
Abstract
Objective
This study aimed to identify the correlation between digital capacity, health promotion participation, and active aging of older people living in rural areas in South Korea to assess the factors influencing participation in programs for health promotion and active aging.
Methods
Data were collected through a 1:1 face-to-face survey using a structured questionnaire from 13 February to 24 February 2023 during the older individuals’ visits in the senior citizen welfare centers and senior citizen centers in the region. The Measuring Digital Skills questionnaire used to assess the digital competence of South Korean individuals was employed in this study. To confirm the structural relationship between digital capacity and health promotion participation and active aging in the older population aged 65 years and older based on the collected data, a structural equation modeling analysis was performed.
Results
Active health promotion participation had a positive effect on active aging. The pathway that older adults in Korea can led to participation in health promotion and active aging in the current situation is not mainly through the digital competency whereas mobile internet skill showed positive influneces.
Conclusions
In the digital era and super-aged society, various programs are provided to older individuals to enhance the utilization of smartphones. However, education and programs for strengthening digital capacity should be organized to explain the advantages of digital use and to inform of the dangers of addiction to ensure healthy aging through social participation and exchange both online and offline.
Introduction
With an increase in average life expectancy following the advances in medical technology, improvements in transportation, and practice of safe food storage worldwide, the proportion of the older population is also gradually increasing. As a result, the global population aged 65 years and older is expected to double from 727 million (9.3%) in 2020 to 1.5 billion (16.0%) in 2050. 1 The living environment of older people is also rapidly changing due to social changes such as reduction in the birth rate, changes in household types, increase in the education level of the younger generation, and intensive migration to cities. These demographic changes are causing various problems for older people, such as an increase in the number of older individuals living alone, a decrease in social activity opportunities for older individuals, and an increase in the incidence of depression.2,3 Accordingly, the World Health Organization established the “Global Network of Age-Friendly Cities and Communities” in 2010 in preparation for the rapid aging of the global population and is forming a network with a vision to create a community suitable for older people to live in, with 1300 member cities in 51 countries currently participating. 4
South Korea is expected to enter a super-aged society and has the fastest aging population among the Organisation for Economic Co-operation and Development (OECD) countries. A super-aged society refers to a society where more than 20% of the total population is aged 65 years or older. Such an increase in the older population rate increases the number of older people living alone and the burden of primary healthcare, national insurance finance, and healthcare workers.5,6
The South Korean government launched a digital government in 2022 and announced a vision to revise the national policies and administrative tasks in accordance with the digital standards. Among them, various policies have been announced to address the problems caused by the digital divide among the older population in South Korea in line with the digital age. Although South Korea's administration and welfare programs for the older population are digitized step by step, a gap is created due to the low digital literacy of the older population, which may even lead to a sense of social alienation. 7 The South Korean government is actively promoting digital literacy education for the older population in aged care facilities, senior citizen cultural welfare centers, centers for dementia care, and senior citizen centers, centered on local governments. Such education is expected to strengthen the digital capacity of older people, increase accessibility to various health information, and encourage social participation through online communities. 8 However, there are negative effects to this as well. As the digital capacity of older people is strengthened, their time spent on digital devices is also likely to increase. Currently, as the penetration and use of smartphones among the older population increases, smartphone addiction among this population has been recognized a major social problem. 9 Smartphone addiction in the older population reduces their participation in offline social gatherings, gradually lowers social participation and social support, and eventually causes social loneliness, depression, and lethargic aging. 10 Therefore, it is necessary to study the effect of digital capacity on participation in programs for health promotion and, furthermore, active aging. Although there have been insufficient studies on digital capacity, such study is essential in line with the digital age and a super-aged society.
First, this study aimed to identify the correlation between digital capacity, health promotion participation, and active aging of older people living in rural areas in South Korea. Second, it aimed to identify the factors influencing participation in programs for health promotion and active aging. The results of this study will serve as a basis for developing digital-related policies and alternatives for older people in South Korea in the advent of a super-aged society and digital age.
