
Abstract
Background
Traditional interventions such as education and counseling are successful in increasing physical activity (PA) participation, but are usually labor and resource intensive. Wearable activity trackers can objectively record PA and provide feedback to help users to achieve activity goals and are an increasingly popular tool among adults used to facilitate self-monitoring of PA. However, no reviews systematically explored the roles of wearable activity trackers in older populations.
Methods
We searched PubMed, Web of Science, Google Scholar, Embase, Cochrane Library, and Scopus from inception to September 10, 2022. Randomized controlled trials were included. Two reviewers independently conducted study selection, data extraction, risk of bias, and certainty of evidence assessment. A random-effects model was used to evaluate the effect size.
Results
A total of 45 studies with 7144 participants were included. A wearable activity tracker was effective in increasing daily steps (standard mean differences (SMD) = 0.59, 95% confidence interval (CI) (0.44, 0.75)), weekly moderate-to-vigorous PA (MVPA) (SMD = 0.54, 95% CI (0.36, 0.72)), and total daily PA (SMD = 0.21, 95% CI (0.01, 0.40)) and reducing sedentary time (SMD = −0.10, 95% CI (−0.19, −0.01)). Subgroup analysis showed that the effectiveness of wearable activity trackers for daily steps was not influenced by participants and intervention features. However, wearable activity trackers seemed more effective in promoting MVPA of participant's age <70 than participant's age ≥70. In addition, wearable activity trackers incorporated with traditional intervention components (e.g. telephone counseling, goal setting, and self-monitoring) could better promote MVPA than alone use. Short-term interventions potentially achieve better MVPA increase than long-term.
Conclusion
This review showed that wearable activity trackers are an effective tool to increase PA for the old population and also favor reducing sedentary time. When used together with other interventions, wearable activity trackers can achieve better MVPA increase, especially in the short term. However, how to more effectively improve the effectiveness of wearable activity trackers is an important direction of future research.
Introduction
Physical activity (PA) offers multiple health benefits for older populations, including reduced risk of all-cause and cause-specific mortality, 1 prevention of chronic diseases, 2 and improved mental health and cognitive function. 3 On the contrary, physical inactivity is recognized as a major risk factor for non-communicable diseases, in particular, cardiovascular diseases (CVDs), type 2 diabetes mellitus (T2DM), cancer, and dementia. 4 It is estimated that globally, 7.2% and 7.6% of all-cause and CVD deaths, respectively, are attributable to physical inactivity. 5 PA guidelines issued by the World Health Organization (WHO) recommended at least 150 to 300 min of moderate-intensity aerobic PA or 75 to 150 min of vigorous-intensity aerobic PA per week for older adults or an equivalent combination of both. 6 But older adults lack sufficient PA. A survey of more than 92,000 people in the United Kingdom (UK) showed that there were less than a quarter of older adults reaching the recommended amount of PA required to maintain health. 7 In addition, sedentary behavior is an independent risk factor negatively affecting the health of older adults independent of PA and is closely associated with adverse health outcomes, including all-cause mortality, CVD mortality, and cancer mortality. 8 And sedentary time is recommended to be limited for older adults. 9 Therefore, effective interventions to help older adults to live more physically active and reduce sedentary behaviors are an urgent issue for public health agencies.
