
Abstract
Objective
To explore the knowledge, perceptions of and attitudes to digital health of Bulgarian hospital professionals in the first study of digital health in this professional group.
Methods
A paper-based questionnaire was administered to doctors, trainee doctors, nurses, midwives, and laboratory assistants working in multiprofile or specialized hospitals. Topics included the following: state, objectives, benefits, and future of digital health; data storage, access, security, and sharing; main software used; patient-held Personal Information System (PIS); and telemedicine. A total of 1187 participants from 14 hospitals completed the survey in two phases: September 2013–April 2014 and May 2015–April 2017. Data were analyzed through descriptive statistics and multilevel logistic regression.
Results
Three-quarters of participants evaluated the state of development of digital health in Bulgaria as subpar (36.0% negative; 38.9% passable; 24.5% positive). 27.2% (323) endorsed patients having unconditional access to their data. In contrast, 89.5% (1062) of participants considered it appropriate to have full access to patient data recorded by colleagues. Doctors were more likely to endorse patients having access to their data than healthcare specialists (OR = 1.79 at facility, OR = 1.77 at location).
Conclusion
The largely negative or lukewarm attitudes toward the state of development of digital health in Bulgaria are likely to result from the high number of failed projects, unmet expectations, misunderstood benefits, and unforeseen challenges. This study provides a much-needed stimulus and baseline for researching the ways in which the digital health landscape in Bulgaria has matured—or not.
Keywords
Introduction
Bulgaria's healthcare system faces globally shared problems of increasing life expectancy 1 and an aging population, 2 an increasing burden of noncommunicable diseases, 3 high levels of difficult-to-modify health-compromising behaviors,1,4 workforce challenges, 5 and, most recently, the onslaught of the COVID-19 pandemic. 6 In 2019, the country was 7th in the world in terms of population aging, with 21.3% of its citizens 65 or older. 1 Levels of pure alcohol consumption and smoking rank it, respectively, 10th and 9th in the world. 1 It has long had the highest mortality in the European Union (EU) from diseases of the circulatory system: 1075.9 vs. 370.2 EU average deaths per 100,000 individuals in 2018. 7 While the doctor-to-patient ratio is highly favorable, of 4.21 doctors per 1000 individuals, 8 ranking the country 7th in the world, 9 53.0% of doctors are aged 55 or above. 5 As of February 2023, the COVID-19 death rate in Bulgaria—of 5499 per 1,000,000 individuals—is the second highest in the world. 6
In 2018, Bulgaria had the second lowest total expenditure on health per capita in the EU-28—$690, over five times lower than the EU average of $3525. Within this, the government health expenditure was $398, the lowest amount EU-wide and ranking the country 87th in the world. 1 Bulgaria also had the highest percentage of out-of-pocket payments for health in the EU, 40.5%. 1 Nevertheless, the health expenditure per capita increased from $94 to $690 between 2000 and 2018, outpacing the increase of the Gross National Income per capita (from $1660 to $8560). 1 Bulgaria is one of the exceptions to the rule of a positive relationship between Gross Domestic Product growth and health status in postcommunist countries, along with Hungary, Ukraine, and Russia. 10
The Bulgarian healthcare system has been undergoing transformations since the 1990s, following the fall of communism. The reforms have been criticized as lacking a comprehensive plan and vision, being implemented slowly and hesitantly, neglecting the need for communication with citizens and healthcare professionals, and having an unclear legal basis and underdeveloped control functions.11–13 According to a Bloomberg report, Bulgaria had the lowest healthcare efficiency score in 2015 out of 56 economies. 14 It is incontestable that the Bulgarian healthcare system continues to need profound and rapid reform.
Digital health is defined as the range of tools based on information and communication technologies (ICT) used to assist and enhance the prevention, diagnosis, treatment, monitoring, and management of health and lifestyle. 15 It has been advanced as a foundation for the deep and rapid reform of the health sector Bulgaria needs.16,17 Empirical research from EU countries with stronger health systems has also demonstrated the capacity of digital health to accelerate healthcare transformation. 18 However, the country's adoption of digital health solutions has remained suboptimal (Supplemental Material 1).
Healthcare professionals play a key role in the adoption and implementation of digital health.
