
Abstract
Purpose
This study was initiated to examine factors that motivate African American students who use wearable devices at an HBCU in Mississippi.
Method
We conducted a correlational research study on undergraduate and graduate students from a southern USA university. The stratified random sample comprised a total of 239 students. The responses of the students were analyzed using the Fisher exact test to determine whether or not there was a significant association between the categorical demographic variables (age, gender, ethnicity, and student classification) and the students’ motivation for using a wearable device.
Results
Students used wearables for one main reason, to help them increase their awareness of their health status because they understand the importance of tracking their health metrics to boost their health status and reduce risk factors for developing chronic diseases. Students also demonstrated that they understand the value of tracking health information, such as heart rate and blood pressure, as a way to reduce the prevalence and impact of risk factors that can lead to chronic diseases.
Conclusions
Wearables enable individuals to regularly observe, measure, and record their physical status and physiological measures, and facilitate medication adherence by enabling individuals to maintain their prescribed medication regimen adequately. The data collected and stored through these wearables can provide data that will be useful for medical personnel in their treatment of patients and in developing strategies for prevention and intervention for the larger community.
Keywords
Introduction
Wearable technology devices are applications for monitoring and tracking fitness-related metrics such as steps taken, distance traveled, and calories consumed. They can be used as a process for medical surveillance, noninvasive medical care, and mobile health and wellness monitoring. 1 Wearables provide users with access to valuable data that help them stay informed about their health conditions and gain a feeling of control. Wearable technology use has advantages in healthcare to (a) promote proactive healthcare, (b) boost patient engagement, (c) reduce healthcare costs, and (d) decrease staff workload by facilitating communications, reducing personal visits, and optimizing the workload of healthcare professionals. 2 According to Yetisen et al. 3 , wearable devices have the potential to provide real-time data about the health status of users and the information and data they compile can assist healthcare providers in managing the path of chronic diseases. It gives them an additional option as they seek to prescribe effective strategies and treatment. 3 Wearable technology provides us with the ability to monitor our fitness levels and track our physical and emotional well-being, enabling us to better understand ourselves and improve our overall health. Wrist-worn smartwatches and fitness monitors have become widely adopted by consumers and are gaining increased attention from researchers for their potential contribution to the digital measurement of health in a scalable, mobile, and inconspicuous way. 4 In 2007, Bravata et al. supported using pedometers as an effective tool to increase physical activity and improve health. 5 In 2014, Neilsen reported that nearly two-thirds of adults in the United States owned a smartphone 6 that has the capability to track health behaviors such as physical activity and provide convenient feedback. 7
Smarr et al. 8 reported that illness-associated cues can be observed using wearable devices and correlate with actual illness occurrence. This research supports the belief that wearable devices can detect illnesses in people even when no symptoms are present. The authors believe that the use of wearable devices can provide enough physiological data to predict disease onset. Beniczky et al. 9 described wearable devices as useful tools in healthcare applications, where detection and prediction are facilitated using wearable devices. According to Natarajan et al., 10 wearable devices can easily measure health metrics, such as respiration rate, heart rate, and heart rate variability, and can potentially provide early signs of illness. Measuring these metrics, along with regular medical professional diagnostics, may lead to better early detection and monitoring of disease occurrence.
Wearable devices, such as Apple Watch, Fitbit, Samsung, Basis, Mio, PulseOn, and Whoop, are used for tracking activity, sleep, and other health-related outcomes. Wearables can provide a myriad of health-related information, including low heart rate alerts, a personal electrocardiogram (ECG) monitor for detecting arrhythmia, sleep tracking (e.g. sleep architecture), and pulse pressure designed to promote healthy living and alert high-risk consumers based on real-time data. These digital health solutions/devices are increasingly used in research and clinical practice. 11
Mensah 12 surmised that communities are settings where health is supported and protected by healthy social connections and environments, or compromised and impaired by detrimental social, environmental, and policy determinants, as well as adverse behavioral and lifestyle choices. Previous research has shown that African American (AA) communities are at increased risk for cardiovascular and metabolic diseases, including obesity, high blood pressure (BP), diabetes, chronic kidney disease (CKD), myocardial infarction, and stroke. 13 Wearable devices present an innovative strategy to manage many of these chronic health conditions away from the doctor's office. African Americans have a 30% more likelihood to die of cardiovascular diseases, as well as a significantly higher rate of obesity. 14 According to Yingling et al., 15 underlying genetic mechanisms may be responsible for the increased frequency of high BP and kidney disease in African Americans. They believe that the prevalence of cardiovascular disease in African Americans highlights the ongoing challenge of suboptimal adoption of evidence-based practices to promote community health and prevent disease and the continuing prevalence of health disparities. By providing continuous monitoring, wearable devices are a valid option that can facilitate the management of chronic diseases that disproportionately affect African Americans compared to Caucasians.