Over the past few decades, traditional lifestyle interventions such as exercise prescription, face-to-face counseling, telephone counseling, and self-monitoring behavior have shown to be effective at increasing the PA level in the short term. 10 However, these interventions are often labor and resource intensive which hinder their wide application. 11 Researchers have been exploring appropriate strategies to promote PA participation. Wearable activity trackers are a subset of wearable devices used for monitoring PA and fitness-related metrics. 12 Lewis et al. 13 defined wearable activity trackers as “commercial wearable devices that objectively measure lifestyle physical activity and can provide feedback, beyond the display of basic activity information (i.e. steps), via the monitor display or through a partnering application to elicit continual self-monitoring of physical activity.” Wearable activity trackers have gradually entered people's daily life and won a large number of user groups with their affordable price, 14 excellent interactivity, and friendliness 15 and have been widely used in health promotion in various scenarios.16,17 Wearable activity trackers enable individuals to monitor the user's PA levels by providing feedback like daily step counts, energy expenditure, or other specific feedback designed by health professionals, such as heart rate and blood pressure. This can help users transform from a sedentary lifestyle to a more active lifestyle, 18 achieve goals such as staying fit and active, losing weight, and health self-monitoring. 19 These devices offer a less resource-intensive alternative to traditional interventions and allow for population-level measurement of PA and large-scale behavior changes. 20 In addition, different activity trackers use different sensors and algorithms to calculate visual indicators. The two most common types of sensors are pedometers and accelerometers. 21 Pedometers can be used to monitor steps with inexpensive and energy-saving characteristics, but it is not as accurate as accelerometers, which are currently the standard for collecting PA data. 22
Although the literature on PA promotion via wearable activity trackers is increasing, the differences in wearable activity trackers types, study designs, and populations render results and conclusions inconsistent. Most of these reviews included studies that recruited participants below 60 years,23–26 or participants were restricted to healthy individuals or patients with chronic conditions,27–30 which limited the generalizability of their results to the older populations. To date, there was only one review that investigated the effectiveness of PA trackers on PA in older adults aged over 60, with daily steps as the main outcome. 31 Walking is a kind of free-living pattern of ambulatory activity that better reflects the PA as it is the most common PA type for older adults. Thus, daily steps are a meaningful metric for PA promotion in clinical and population settings. Taking more daily steps is associated with a gradually declined risk of all-cause mortality with larger effects observed in older adults than young adults.32,33 However, daily steps cannot fully reflect the PA level of older adults, especially when the time and intensity of PA were targeted. The total daily PA level, the intensity of PA (moderate-to-vigorous PA (MVPA)), and sedentary time are also closely associated with mortality and health outcomes.34–36 The purpose of this study was therefore to add to the evidence on the effectiveness of wearable activity trackers on PA (daily steps, MVPA, and total daily PA) and sedentary time in older adults. Subgroup analysis and meta-regression analysis were used to explore the potential modulators of heterogeneity across studies.
Methods
Protocol and registration
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Our study protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) with registration number: CRD42022357959 (Supplemental Table S1).
Search strategy
We searched PubMed, Web of Science, Google Scholar, Embase, Cochrane Library, and Scopus for randomized controlled trials (RCTs) of wearable activity trackers intervention in PA participation in older adults. Each database was searched from inception to September 10, 2022. Search strategies were developed relating to three primary concepts of the review: wearable activity trackers, PA, and older adults. The search formula was combined with medical subject headings (Mesh) and free-text terms. Search strategies were adapted for each database as necessary. For example, to identify studies that included the wearable activity tracker, we used search terms including Wearable devices (Mesh), Activity tracker (Mesh), Fitness tracker (Mesh), Wearable tracker, and Wearable monitor. The full search strategy is available in Supplemental Table S2. Manual searches were performed on the references of the studies to find those that might meet the inclusion criteria but could not be detected in the initial search.
Eligibility criteria
We included RCTs that evaluate the effectiveness of wearable activity trackers for increasing PA and reducing sedentary time in older adults. Eligible studies were restricted to English-language publications, and only peer-reviewed journal papers were considered. Participants over 60 years old were included. We excluded participants who suffer from severe cognitive impairment or mental illness which may affect the use of wearable activity trackers. We also excluded participants with physical disability (impaired moving ability) as their activity patterns were not comparable to other participants. Studies using wearable activity trackers alone or in combination with other components to promote PA or reduce sedentary time were included. Other intervention components could be face-to-face counseling, telephone counseling, group education, exercise prescription, goal setting, etc. This study mainly discussed wearable activity trackers using sensor types of either pedometers or accelerometers. Studies using wearable activity trackers only as a PA measurement tool before and after intervention were excluded. In addition, the control group can be usual care, waitlist, and no intervention. The primary outcome measure was an objective measure of PA, including daily steps, weekly MVPA time, total daily PA time, and sedentary time. Self-reported measures of PA were not included in this meta-analysis.
Data extraction
Two independent reviewers extracted the data (LD and GL). A data extraction sheet was created to collect data including basic information (authors, publication time, and country), sample characteristics (sample size, participant's age, gender, and health status), and characteristics of intervention (model of devices, intervention duration, and intervention components). The data of PA measures including daily steps, weekly MVPA time, total daily PA time, and sedentary time before and after intervention were extracted in the form of mean ± standard deviation (SD).
Risk of bias
The risk of bias in included studies was assessed using the Cochrane risk assessment tool. The Cochrane risk assessment tool has become the standard approach to assessing the risk of bias in randomized clinical trials that has frequently been used in systematic reviews. 37 Two reviewers (LD and GL) independently conducted the assessment and resolved disagreement in consultation with the third reviewer (QH). The Cochrane risk assessment tool had seven domains including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. Each of these criteria was judged and classified as “low risk,” “high risk,” or “unclear risk.”