Methods
Study design
This cross-sectional study determined the correlation between digital capacity and participation in programs for health promotion and active aging in the older population aged 65 years and older residing in rural areas of South Korea and to identify the influencing factors on active aging (Figure 1). This study was developed based on the research protocol for Digitally Inclusive, Healthy Aging Communities and utilized the methodology presented in that protocol. 11

Research model.
Participants
This study included older individuals aged 65 years or older living in Yeoju-si, Gyeonggi-do, and Wonju-si, Gangwon-do, South Korea. Wonju City has a total population of 360,809, of whom 56,771 are older individuals, while Yeoju City has a total population of 115,358, of whom 27,519 are older individuals. Yeoju-si and Wonju-si are urban–rural complex cities and divided into the following administrative units: dong, myeon, and ri. As a result of calculating the sample size using the G-Power 3.1 program with an effect size of 0.1, a power of 0.95, and a significance level of 0.05, the minimum number of samples required per city was 150, with a total of 300.
Data collection
Data collection was conducted through a 1:1 face-to-face survey using a structured questionnaire from 13 February to 24 February 2023 during the older individuals’ visits in the senior citizen welfare centers and senior citizen centers in the region. The survey was conducted among older individuals who agreed to participate in the survey at a place provided through the official cooperation of senior welfare centers and senior citizen centers. The survey was conducted by five surveyors who received survey training in advance and took an average of 15 minutes per respondent. We obtained informed consent in written form from all the respondents. They were also informed of their right to refuse to answer any question. During the survey, the risk factors for the identification of personal information were deleted. After excluding dropouts and participants with insincere responses, only 440 were selected for the final analysis.
Questionnaire
The Measuring Digital Skills questionnaire developed by the Oxford Internet Institute University used to assess the digital competence of South Korean individuals was employed in this study. The exogenous latent variables consisted of general characteristics and digital environment characteristics, while the endogenous latent variables consisted of mobile Internet skills, information navigation skills, communication/social network services (SNS) skills, and active aging. 12 The Cronbach's alpha was 0.813, indicating appropriate reliability for the analysis.
General characteristics. The demographic characteristics were classified as exogenous variables, of which sex, education level, age, family living status, and income level were investigated as observation variables to represent them. The education level was classified into “none,” “elementary school,” “middle school,” “high school,” and “college or higher”; age was classified into “65–74 years,” “75–84 years,” and “85 years or older.” Family living status was classified into “living alone,” “spouse,” “children,” and “grandchildren.” Monthly income was classified into “none,” “≤KRW 1 million,” “KRW 1–2.5 million,” “KRW 2.5–5 million,” and “>KRW 5 million.”
Digital characteristics. The digital characteristics were classified as exogenous variables and investigated by observing the digital use environment in terms of smartphone use and Internet use at home. Internet use at home was classified into “do not use,” “wireless Internet (mobile phone),” “wired Internet,” and “do not know.”
Mobile Internet skills. Mobile Internet skills were classified as endogenous variables; to represent them, then items “how to use digital device applications” and “tracking mobile app/Internet expenses” were observed and assigned as latent variables.
Information navigation. Information navigation was classified as an endogenous variable; five variables were assessed on a five-point Likert scale: “online search,” “previously visited sites,” “Internet search fatigue,” “difficulty in accessing the route,” and “website design.” These items were observed and expressed as latent variables.
Communication/SNS skills. Communication/SNS skills were classified endogenous variables; five variables were assessed on a five-point Likert scale: “information sharing decision,” “information sharing timing,” “appropriate comments,” “content sharing method,” and “use of contact information.” These items were observed and expressed as latent variables.
Health promotion participation. Health promotion participation was an endogenous variable; this variable was measured by answering the following question: “Have you participated in social or cultural activities at least once in the past week at your own choice?” The responses were rated on a five-point scale, ranging from one point (“never”) to five points (“always”).
Active aging. Active aging was classified an endogenous variable and measured by answering the following question, “Please rate how active you consider yourself regarding physical activity and social participation.” The participants’ responses were rated on a 10-point scale, ranging from 1 point (“not active at all”) to 10 points (“very active”).