In Mississippi, social determinants of health are recognized as a major risk factor for the development of chronic disease and are primarily responsible for branding the state of Mississippi and African Americans in Mississippi as the leaders in the prevalence of cardiovascular disease in the United States of America (USA). 16 Many public health officials have been searching for alternative ways to reduce the degree of health disparities in the US and to lift Mississippi's standing from last place in health metrics. 16 Self-management is recognized as a critical component of the strategies to reduce health disparities in Mississippi. There is limited information available and limited understanding about the actual use of wearables and the key factors motivating the use of these devices by African Americans. Since there is little research available about the use of wearable devices among African Americans in Mississippi, this study was initiated to better understand the factors that motivate AA students who use wearable devices at an HBCU in Mississippi to determine the extent to which they use wearables as a health promotion strategy to reduce potential barriers to positive health outcomes.
The following are the four hypotheses that were developed for this study:
Hypothesis one:
Null (H01): There is no association between age and primary motivation for using consumer wearables. They are independent.
Alternative (HA1): A relationship between age and primary motivation for using consumer wearables exists in the population.
Hypothesis two:
Null (H02): There is no association between gender and primary motivation for using consumer wearables. They are independent.
Alternative (HA2): A relationship between gender and primary motivation for using consumer wearables exists in the population.
Hypothesis three:
Null (H03): There is no association between ethnicity and primary motivation for using consumer wearables. They are independent.
Alternative (HA3): A relationship between ethnicity and primary motivation for using consumer wearables exists in the population.
Hypothesis four:
Null (H04): There is no association between student classification and the primary motivation for using consumer wearables. They are independent.
Alternative (HA4): A relationship between student classification and the primary motivation for using consumer wearables exists in the population.
Figure 1 represents the study processes. It includes the study preliminary activities followed by the methodology, data collection, and data analysis. Report of the findings is the final step in the process.
Methods
Ethics approval
Approval to conduct the study was obtained from the Institutional Review Board (IRB) at Jackson State University (protocol 0085–22).
Approach, participant recruitment, and data collection
We conducted a correlational research study that focused on a population of interest consisting of undergraduate and graduate students from a university located in the state of Mississippi, USA. The stratified random sample comprised a total of 239 students. To calculate an adequate sample size for estimating the population prevalence with some degree of precision in making inferences about the population, a power analysis was conducted. The results of the power analysis indicated that a sample size of 239 would be adequate.
We obtained approval to conduct the study from the IRB at Jackson State University and followed all the ethical requirements expected, including signed consent forms before any survey was administered to the students. A 50-question survey was developed to solicit information from college students. Since this study was focused on students’ motivation for using wearable devices, the main outcome variable of interest was one question selected from that survey that asked about the primary motivation for the use of a wearable healthcare device, specifically the students’ primary motivation for using the individual wearable(s) chosen. This motivation was assessed as a four-response question. The four primary motivations were chosen based on the results of research conducted by We’R Sports and Bocas.2,17 These research sources provided information indicating that the primary motivations for using wearable devices observed from their studies were (a) to enhance telephone use, (b) to serve as clothing or other style accessories, (c) to reduce sedentary lifestyle, (d) to track health information such as heart rate or blood pressure, etc. We sought to test the results of these studies using an AA group of students.
On the issue of reliability, we used a single question selected from the initial 50-item survey to define the outcome variable, students’ primary motivation for using wearable devices. In terms of validity, the construct under investigation in this study, the primary motivation to use wearable devices, is sufficiently homogeneous to be adequately operationalized with a single survey question. Previous researchers support the use of a single item for measuring a one-dimensional construct that is well understood.18–21 REDCap software was used to capture the participants’ responses and to create the database. For data analysis, and in order to respond to the hypotheses, we included only the 94 students who provided a response to the question about their primary motivation for using wearable devices. IBM SPSS 28.0 software was used to conduct the analyses.