Certainty of evidence
The Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) system was used to determine the certainty of evidence by GRADEprofiler software. The GRADE system is widely used to evaluate the certainty of evidence in the systematic review, which reflects the author's confidence that the effect estimates are adequate to support a particular recommendation. 38 Five domains were used to assess the certainty of evidence (risk of bias, indirectness, imprecision, publication bias, and inconsistency), and the certainty of evidence was graded into four levels such as high, moderate, low, and very low. Two reviewers (LD and GL) independently conducted the assessment and resolved disagreement with the third reviewer (QH).
Data analysis
Statistical analyses were performed using Review Manager (RevMan 5.4, The Cochrane Collaboration, Copenhagen, Denmark). Two reviewers (SW and SC) independently performed data analysis and resolved disagreement with the third reviewer (QH). A random-effects model was used to estimate the effect size which was expressed as standard mean differences (SMD) with 95% confidence intervals (CIs). 39 The SMD was interpreted according to the Cohen rule of interpretation (small 0.2 ≤ SMD < 0.5, medium 0.5 ≤ SMD < 0.8, and large SMD ≥ 0.8). 40 Heterogeneity across studies was assessed using a chi-squared test and the I2 statistic, in which the boundary limits 25%, 50%, and 75% were designated as low, moderate, and high heterogeneity. 41 Sensitivity analyses were performed to evaluate the robustness of the results by removing each study. When significant heterogeneity was found, meta-regression analysis was used to explore the source of heterogeneity. Subgroup analysis was used to examine the influence of potential modulating factors on pooled effect size. Publication bias was assessed using funnel plots and Egger's test. Trim and fill analysis was performed if there is significant publication bias.
Results
Study selection
A total of 6731 studies were initially retrieved from six databases, and there were 11 additional records identified through reference checks (Figure 1). After removing duplicate documents, 3762 studies remained. After preliminary screening by titles and abstracts, 3621 irrelevant studies were excluded. The remaining 141 articles were assessed through full-text reading, and a total of 45 studies were included in the meta-analysis.42–66,67–86

Flowchart of study selection.
Characteristics of included studies
The characteristics of included studies are shown in Table 1. A total of 7144 participants were included in the primary analysis of PA outcomes. Twelve studies are from America, seven studies are from the UK, seven studies are from Holland, four studies are from Japan, and another 15 studies are from Canada, Australia, Germany, Belgium, Portugal, China, and other countries.
Participant characteristics of eligible studies.

T: intervention groups; C: control groups; M: male; F: female; COPD: chronic obstructive pulmonary disease; MVPA: moderate-to-vigorous physical activity; T2DM: type 2 diabetes mellitus. Daily steps (step/day), MVPA (min/week), total daily physical activity times (min/day), sedentary time (min/day).
The mean age of participants ranged from 60 to 86 years, and most included studies recruited both men and women while few recruited men or women. There were 22 studies performed in older adults with chronic disease,50,53,56,57,59–62,64–67,70,71,75–79,82,83,85 including five studies on T2DM,56,59,66,71,76 10 studies on choric obstructive pulmonary disease,57,62,64,65,67,75,77,79,83,85 and seven studies on other diseases.50,53,60,61,70,78,82 For the primary outcome of PA measures, 38 studies used daily steps as the primary outcome.42,44–47,49–51,53,54,56–66,67,69–81,83–85 Eighteen studies used weekly MVPA time as the primary outcome,43–45,48,49,54–56,60,64,65,68,70,71,73,78,82,84 11 studies used sedentary time as the primary measure of PA,45,51,52,54,56,61,65,68,71,82,86 and only four studies measured total daily PA time.48,56,65,66
The duration of the interventions ranged from four to 48 weeks. Nineteen studies received intervention duration longer than 12 weeks,44,45,47,48,50,53,56–58,61,62,66,71,72,76,77,80,84,86 and 26 studies had intervention duration <12 weeks.42,43,46,49,51,52,54,55,59,60,63–65,67–70,73–75,78,79,81,82,85 In terms of the sensor type of wearable activity trackers used, 29 studies used pedometer-based intervention,42,43,46,49,51,52,54,55,59,60,63–65,67–70,73–75,78,79,81,82,85 and 16 studies used accelerometer-based intervention.44,48–51,55,60,61,67,68,70,78,79,82,84,86 We found that nine studies used wearable activity trackers alone as the intervention44,47,48,50,52,53,57,59,62 while 36 studies used wearable activity trackers combined with other intervention components.42,43,45,46,49,51,54–56,58,60,61,63–73,74–86 Other intervention components mainly used exercise prescription/program, telephone consultation, face-to-face consultation, goal setting, group education, and self-monitoring. And these interventions have been proven to be effective at increasing PA participation as well as reducing sedentary time in the short term. 87
Risk of bias
The results of the risk of bias assessment are shown in Figure 2. All included studies reported appropriate random sequence assignment and were assessed as low risk of bias. Twenty-four studies provide insufficient information regarding the procedures used to conceal the allocation and were assessed as unclear.42–45,48,49,52,53,55–61,63,65,68,69,73,74,76,77,81,84 High risk of bias was mostly identified in performance bias with most articles not blinding researchers and participants. At the same time,14 articles were assessed as high risk in detection bias.46,48–50,62,63,67–69,72,74,78,83 Most of the studies provided complete outcome data, while two studies were classified as high risk of attrition bias due to incomplete outcome data.71,80 In addition,14 studies were assessed as high risk for selective outcome reporting.43–45,48,50,51,54,56,63,64,66,71,75,80 No studies were assessed as high risk for other sources of bias because of conflicts of interest declared by the authors (Supplemental Table S3).

