative staff who were not involved in participant assessment or data handling, and no demographic, clinical, or cognitive information was used in the assignment process. Participants were allocated based on predefined inclusion and exclusion criteria, namely: Inclusion criteria: (1) age 60 years or older; (2) ability to remain on task; (3) evidence of cognitive impairment or dementia; (4) no diagnosis of a psychopathological disorder; and (5) motivation to participate in the Cognitive Training programme; Exclusion criteria: (1) severe neurological disorders; (2) alcohol and/or drugs abuse; and (3) reduced insight. The final sample comprised 41 participants.

Study procedure.
Outcome measures
The evaluation protocol included two standardized assessment tools designed to measure global cognitive functioning and symptoms of anxiety and depression. An anamnesis interview was also conducted to collect sociodemographic and clinical data. The selection of instruments was based on several criteria: representativeness, relevance of the constructs measured, cultural and linguistic adaptation for the Portuguese population, empirical validation, and the availability of normative data. Together, these measures enabled a comprehensive characterization of the sample in sociodemographic and clinical terms, and provided an objective evaluation of the participants’ neuropsychological functioning. This approach allowed for the quantification of both impairments and preserved abilities across cognitive domains, distinguishing normal aging processes from potential neuropsychopathological conditions.
Sociodemographic Questionnaire: as part of the anamnesis, personal information, health status, and clinical history were collected to characterize the sample. Hospital Anxiety and Depression Scale (HADS59,60: symptoms of anxiety and depression were assessed using the validated Portuguese version of the HADS. This self-report instrument is widely used in clinical and research settings to screen for emotional distress. Given that the sample consisted primarily of older adults, the HADS items were administered verbally by trained the assessors to ensure participants full comprehension, particularly among those with potential literacy or visual difficulties. The original authors note that individuals with limited literacy may experience embarrassment when completing self-report questionnaires
61
; this consideration informed the decision to adopt a standardized verbal administration procedure in the present study. To minimize interviewer bias, all assessors followed a standardized administration protocol, reading each item verbatim in a neutral pace and tone, without paraphrasing, providing explanations, or emphasizing any response options. Montreal Cognitive Assessment (MoCA62,63: the MoCA is a brief cognitive screening tool used to differentiate between age-related cognitive changes and those associated with pathological conditions. It has been extensively validated in the Portuguese population. The MoCA evaluates eight cognitive domains: executive functions, visuospatial abilities, short-term memory, language, attention, concentration and working memory, and temporal and spatial orientation.54–68 The maximum score is 30 points, with normative data stratified by age and educational level.
68
Outcome assessors were not blinded to group allocation because they also provided support during the intervention sessions. To minimize possible assessment bias, all evaluations were conducted using standardized administration procedures.
Procedure
This study comprised three phases: pre-intervention, intervention, and post-intervention, as summarized in Figure 2.

Study phases.
Pre-intervention
The first phase consisted of a single neuropsychological assessment session conducted individually with each participant. These evaluations were administered on-site by clinical psychologists experienced in neuropsychological assessment. In line with the established protocol, the purpose of this session was to characterize participants’ baseline cognitive and emotional functioning, enabling later comparison with post-intervention outcomes. The duration of each session varied depending on individual performance, but on average the full protocol required approximately 30 min to complete.
Intervention phase
The intervention sessions consisted of multidomain Cognitive Training activities (see Table 2). Neuropsychologists were responsible for designing the exercises and conducting the sessions, including those delivered via TV. The programme was developed to stimulate several cognitive domains: some tasks targeted a specific cognitive function, while others required the simultaneous engagement of multiple low-level processes. Training focused on four core domains: (i) memory; (ii) attention; (iii) language; and (iv) executive functions (see Table 2).
Cognitive functions trained and description of the serious games.

Note: The shaded cells means that the specific serious game is responsible to train the correspondent cognitive function.