We used the Fisher exact test (FET) to determine whether or not there was a significant association between the categorical demographic variables (age, gender, ethnicity, and student classification) and the students’ motivation for using a wearable device. FET calculates the number of all possible contingency tables with the same row and column totals (i.e. marginal distributions) as the observed table. Then, it calculates the probability for the p-value by finding the proportion of possible tables that are more extreme than the observed table. Statisticians generally use this test for smaller sample sizes.
The data were recoded and collapsed to make the analyses more meaningful and useful. Collapsing allowed us to combine several selected choices into a single category. Collapsing allowed for new categories to be created that correspond to the original categories/choices. The new categories were coded and then analyzed. The analyses were conducted using only the students who indicated that they were using a wearable device and who provided a response to the question about their motivation for using a wearable device. The FET was used because some of the cells had values that were less than five. FET determines whether a statistically significant association exists between two categorical variables. In this study, we examined if a relationship exists between demographic variables (age, gender, ethnicity, and student classification) and the students’ motivation for using consumer wearables. The FET is displayed in a two-way contingency table, and the analyses computed assessed the contingency tables.
Results
Table 1 is a presentation of the demographic characteristics of the students. Over 55% of the 239 students were in the 18–24-year age group, and 19.2% of them were in the 25–34 age group. About 2.1% of them were over the age of 55 years. The vast majority of them (81.6%) were African Americans. Two-thirds of them (63.6%) were female, and 23.4% of them were male. With regard to classification, the largest groups of students were seniors (27.6%) and masters/doctoral students (25.5%). In the area of academic concentration, the largest group of students (28.9%) comprised students enrolled in the College of Science and Technology. More than half of the students (50.2%) indicated that they were currently using wearables.