Summary of the risk of bias results from eligible studies.
Certainty of evidence
The certainty of evidence for daily steps and MVPA was rated very low and low due to three downgrades, including a high risk of bias due to no blinding of participants and personnel, insufficient information on allocation concealment, high heterogeneity, and publication bias, respectively. The certainty of evidence for sedentary time was rated moderate, due to one downgrade on risk of bias. In addition, the certainty of evidence for total daily PA time was rated as low due to no blinding of participants and personnel and a small sample size. All in all, the certainty of evidence for daily steps and MVPA was rated very low and low, sedentary time was rated moderate, and total daily PA time was rated as low (Supplemental Table S4).
Publication bias
The results of publication bias are shown in Table 2. No significant asymmetry was found by funnel plots for all outcomes (Supplemental Figures S1 to S4). However, Egger's test showed significant publication bias for MVPA (P = 0.048). Trim and fill analysis was performed, and MVPA results are expected to be stable after eight studies are filled as Figure 3 indicated.

Trim and fill analysis of moderate-to-vigorous physical activity (MVPA).
Summary of publication bias.

The bold value represents the significant results (P-value ≤ 0.05).
Synthesis of results
Daily steps
Figure 4 shows the effectiveness of wearable activity tracker intervention on daily steps. A total of 38 studies were analyzed, and the results showed that the wearable activity trackers had a medium effect size (SMD = 0.59, 95% CI (0.44, 0.75), P < 0.00001) on increasing daily steps compared with the control group, representing an approximate 1430 steps (95% confidence interval (CI): 1092 to 1767 steps). However, there was significant heterogeneity across studies (I2 = 85%, P < 0.00001). To further determine the robustness of the analysis, sensitivity analysis was performed to detect the changes of heterogeneity by removing studies one by one. The result revealed no significant changes.

Forest plot of the effect of wearable activity trackers on daily steps.
Total daily PA
Figure 5 suggests that four studies compared the effectiveness of wearable activity trackers with the control group on total daily PA time. The wearable activity trackers induced a small but significant average effect size (SMD = 0.21, 95% CI (0.01, 0.40), P = 0.04) on the total daily PA time, representing an increase of approximately 17 min more than the control group (95% CI: 0.8 to 33 min). Moderate heterogeneity was identified (I2 = 47%, P = 0.07).

Forest plot of the effect of wearable activity trackers on total physical activity time.
MVPA
A total of 18 studies were analyzed to estimate the effectiveness of wearable activity tracker interventions on weekly MVPA time in Figure 6. It is estimated that wearable activity trackers had a medium effect size on MVPA (SMD = 0.54, 95% CI (0.36, 0.72), P < 0.00001), representing an increase of approximately 38 min (95% CI: 25 to 50 min) more than the control group. Significant heterogeneity across studies was identified (I2 = 85%, P < 0.00001). However, sensitivity analysis suggested a relatively robust result.

Forest plot of the effect of wearable activity trackers on moderate-to-vigorous physical activity (MVPA).
Sedentary time
A total of 11 studies reported changes in sedentary time following wearable activity tracker-based interventions (Figure 7). The results showed a small favorable effect size (SMD = −0.10, 95% CI (−0.19, −0.01), P = 0.03), representing an average decline of 7.54 min compared with the control group (95% CI: −15.54 to 0.45 min). There was moderate heterogeneity across studies (I2 = 35%, P = 0.09).