To maintain an appropriate level of challenge and prevent boredom, frustration, or demotivation, the exercises were adapted to each participant’s cognitive abilities by adjusting task parameters (e.g. speed, number of stimuli). This adaptive feature enables personalized learning tailored to individual needs.
The content of the activities was linked to participants’ interests, incorporating elements such as crosswords, common Portuguese proverbs, and tasks connected to daily life. The application design also integrated features highlighted in the literature as essential for older adults: (i) sensitivity to slower response times and reduced sensory acuity (e.g. large fonts, large buttons, and clear stimuli); (ii) multiple levels of difficulty and categories; (iii) real-time performance feedback; (iv) visual and auditory reinforcement; (v) participant awareness of the training’s relevance; and (vi) the absence of time limits.69–75 These features were embedded in the training interface used in this study.
To promote the transfer to everyday life, several exercises were ecological in nature, requiring participants to solve tasks resembling real-life situations. The Cognitive Training included a variety of serious games designed to stimulate different cognitive processes: (i) Puzzle, (ii) Maze, (iii) Quiz, (iv) Reaction Games, (v) Whack-a-Mole, (vi) Pairs, and (vii) Word, Symbol and Number Search, as detailed in Appendix 1. Some of these tasks had been described previously in a study by Simões et al. 58
The tablet-based intervention sessions were held three times per week using tablet devices. The technology was selected for its high interactivity and motivational potential, which facilitate adaptation and engagement among older adults. Its portability also allows for greater flexibility, as tablets are not dependent on external equipment or fixed locations. Sessions were conducted within each nursing home, lasted approximately 40 min, and extended over 6 months, totaling 30 sessions per participant, consistent with the findings of Chen et al. 23 All sessions were conducted by neuropsychologists, whose primary role was to support participants during the activities, monitor performance, and provide feedback. They also offered motivational support and ensured participants remained engaged throughout the tasks. Attendance, completion rates, and in-app activity data were automatically recorded by the platform, allowing objective monitoring of adherence and engagement over the course of the intervention.
The TV group participated in weekly sessions of the multidomain Cognitive Training programme, following the same principles as the Tablet group. All sessions were held in the three nursing homes, lasted approximately 20 min, and spanned six months, totaling nine sessions per participants. The sessions were delivered via a Smart TV using an Android-based interface from the Neurohab platform. 57 The system was organized around three core modules: (1) tasks simulating activities of daily living, (2) monitoring of health parameters, and (3) neurocognitive training delivered exclusively through serious games. The Cognitive Training module included the same games used in the Tablet group, also used in the intervention with the Tablet group: (i) Puzzle, (ii) Maze, (iii) Quiz, (iv) Reaction Games, (v) Whack-a-Mole, (vi) Pairs, and (vii) Word, Symbol and Number Search.
The modules operate in an interconnected and interdependent manner, integrating data collected from biosensors and environmental sensors (e.g. motion detectors), to programme the training sessions and select the targeted cognitive domains. All sessions were supervised by biomedical professionals with specialized training in the area. Their primary role was to support participants during the activities, oversee task execution, provide feedback, and offer motivational reinforcement when required.
Data collected through the interface were processed by an external unit installed remotely, enabling continuous monitoring of task performance. The system generated activity patterns, identified deviations, and allowed for the personalized planning and adjustment of each session. In addition, algorithms incorporated into the system were capable of generating real-time alerts within the local unit. Session attendance, duration, and completion were automatically logged by the platform, allowing objective monitoring of adherence and engagement throughout the intervention.
To further enhance engagement, the platform was designed to promote positive reinforcement in collaboration with caregivers and institutional staff. Participants’ achievements and progress were rewarded with meaningful and enjoyable experiences, including cultural and leisure activities tailored to their preferences.
Post-intervention
All participants completed the final phase, which consisted of a post-intervention neuropsychological assessment session. This session followed the same structure and procedures as the pre-intervention phase, ensuring consistency in data collection.