Demographic characteristics of students.

This section presents the results of the analyses that were computed to address the hypotheses that were developed.
Null (H01): There is no association between age and primary motivation for using consumer wearables. They are independent.
Alternative (HA1): A relationship between age and primary motivation for using consumer wearables exists in the population.
The data in Tables 2 and 3 present the results of the FET that was computed to examine the relationship between students’ age and their motivation for using a wearable device. Table 2 presents the data for the FET. As seen in Table 3, a significant association was not observed between the students’ age and their motivation for using a wearable device (p = 0.300, FET). The analysis yielded a p-value of 0.300 for the FET, which is greater than our alpha level of 0.05. Our results are not statistically significant. We can accept the null and conclude that no relationship exists between students’ age and their primary motivation for using a wearable device.
Contingency table: age * primary motivation for using a wearable device.

Fisher exact test—age * primary motivation for using a wearable device.
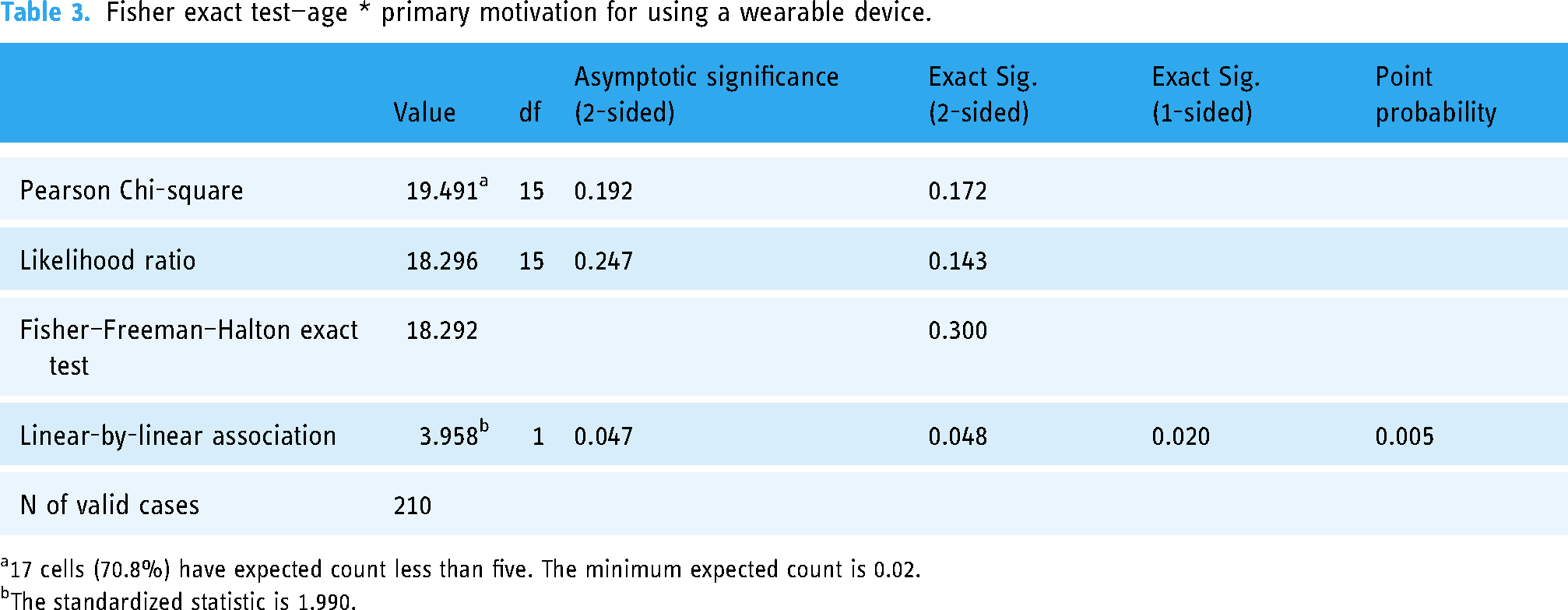
17 cells (70.8%) have expected count less than five. The minimum expected count is 0.02.
The standardized statistic is 1.990.
Null (H02): There is no association between gender and primary motivation for using consumer wearables. They are independent.
Alternative (HA2): A relationship between gender and primary motivation for using consumer wearables exists in the population.
The data in Tables 4 and 5 present the results of the FET that was computed to examine the relationship between students’ gender and their motivation for using a wearable device. The following contingency table (Table 4) presents the data for the FET. As seen in Table 5, a significant association was not observed between the students’ gender and their motivation for using a wearable device (p = 0.109, FET). The analysis yielded a p-value of 0.109 for the FET, which is greater than our alpha level of 0.05. Our results are not statistically significant. We can accept the null and conclude that no relationship exists between students’ gender and their primary motivation for using a wearable device.
Contingency table: gender * primary motivation for using a wearable device.