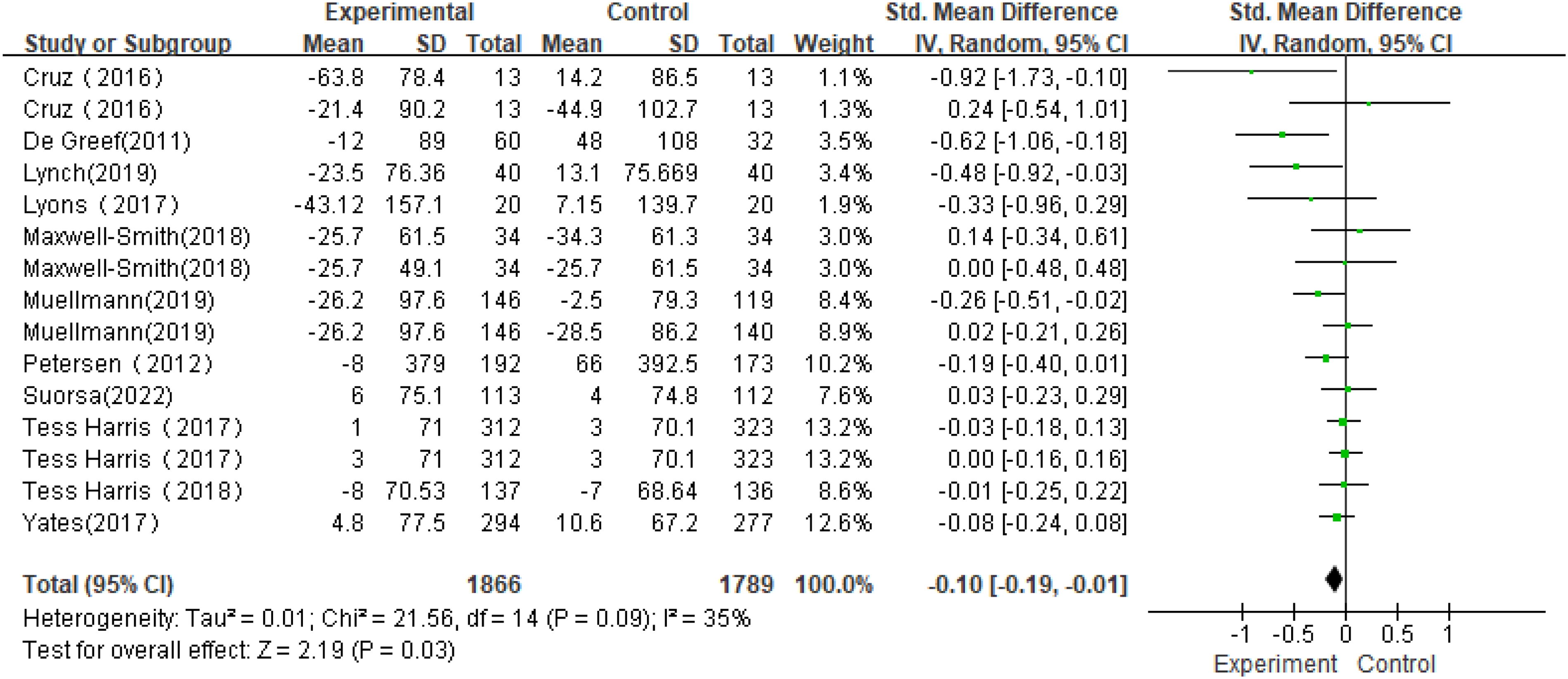
Forest plot of the effect of wearable activity trackers on sedentary time.
Meta-regression
To further explore the source of heterogeneity in daily steps and MVPA, meta-regression analysis was performed by intervention duration, intervention components, health status, sample size, age, and publication years (Table 3). Heterogeneity was discussed using univariate meta-regression. Intervention duration, health status, sample size, intervention type, age, and publication years had no significant effect on heterogeneity in daily steps while intervention duration (β = −0.187, 95% CI (−0.54, 0.17), P = 0.03) and intervention components (β = −0.31, 95% CI (−0.71, 0.10), P = 0.03) are probably the sources of heterogeneity in MVPA.
Meta-regression for daily steps and moderate-to-vigorous physical activity (MVPA).

The bold value represents the significant results (P-value ≤ 0.05).
Subgroup analysis
The subgroup analysis results are presented in Table 4 and Supplemental Figures S5 to S14. The potential modulating factors included age, health status, sensor type used by the wearable device, intervention components, and intervention duration.
Subgroup analysis of daily steps and MVPA.

MVPA: moderate-to-vigorous physical activity; SMD: standard mean differences; CI: confidence interval; Pa: significance of subgroup effect sizes; I2a: heterogeneity of subgroup; Pb: significance of heterogeneity between subgroups; I2b: heterogeneity between subgroups.
