
Abstract
Objective
The relative deprivation of income among chronically ill patients may create a perception of inequity in their access to quality healthcare, which may lead to a decline in patients’ trust and further increases the burden of chronic diseases. Digital finance could be the antidote. To promote equity in healthcare delivery, this study explores the mitigating effect of digital finance by elucidating the relationship between relative deprivation of income and chronically ill patients’ trust.
Methods
Using data from the China Family Panel Study, a Poisson regression model was applied to assess the effect of relative deprivation of income on chronically ill patients’ trust. A marginal effect analysis was used to verify the effect and a two-stage least squares method was used to test robustness.
Results
Chronically ill patients’ trust was at a medium level (5.98 ± 2.05). Relative deprivation of income significantly reduced patients’ trust (β=−0.056, p < 0.1). The digital finance had a positive effect on patients’ trust (β=0.035, p < 0.01) and alleviated the negative effect of relative deprivation of income on patients’ trust (β=0.105, p < 0.01). The instrumental variable estimation results confirmed the robustness of the benchmark regression results.
Conclusions
The inequity resulting from relative deprivation of income undermines patients’ trust. Digital finance has a long-term effect on alleviating perception of inequity among chronically ill patients. The government should promote the integration of digital finance and smart healthcare to enhance patients’ trust and contribute to equality in healthcare delivery. Limitations include self-reported data and an insufficient correlation between selected indicators and healthcare services.
Highlights
The three-period panel data from CFPS was used to assess the causal relationship.
Patients’ relative deprivation of income could reduce their trust in doctors.
Digital finance may mitigate lack of patients’ trust due to relative deprivation.
It should promote the integration of digital finance with smart healthcare service.
Introduction
Over the past four decades, China has experienced a rapid shift in disease patterns, accelerating the spread of chronic diseases, thereby increasing the burden of disease and death. a By the end of 2019, the prevalence of chronic diseases in China reached 23%, and the number of corresponding deaths accounted for 88.5% of the total deaths 1 . Except for advances in medical testing technology, the deterioration of the natural environment, changes in lifestyle and the rapid increase in the burden of chronic diseases in China are closely related to patients’ bad behaviours such as ‘not seeking medical advice in time and not following doctors' advice’. 2 Chronic diseases have complex causes, long courses and are difficult to cure; therefore, patients must seek timely medical advice and strictly adhere to it. 3 However, patients in China currently lack trust in doctors, which makes them reluctant to seek and follow timely medical advice. 4 This can aggravate the adverse health outcomes of chronically ill patients and further reduce their trust in doctors. Further, it may erode the trust of doctors in patients and affect the standardized diagnosis and treatment behaviour of doctors, leading to abnormal medical processes in chronically ill patients and increasing the burden of chronic diseases. 5
Patients’ distrust of doctors often stems from the perception of inequity in healthcare and medical services, caused by the inability of individuals to obtain high-quality healthcare and medical services. 6 The greater the quantity and quality of healthcare and medical services that individuals receive, the higher their perception of the equity of healthcare and medical services, and the more inclined they are to evaluate the intentions of doctors positively and to trust them. 7 Individuals’ absolute income level is closely related to the quantity and quality of healthcare and medical services that individuals may obtain and is an important factor that affects patients’ trust. 7 However, several studies have found that the relationship between patients’ trust and individuals’ absolute income level is not clear and that it decreases as an increase in the average income level in the region. 8 This is because absolute individual income places more emphasis on an individual's absolute position in the overall income distribution 9 and does not protect them from the feeling of deprivation resulting from the relatively inadequate quantity and quality of healthcare and medical services they receive. In contrast, perceived resources from the patient's perspective have a greater influence on the patient's belief than the availability of resources. 10 Coincidentally, the influence of personal relative deprivation of income on trust of chronically ill patients stems primarily from individuals’ perception of inequity in the quality of healthcare resources available for comparison. 11 Further, with the widespread application of emerging technologies such as cloud computing, big data and artificial intelligence in various fields, the digital finance based on a trust system has been increasingly popularized among residents and gradually become an integral tool of their daily lives. It imperceptibly transforms people's psychological perception and behavioural patterns. It is considered that the economic support provided by digital finance can effectively reduce the perceived inequity in patients’ access to healthcare resources from the patient's perspective, 12 and others argue that digital alienation in digital finance may exacerbate perceived inequities among chronically ill patients and increase the relative deprivation of income for individuals, 13 impair their trust in doctors and undermine the equity of healthcare and medical services. 14
Based on the above arguments, this study uses a panel data of China Family Panel Studies (CFPS) for the years 2014, 2016 and 2018. In this study, we aim to explore the mechanisms through which individual perceptions of relative inequity influence the trust of chronically ill patients. We will analyze the relationship among factors such as relative deprivation of income, the use of digital finance, and trust of chronically ill patients. Exploring the mechanism of influence of individual relative inequity perception on trust of chronically ill patients by analysing the relationship among relative deprivation of income, the use of digital finance and trust of chronically ill patients. This is of great practical significance in China, where the rapid development of chronic diseases and aging have become serious concerns. Also, the digital transformation of healthcare and medical service institutions has been continuously promoted. Specifically, we address the following two research questions: (1) to clarify the impact of personal relative deprivation of income on trust of chronically ill patients and (2) to explore the role of digital finance use in the relationship between relative deprivation of income and trust of chronically ill patients. Simultaneously, to obtain clearer causal inference, this study uses panel data to control individual heterogeneity, address missing variables and reduce endogeneity bias. Also, a Poisson regression model based on event-counting variables was used to assess the interrelation of relative deprivation of income, digital finance and trust of chronically ill patients. Compared with the general regression model, this regression model can meet the characteristics of over-discretization and excess zeros of count data, meet the assumptions of independent events, overcome the limitations of obvious skewness of variable distribution and the correlation between the variance of model residuals and the mean and have a higher prediction accuracy. Simultaneously, this study provides systematic evidence of the relationship among relative deprivation of income, digital finance use and trust of chronically ill patients by overcoming the endogeneity bias of instrumental variable estimation. First, the study confirms that relative deprivation of income has a significant negative effect on the trust of chronically ill patients. Second, the use of digital finance has a significantly positive effect on the trust of chronically ill patients and can significantly alleviate the negative relationship between personal relative deprivation of income and trust of chronically ill patients. Compared to previous studies, the contribution of this study is reflected in two aspects. First, the evaluation of patients’ perception of relative inequity is more consistent with the connotations of equity perception theory. Assessing the perception of relative inequity of patients with chronic diseases by covering relatively vulnerable people with different income levels is more consistent with the reality that individuals perceive equity through mutual comparison in real-world scenario. Second, it provides evidence of the integration of digital finance and healthcare and medical services. Digital finance in the field of healthcare and medical services does not exhibit the characteristics of digital alienation and may subtly change individuals’ perception of inequities in healthcare and medical delivery, and its combination with healthcare and medical services is an important force in the development of intelligent healthcare, which is of great significance in promoting the digital transformation and intelligent operation of medical service institutions.