Fisher exact test—gender * primary motivation for using a wearable device.

Two cells (25.0%) have expected count less than five. The minimum expected count is 0.54.
The standardized statistic is 1.900.
Null (H03): There is no association between ethnicity and primary motivation for using consumer wearables. They are independent.
Alternative (HA3): A relationship between ethnicity and primary motivation for using consumer wearables exists in the population.
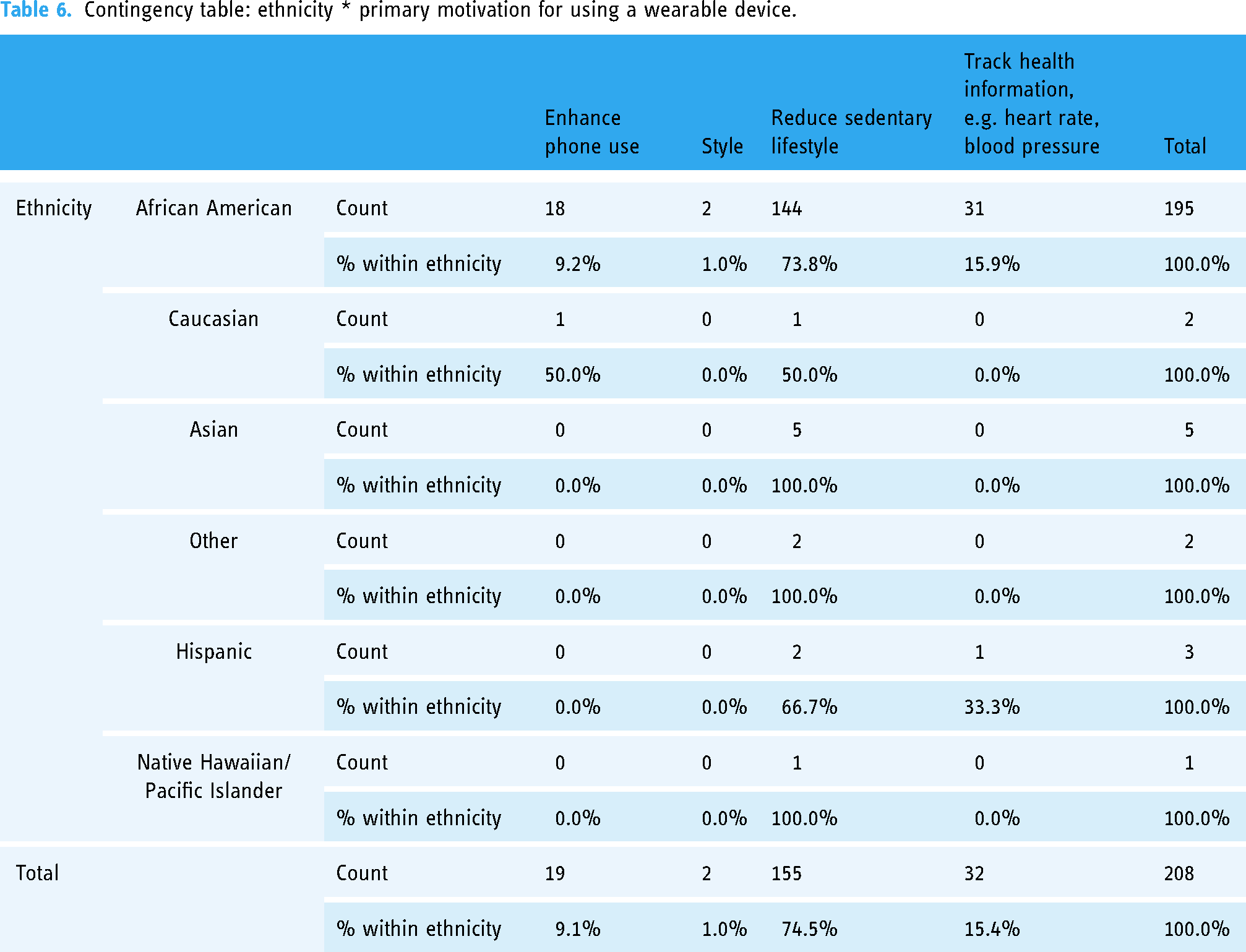
The data in Tables 6 and 7 present the results of the FET that was computed to examine the relationship between students’ ethnicity and their motivation for using a wearable device. Table 6 presents the data for the FET. As seen in Table 7, a significant association was not observed between the students’ ethnicity and their motivation for using a wearable device (p = 0.696, FET). The analysis yielded a p-value of 0.696 for the FET, which is greater than our alpha level of 0.05. Our results are not statistically significant. We can accept the null and conclude that no relationship exists between students’ ethnicity and the students’ primary motivation for using a wearable device.
Contingency table: ethnicity * primary motivation for using a wearable device.
Fisher exact test: ethnicity * primary motivation for using a wearable device.
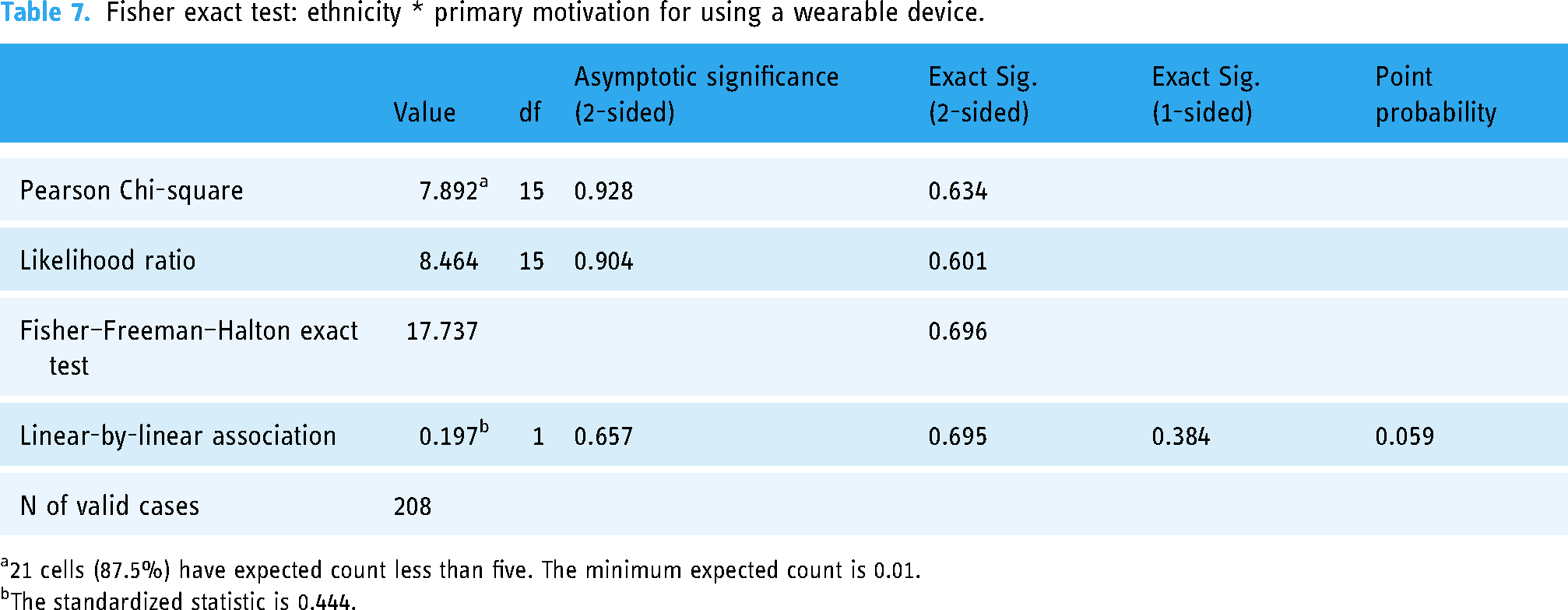
21 cells (87.5%) have expected count less than five. The minimum expected count is 0.01.
The standardized statistic is 0.444.
Null (H04): There is no association between student classification and primary motivation for using consumer wearables. They are independent.
Alternative (HA4): A relationship between student classification and primary motivation for using consumer wearables exists in the population.
The data in Tables 8 and 9 present the results of the FET that was computed to examine the relationship between students’ classification and their motivation for using a wearable device. Table 8 presents the data for the FET. As seen in Table 9, no significant association was established between the students’ classification and their motivation for using a wearable device (p = 0.110, FET). The analysis yielded a p-value of 0.110 for the FET, which is greater than our alpha level of 0.05. Our results are statistically significant. We can accept the null and conclude that no relationship exists between students’ classification and their primary motivation for using a wearable device.