Subgroup analysis by age indicated a similar pooled effect size between participants on daily steps (SMD≥70 = 0.44, 95% CI (0.11, 0.79), P = 0.009; SMD<70 = 0.66, 95% CI (0.45, 0.86), P < 0.0001) following wearable activity tracker intervention compared with the control group. Similarly, wearable activity tracker intervention induced a relatively high weekly MVPA increase in younger participants (SMD<70 = 0.65, 95% CI (0.37, 0.93), P < 0.0001) than that of older participants (SMD≥70 = 0.27, 95% CI (0.1, 0.45), P = 0.002); statistical significance was reached between subgroups.
There was no significant difference between participants with chronic conditions and participants without in daily steps (SMDwithout = 0.55, 95% CI (0.32, 0.78), P < 0.0001; SMDwith = 0.55, 95% CI (0.33, 0.77), P < 0.0001) as well as weekly MVPA (SMDwithout = 0.39, 95% CI (0.20, 0.57), P < 0.0001; SMD with = 0.77, 95% CI (0.34, 1.20), P = 0.0004).
The accelerometer-based intervention had a small pooled effect on daily steps (SMDaccelerometer = 0.44, 95% CI (0.17, 0.71), P = 0.001) while the pedometer-based intervention had a medium effect on daily steps (SMDpedometer = 0.58, 95% CI (0.39, 0.76), P < 0.0001). No significant subgroup difference was observed. Similarly, both accelerometer- and pedometer-based interventions had a medium pooled effect on MVPA (SMDaccelerometer = 0.50, 95% CI (0.24, 0.76), P = 0.0002; SMDpedometer = 0.65, 95% CI (0.33, 0.97), P < 0.0001) with no subgroup difference.
Subgroup analysis by intervention components demonstrated that wearable activity trackers alone had a small to medium pooled effect size on daily steps (SMDsingle = 0.51, 95% CI (0.12, 0.91), P = 0.01) while a combination of wearable activity trackers with other components had a medium effect on daily steps (SMDcombined = 0.57, 95% CI (0.39, 0.75), P < 0.0001). No significant subgroup difference was identified. In addition, wearable activity tracker single use had no effect on MVPA (SMDsingle = −0.03, 95% CI (−0.4, 0.35), P = 0.89). However, when combined with other components, wearable activity trackers had a larger pooled effect size on weekly MVPA (SMDcombined = 0.70, 95% CI (0.44, 0.87), P < 0.0001) than wearable activity trackers alone. And there is a significant subgroup difference (P = 0.002).
Long-term and short-term interventions had a small and medium pooled effect on daily steps (SMD>12weeks = 0.49, 95% CI (0.33, 0.64), P < 0.0001; SMD≤12weeks = 0.56, 95% CI (0.26, 0.86), P = 0.0003), respectively. No significant difference between subgroups was identified. However, short-term interventions had a significantly larger pooled effect (SMD≤12weeks = 0.68, 95% CI (0.40, 0.96), P < 0.0001) than long-term interventions (SMD>12weeks = 0.33, 95% CI (0.08, 0.58), P = 0.009) on MVPA.
Discussion
The present systematic review and meta-analysis synthesized the most complete evidence available to date about the effectiveness of wearable activity trackers on PA and sedentary time in older populations. The main finding is that wearable activity trackers induced a significant increase for all measures including daily steps, weekly MVPA time, total daily PA time, and favored reducing sedentary time for old populations. Our results indicated that old adults would accumulate more step counts per day as long as they used wearable activity trackers. This finding would help encourage old adults to use wearable activity trackers to increase daily steps. However, participants <70 ages had a larger MVPA increase than participants ≥70 ages following intervention and interventions combined with other components appeared to have a higher MVPA increase than interventions using wearable activity trackers alone. Moreover, the effectiveness of short-term intervention seemed better than long-term intervention. In addition, walking is a safe and economical form of PA for older populations, and the health benefits of more daily steps have been widely accepted.88,89 Similar to previous relevant reviews, we found significant improvement in daily step counts following the wearable-based intervention. Overall, the effect size of the wearable activity tracker intervention varied in previous studies when evaluated by SMD (0.23–0.85).23,26,28,29,90 A medium effect size was found in our study (SMD = 0.59) which represented an added approximate 1430 steps per day when expressed as actual units. It is suggested that 6000 to 8000 steps per day can provide the biggest protection from the risk of mortality for adults aged over 60. 89 Thus, an extra increase of 1430 steps would contribute more health benefits for old adults. The main reason for the variance in effect size across these reviews can possibly be an interaction of the participant’s features, intervention features, etc. Brickwood et al.26 reported a small effect size (SMD = 0.23) probably due to a broad definition of wearable activity trackers (tools such as regular emails and text messages were also classified as wearable-based intervention). Hodkinson et al. 29 showed a large effect size (SMD = 0.85) on steps, and this might be associated with the fact that participants with cardiometabolic conditions are strong-willed to improve their health.