19
Bulgarian GPs have scored high (above 90%) on 3 out of 13 indicators of eHealth—GP practices receiving professional IT support, use of computers in practices, and electronic recording and storage of individual administrative patient data,
20
yet the level of adoption of eHealth in hospitals remains underexplored. To our knowledge, the present study—Bulgarian eHealth Study (BEHEST)—is the first to explore the knowledge, perceptions of and attitudes to eHealth of Bulgarian hospital personnel. It aimed to answer the following questions:
What are Bulgarian hospital professionals’ knowledge, perceptions of and attitudes to: digital health in general and in terms of its current state and expectations for the future; objectives and intended benefits; data storage, access, and sharing; security issues; and key software? How do these vary by characteristics of respondents’ workplaces and by characteristics of respondents’ demographic and professional profiles?
Methods
This was a questionnaire-based study conducted in three types of inpatient facilities and three types of location in two phases between September 2013 and April 2017. In each of the study settings, the data collected were cross-sectional.
Questionnaire design
A draft questionnaire was developed by DP based on three semistructured interviews with two doctors, a nurse, and a midwife and further discussions with a senior digital health specialist. Questions and response options generated through this collaborative work were organized in the following thematic domains:
state of development and objectives of digital health (q1 and q4); current and future storage of patient data (q2 and q3); benefits of digital health to patients (q5); patients’ and healthcare professionals’ access to data (q6 and q7); expectations concerning the future of digital health products (q8); evaluation of the main digital health software used by respondents (q9 and seven sub-questions); patient-held Personal Information System (PIS) (q10–q13); authentication and security (q14–q17); health information exchange (HIE) and telemedicine (q18–q20).
There were 27 questions in the above domains. Demographic and professional profile data were collected on the following: gender, professional group (doctor, trainee doctor, nurse, midwife, and laboratory assistant), age group (under 30, 31–45, 46–55, and over 55), length of service (1–5, 6–10, 11–15, and over 15 years), and specialty (doctors only).
Concerted effort was made to ensure the clarity and simplicity of language. Technical IT terms were avoided so that clinicians with limited interest in IT could still find the questionnaire understandable and relatable. For instance, “computer program” was preferred to “clinical IT system,” as “clinical system” was often taken to mean a system for administering intravenous drugs and fluids. The interviewees, further pilot participants (n = 20), and academic colleagues commented on several versions of the questionnaire (Supplemental Material 2).
Choice of hospitals
Our sampling framework included all “multiprofile hospitals for active treatment” (N = 181) and all “specialized hospitals” (N = 87) in Bulgaria. Specialized hospitals in the country are further subdivided into “specialized hospitals for active treatment” (N = 80) and “complex oncology centers” (N = 7). For brevity, we will hereinbelow use “multiprofile hospitals”, “specialized hospitals”, and “oncology centers.” In these institutions, healthcare professionals work with software products daily and are more likely to exchange information electronically with other units within their own organization or other settings. For further information on healthcare facilities in Bulgaria, see Supplemental Material 1.
To be eligible for inclusion in the study, an institution had to:
have a relatively mature IT infrastructure (including hospital servers, data storage servers, and PCs in a client–server network); be using clinical IT software actively or to have made recent investment in such software; be exchanging health data internally, primarily by electronic means.
The sampling approach also aimed to ensure variability in terms of location (importance and size of town/city), responsible entity (e.g. Ministry, such as of Health or Defense; municipality; a commercial entity; or a combination of these), and funding sources (public/private).
Healthcare professionals were eligible to participate if they:
worked with clinical software products; had length of service of at least 1 year; were on shift at the time of the questionnaire distribution.
Study ethics, permissions, and recruitment processes
In Bulgaria, surveys do not require approval by an independent ethics committee or an institutional review board (see, for instance, the official letter from the Minister of Health provided in response to a researcher’s query regarding a Europe-wide survey 21 ). However, the study needed a range of approvals and permissions by participating institutions, which were intertwined with the recruitment processes. These are represented schematically in Figure 1 and described below.

Stages of study in each hospital.
Since there is no centralized information on the IT infrastructure of Bulgarian hospitals, DP used the following sources to search for information on eligibility criteria: the website of eHealth Bulgaria Foundation (www.ehealth-bg.org, no longer live); expert advice; information in the mass media; and personal judgment based on the reputation, size, and financial state of a hospital (since IT projects are not reimbursed by the National Health Insurance Fund, they are typically implemented by larger hospitals).