Contingency table: college classification * primary motivation for using a wearable device.

Fisher exact test: college classification * primary motivation for using a wearable device.
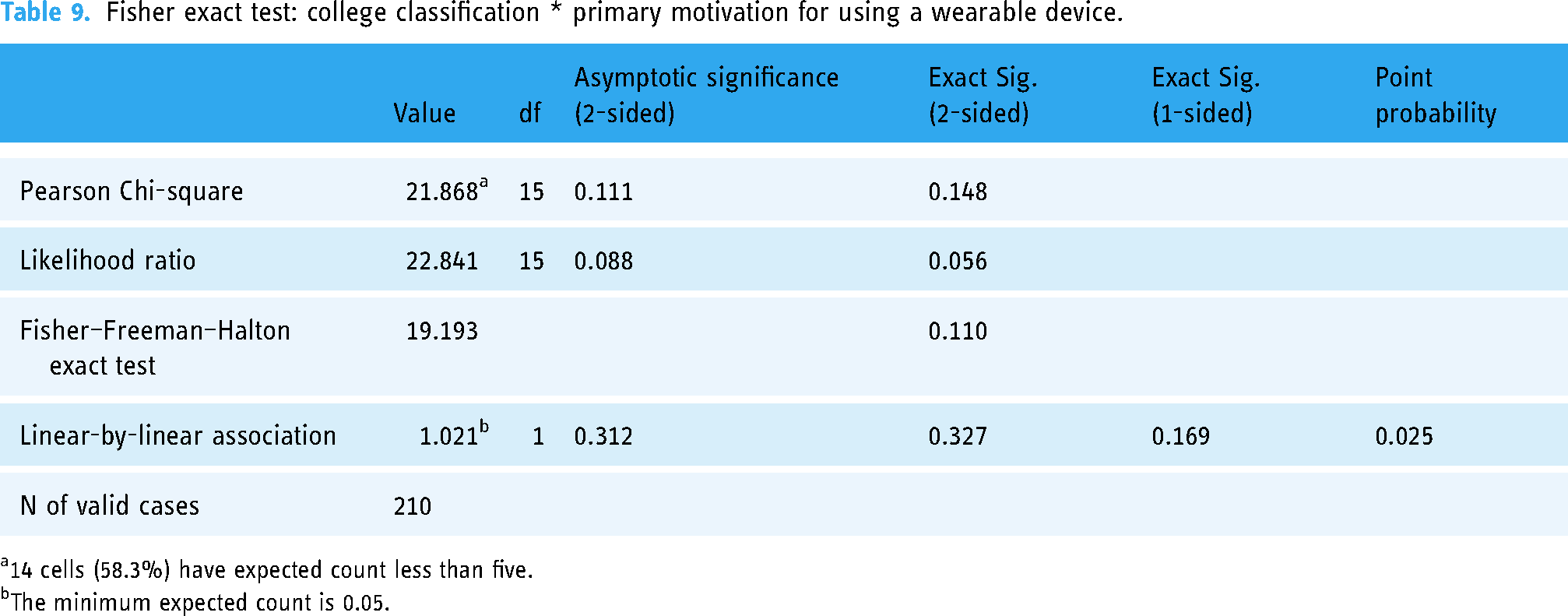
14 cells (58.3%) have expected count less than five.
The minimum expected count is 0.05.
The contingency table (Table 8) indicates the following findings: (a) seniors (22.7%) and sophomores (20.0%) are more likely to use wearable devices to track health information; (b) most of the students indicate that they are more likely to use wearable devices to reduce sedentary lifestyles; (c) sophomores (20.0%) are more likely to use wearable devices for phone use, like texting, messaging, and communication; and (d) juniors (4.3%) are more likely to use wearable devices as a fashion item (for clothing and accessories).
Discussion
Wearable devices are important tools to encourage individuals to improve their health because they make it possible to easily self-monitor risk behaviors and negative health metrics. This study was warranted, especially in the AA population, because, according to Al-Emran et al., 22 there is a scarcity of knowledge about what influences people to adopt wearing these devices. James and Harville 23 believed that most AA men who own a smartphone can be targeted for a variety of programs, services, and health interventions, using mobile devices (mHealth). Grande and Sherman 24 reported conclusions that are in support of the need to conduct this study and other similar studies because they believed that there is a dire need to expand research in this area to reduce the overwhelming burden of chronic illness. This paper expands previous research on the appropriateness of single-item scales.
According to Chandrasekaran et al., 25 about 30% of US adults use wearable healthcare devices, those with some level of college education or college graduates (25.60%), and those with annual household incomes greater than US$75,000 (17.66%) were most likely to report using wearable healthcare devices. As proposed by Al-Emran et al., 22 the evidence from this study can indicate areas where policy-makers can implement practices to promote the use of wearable devices in AA communities.