Strong scientific evidence supported the health benefits associated with MVPA. Finishing over 150 min MVPA per week as recommended can significantly reduce the relative risk of call-cause mortality. 91 Previous meta-analyses demonstrated that wearable activity trackers induced a small effect size (SMD 0.28 to 0.33) on MVPA, representing an average increase of 75 and 43 min, respectively.25,90 Although a medium pooled effect size (SMD = 0.54) was identified in our study, there was a relatively small average increase of MVPA (38 min) compared with these studies. In addition, another three meta-analyses reported a small to medium effect size (SMD 0.30 to 0.61) on MVPA following the wearable activity tracker-based intervention; however, these studies did not report the MVPA level by actual units.23,28,29 All in all, the difference in SMD values might be a consequence of the broad range of included interventions, compactors, and populations. For instance, the application of wearable activity tracker intervention in cancer survivors revealed a medium effect size (SMD = 0.61) on MVPA which can be explained by the dramatic decline of the PA level post-diagnosis and during cancer treatment.92,93 In addition, the discrepancy between SMD and MD (mean differences) values can be partly explained by the participants. Older adults naturally had lower baseline MVPA levels while young adults had relatively higher MVPA levels. 94 Thus, it is reasonable that wearable activity trackers had a large effect size on older adults but indeed with a low increase of MVPA time.
The potential factors that modulate the effectiveness of wearable activity trackers on steps and MVPA have been explored in different reviews.23,28,29,90 In terms of participant features, subgroup analyses demonstrated that participants aged <70 had a larger MVPA increase than participants aged ≥70. This finding is supported by many studies that consistently show a decrease in PA progressively with age, 95 and the MVPA time declines with aging. 94 However, there was no significant difference in daily steps. Li et al. 90 investigated the impact of age on the effects of wearable activity trackers for steps or MVPA by meta-analysis and found that younger participants had larger step increases which conflicted with our finding. However, they separated participants into ages <60 and ≥60 which cannot provide a reference for us. We compared interventions ≤12 weeks and >12 weeks as previous meta-analyses did.28,31,90 The health status of participants also might modulate the effects of interventions. However, previous reviews just examined the effects of wearable activity trackers in promoting steps in participants with29,30 and without 23 chronic conditions, respectively. Franssen et al. 96 further determined that patients with different chronic conditions achieved different step increases by subgroup analysis of chronic conditions which was not available in our study.
Our results showed that wearable activity trackers combined with other components had larger effects for increasing MVPA while no difference was observed for daily steps. This finding was in line with the results of Singh et al., 28 which reported a higher MVPA increase in cancer survivors following wearable activity tracker intervention with baseline counseling. However, Brickwood et al. 26 reported no difference in MVPA and steps between wearable-based and multifaceted interventions. Indeed, traditional interventions such as telephone counseling, face-to-face counseling, and group education were extensively studied and generally yield positive effects for increasing PA participation in various populations, although they are labor and resource intensive.97,98 The investigation into the impact of intervention duration on the effects of wearable activity trackers for increasing MVPA or daily steps was inconsistent. Singh et al. 28 found that a longer duration of intervention was more effective than a short duration of intervention for improving MVPA, not daily steps. However, on the contrary, we found that shorter-term interventions could induce higher MVPA increases than long-term interventions, and no significant difference in daily steps was observed. This finding is consistent with existing reviews.90,99,100 Indeed, a survey suggested that over 50% of users stopped wearing them within six months, and only <20% keep using them after six months. 101 Older adult's positive attitude toward wearable activity tracker use did not persist long, and both step counts and MVPA time showed waning patterns through the three-month study period. 102
In addition, the different sensors and algorithms used to record PA might be a potential modulator of the effectiveness of the intervention. 21 Pedometers are a kind of portable electrical or electrical–mechanical trackers that record the steps a person takes while an accelerometer or fitness tracker used algorithms to measure acceleration forces to accurately detect periods and intensity of PA. 103 So the effectiveness and reliability of different activity trackers are different. 104 Therefore, it is necessary to select an appropriate activity tracker according to the specific requirement of users for PA measurement (steps, MVPA, energy consumption, etc.). 105 However, we found that there was no significant difference between pedometer- and accelerometer-based interventions on daily steps and MVPA. Li et al. 90 reported a larger MVPA increase following accelerometer-based interventions than pedometer-based interventions while in contrast, the pedometers showed more increase in MVPA in studies led by Hodkinson et al. 29
Reducing sedentary time is important for improving overall health. 106 This study for the first time showed that wearable activity trackers can significantly reduce sedentary time in older adults. However, most previous meta-analyses reported no significant sedentary time changes in adults following wearable activity tracker intervention, possibly due to limited studies focusing on sedentary time. 90 There is only one meta-analysis suggesting that computer, mobile, and wearable technology-based intervention resulted in an average reduction of 41.28 min per day of sitting time, and their effectiveness is most prominent in the short term (≤3 months). 107 In line with this review, the majority of studies included in our study were older adults with an intervention duration of ≤12 weeks, while more than half of the studies included in the above two reviews included an intervention duration of >12 weeks.