Statistical analyses
To confirm the structural relationship between digital capacity and health promotion participation and active aging in the older population aged 65 years and older based on the collected data and identify the direct and indirect effects of this structural relationship on the use of senior citizen centers, a structural equation modeling analysis was performed using SPSS 25.0 and AMOS 21. The analysis of this study proceeded as follows.
First, Pearson's correlation coefficient analysis was conducted to determine the correlation between latent variables.
Second, exploratory factor analysis was conducted for the factor analysis of latent variables, while correlation matrix analysis was used as the principal component analysis method for factor extraction. Varimax rotation was used for factor rotation in the factor analysis. To verify the validity of factor analysis, Bartlett's sphericity test and Kaiser–Meyer–Olkin test were performed.
Third, a structural equation analysis of the latent factors affecting active aging in older individuals was conducted. Meanwhile, Spearman's correlation coefficient matrix was used as an input equation matrix of the structural equation analysis, and the parameters were estimated using the maximum likelihood method.
Fourth, a goodness-of-fit test was conducted to determine the goodness-of-fit of the structural equation model. The goodness-of-fit was evaluated using nine indexes, including the absolute fit index, incremental fit index, and parsimonious fit index; the model's goodness-of-fit was improved based on the modification index.
Finally, the direct effects, indirect effects, and total effects of the latent variables of the structural equation model were analyzed to confirm the influence of the independent variables and parameters on the dependent variables.
Results
General characteristics
This study consisted of 122 (27.5%) male and 322 (72.5%) female respondents. With regard to education level, 28.4% of the respondents graduated “elementary school,” 23.6% graduated “high school,” 23.4% graduated “middle school,” 15.9% had “none” at all, and 11.4% graduated “college or higher.” In terms of age, 42.8% of the respondents were aged “75–84 years,” 41.7% were aged “65–74 years,” and 15.5% were aged “85 years or older,” with an average age of 76.5 years.
In terms of family living status, 56.3% of the respondents lived with their “spouse,” 31.3% were “living alone,” 11.9% lived with their “children,” and 0.5% lived with their “grandchildren.” With regard to monthly income, 62.2% of the respondents answered “none.”
In relation to smartphone use, 50.7% of the respondents answered “no,” while 49.5% answered yes. In terms of Internet usage at home, 53.6% of the respondents answered “do not use”, 28.4% answered “wired Internet,” 17.6% answered “wireless Internet (mobile phone),” and 0.5% answered “do not know” (Table 1).
General characteristics (n = 440).
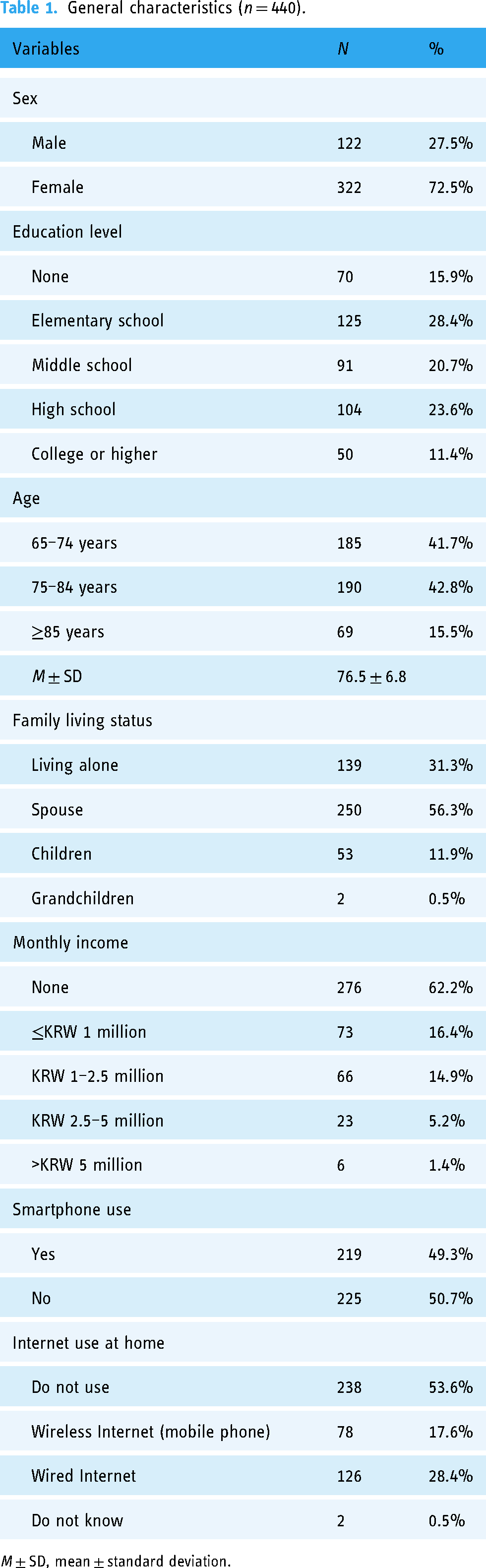
M ± SD, mean ± standard deviation.