The purpose of this phase was to determine magnitude of the intervention’s effects through objective outcome measures, allowing direct comparison with the participants’ pre-intervention performance.
Statistical analysis
All statistical analyses were conducted using IBM SPSS, Version 23. As some variables did not meet the normality assumption (Shapiro–Wilk test), both parametric and non-parametric tests were initially computed. The results were consistent across methods; therefore, for clarity and interpretability, only parametric test results are reported in the main text. This decision is supported by methodological recommendations, 76 which emphasize the robustness of parametric tests and the interpretability of mean-based outcomes.
MoCA scores were used to assess cognitive functioning at both pre- and post-intervention timepoints. Means and standard deviations were calculated, and score changes were examined by comparing timepoint 2 (post-intervention) with timepoint 1 (pre-intervention) within each intervention group using paired-samples t tests. Ninety-five percent confidence intervals were computed for the mean difference, and Cohen's d was calculated as the effect size.
To evaluate group differences in MoCA scores at both timepoints, independent-samples t tests were conducted to compare the Tablet and TV groups at pre- and post-intervention. Hedges’ g was reported as the effect size to account for unequal sample sizes. When appropriate, a mixed-design ANOVA was performed to examine the interaction between timepoint and group, with eta squared η2 reported as the corresponding effect size.
Pearson correlation coefficients was computed to explore the relationship between MoCA scores and HADS depression and anxiety scores. In addition, independent-samples t test was used to compare the Tablet and TV groups on their HADS depression and anxiety scores.
Results
Recruitment of participants
A total of 48 older adults, who expressed clear interest in participating, were initially recruited to take part in a Cognitive Training programme delivered via tablet and TV interfaces. As this was a pilot study, the sample size was determined by practical considerations, including available resources, timeframe, and recruitment feasibility across sites. The primary aim was to evaluate the feasibility and acceptability of the study procedures rather than to test efficacy. During the intervention phase, five participants dropped out: three withdrew voluntarily, and two passed away. The final sample consisted of 41 participants (10 males and 31 females), aged between 60 and 93 years. Regarding educational background, six participants lacked reading and writing skills but had attended elementary school; 17 had not completed basic education; another 17 completed the first cycle of basic education; and one participant completed the second cycle. The sampling flowchart is presented in Figure 3.

Flowchart of the non-randomized pilot trial.
Intervention effects
Pre- (T1) and post-intervention (T2) assessment using the Montreal Cognitive Assessment (MoCA), along with the mean differences between timepoints, are reported in Tables 3 and 4 for the Tablet and TV groups, respectively.
Differences between MoCA pre- (T1) and post-intervention (T2) results for the Tablet group (n = 10).

Note: M: mean; SD: standard deviation; CI: confidence interval; d: effect size.
Differences between MoCA pre- (T1) and post-intervention (T2) results for the TV group (n = 31).

Note: M: mean; SD: standard deviation; CI: confidence interval; * Significant results (p < 0.05); d: effect size.
Following the tablet-based intervention, improvements were noted across all MoCA subdomains, particularly in language and attention. However, these changes did not reach statistical significance (all p > 0.05).
In contrast, participants in the TV-based intervention group demonstrated negative variations in the attention, language, abstraction and orientation subdomains, resulting in an overall decline in the MoCA total scores. Statistically significant pre-post differences were detected in two domains: visuospatial/executive, which improved post-intervention (p < 0.001), and language, which demonstrated a decline (p = 0.018) in performance following the intervention.
When comparing MoCA total scores between groups, significant differences emerged only at the post-intervention assessment (p = 0.044, g = 1.11), with the Tablet group outperforming the TV group, suggesting a positive effect of the tablet-based intervention. No significant group differences were found at the baseline (p = 0.102, g = 0.61). The effect of the timepoint × group interaction was statistically significant, F(1, 39) = 5.84, p = 0.020, η2 = 0.13, indicating that MoCA total scores improved from T1 to T2 exclusively in the Tablet group (see Figure 4).