The PA volume also matters in the older population's health. As a prospective cohort study in US adults reported, greater total PA is associated with lower all-cause mortality with those in the highest tertile having one-fifth the risk of death of those in the lowest tertile (HR = 0.21). 34 So, taking more total daily PA is another option for health promotion. However, most existing relevant reviews did not report total daily PA time as an outcome.23,29 Singh et al. 28 reported a medium effect size (SMD = 0.62) on total PA following wearable activity tracker intervention compared with usual care in cancer survivors. Consistent with this meta-analysis, we found a small increase in total daily PA (SMD = 0.21). The difference might be associated with the decline in overall PA levels in cancer survivors post-diagnosis or during treatment. 92 Thus, these cancer survivors with low baseline PA levels would gain larger benefits following the intervention.
However, most RCTs included in this review were conducted in developed countries; only a few studies investigate the use of wearable activity trackers in old adults in developing countries where public health conditions extremely need to be addressed with new or innovative approaches. Therefore, we call for more attention to the possibility of carrying out RCTs in developing countries. Secondly, the effectiveness of wearable activity trackers will weaken over time. How to increase the effectiveness of long-term use of wearable activity trackers for old adults in the future should be a future direction of study. Moreover, we think that future research directions should pay more attention to which kind of intervention or combination (wearable devices alone or self-monitoring alone, finial incentive alone, or multifaceted interventions with different combinations of components) is the best strategy to promote PA in adults or a specific population. Therefore, a network meta-analysis is needed in the future.
Strengths and limitations
There are several limitations needed to be addressed. Many studies included small sample sizes and had large effect sizes which may overestimate the effects. Future studies should recruit larger sample sizes. There was significantly high heterogeneity across studies. Most interventions consisted of multiple components rather than wearable activity trackers alone, and the effect of each individual component cannot be evaluated in this study. Finally, the certainty of evidence of outcomes suggested that several outcomes were rated as low or very low in this study due to the presence of risk of bias. So, the results should be interpreted carefully. And future high-quality studies are needed in this field.
Conclusions
This study suggested that a wearable activity tracker is a promising strategy to enhance steps, weekly MVPA, and total daily PA time and has a small favorable effect on reducing sedentary time for older populations. Wearable activity trackers used as the main component of intervention or a part of the intervention can encourage more daily steps for old people, regardless of age, health status, sensor types, and length of intervention duration. And when combined with other traditional components, wearable activity trackers generally induce a higher increase in MVPA than alone use. So, wearable activity trackers can be used as a complementary to interventions like group or individual education or counseling. Short-term intervention was more effective than long-term intervention for promoting MVPA. Indeed, this was associated with decreased adherence to using wearable activity trackers. Thus, the strategy of how these devices can be adopted for long-term use should be targeted in the future.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231176705 - Supplemental material for The effectiveness of wearable activity trackers for increasing physical activity and reducing sedentary time in older adults: A systematic review and meta-analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076231176705 for The effectiveness of wearable activity trackers for increasing physical activity and reducing sedentary time in older adults: A systematic review and meta-analysis by Shuang Wu, Guangkai Li, Litao Du, Si Chen, Xianliang Zhang and Qiang He in DIGITAL HEALTH
Footnotes
Contributorship
SW contributed to data curation, formal analysis, visualization, and writing—original draft preparation; GL contributed to formal analysis, visualization, and writing—review and editing; LD contributed to data curation and formal analysis; SC and XZ contributed to methodology, supervision, and writing—review and editing; QH contributed to conceptualization, project administration, funding acquisition, and writing—review and editing. All authors have read and agreed to the version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Office of Shandong Philosophy and Social Science provided fund for this study (Shandong Province Social Science Foundation, grant number 22CTYJ06).
Guarantor
QH.
Informed consent
According to the journal submission guidelines, the patient consent statement was not necessary due to the study being a systematic review.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.