DP then deposited, in the administrative office of each preselected institution, a study information pack to be brought to the attention of its director. Once a decision was made (variably by the director personally or at a medical council), he proceeded with arranging the practicalities around the questionnaire administration, typically with the head nurse. At an initial meeting, he explained the goals of the study and answered questions about it. The number of questionnaires needed for the different units was estimated, with the estimate reflecting all healthcare professionals in a unit perceived by the head nurse to meet the eligibility criteria. Subsequently, the head nurse introduced the study to the chief nurses of the various departments and handed out copies of the questionnaire. This mediated approach was taken primarily because of visitor restrictions at the hospitals.
Healthcare professionals returned completed questionnaires to the office of their unit's chief nurse. She then passed them on to the hospital head nurse, from whom DP collected the full set. The time between passing on questionnaire copies to the head nurse and having the completed questionnaires returned to the lead researcher ranged from 2 days to over a month across participating hospitals.
Periods of data collection
The first phase of the study ran between September 2013 and April 2014. Data were collected in four large and four small hospitals. As the primary investigator was advised of new IT projects starting in five large and one middle-sized hospital, a second phase of the study was initiated. It ran between May 2015 and April 2017.
Data entry and preparation for analysis
Data were entered in SPSS version 25.0 (IBM Corp., Armonk, NY, USA). The resulting dataset was verified against the paper questionnaires at least twice. A small number of errors were found and corrected. Questionnaires that had numerous missing or repetitive responses or, in some cases, appeared to have been filled in by the same person twice were discarded (49 such questionnaires).
The following variables were created to support the analysis:
location—capital, city, and town; staff type—doctors (fully qualified and trainee doctors) and healthcare specialists (nurses, midwives, and laboratory assistants). The aggregation of staff type was performed as the number of trainee doctors, midwives, and laboratory assistants in the sample was small.
Pilot testing the questionnaire with a 9-point Likert scale for evaluation questions showеd that respondents defaulted disproportionately often to extreme values or the midpoint. As a result, we switched to using the marking scale of Bulgarian schools (2–6), which respondents found much more intuitive. The two lowest marks (2 for “poor” and 3 for “mediocre”) were combined into a “negative perception.” The two highest marks (5 for “very good” and 6 for “excellent”) were combined into a “positive perception". The middle point (4, formally referred to as “good” in the Bulgarian marking system but having the connotations of “passable”) remained unchanged.
Data on the target population were requested from the National Statistical Institute and the National Center of Public Health and Analysis (see Table 1).
Comparison of the target and sample population by demographic characteristics, location of work, and length of service.

National data for age distribution used other age groups: <35, 35–44, 45–54, 55–64, 65–74, and 75+. 25
Samples differ from the target population—p < .001.
Percentages (number) of target population that were not included in the study—primarily mental health institutions, as at the time of the study they had no IT infrastructure whatsoever.
Healthcare staff at the Military Medical Academy are excluded from the distribution by location, as relevant data are not collected by the official statistical institutions.
Statistical methods
Statistical analyses were conducted using SPSS v25.0 and SAS v9.4 (SAS Institute Inc., NC, USA). Descriptive statistics were used to represent characteristics of respondents and distributions of responses. For five key dependent variables, multilevel logistic regression analysis (PROC GLIMMIX) was performed, exploring their relationship to respondent characteristics while accounting for clustering at the level of healthcare facilities’ type and/or location and study period.22,23 The five dependent variables concerned the benefits of digital health for patients (q5), healthcare professionals’ rights to access patient data (q7), patients’ rights to access their own data (q6), attitudes to the main software (q10), and feeling more informed and motivated by virtue of using such software (sub-questions to q9). These were considered key beliefs and attitudes concerning digital health, likely to have a powerful impact on its adoption. The use of multilevel logistic regression was driven by a judgment that the data are likely to have a hierarchical structure. The survey was conducted among healthcare professionals from three types of facility in three types of location and in two periods. Ignoring potential clustering effects could lead to drawing inaccurate inferences. 24 A χ² test was used to explore the relationship between respondent characteristics and the three cluster variables (healthcare facility, location, and period). Multilevel logistic regression was then used to investigate the relationship between respondent characteristics and dependent variables in the context of the cluster variables.22,23 Methodological detail is provided in Supplemental Material 3.