Though there was no significant association detected in viewing all the demographic characteristics under investigation, the findings indicate that the students demonstrated that they understand the value of tracking health information, such as heart rate and blood pressure, as a way to reduce the prevalence and impact of risk factors that can lead to chronic diseases. The results of this study reveal that more than half of the students surveyed are currently using wearable devices and that students who participated in this study used wearables for one main reason: to help them increase their awareness of their health status because they understand the importance of tracking their health metrics in order to boost their health status and reduce risk factors for the development of chronic diseases. This use of wearable health devices among people with and at risk for cardiovascular disease and other chronic diseases is particularly important because they will be in a position to share the health information tracked by the device with their healthcare providers to improve their care and reduce their chances of developing chronic diseases prematurely.
As Finklestein et al. 26 and Jo et al. 27 previously reported, the use of wearables can provide beneficial feedback to users that would alert them to make appropriate changes to their daily routines or behavior to reduce the risk of developing disease. The findings reported by Burnham et al. support the belief that wearables can facilitate remote patient monitoring and provide proactive and faster data access to physicians, resulting in improved health outcomes. 28 There appears to be a small trend toward using wearables as an important step toward improving behaviors that will eventually result in improved health status.
Strengths
The major strength of this study is that the results provide an indication of the perceptions of the students regarding wearable devices and their practices in relation to the use of these devices. This information has the potential to revolutionize the healthcare of African Americans by making it easier for patients, hospital employees, and caregivers to stay connected and interact with their community members in need of care. By tracking their physical and emotional well-being, wearable technology can help individuals better understand themselves and improve their overall health.