Literature review
Patients’ trust
The concept of patients’ trust originates from the concept of trust. Deutsh (1958), a social psychologist, was the first to define trust systematically and scientifically as the behavioural and psychological response of individuals to various external stimuli and believed that it would change with the change in external stimuli. 15 With the continuous deepening and development of sociological theory, Hosmer (1995) defined trust as an irrational choice made by individuals in the face of uncertainty regarding future expectations and benefits. 16 Henceforth, the trust has made significant progress across several disciplines. Lee (2002) summarized the definitions of trust by scholars from the 17th century to the 20th century by integrating the views from various fields and divided the definition of trust into three different views. 17 The first view emphasizes that a trusted party dominates trust, that is, the trust party's confidence in the sincerity and ability of the trusted party. A trusted party gains the trust of a trusted party by its sincerity and ability. 18 The second view emphasizes trust-led trust, that is, trust-led trust based on the psychological and behavioural expectations of the trusted party, which prefers to accept losses and is willing to actively expose its weaknesses to the trusted party. After weighing the advantages and disadvantages, the trusted party decides to trust them. 19 The third view emphasizes the willingness of both parties, that is, both parties rely on their subjective emotional willingness. 20 Patients’ trust tends to emphasize the second view that trust is dominated by a trusted party. Hall et al. (2002) extended this view to the field of medical and healthcare and defined patients’ trust as a subjective psychology in which patients can accept the behaviour of medical parties without control and supervision. 21 Zhou (2018) further divided patients’ trust into a broad sense and narrow sense. A broad sense of patients’ trust refers to patients’ (patients and their family members) trust in doctors (medical service providers) in the process of healthcare and medical delivery. The narrow sense of patients’ trust was the trust of patients in doctors, that is, patients believe in the ability and motivation of doctors and believe that doctors will do their best to treat their diseases. 22 Ulteriorly, patients’ trust was a component of patient satisfaction with healthcare providers and the health system. 23 It can be divided into interpersonal trust and systemic trust. Interpersonal trust was trust established on the basis of familiarity in the course of communication, including the doctor's work ethic and professional skills. Systemic trust refers to the trust generated by individuals in specific situations based on the professionalism of specific institutions (e.g. the equipment, management and regime of medical institutions). 24
Patients’ trust may improve patients’ confidence in avoiding opportunistic behaviour, positive expectations and willingness to take risks. 25 The higher the patients’ trust, the lower the information search and transaction costs, which can effectively avoid opportunistic risk. 26 Therefore, patients’ trust can predict health outcomes, healthcare and medical services quality and patient's adherence behaviours and plays a prominent role in promoting the sustainable development of the doctor–patient relationship. The aetiology of chronic diseases is complex and constantly evolving, and patients undergo long-term and complex disease treatments and rehabilitation management. A harmonious doctor–patient relationship is necessary for chronically ill patients to get the best prevention and treatment. However, trust is constituted of a systematic vulnerability and dynamic nature, 27 which can be easily broken by daily encounters, not only the grand acts of betrayal but also failing to keep promises or commitments. It is important to continuously assess levels of trust, as trust is dynamic and can change trajectory – either positively or negatively – multiple times over time. 28 Therefore, in this study, longitudinal panel data pairs were used to evaluate patients’ trust.
Relative deprivation of income
Relative deprivation of income is a sub-concept of relative deprivation. Relative deprivation is defined as negative subjective experience when an individual or group is disadvantaged position by comparing themselves to others. 29 The concept of relative deprivation was first proposed by Stouffer et al. (1949). 30 Since then, several researchers have conducted multidisciplinary studies on this topic. Merton (1957), based on the social comparison theory, emphasized from the sociological perspective that the core of relative deprivation lies in the psychosocial experience of ‘relative’ and believed that relative deprivation refers to the sense of deprivation caused by an individual's inferiority when compared with other reference groups. 31 Runciman (1966) defines relative deprivation from the perspective of economics as the subjective feeling of an individual's desire to have something that he does not have but that others have. Relative deprivation can be divided into two dimensions, egoistic and fraternal, depending on the level of the reference object. 32 From a psychological perspective, Gurr (1970) believed that relative deprivation stems from an individual's cognition of the inconsistency between value expectation and value ability. 33 This value expectation can be derived from income, social status or prestige. 34 Income inequality and relative deprivation are among the main causes of poverty and social instability. Relative deprivation theory and models are important tools in the study of income inequality and poverty. Therefore, Yitzhaki (1979) introduced a reference group into the income distribution and determined the concept of relative deprivation of income. 35 Relative deprivation of income refers to the income distribution gap between the individual group and the reference group. This comparative gap enables individuals to perceive their own inferiority relative to that of others and to produce corresponding negative perceptions and emotions (e.g. resentment and anger).36,37 Furthermore, the relative deprivation hypothesis suggests that individuals’ perceived inequity may lead them to exhibit more malice towards social relations. 38 An individual with relative deprivation of income indicates a reduced likelihood for individuals to access high-quality public goods and services and actively participate in social activities, 39 which will exacerbate individuals’ malice and make them tend to show scepticism and distrust in social activities. Compared to general patients, chronically ill patients have to coexist with the disease for a long time. Disease stigma and prolonged suffering from treatment make chronically ill patients more prone to perceiving disadvantages. 40 The perception of inequity in healthcare and medical delivery arising from relative deprivation of income may be relatively high, leading to lower levels of trust and engagement in social relationships. The lack of patients’ trust caused by such perception of inequity will seriously hinder the disease treatment and management of such patients, resulting in a greater burden on their health conditions.