Results
Sample
Healthcare professionals from 14 hospitals, located in 7 out of 28 districts in Bulgaria, took part in the study. Eleven of the hospitals were multiprofile ones, with one of them also a military facility; two were specialized hospitals; and one was an oncology center. Eight hospitals were public, funded by the Ministry of Health and/or the relevant municipality; five were private; and one was funded by the Ministry of Defense. Five were teaching hospitals. Data from the Military Medical Academy are presented separately, reflecting facility-specific hypotheses as well as the way national data are collected.
The number of healthcare professionals who returned analyzable questionnaires was 1187, of which 578 (48.7%) were from the first phase and 609 (51.3%) from the second phase. This was out of 1379 distributed and 1236 returned questionnaires. A response rate, however, cannot be calculated, as head and chief nurses were not asked to record how many potential participants they approached, and in some cases they made further copies of the questionnaire. Respondents were 73.0% women and 27.0% men. 13.1% were up to 30 years old, 41.0% between 31 and 45, 30.6% between 46 and 55, and 15.3% over 55 years. 58.1% of respondents have worked as healthcare professionals for over 15 years. Doctors constituted 40.7% (483) of the sample; healthcare specialists were 52.6% (624); trainee doctors were 6.7% (80).
Almost two-thirds (65.7%) of participants worked in multiprofile hospitals, 17.3% in specialized hospitals (11.3% in hospitals for active treatment and 6.0% in an oncology center), and 17.0% in the Military Medical Academy. The majority (58.7%) worked in the capital, 25.4% in cities, and 15.9% in towns.
Key characteristics of the sample are presented in Table 1, mapped against features of the target population. The sample is close to representative of the target population in terms of gender of doctors (p = .948); nonrepresentative in terms of location; and undefinable in terms of representativeness for the remainder of the parameters as relevant national data, or national data using the types of categories used in the study, were not available.
Valence of perceptions: positivity/negativity around digital health
Positive/negative perceptions were elicited about the overall state of digital health in Bulgaria, the state of HIE, and the main type of digital health software participants were using. More participants evaluated the state of development of digital health in Bulgaria as negative or passable than as positive (36.0% negative; 38.9% passable; 24.5% positive). More participants had positive, as opposed to negative, perceptions of the main digital health software they used and of HIE (respectively, 28.8% vs. 21.5% and 30.5% vs. 23.2%), although lukewarm responses still dominated (respectively, 47.9% and 44.6%) (Figure 2).

Positive/negative perceptions of aspects of digital health (%; No)
Objectives, benefits, and future of digital health in general