Descriptive statistics of the observed variables
Based on the responses to the questionnaire used in this study, the means and standard deviations were 3.5 ± 2.9 of 10 points for “mobile Internet skills” and 20.4 ± 6.8 of 25 points for “information navigation.” The means and standard deviations were 10.8 ± 8.0 of 25 points for “communication/SNS skills,” 7.53 ± 3.4 of 24 points for “health promotion participation,” and 5.5 ± 2.7 of 10 points for “active aging” (Table 2).
Descriptive statistics of the observed variables.
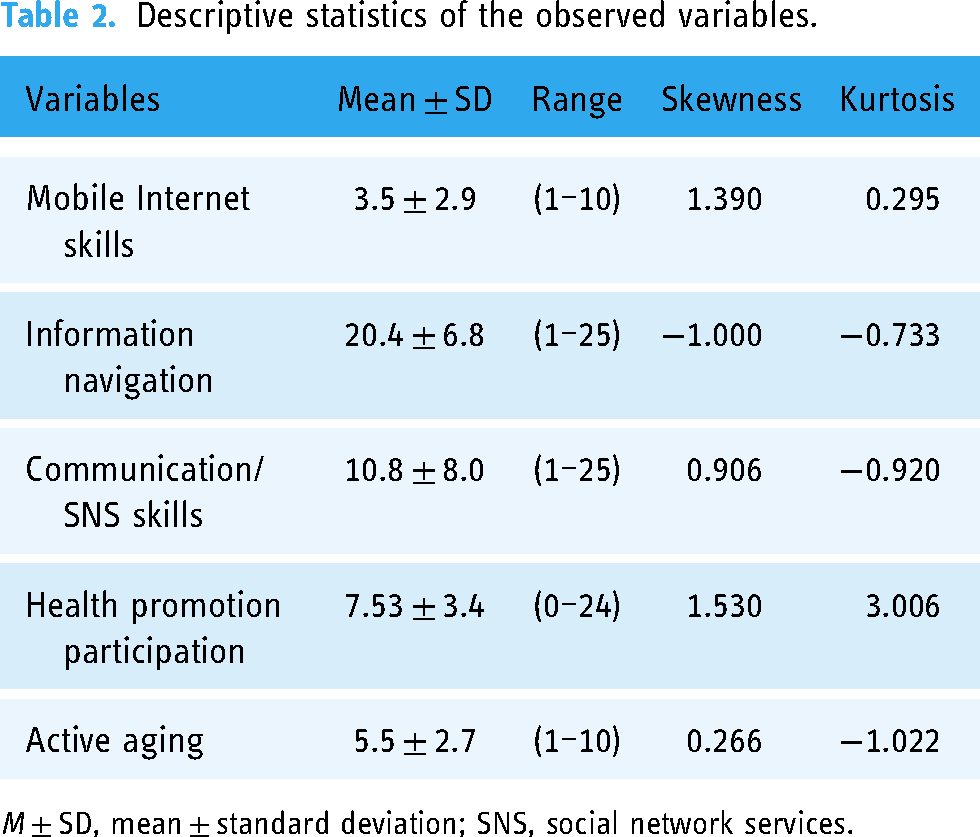
M ± SD, mean ± standard deviation; SNS, social network services.