However, existing research has mostly focused on exploring the impact of income inequality on social trust, finding that income inequality deepens social anxiety and class conflicts while eroding social trust and cohesion. 41 Meanwhile, only a few studies have examined the influence of income inequality on patients’ trust. Moreover, although limited research has revealed a link between patients’ lack of trust in doctors and their inequity experiences, as well as a significant relationship between low income and patients’ lack of trust in doctors,42,43 there is a lack of studies analysing the potential impact of income comparisons on patient's trust from the perspective of relative inequity perception.
Digital finance
Digital finance is a new type of finance that relies on advanced technologies, such as the Internet, cloud computing and big data. Broadly speaking, digital finance refers to a new business model based on digital technology that changes the trading patterns and financing forms of traditional financial markets, 44 including mobile payments, online lending, financial services outsourcing, online loans, online insurance, online funds and other forms. Instead of relying on the physical channels on which traditional finance relies, digital finance utilizes digital technologies and integrates scenarios, data and finance to innovate products and services with unique advantages such as wide coverage, convenient access, strong policy targeting and almost zero marginal cost compared to traditional finance. 45 These advantages enable digital finance to improve the efficiency of resources allocation, enhance the cooperation capacity of institutions in various regions and deepen the development of finance to improve the role of the financial system in supporting and promoting the economy. 46 At the same time, digital finance can reduce the transaction cost, information asymmetry and difficulty of credit judgement through digital technologies such as big data and artificial intelligence and then may encourage individuals to engage with financial services and benefit from them to achieve digital financial inclusion. 47 The role of digital finance in promoting inclusive economic growth has also achieved financial inclusion for residents in terms of income and consumption. In terms of the income effect of digital finance, it can provide convenient financial support to promote residents’ entrepreneurship to help residents increase their income and effectively narrow the income distribution gap among individuals. 48 In terms of the consumption effect of digital finance, it enables residents to benefit from it to alleviate liquidity constraints of funds, achieve intertemporal balance of consumption, reduce household uncertainty and release individual consumption demand. 49 The income and consumption effect of digital financial inclusion can help alleviate the perceived inequity of individuals and the corresponding negative effects of relative deprivation of income on individuals. However, existing studies also found that the income increase effect of digital finance is not completely consistent, and it can backfire due to the exclusion of digital finance caused by the digital divide among low-income groups. 50 Also, the consumption effect of digital finance may make individuals fall into the trap of consumerism, further aggravating class contradictions and triggering individual perception of inequity. 51
Most studies have confirmed the positive role of digital finance in improving work and production efficiency across industries, with deepening applications in various scenarios such as enterprise innovation, mass entrepreneurship, agricultural production and environmental governance. The conclusions showed that digital finance can significantly improve the quantity and quality of corporate green innovation, 52 promote household entrepreneurship 53 and food security production 54 and curb regional carbon emission intensity. 55 On the contrary, some scholars revealed that digital finance can widen the digital divide, negatively affecting entrepreneurial activities among residents in underdeveloped areas 56 and potentially hindering the initial digital transformation of agricultural enterprises. 57 However, it should be noted that while Gomber et al. (2018) 12 have theoretically demonstrated the potential for achieving equalization of medical services through the combination of digital finance and healthcare, there is a lack of relevant empirical research specifically focused on the on-going digitization transformation in the healthcare and medical services in China. The literature review is shown in Table 1.
Literature review.

Theoretical analysis and research questions
The core of relative deprivation of income lies in the perception of personal income disadvantage after comparing with others. As postulated by the social comparison theory,
59
individuals often compare themselves to others in their daily lives to learn where they stand. Moreover, the equity theory60,61 tells us that if the income comparison is unequal, the exchange is inequitable and that person feels dissatisfied.
61
Correspondingly, the perceived inequity derived from such comparison will bring the sense of individual income disadvantage, which in turn results in the relative inequity perception of chronically ill patients throughout the process, manner and outcomes of receiving healthcare and medical services. Once the disadvantaged feel this inequity, the experience of individual relative deprivation follows, and it affects patient trust through cognitive and affective response pathways.
36
This is because interpersonal trust can be classified into cognition-based trust and emotion-based trust. In the healthcare and medical services, individuals’ cognition-based trust requires they trust the diagnosis and treatment technique of doctors based on the available information
62
; individuals’ emotion-based trust focuses entirely on the emotional connection established between patients and doctors, as it believes that the doctor will not harm their own interests, thus giving trust.
63
Specifically, in the cognitive response pathway, experiences of personal relative deprivation are associated with negative perceptions.
38
According to cognitive appraisal theory,
64
cognitive assessment, as a core process for coping with stress, can explain the emotional and behavioural responses of individuals when they are confronted with public problems. Thus, such negative perceptions derived from personal relative deprivation experiences will further increase the negative bias of patients with high personal relative deprivation of income,
65
inducing them to be more focused on negative information about doctors and patients, and produce strong intergroup bias and hostile tendencies towards doctors, resulting in a reduction in patients’ trust.
66
In the affective response pathway, the individual relative deprivation experiences can easily lead to dissatisfaction, hostility and other negative emotions, which can increase with the accumulation of personal relative deprivation experiences.9,67 According to the affect-as-information model,
68
the stronger the negative emotions felt by patients, such as sadness and anger, the more likely they are to believe that the medical environment in which they live in is relatively poor, and the more prone they are to make negative subjective evaluations of doctors. Subsequently, they show a low level of trust in doctors.
69
Therefore, this study proposes the first question:
Question 1: Does relative deprivation of income has a negative effect on trust of chronically ill patients?
The feeling of income inequity motivates a person to acquire more social capital to achieve equity or to reduce inequity.
61
According to the social capital theory,
70
individuals obtain tangible and intangible resources at the individual, group and organizational levels through social interaction and contact with others. The higher an individual's social capital, the more conducive it is to the formation of values such as trust, cooperation, reciprocity and sharing. The greatest advantage of digital finance lies in its inclusiveness, which can bring individuals with relative deprivation of income into the scope of social resource allocation and promote social interaction of individuals to help them access more tangible and intangible resources,
71
which increases social equity and even resolves the problems of distribution and equality. Therefore, digital finance can help improve the negative perceptions and negative emotions of chronically ill patients due to perceived inequities resulting from relative deprivation of income and alleviate their distrust of doctors. Specifically, on the one hand, digital finance enhances traditional financial services such as payment services, credit services, insurance services and investment services, thereby breaking through the ‘80/20 rule’ of traditional finance, highlight the tail effect and scale effect,
72
provide more social resources for individuals with relative deprivation of income and improve the enthusiasm of individuals to participate in financial activities to increase their social interaction.