Easy access to medical records and instant access to the results of laboratory tests were perceived as the key objectives of digital health, identified as such by, respectively, 67.8% (805) and 54.8% (651) of participants. A minority (6.4%, 76) reported being unfamiliar with its objectives (see also Table 2, T2.1). Taking the patients’ perspective, 45.1% (535) of respondents believed that patients valued the time gains around information processing, while 36.1% (428) considered diagnosis and therapy to be far more important to patients than the processes underpinning them (Table 2, T2.2).
Objectives, benefits, and the future of digital health.
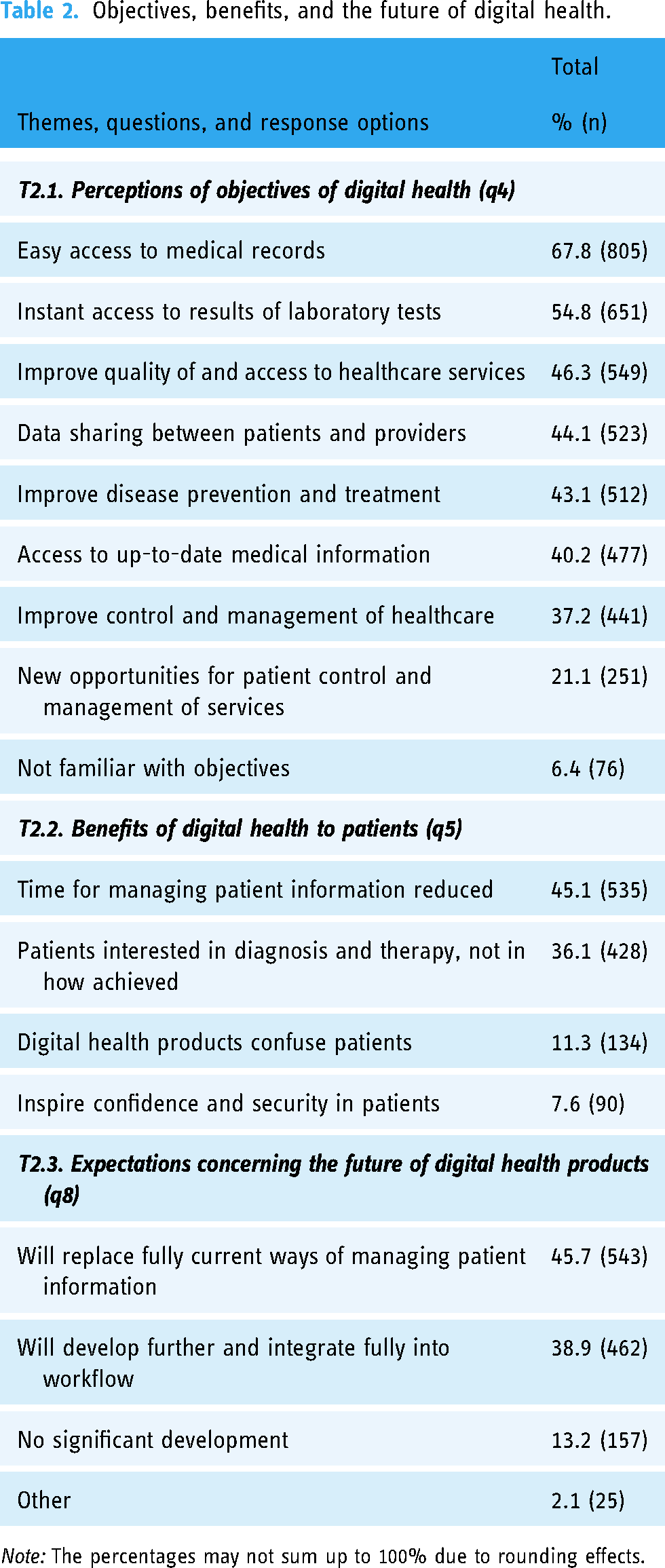
Note: The percentages may not sum up to 100% due to rounding effects.
In terms of the future of digital health products, 45.7% (543) of respondents believed that they would replace fully current ways of handling health information, while 13.2% (157) envisaged no significant future development (Table 2, T2.3).
Perceptions of the patient-held PIS
Over three-quarters of respondents (77.7%, 922) indicated willingness to use the patient-held PIS of the National Health Insurance Fund, containing information about all services provided to the patient by contracted providers. 37.3% (443) of respondents considered the information in it sufficiently reliable, while 40.4% (479) found it incomplete but useful for reference purposes. A small proportion of respondents had serious concerns about PIS: 5.4% (64) perceived its information as unreliable and 8.3% (99) as unusable. Interestingly, 58.2% (691) had not accessed their own PIS (Table 4, T4.8, T4.9).
Storage, access, and security of health information
Participants believed that the information they entered about patients was stored on hospital servers (64.1%, 761). They were also likely to express a preference for this to be the case in the future (61.6%, 731). A relatively small proportion of respondents believed that patient information was stored on the computer they worked on (15.4%, 183). See T3.1 and T3.2.
While over 77% (922) of respondents were willing to use the patient-held PIS in their practice, they were far less positive about patients having access to data. Only 27.2% (323) endorsed unconditional access, with 23.7% (281) considering it unnecessary since patients were given paper documents and 22.5% (267) believing it would overload the system and interfere with their work (T3.3). As for accessing data that other healthcare professionals had entered about a patient, 51.1% (606) indicated that it would help them make a diagnosis; 28.4% (337) indicated that it would save time and money for laboratory tests; and 10.0% (119) chose both answers (even if only one was required). 6.5% (77) did not want such access (T3.4).
60.9% (723) of participants had the data security–compromising habit of using the same password across different IT systems. Complexity of passwords showed a spread across types, with passwords of moderate strength, consisting of lowercase letters, digits, and symbols, being the most frequent (31.0%, 368); see also Table 3 (T3.5–T3.7). 58.2% (691) of respondents were worried about unauthorized access (Table 4, T4.6).
Information storage and rights of access and security.

Note: The percentages may not sum up to 100% due to rounding effects.
*While q7 required only one response, 119 respondents ticked the above two responses. An exception was made and an additional category created.
Perception of the main digital health software used (q9) and PIS (q10–q12).