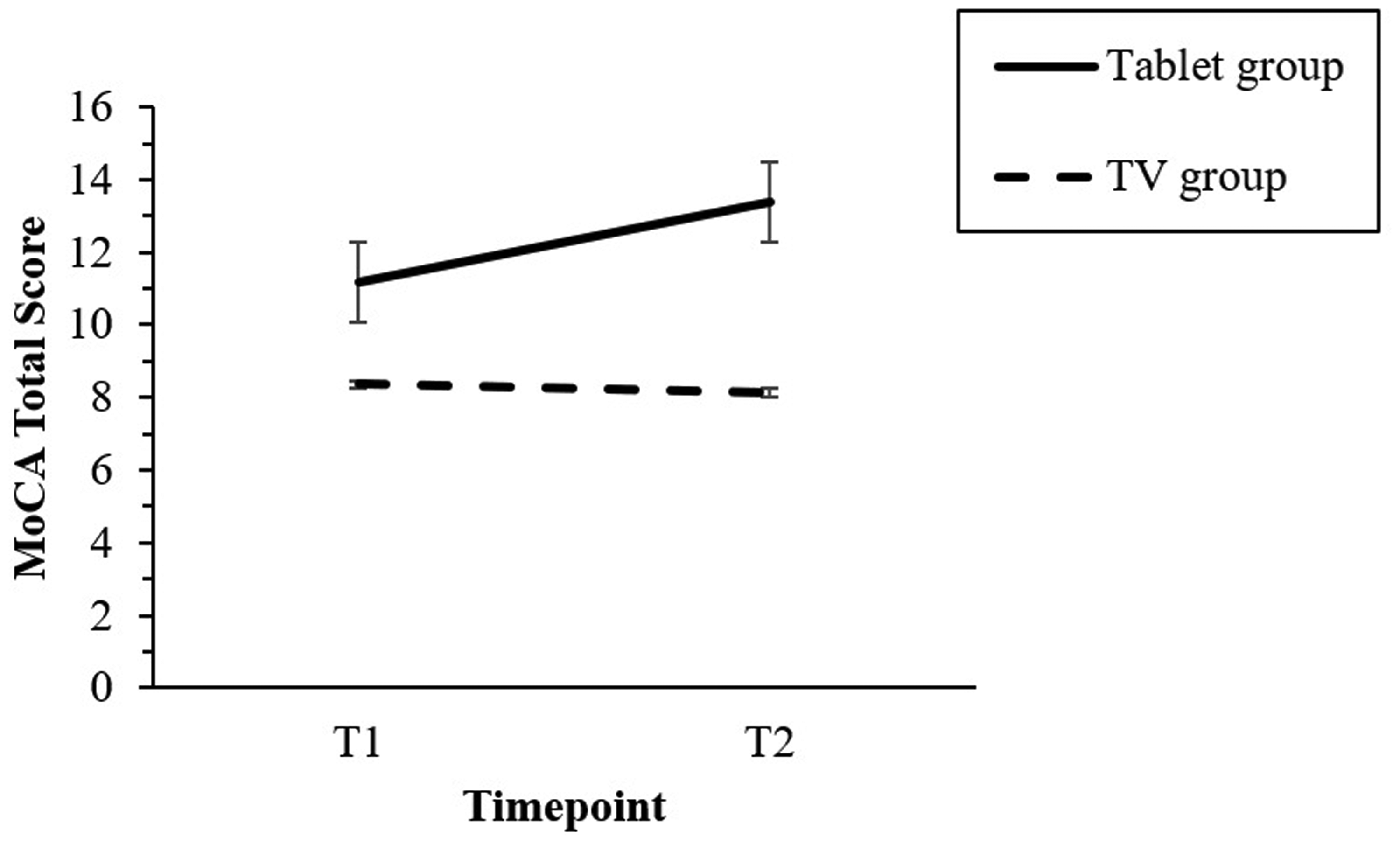
Timepoint by group interaction effect on MoCA total score. Only Tablet group revealed a superior performance after the intervention, comparing to the baseline point.