73
The financial and information constraints of individuals with relative deprivation of income can be alleviated, and the income and information resource gap among different individuals can be significantly narrowed.
74
On the other hand, digital finance can provide risk protection for individuals and reduce the concerns of individuals with relative deprivation of income about future uncertain expenditure,
75
which helps improve patients’ ability to take medical risks and provides flexibility to choose the suitablehospital
76
to reduce the perception of inequity caused by relative deprivation of income and mitigate the negative impact of relative deprivation of income on the trust of chronically ill patients.
76
Also, digital finance is established on a credit management system, and the cost of knowing whether other people are trustworthy will be reduced (i.e. the degree of information asymmetry will be reduced) during interactions, which increases patients’ social trust.
77
Individuals can trust people other than relatives and friends based on the ‘trial rule’,
78
and the social capital that provides patients with material resources, information and emotional support also further increased and forms a virtuous circle to improve the trust of chronically ill patients.
However, digital technology is a double-edged sword, which not only brings digital dividends but also brings digital alienation and increases the degree of social alienation,
79
thus enhancing the negative impact of relative deprivation of income on patients’ trust. As can be seen from the logic of digital alienation in the spatial domain,
80
first, digital technology leads to an increasing sense of isolation and closure in individual's real-life spaces, social relevance, social proximity and spatial proximity more and more out of line; the relationships between individuals are increasingly digitization and desertification; and individuals’ sense of belonging and identity to the environment is increasingly reduced,
81
which further reduces the trust of individuals with relative deprivation of income in doctors. Second, the virtual money and information explosion of digital finance easily lead to the expansion of individuals’ needs out of the normal category and induce individuals to fall into the trap of consumerism, which makes the gap between different classes become wider and wider and leads to human alienation.
82
At the same time, the digital alienation of income between the relative deprivation of income group and the dominant group may deepen digital divide, preventing the former from effectively obtaining the social capital dividend brought by digital finance,
58
thus increasing the contradiction between the relative deprivation of income group and the dominant group and reducing their trust in society and doctors. Therefore, this study proposes the second question:
Question 2: Can digital finance mitigate the negative effect of relative deprivation of income on the trust of chronically ill patients in doctors?
The theoretical framework is shown in Figure 1.

Theoretical framework of the study.
Methods
Samples and data sources
The study data were obtained from the CFPS conducted by the Institute of Social Science Survey (ISSS). This database covers 25 provinces (autonomous regions and municipalities directly under the central government) in China, excluding Hong Kong, Macau, Taiwan, Xinjiang, Tibet, Qinghai, Inner Mongolia, Ningxia and Hainan. It focuses on the economic and non-economic well-being of Chinese residents and covers many research topics, including economic activity, educational outcomes, family relationships, population migration and health. It emphasizes the long-term dynamic follow-up of survey respondents. All baseline families were investigated in the 2010 baseline survey, and their future blood or adopted children who were baseline members of the CFPS were considered as permanent follow-up targets. There were three types of questionnaires: community, household and individual. The community questionnaire was used to investigate the environment of the sample households, which aims to understand the household environment in which the sample individuals live, including the family social relationship network, living facilities, assets, socio-economic activities and socio-economic status, and covers the status of the sample individuals, including history and education, economic, health and trust status.
This study examines the relationship among personal relative deprivation of income, digital finance use and trust of chronically ill patients. As the survey data from the CFPS (2010, 2012) lack data on the frequency of e-shopping behaviour, considering that the frequency of e-shopping behaviour is a proxy variable for digital finance use as a core explanatory variable in this study, we used a sample of chronic disease patients from the CFPS 2014, 2016 and 2018 surveys to construct a three-period panel data for empirical analysis. Among them, the variables related to personal characteristics and feelings about medical treatment were obtained from the adult questionnaires, whereas the family characteristics were obtained from the family questionnaires. We matched the adult and household questionnaire data using individual codes. Three periods of unbalanced panel data with sample sizes CFPS2014 (587), CFPS2016 (279) and CFPS2018 (1135) were screened after removing missing and invalid values.
Variables
Dependent variables. The explanatory variable in this study is the trust of chronically ill patients. A question ‘How much do you trust your physician?’ in the CFPS adult questionnaire is administered to assess the trust of chronically ill patients and is set as a continuous variable ranging from 0 to 10. The higher the value, the higher the trust level of patients.
Core explanatory variables. The core explanatory variables were personal relative deprivation of income and digital finance use.
(1) Personal relative deprivation of income. Given that the Kakwani index 83 can overcome the defects of non-normalization, quantitative rigidity and non-scale invariance and normalize the measure by dividing the mean income in the reference group, 84 we use it to measure the personal relative deprivation of income.
Let X represent all individuals surveyed in the CFPS database with a sample size of n. The income of individuals within the group is ranked in an ascending order to obtain the overall income vector of the reference group as 
The (2) Digital finance use. Digital finance services include digital payments, digital credit and digital wealth management.
49
Online shopping, an important application and carrier of digital finance, is closely related to the development of digital finance. Online shopping requires digital payments (such as Alipay, WeChat and other third-party trading platforms) connected to digital wealth management. Some major payment platforms have provided safe Internet wealth management products, such as Yu’ E Bao, which have higher returns than traditional savings, so consumers gradually get used to putting their money on payment platforms such as Alipay or WeChat, which facilitate online payments. Online shopping is linked to digital lending, such as the Jingdong White Stripe, the ants spend bai and other digital financing products. They can give consumers an advance on credit and let them enjoy the ‘spend first, pay later’ shopping experience. Thus, the higher the frequency of e-shopping behaviour, the more frequent the use of digital finance. Therefore, our study uses frequency of e-shopping as a proxy variable for digital finance use to investigate the frequency of e-shopping behaviour by using the question ‘How often do you use the Internet for business activities (e.g. online shopping)?’; the value should be as follows: almost every day = 7, 3–4 times a week = 6, 1–2 times a week = 5, 2–3 times a month = 4, once a month = 3, once every few months = 2 and never = 1. 3. Control variables. To effectively measure the effect of relative income deprivation on the trust of chronically ill patients, we referred to previous literature and selected control variables (individual and family characteristics) as follows.
(1) Individual characteristics. 1. Gender (male = 1; female = 0). Compared with male patients, female patients are less tolerant of the disease and attach more importance to their health, resulting in higher trust in doctors.