In this study, a correlation analysis between endogenous latent variables was conducted (Figure 2). Mobile Internet skills showed a significant negative correlation with information navigation (γ = −0.84, P < .001) and a significant positive correlation with communication/SNS skills (γ = 0.86, P < .001). Furthermore, information navigation showed a significant negative correlation with communication/SNS skills (γ = −0.87, P < .001). Health promotion participation showed a significant positive correlation with active aging (γ = 0.48, P < .001).
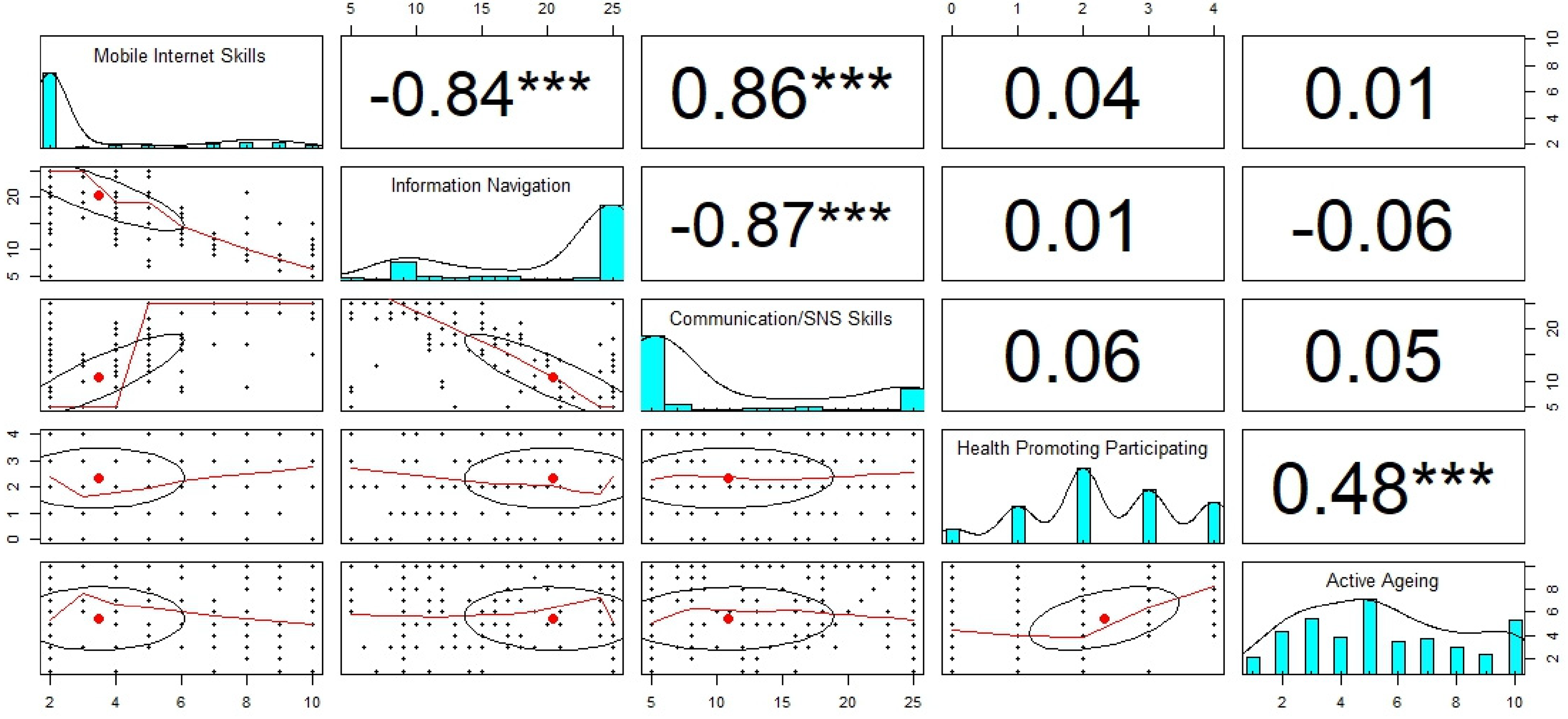
Correlation coefficients of mobile Internet skills, information navigation, communication/SNS skills, health promotion participation, and active aging.