Anxiety and depression levels, assessed with the HADS at both timepoint, were examined to ensure that no significant variations could have confounded the observed cognitive outcomes. No significant differences were found between the Tablet and TV groups for anxiety (p = 0.420, g = 0.30 and p = 0.991, g = 0.00, at pre- and post-intervention, respectively) or depression (p = 0.131, g = 0.56 and p = 0.344, g = 0.35, at pre- and post-intervention, respectively), thus minimizing the likelihood of their influence on MoCA scores improvements. Additionally, no significant correlations were detected between anxiety or depression scores and MoCA scores, at both timepoints (all r < 0.22, p > 0.05).
Discussion
The primary aim of this study was to evaluate the effectiveness of the GameAAL Cognitive Training programme, delivered via tablet, in strengthening multiple cognitive domains, including attention, reaction time, memory, language, and executive functioning, compared with a TV-Based Cognitive Training format.
Following the intervention, participants in the Tablet group demonstrated improvements across all assessed cognitive domains, with the largest gains in language and attention. Although these improvements did not reach statistically significance, the direction of these effects aligns with findings reported by Shamir et al. 48 By contrast, the TV group exhibited negative variations between pre- and the post-test MoCA scores in several domains, excluding naming, delayed recall, and visuospatial abilities, with the latter showing statistical significance. The only significant improvement in this group was observed in the visuospatial/executive domain between timepoints; while language performance significantly declines. These results are consistent with those of Shatil et al., 55 who also observed significant improvements in executive functioning following TV-Based Cognitive Training. Importantly, when comparing groups, the Tablet condition yielded statistically significant MoCA total scores at post-intervention (p = 0.044), suggesting a superior overall effect of the tablet-based intervention.
Several factors may account for these differences. First, the training intensity varied substantially: the Tablet group participated in three 40-min sessions per week, whereas the TV group engaged in a single 20-min session weekly. Greater exposure may have amplified learning opportunities for the Tablet group. Second, motivation and prior familiarity with technology could have influenced outcomes. Many participants in the Tablet group already engaged in cognitively stimulating activities (e.g. crosswords and puzzles) and were comfortable with digital devices. Their enthusiasm for tablet use was evident, and the programme’s individualized features, tailoring tasks to each participant’s skill level and preferences, likely further reinforced engagement. Direct interaction with a therapist, providing immediate feedback and motivational support, was also have enhanced adherence and performance. For a broad comprehension about factors related to compliance with tablet CCT programmes, see this study. 77
Nevertheless, caution is warranted in interpreting these findings. Different training intensity, the participants’ baseline cognitive engagement, the differences in motivation levels, the individualized support provided by the specialists (including the difference in the facilitators’ expertise) and, consequently, the possible Hawthorne effect due to their presence, are some relevant aspects to consider not only as an explanation for the observed superior performance in the Tablet group, but also as a possible confounder to those results. These considerations highlight the need for future studies to systematically control for such variables when comparing different modes of delivery.
Despite these limitations, our findings suggest that sustained and tailored cognitive training may support engagement and functional outcomes in older adults, although further research is needed. We could anticipate that interventions sustained over time and adjusted to individual needs contribute to maintain the benefits, as suggested by previous authors78,79 and further corroborated by evidence from the ACTIVE trials.