85
2. Age (continuous variable). The older the patients, the more serious the decline in all aspects of defence function. As patients get older, their mental and physical functions gradually decline, and they are vulnerable to negative moods such as anxiety, honour and depression, resulting in the lower trust in doctors.
42
We use the ‘actual age of the patient’ to measure individual's age and control the squared term of age, mitigating omitted variable bias. 3. Education. [low-level education = 1, moderate-level education = 2, high-level education = 3 (none/primary/low-level vocational education) = 1, intermediate educational level (secondary school/intermediate vocational education) = 2, high educational level (higher vocational education/university) = 3]. Patients with higher education may have a more rational and objective attitude towards the judgement of the medical system and may even have higher critical awareness, resulting in lower trust in doctors.
7
We use the number of responses to the question ‘What is your highest level of education?’ in the CFPS questionnaire to measure the respondents’ educational level. 4. Medical insurance (yes = 1, no = 0). Patients without medical insurance tend to develop strong intergroup bias and hostility due to high healthcare costs, resulting in lower trust in doctors.
86
5. Self-rated health (continuous variable). The worse the self-rated health, the higher the attention, the more they rely on medical staff and the higher their trust in their doctors.
66
A question ‘How do you think of your health?’ in the CFPS adult questionnaire is used to assess the self-rated health status of chronically ill patients, ranging from 1 (unhealthy) to 5 (extremely healthy). The higher the value, the better the self-rated health. 6. Patient satisfaction (continuous variable). The higher the patient satisfaction, the more positive the evaluation of the doctor, and the higher the patients’ trust will be.
23
A question ‘Are you satisfied with the overall conditions at the point of care?’ in the CFPS adult survey to emulate patient satisfaction. Values range from 1 (very dissatisfied) to 5 (very satisfied), with higher values indicating higher levels of patient satisfaction. (2) Family characteristics. 1. Registered permanent residence (non-agricultural household = 1, agricultural household = 0). Rural residents tend to hold more conservative and traditional cultural values or autocratic values, with a more pronounced worship of authority and professionalism. Therefore, rural residents have higher trust in doctors than urban residents.
87
2. Family income per capita (continuous variable). Patients with a higher family income who occupy more resources are more self-confident in having a positive attitude towards their doctors; therefore, they will have a higher trust in their doctors.
8
Thus, we adopt the logarithm of family income per capita for measurement purposes. As shown in Table 2. 4. Instrumental variable. Our study examines the mechanisms influencing the trust of chronically ill patients and identifies possible challenges to the pathway as follows: First, the omitted variable. In this study, we controlled for many variables at the individual and family levels, but many factors influencing patients’ trust (e.g. the patient's psychological state at the time and personality traits) may make it difficult to exhaust them. Second, there is a measurement error. The main data in the text are from CFPS2014, CFPS2016 and CFPS2018, which are relatively authoritative survey data. However, there may still be respondent memory bias or interviewer recording errors during the survey.
Variable description table.

To reduce the bias caused by the above problems, ‘Pro-index’ is chosen as the instrumental variable. The index is compiled jointly by the Digital Finance Research Center of Peking University and the Ant Financial Services Group. It is based on Ant Financial Services’ big data on transaction accounts, covering data related to 31 provinces (autonomous regions and municipalities directly under the central government), 337 cities (regions, autonomous regions and leagues) above the prefecture level and nearly 2800 counties (counties, county-level cities, banners and municipal districts) in China. It is widely used in research related to the economic effects of digital finance development and is highly authoritative in measuring the level of digital finance development. On the one hand, the instrumental variable satisfies the correlation hypothesis. The higher the digital finance development index, the higher the likelihood of patients’ digital finance use, which, in turn, alleviates patients’ sense of relative deprivation of income. On the other hand, the instrumental variable also satisfies the exogenous hypothesis. After controlling for relevant variables, there is no direct association between the digital finance development index and trust of chronically ill patients. Therefore, the provincial digital finance development index is used as an instrumental variable.
The random-effects panel Poisson regression model
Trust of chronically ill patients was ordered as discrete variables, ranging from 1 to 10. According to the previous section, more than 75% of the 4048 groups of data have only a one-year record, and only a few individuals have records of two or three years. Considering the extreme imbalance of the data, a fixed-panel Poisson regression loses a large amount of data; therefore, we choose a random panel Poisson regression. The equations are as follows:
Since the relative deprivation of income and digital finance use may interact to affect the trust of chronically ill patients, this study adds an interaction term to equation (2):
Results and discussion
Table 3 describes the social background characteristics of the 2001 participants in this study; of the individual characteristics, 51.2% (n = 1026) were male, and the mean age was 42.02 years. The overall educational level of the respondents was low, with an average of 10.16 years of education, and 1108 (55.3%) reported that they had not graduated high school. Of the respondents, 94.5% had medical insurance, and their self-rated health status was low (mean =2.37), while their medical satisfaction was above the middle level (mean =3.38). In terms of family characteristics, 55.1% of the patients were registered in agricultural households, and most of the 2001 respondents were non-agricultural workers (59.3%, n = 1187). Most were engaged in the manufacturing industry (12.8%, n = 258), followed by the wholesale and retail industries (9.9%, n = 200). In terms of specific occupations, 12.0% (n = 242) were field crop production personnel, 6.9% (n = 139) were business personnel and 3.4% (n = 69) were administrative personnel. A total of 2.8% (n = 57) of patients were public (road) transport machinery equipment operators and related personnel. The average annual household income was 4.28, and according to the source of income, the total household income was divided into five types of income: wage, business, transfer, property and other income. Wage income refers to after-tax wages, bonuses and welfare in kind earned by family members engaged in agricultural or non-agricultural employment; business income refers to the net income of the family after deducting costs from the production and operation of agriculture, forestry, animal husbandry, by-products and fishery; it also includes the value of the agricultural products produced by the family for its own consumption and the net profit of the family from the self-employed operation or the establishment of private enterprises. Transfer income refers to the income received by households through government transfer payments (e.g. pensions, subsidies and relief) and social contributions. Property income refers to the income earned by households by renting land, houses and means of production. Other types of income include financial support, gifts and gifts from relatives and friends.
Table of descriptive statistics of variables.