Approximately two-thirds of participants (65.0%, 772) reported that using a software product facilitated their work. Just under half of them felt that they were more informed and motivated because of it (45.5%, 540). Almost half of participants (49.6%, 589) entered data after a consultation. See also Table 4.
Findings on e-signature and telemedicine are reported in Table A5, Supplemental Material 3.
Logistic regression findings
We found no impact of either type or location of healthcare facility or study period on the five dependent variables of interest (level 2 intercept was not statistically significant, Tables A1 to A7, Supplemental Material 3). After adjusting for confounding, only one of the independent variables—professional group—was found to be associated with one dependent variable. Doctors, independent of the settings, were more likely to approve of patients’ access to their data as opposed to healthcare specialists (OR = 1.79, 95% confidence interval (CI), 1.35–2.35 for type and OR = 1.77, 95% CI 1.35–2.33 for location), Tables A2 and A4, Supplemental Material 3.
Discussion
Summary of key findings
Three-quarters of participants evaluated the state of development of digital health in Bulgaria as either negative or passable. The objectives of digital health which respondents were most familiar with were ease- and immediacy-focused objectives related to their daily work (“easy access to medical records” and “instant access to the results of laboratory tests”) as opposed to broader and long-term healthcare system objectives (such as “improve disease prevention and treatment” and “improve control and management of healthcare”). Over three-quarters of respondents were willing to use the patient-held PIS. To our knowledge, the latter is the only large-scale digital health project in Bulgaria to have been successfully implemented. It has also been evaluated as a suitable foundation for the future development of an Electronic Health Record (EHR). 26 Almost two-thirds of respondents experienced the digital health software they used as facilitating their work. Overall, while participants were lukewarm to skeptical about the development of digital health in Bulgaria, most likely due to the numerous failed projects and unmet expectations (as described in Supplemental Material 1), misunderstood benefits, and unforeseen challenges, they also showed enthusiasm for specific products and appreciated their value and potential.
Patients’ unconditional access to data about them was supported by a little over a quarter of respondents. In contrast, almost 90% of respondents thought it was appropriate to have full access to patient data recorded by other healthcare professionals. While there is a need for further focused research on such attitudes, one of the likely explanations is that Bulgaria is a country with a totalitarian past, and it still bears the marks of a system where the personal space of individuals could be readily encroached upon by the state and authority figures. It is important to note that this apparent lack of respect for patients’ data privacy was also against the backdrop of practices of password creation and use that often compromised data security and relatively high levels of concern about unauthorized access. More charitably, the General Data Protection Regulation (GDPR) had not come into force at the time the study was conducted, and the response options to the data access questions themselves did not incorporate clear recognition of patients’ data rights.
Multilevel logistic regression suggested that doctors were more likely to approve of patients’ access to their data than nurses, midwives, and laboratory assistants. Again, there is a need for further research on the reliability of such findings and likely explanations for it. Potentially, doctors may feel they have greater authority to approve or disapprove of such rights by virtue of having greater authority overall. Alternatively, they may experience their notes as more relevant to patients than other healthcare professionals do.
Comparison with the literature
During the early stages of data collection for this study, Europe showed significant variability in the adoption of digital health in hospitals, with Nordic countries on the high-performing end and Eastern European countries (the region of Bulgaria) and Greece being less advanced users. 27 It remains to be seen if the impetus toward digital health arising from COVID-19 will mean Bulgaria, and other Eastern European countries, will catch up with more advanced member states, including in terms of knowledge, attitudes, and practices associated with digital health among hospital personnel.
Patients’ access and healthcare professionals’ access to patient data were identified as two out of six digital health indicators of patient-centered care in a 2017 survey of international informatics experts. 28 The survey also found that patients had full access to their hospital data in Finland and South Korea; partial access in Austria, Sweden, and the USA; and no access in Denmark and Hong Kong. Other healthcare professionals had access to patients’ hospital data in Finland, Hong Kong, and Sweden; partial access in Austria and the USA; and no access in Denmark and South Korea. 28 A Swedish study found healthcare professionals with personal experience of a new digital health service to be more supportive of patients’ online access to their health records than those without experience. 29 As far as the patients’ perspective is concerned, a pan-European survey showed patients’ support for storing health information for the purposes of improving treatment quality and preventing epidemics, resistance to it being viewed by immediate family members and home care nurses, and strong resistance to it being accessed by insurance and pharmaceutical companies and academic researchers. 30
Here we found, albeit with disclaimers about the formulation of the response options, that almost 90% of respondents felt they should have access to other healthcare professionals’ data about patients, while only 27% supported unconditional access of patients to data about their own health. It is important to acknowledge that our data are from a period that precedes both the studies summarized above and the introduction of the GDPR. Nonetheless, the findings are concerning, as this is a baseline that may be hard to change, especially in a country where doctors hold significant authority, where patients tend to be treated paternalistically, and where the debate around the ownership of patient data is not part of the normal social discourse. In their 2022 Data Protection Overview, Micheva and Koleva 31 identified no sanctions or enforcement decisions for breaches in data regulations in the healthcare sector. Relative to our findings, this is more likely to reflect lack of individual and societal attention than lack of breaches.