Goodness-of-fit for model
The goodness-of-fit of the structural equation model used in this study was confirmed using the indices shown in Table 3. In the “absolute fit index,” χ2 = 10.393, P < .001, goodness-of-fit index (GFI) = 0.911, and root mean square error of approximation (RMSEA) = 0.146. In the “incremental fit index,” normed fit index (NFI) = 0.795, incremental fit index (IFI) = 0.911, and adjusted goodness-of-fit index (CFI) = 0.911. In the “parsimonious fit index,” parsimony adjusted normed fit index (PNFI) = 0.697 and parsimony adjusted comparative fit index (PCFI) = 0.711. As a result, the model was confirmed to be suitable in six of nine indices.
Goodness-of-fit of the model.
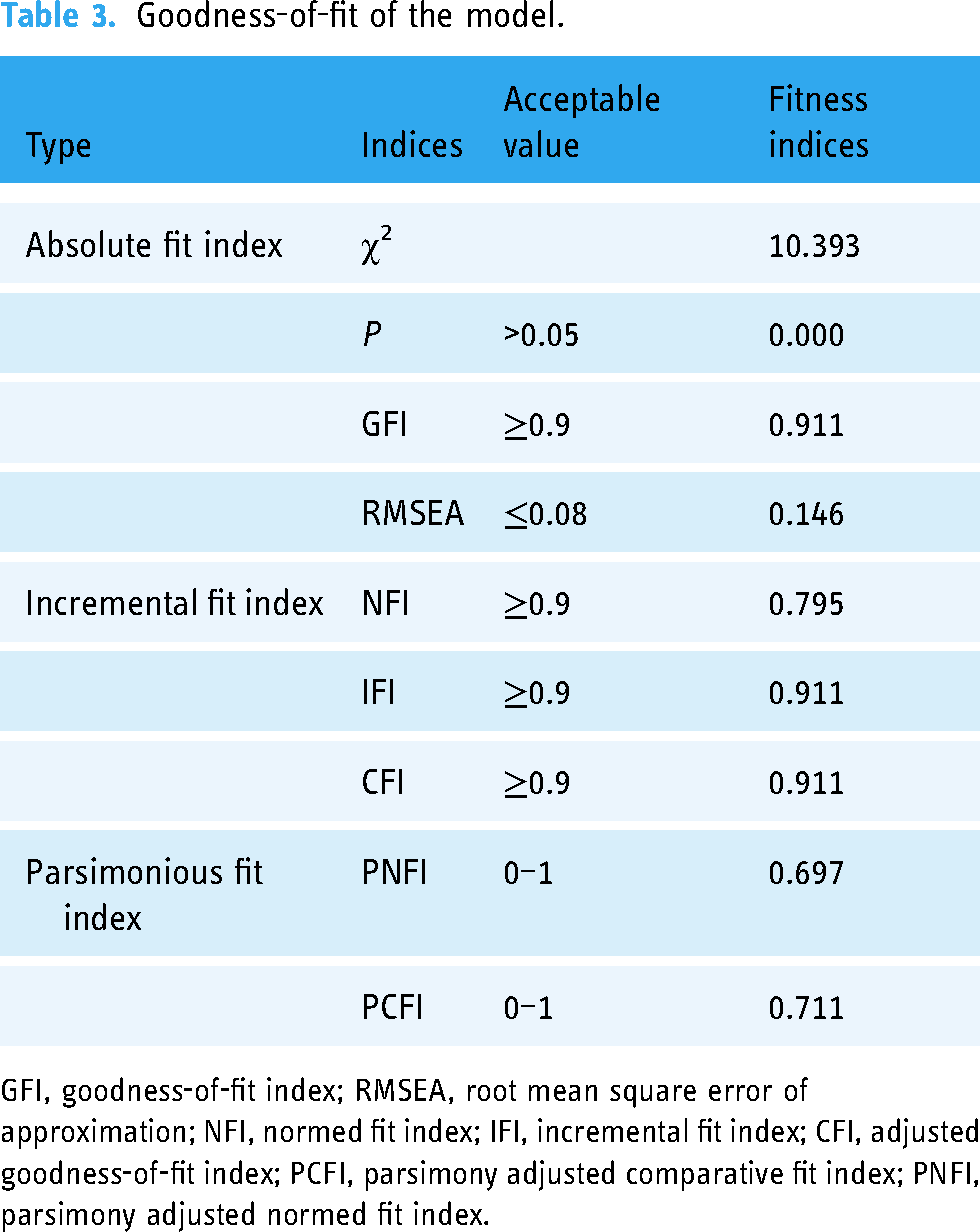
GFI, goodness-of-fit index; RMSEA, root mean square error of approximation; NFI, normed fit index; IFI, incremental fit index; CFI, adjusted goodness-of-fit index; PCFI, parsimony adjusted comparative fit index; PNFI, parsimony adjusted normed fit index.
Structural model
As a result of the analysis of the structural equation, the general characteristics had a significant positive effect on participation in health promotion activities (0.739, P < .005), and the digital environment had a negative correlation with health promotion participation (P < .01). In addition, mobile Internet and digital information had a negative effect on health promotion participation, but it was not significant.
The indicators related to digital capacity, such as the digital environment, mobile Internet, digital information, and SNS communication, had a negative effect on active aging, but it was not significant. However, health promotion participation had a strong effect on active aging (Table 4).
Standardized direct, indirect, and total effect on HPP and active aging.

NP, no path.
* P < 0.05, ** P < 0.01, *** P < 0.001.
Discussion
This study aimed to determine the correlation between digital capacity and health promotion participation and active aging in older individuals aged 65 years and older residing in the rural areas of South Korea and to identify the influencing factors on active aging.