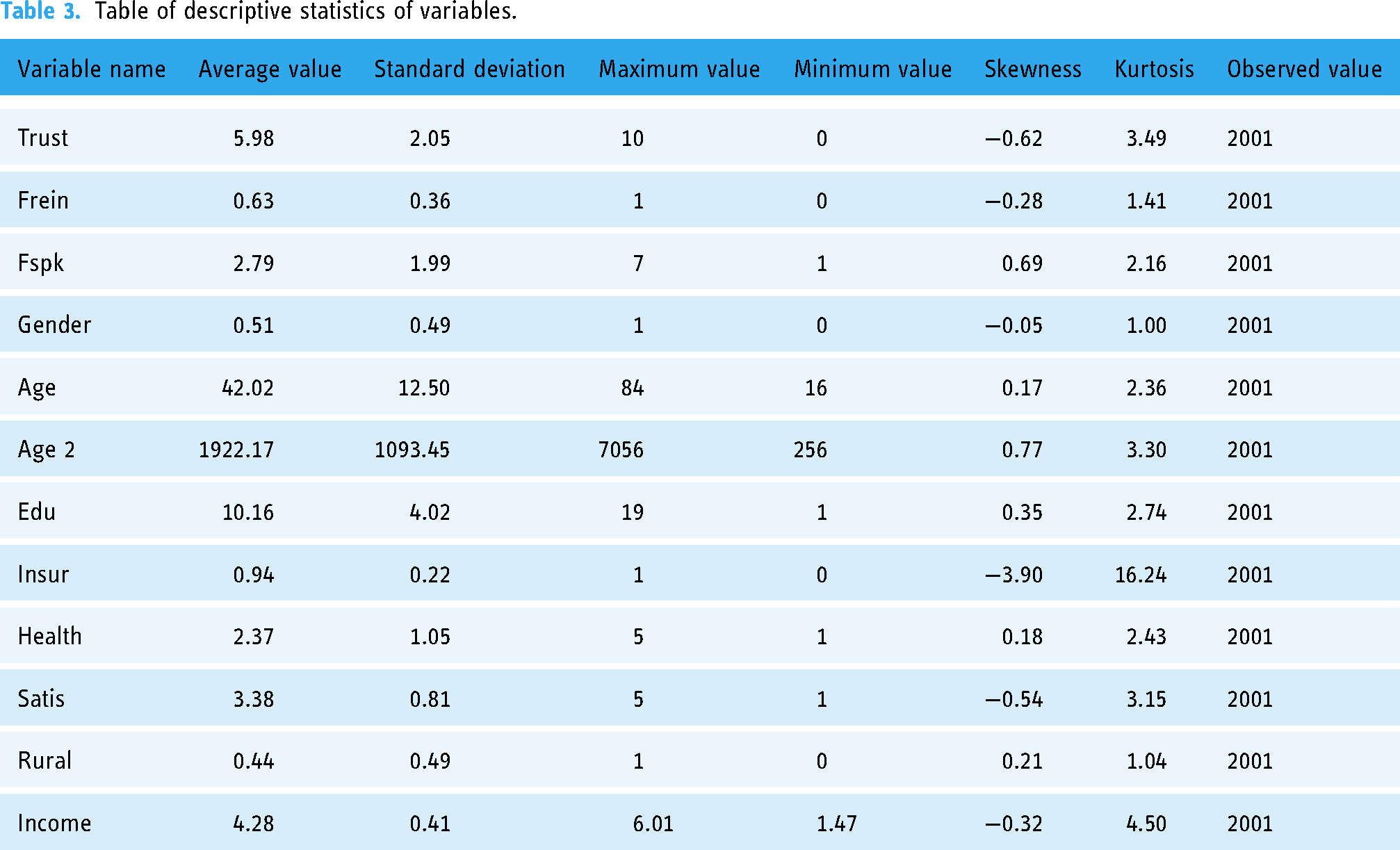
At the same time, according to the results of descriptive statistical analysis, the mean value of trust of chronically ill patients was 5.98, which was at a medium level, and this is similar to the results of Chen et al. (2022). 88 However, Liu et al. (2019) systematically reviewed 32 studies on the changes of patients’ trust in doctors in China from 2007 to 2017 and found that patients’ trust in doctors showed a linear decline in tendecy. 89 This means that the level of patients’ trust in doctors has yet to be improved, and this requires not only to improve the professional ethics and skills of doctors but also to improve the management level of medical institutions. 24 Moreover, the relative deprivation of income index of 17.5% of individuals was less than 0.2, indicating that they experienced little relative deprivation of income. The relative deprivation of income index of 17.3% of individuals was in the range (0.2–0.4), subject to a certain degree of relative deprivation of income. The value of the relative deprivation of income index of 11% of individuals was in the range (0.4–0.6), experiencing strong relative deprivation of income. Further, 54.2% of the individuals had a relative deprivation of income index greater than 0.6, indicating that they might suffer more serious relative deprivation of income. The average relative deprivation of income index for patients with chronic disease was 0.63, indicating that the relative deprivation of income of patients with chronic disease in China was severe. This also proves laterally that the economic burden of diseases borne by chronically ill patients in China is relatively elevated. 90
The effect of personal relative deprivation of income on trust of chronically ill patients
Regressions 1 and 2 in Table 4 report the results of the fixed-panel Poisson regression for the full sample of CFPS2014, CFPS2016 and CFPS2018. Regression 1 only adds the core explanatory variable of personal relative deprivation of income, and regression 2 adds individual-level and household-level control variables on the basis of regression 1. Comparing the results of regressions 1 and 2, the coefficients of personal relative deprivation of income were −0.114 and −0.056, which were significant at the 1% and 10% confidence levels, respectively, indicating that personal relative deprivation of income has a significant inhibitory effect on the trust of chronically ill patients. Chronically ill patients and high personal relative deprivation of income feel the dual pressure of disease and economy through social comparison with others7,67 and have a perception of inequity of the quantity and quality of healthcare and medical services they receive, 52 which leads to an increase in negative emotions and negative cognition of the medical environment, thereby showing a lower level of trust in doctors.
Results of regression analysis.

Note: *, ** and *** indicate significance at 10%, 5% and 1% confidence levels, respectively, and the values in parentheses are standard deviations.