Strengths and limitations
To our knowledge, BEHEST is the only study on digital health in Bulgaria that explores the perspectives of hospital professionals. Its specification of digital health domains, questionnaire, and approach to recruitment can be used as a basis for future studies, with adaptations to accommodate the lessons learned. The study had a large sample size, including respondents from all three types of healthcare facilities in the country and from three types of location—the capital, cities, and towns. We applied multilevel logistic regression to account for the likely hierarchical nature of the data and thus avoided spuriously significant results. 32
The questionnaire had several limitations, primarily in terms of individual response options’ clustering phenomena that need not co-occur; response sets not exhausting the range of logical possibilities; and, at times, ambiguous phrasing. While it had received extensive feedback and was piloted with 20 participants, it was not validated. A further limitation was that data were collected through intermediaries—head and chief nurses. As a result, we could not calculate a reliable response rate. More importantly, we cannot be certain if instructions around the completely voluntary nature of the study were followed. Hierarchical distances in Bulgarian hospitals can be significant, and (tacit) pressure can be exerted even for activities that should be entirely at the discretion of a staff member. Further research is needed using different recruitment approaches (e.g. through professional unions or discussion forums) and data collection methods where the relationship between a researcher and a participant is more direct (e.g. in-depth interviews).
Implications for policy, practice, and research
In view of the scarcity of research on digital health in Bulgaria and the datedness of our findings, the primary recommendation arising from this study is for more research. Mapping live and in-progress projects and transparency about and learning the lessons of discontinued ones are also key steps in advancing digital health in the country. As Bulgaria has a small and underresourced health research and evaluation community, participation in international projects will be highly advantageous.
The Ministry of Health and the National Health Insurance Fund must introduce uniform standards for digital health products. Government support is needed for utilizing available EU funding. Healthcare professionals need further training in digital skills as well as awareness raising about the goals and benefits of digital health. Issues of ownership and access to and sharing of patient data require a broad social discussion, in addition to appropriate legislation. Good legislation has been demonstrated to increase levels of adoption of digital health. In the USA, the 2009 Health Information Technology for Economic and Clinical Health Act (HITECH) has contributed to a rise from 7.6% of the use of at least a basic digital health system in 2008 33 to 80% in 2016. 34 Hospital-specific data governance rules also need urgent attention, as well as pragmatic facilitators of secure access to data. For instance, while smart cards are used by default to give healthcare professionals access to their workplace, they are not used to enable authentication when accessing data systems. In the current day and age, the pros and cons of using biometrically enabled access to patient data also need consideration.
Beyond the country-specific implications, this study offers a striking illustration that regional legislation with implications for digital health (in this case GDPR) is implemented in the context of widely divergent preexisting practices and cultures across a region, as well as ones that can be quite distant from the spirit of the new legislation. This highlights the importance of researching country-level baselines and monitoring the implementation and impact of such legislation closely. The study also showed that general (overall negative or lukewarm) attitudes to digital health and product-specific ones can be sufficiently divergent—a reassuring observation for developers and project implementers in view of the constant need for innovation and improvement and the pipeline of new products.