The present study is not without limitations. The small sample size, from only three nursing homes within a single district, may have reduced statistical power and limited generalizability of the findings. Some caution is needed, as this population may not fully represent older adults in broader community settings. Another limitation concerns group allocation, which was performed manually rather than through true randomization, potentially introducing selection bias and reducing internal validity. Future research should replicate these findings in larger, blinded RCTs to strengthen evidence and support these findings on a broader scale. The restricted range of outcome measures also represents a limitation. Although the MoCA and HADS are valid and reliable instruments, their focus on global cognition and mood may have overlooked changes in functional performance or quality of life. Including standardized ADL/IADL or other ecologically oriented measures in future studies would provide a more comprehensive understanding of intervention effects. Furthermore, outcome assessors were not blinded to group allocation, which may have introduced assessment bias despite adherence to standardized administration procedures. In addition, the sample excluded healthy older adults and individuals with different dementia profiles, limiting the scope of conclusions. Finally, methodological differences between the two interventions formats (Tablet and TV groups), including variations in session frequency, intensity (e.g., the Tablet group received a more intensive intervention), and engagement, constraint the validity of direct comparisons. Advanced approaches such as meta-regression analyses could provide valuable information, for example, which populations derive the greatest benefit (e.g. people with dementia vs. healthy older adults), which type of Cognitive Training is most effective (e.g. multidomain vs. single-domain), and whether improvements generalize to daily functioning.
Conclusion
In summary, findings from this pilot study suggest that the GameAAL Cognitive Training programme, delivered via tablet, may enhance cognitive functioning in older adults with cognitive impairment or dementia. The platform is relatively low-cost, widely accessible, and potentially scalable, offering promise not only as a preventive tool against age-related cognitive decline in healthy populations but also as a supportive intervention to preserve cognitive abilities in those already experiencing cognitive deterioration.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076261417771 - Supplemental material for Remote cognitive training for older adults using tablets: A pilot trial
Supplemental material, sj-pdf-1-dhj-10.1177_20552076261417771 for Remote cognitive training for older adults using tablets: A pilot trial by Liliana Mendes, Joana Oliveira, Marco Simões, Marta Pinto and Miguel Castelo-Branco in DIGITAL HEALTH
Supplemental Material
sj-doc-2-dhj-10.1177_20552076261417771 - Supplemental material for Remote cognitive training for older adults using tablets: A pilot trial
Supplemental material, sj-doc-2-dhj-10.1177_20552076261417771 for Remote cognitive training for older adults using tablets: A pilot trial by Liliana Mendes, Joana Oliveira, Marco Simões, Marta Pinto and Miguel Castelo-Branco in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors thank the team involved in supporting data collection, as well as the senior care institutions in the district of Coimbra that participated in the study. The authors also thank ANAI for the collaboration in the project, in concrete all the participants, as well as our IntelliCare partner.
Ethical approval
Ethical approval was obtained from Ethics Committee of the Faculty of Medicine of the University of Coimbra (CE-077/2018).
Contributorship
Liliana Mendes drafted the original manuscript, designed the intervention and post-intervention phases of the study, and supported data collection, analysis, and organization. Joana Oliveira collaborated during the intervention and post-intervention phases in collecting the data; organized the database with direct collaboration from Liliana Mendes; and wrote sections of the manuscript. Marco Simões contributed to the design and development of the NeuroHab platform used in the study, and provided technical input for its integration within the intervention protocol. Marta Pinto contributed to the conceptualization and design of the GameALL application and provided technical input for its integration within the intervention protocol. Miguel Castelo-Branco contributed to conceptualization, data curation, funding acquisition, project administration, supervision, and writing—review and editing. All authors contributed to manuscript revision and read and approved the submitted version.
Funding
This research was funded by Portugal2020 PO Centro 22/SI/2015 FEDERCompete, Project n° 17948—GAMEAAL, and Compete Project POCI-01-0145-FEDER-007440; Promoter: Intellicare—Intelligent Sensing in Healthcare, Lda; Co-Promoter: IBILI—Instituto de Imagem Biomédica e Ciências da Vida/CIBIT and UID/4950/2025.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Liliana Mendes.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.