The control variables of the presence or absence of medical insurance, self-rated health status, patient satisfaction and family income per capita show significant and positive influences on the trust of chronically ill patients, non-agricultural household show significantly negatively affects the trust of chronically ill patients. This is consistent with the conclusions of Zhao et al. (2016), 86 Kim et al. (2018), 66 Du et al. (2020) 6 and Zhao and Zhang (2019). 8 In addition, patient gender, age, non-agricultural household and educational level did not have a significant effect on the trust of chronically ill patients. The reasons may be as follows: first, compared to the patients’ age, gender and non-agricultural household, certain potential individual variables of patients (such as patients’ psychological state and personality traits at that time) are more likely to influence patients’ judgements about their trust for doctors’; second, the sample patients’ literacy level is low, and the control effect of patients’ educational attainment on the model is not obvious.
The effect of digital finance use on the trust of chronically ill patients
Regressions 3 and 4 in Table 4 report the results of the fixed-panel Poisson regression estimation of the effect of digital finance use on trust of chronically ill patients. The results of regression 3 show that digital finance use was significantly associated with the trust of chronically ill patients, with the estimated coefficient of digital finance being significantly positive at the 1% level. After adding the control variables in regression 4, the estimated coefficient remains significant at the 1% level. The regression results indicate that digital finance use has a significant positive effect on the improvement of the trust of chronically ill patients. Additionally, the direction and significance of the control variables in regression 3 and 4 are essentially the same as those in regression 2.
The interaction effect of digital finance use and relative deprivation of income on trust of chronically ill patients
The interaction term between relative deprivation of income and digital finance use was re-regressed by introducing the above baseline regression to verify the moderation effect of digital finance use on the relationship between relative deprivation of income and trust of chronically ill patients. Regressions 5 and 6 in Table 4, without considering interaction, show that digital finance use can significantly promote the trust of chronically ill patients. Regressions 7 and 8 in Table 4 show a significantly positive interaction between relative deprivation of income and digital finance use when considering the effect of the interaction term, indicating that digital finance use significantly mitigates the negative effect of relative deprivation of income. According to the estimation results of regressions 7 and 8, the regression coefficients of the interaction terms were 0.101 and 0.105, both of which are significant at the 1% confidence level, indicating that digital finance use has a positive moderating effect on the relationship between relative deprivation of income and trust of chronically ill patients. This also suggests that in healthcare and medical service, digital finance tends to improve the social capital of patients, rather than develop issues of digital alienation. The digital financial platforms, which act as a major port of call for residents to access financial information, can improve the availability of financial resources for patients, 76 help patients increase the developmental consumption of residents, represented by health security consumption and improve the perception of equity of patients. Simultaneously, digital financial online platforms that allow residents to pay conveniently can further alleviate patients’ perception of inequity of the quality of available medical resources by saving patients’ time costs and improving medical experience and improving medical treatment efficiency. 85
In regressions 7 and 8, the regression coefficients of relative deprivation of income were −0.073 and −0.066, which were significant at the 1% and 5% confidence levels, respectively, and H1 is verified again. The regression coefficients of digital finance use were 0.041 and 0.035, which were both significant at the 1% confidence level, basically in the same direction and significance as regression 4. In addition, the direction and significance of the control variables in regressions 7 and 8 are essentially the same as those in regression 2.
The marginal effect calculations in Table 5 show that when the relative deprivation of income increases by one unit, the trust level of chronically ill patients decreases by 6.72%; when digital finance use increases by one unit, the trust level of chronically ill patients increases by 4.13%. The roles of relative deprivation of income and digital finance on trust of chronically ill patients were further verified.
Results of marginal effect analysis.

Robust test
Table 6 reports the parameter result of the instrumental variable regression by using the two-stage least square (2SLS). We first examine the validity of the instrumental variable. The results show that, first, the F-statistic value of 123.34 for the first-stage regression results far exceeds the critical value of 10 for the first stage of the relevant instrumental variable proposed by Staiger and Stock (1997), 91 indicating that the instrumental variable selected in this study is highly correlated with the endogenous explanatory variables. In other words, the instrumental variable has a strong explanatory power for the endogenous variables. Thus, the problem of ‘weak instrumental variable’ was significantly excluded. And the results of the overdispersion tests show that the variance of the explained variables was 0.7 times the mean, so there was no overdispersion. Second, the results of the unidentified test for instrumental variable show that the LM statistic rejects the original hypothesis of ‘unidentifiability of instrumental variable’ at the 1% level, indicating that there was no unidentifiability of instrumental variable. These two test types jointly illustrate that the instrumental variable selected in this study was valid and the estimation results are reliable. In addition, the estimated coefficient of Pro-index was significantly positive at the 1% level, indicating that the instrumental variable constructed was highly correlated with digital finance use and that there may be endogenous issues in the baseline model that require a second stage of regression estimation.
Endogenous discussion.
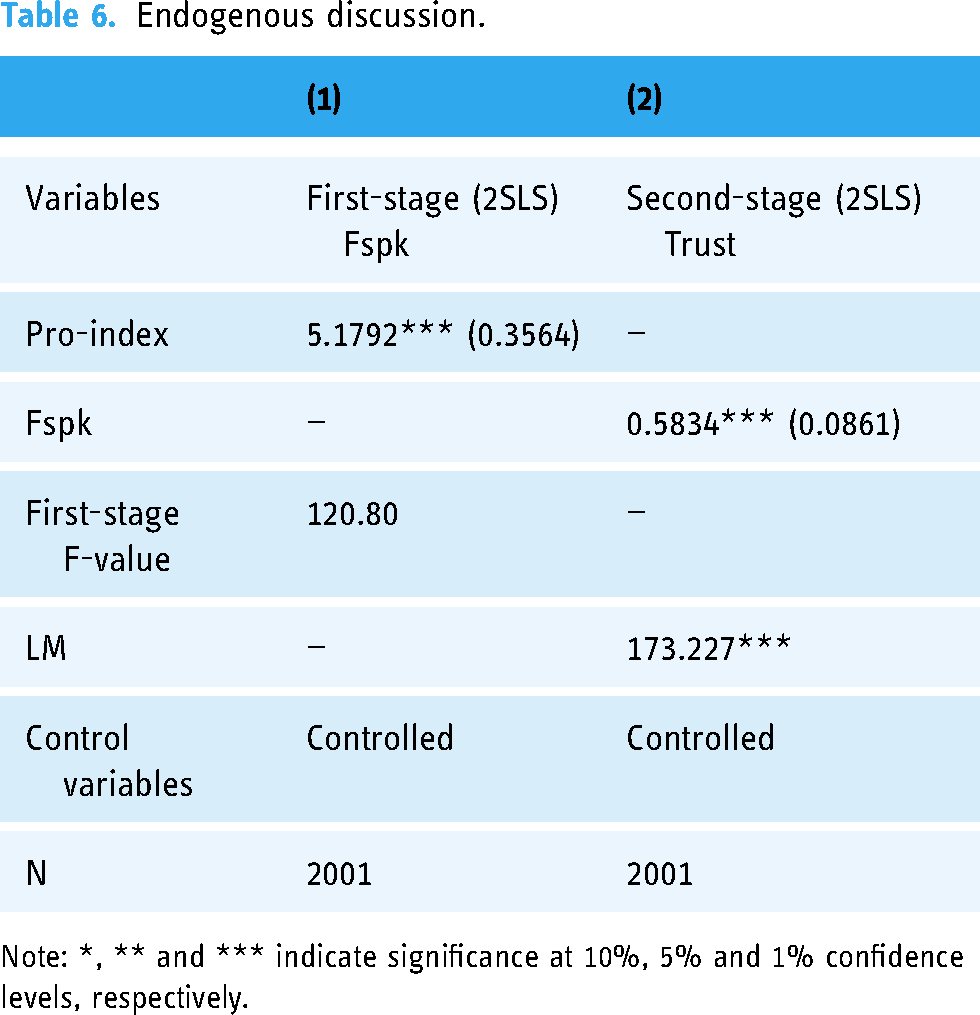
Note: *, ** and *** indicate significance at 10%, 5% and 1% confidence levels, respectively.