Conclusions
Shortly before GDPR came into force and 4–7 years prior to the start of the COVID-19 pandemic, Bulgarian hospital professionals’ attitudes to the state of development of digital health in the country were largely negative or lukewarm. Awareness of patients’ rights in determining access to their records was minimal. Globally and in Bulgaria, GDPR has changed overall attitudes and practices with regard to data protection. Similarly, both globally and in the country, the pandemic has pushed forward a culture change in digital health. Bulgaria's healthcare system is struggling and is in urgent need of further and more effective reform. The increased and meaningful adoption of high-quality digital health tools will enable a shift toward more patient-centered care and will support the improvement of the currently poor population health indicators. It remains to be seen if the next stage of development of digital health in Bulgaria will resemble more closely the slow and disappointing reforms of its health system since the 1990s or the rapid, remarkably successful transformation of its IT infrastructure in the last decade.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076231185276 - Supplemental material for A survey of the knowledge, perceptions of and attitudes to digital health of healthcare professionals in 14 Bulgarian hospitals: First large-scale study on digital health in Bulgarian inpatient facilities
Supplemental material, sj-pdf-1-dhj-10.1177_20552076231185276 for A survey of the knowledge, perceptions of and attitudes to digital health of healthcare professionals in 14 Bulgarian hospitals: First large-scale study on digital health in Bulgarian inpatient facilities by Damyan Petrov, Mila Petrova, Irena Mladenova, Nedko Dimitrov and Galina Mratskova in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076231185276 - Supplemental material for A survey of the knowledge, perceptions of and attitudes to digital health of healthcare professionals in 14 Bulgarian hospitals: First large-scale study on digital health in Bulgarian inpatient facilities
Supplemental material, sj-pdf-2-dhj-10.1177_20552076231185276 for A survey of the knowledge, perceptions of and attitudes to digital health of healthcare professionals in 14 Bulgarian hospitals: First large-scale study on digital health in Bulgarian inpatient facilities by Damyan Petrov, Mila Petrova, Irena Mladenova, Nedko Dimitrov and Galina Mratskova in DIGITAL HEALTH
Supplemental Material
sj-pdf-3-dhj-10.1177_20552076231185276 - Supplemental material for A survey of the knowledge, perceptions of and attitudes to digital health of healthcare professionals in 14 Bulgarian hospitals: First large-scale study on digital health in Bulgarian inpatient facilities
Supplemental material, sj-pdf-3-dhj-10.1177_20552076231185276 for A survey of the knowledge, perceptions of and attitudes to digital health of healthcare professionals in 14 Bulgarian hospitals: First large-scale study on digital health in Bulgarian inpatient facilities by Damyan Petrov, Mila Petrova, Irena Mladenova, Nedko Dimitrov and Galina Mratskova in DIGITAL HEALTH
Supplemental Material
sj-pdf-4-dhj-10.1177_20552076231185276 - Supplemental material for A survey of the knowledge, perceptions of and attitudes to digital health of healthcare professionals in 14 Bulgarian hospitals: First large-scale study on digital health in Bulgarian inpatient facilities
Supplemental material, sj-pdf-4-dhj-10.1177_20552076231185276 for A survey of the knowledge, perceptions of and attitudes to digital health of healthcare professionals in 14 Bulgarian hospitals: First large-scale study on digital health in Bulgarian inpatient facilities by Damyan Petrov, Mila Petrova, Irena Mladenova, Nedko Dimitrov and Galina Mratskova in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors are particularly grateful to the managers and head and chief nurses of the healthcare settings where the study was conducted for authorizing our requests and/or for their assistance in the process. The authors would like to thank respondents for taking the time to complete the questionnaire. We would also like to thank colleagues at formal and informal scientific meetings for their commentaries, questions, and suggestions. The authors gratefully acknowledge the help of Dimitar Georgiev, PhD. Without his help and without his confidence in this work, the latter would never have been possible. He also made numerous constructive suggestions in preparing the questionnaire and analyzing the results of the pilot study. The authors would also like to thank two anonymous reviewers for their helpful and insightful comments.
Contributorship
DP led the development of the overall study design and the questionnaire design. He also secured the study approvals and permissions. DP performed the statistical analysis, following discussions with MP. DP and MP drafted all sections of the manuscript, with IM contributing to the drafting of the Results section. DP, ND, and GM conducted the literature review for Appendix 1, with MP advising on its contents and editing multiple versions of it. DP and MP drafted ![]() . DP and MP revised multiple drafts of the manuscript.
. DP and MP revised multiple drafts of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
In Bulgaria, studies of healthcare staff do not require approval by an independent ethics committee or an institutional review board. There is also no expectation of obtaining explicit consent for filling in a questionnaire. The act of choosing to fill one in or not is considered to represent such consent or otherwise.
Funding
The author(s) received no financial support for the research and/or authorship of this article. Medical Faculty, Trakia University paid the article processing charge for this publication.
Guarantors
DP and MP.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.