While wearable technology provides us with the ability to track our location with GPS and view text messages more quickly, we also gain the ability to monitor our fitness levels and health status. Our research confirmed that health and fitness tracking features are the most important reason why students choose to buy wearable devices.
Limitations
A limitation of the study is the fact that the analysis sample cannot be viewed as representative of the entire university's student population or of the entire AA community. Other limitations of this cross-sectional study include the possibility of recall bias and selection bias. In addition, since the outcome and the exposure are measured at the same time, this limits the ability of the researcher to assume any temporal link between them. So, this procedure has limited predictive potential and a limited ability to assess incidence. Another limitation is the fact that the study was based on the students’ responses to one survey question. However, the findings present some preliminary cues about where intervention and prevention strategies should be focused as African Americans continue to battle to reduce health disparities and reduce the prevalence of cardiovascular disease and its risk factors. Future research would benefit from the inclusion of a larger sample of students and students from additional institutions.
Conclusion
It is evident that wearable devices represent an innovative strategy for reducing a variety of health behaviors. Improving the prevalence of self-monitoring is necessary for behavior change and disease burden reduction among African Americans. Overall, these findings provide preliminary support that these devices appear to be useful for implementing ambulatory measurement of cardiac activity in research studies, especially those where the specific advantages of these methods (e.g. scalability, low participant burden) are particularly suited to the population or research question. The increasing use of wearable devices is making it possible for individuals to track their physical activity and nutritional habits that can be shared with their medical providers in real time to proactively address health concerns. These appear to be additional tools that should be more widely promoted in communities that are striving to reduce the prevalence of chronic diseases that result in premature morbidity and mortality.
So, what is the promise of health wearables? Health wearables are a promising new technology that could be used to strengthen the responses of healthcare professionals and public health experts to the challenges of chronic noncommunicable diseases (NCDs). 29 NCD is a term used to describe certain conditions that lead to health consequences requiring long-term treatment and care. These are types of diseases that are not caused mainly by an acute infection and are regarded as the number one cause of death and disability in the world.
Wearables are fast becoming a new personal strategy that involves integration of individuals’ personal behavioral choices with professional medical analytics to combat chronic disease. It is particularly effective in at-risk communities where the battle to reduce health disparities has been waging for decades. Wearables enable individuals to regularly observe, measure, and record their physical status, as well as their physiological measures. They can also facilitate medication adherence by enabling individuals to adequately maintain their prescribed medication regimen. The medication data collected and stored through these wearables can provide data that will be useful for medical personnel in their treatment of patients and in their development of strategies for the prevention and intervention for the larger community. These types of technology platforms can help to promote a healthier lifestyle and, at the same time, supply vital medical data for health providers to monitor metabolic status, diagnosis, and treatment. 3 In a state like Mississippi, where African Americans lead the nation in the prevalence of cardiovascular disease, 30 communities cannot afford not to promote the use of wearable devices that have the potential to enable community members to personally participate in their own risk factor reduction. 31
Implications
Implications for practice include promoting community-based behavioral interventions focusing on cardiovascular health by promoting and incorporating more use of wearable devices.
Implications for policy include promoting strategies to reduce barriers to using wearable devices to help reduce health disparities in at-risk populations, especially obstacles relating to cost and accessibility.
Implications for future research include seeking to determine how wearable devices can be implemented at all ages to promote increased physical activity and better nutritional practices, in addition to other risk-reduction behaviors in at-risk communities in Mississippi.

Flow chart of study processes.
Footnotes
Acknowledgments
The authors are thankful to the students from Jackson State University, Jackson, Mississippi, who participated in the study.
Contributorship
The study concept, design, and interpretation of findings were drafted by Monique White. Fidelis Ikem conducted data analysis. Candis Pizzetta revised the manuscript. Shelia Malone and Lena Jones assisted with revisions of the manuscript. Edith Davidson, Andrea Hines, and Mario Azevedo assisted with the revision of the manuscript. All authors read and approved the final version of the manuscript. Girmay Berhie managed the research activities/operation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by Jackson State University's IRB (protocol number 0085-22).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the K.W. Kellogg Foundation (Grant Number G636699).
Guarantor
Monique White, PhD
Informed consent
Informed consent was secured from all survey participants prior to the administration of the surveys.