As shown by the estimation results of the second stage in column (2) of Table 6, the effect of digital finance use on trust of chronically ill patients was significantly positive at the 1% level, indicating that the improvement effect of digital finance use on trust of chronically ill patients still exists when considering endogenous issues, confirming the robustness of the baseline regression results. It was worth noting that the absolute values of the estimated coefficients of digital finance use obtained using the instrumental variable approach were larger than those of the baseline regression model, implying that the role of digital finance in improving trust of chronically ill patients may be underestimated if potential endogenous issues were not considered.
Limitations
While the data used in this study are nationally representative, the following shortcomings remain due to the limitations of the database. First, there is a lack of indicator measurements. Among the socio-economic indicators available for this study, online shopping frequency is the proxy variable closest to digital finance use by chronically ill patients. However, the online shopping frequency variable is a comprehensive indicator and represents multiple factors. Therefore, variables that more accurately represent the use of digital finance should be selected for testing in future studies. The digital financial indicators in this study were not related to healthcare and medical services. As the digital finance and healthcare continue to be combined, more direct measures of digital finance indicators related to medical services may emerge, which will be more conducive to estimating results close to the true value. Second, there is a lack of data on this topic. Data in the CFPS database were obtained through self-reported data from the respondents, which may introduce acquiescence, social desirability and interviewer bias.
Conclusion and recommendation
The integration of digital finance into smart healthcare is a key initiative in China's on-going healthcare and medical service reform, which will inevitably affect the environment, cognition and emotions of residents seeking healthcare. In the face of the dispute between the social capital path and the digital alienation path in terms of the effect of digital finance on individual inequities, it is necessary to clarify whether digital finance has a beneficial effect before further promoting digital finance to reform healthcare and medical services. Meanwhile, trust is not only a crucial element of healthcare and medical services but also the core of conducting transactions in the digital era, and doctor-patient trust is the basis for enhancing patients’ trust in the digital healthcare and medical service system and promoting the adoption of digital healthcare and medical services. In the context of the irreversible digital transformation of healthcare and health services, analysing the impact of digital factors on doctor–patient trust is of significant importance for promoting the establishment of a credit system for digital healthcare and medical services, as well as the digital transformation of healthcare and medical services.
Our study provides systematic evidence on the relationship between relative deprivation of income, digital finance use and trust of chronically ill patients, validating the long-term role of digital finance in helping equalize healthcare delivery and enhancing patients’ trust from the perspective of the entire population with chronic diseases. The logic of the impact of digital finance on patient trust benefits the disadvantaged populations to increase their social acceptance, understanding and resource integration capabilities. In the digital living environment, it may be best for individuals to use digital finance by the ‘trial rule’ (i.e. residents are willing to give trust) to improve their own health inequity. Meanwhile, to promote harmonious doctor–patient relationships and health equity, the Chinese government should promote the deep integration of digital finance, especially digitally inclusive finance, with smart healthcare and medical services from three aspects. First, it provides mutual assistance through digital financing. Through credit ratings and disease ratings, we create different levels of ‘credit medical’ financing services, linked to social security accounts, to help disadvantaged groups improve their access to quality care through ‘see first, pay later’ services. Second, digital financing is used to assist the entire smart healthcare system. In the future, we will build a healthcare finance cloud platform, expand the in-depth application of digital finance in the ‘prevention–medical–rehabilitation’ of patients across the healthcare and medical service and explore the potential of digital finance to help equalize healthcare and medical services. Third, digital financing enhances patient stickiness. The way forward would be to design digital finance healthcare and medical service products that are applicable to different behavioural habits, regulate the development of digital finance in the healthcare services industry and improve patients continued use of digital finance in healthcare and medical services.
Footnotes
Acknowledgements
We thank the Institute of Social Science Survey at Peking University for allowing access to the China Family Panel Studies data.
Contributorship
JL: conceptualization, methodology, supervision, writing – original draft and writing – review and editing. YL: validation, visualization, writing – original draft and writing – review and editing. LC: software, data curation, formal analysis, investigation, writing – review and editing and visualization. ZZ: supervision and writing – review and editing. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The authors are accountable for all the aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. This study received ethical review from the Biomedical Ethics Committee, Peking University (approval number IRB00001052-14010).
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article. This work was supported by Humanity and Social Science Foundation of Ministry of Education of China (grant number 22YJA630059), China Postdoctoral Science Foundation (grant number 2022T150514) and National Natural Science Foundation of China (grant number 71804101).
Guarantor
JL and ZZ.
Informed consent
I have been informed about the background, purpose, procedures, risks and benefits of the study of the China Family Panel Studies. I had plenty of time and opportunity to ask questions, and I am satisfied with the answers. I was also told to contact the China Social Sciences Research Center at Peking University (contact number 400626 1069) when I had questions, difficulties, concerns, suggestions for the study, or wanted further information or assistance with the study. I have read this informed consent form and agree to participate in the study. I know that I can withdraw from the study at any time during the study without any reason. I was told that I would be given a copy of this informed consent form containing my signature and that of the investigator.