Of older individuals included in this study, 49.3% were using smartphones. According to a previous survey, the smartphone usage rate among older individuals aged 65 years or older in South Korea was 84.2%, confirming the low smartphone ownership rate among the respondents of this study. 5 This may have been due to the fact that the survey took place in an urban–rural area and the rural area had a relatively lower smartphone penetration rate compared with that of the urban area. Majority of the study participants were women (72.5%). According to statistics, female older individuals had a lower smartphone ownership rate compared with male older individuals; moreover, the smartphone usage rate of older individuals seemed to be low due to the characteristics of rural areas.
In this study, correlation and structural equations were used to analyze the relationship between digital capacity, health promotion participation, and active aging, as well as to determine the influencing factors. First, a higher level of mobile Internet skills significantly reduced the difficulty in information navigation and enhanced the communication/SNS skills. In previous studies, the ability of older individual to communicate through the smartphone strengthened their social relationships with family and friends and improved their psychological well-being.13,14 The survey area was an urban–rural complex city with a low population density and large physical distance between households, which limited the communication due to the distance. In this environment, strengthening the digital capacity seemed to enhance the communication capacity. In addition, strengthening the smartphone capacity significantly reduced older individual's fatigue when searching online for information. A variety of online information is necessary to improve the quality of life of older individuals, such as health information and hobbies. Digital empowerment will reduce the fatigue when searching and using this information, thus allowing access to the right information. Although access to the appropriate online information is very important among older individuals, they may acquire incorrect information (infordemic) on the Internet, which negatively affects their health. 15
Second, digital capacity had a negative effect on health promotion participation and healthy aging. According to a recent study conducted by the National Information Society Agency, as the penetration rate of smartphones increases, smartphone use among older individuals increases. As a result, smartphone addiction among older individuals has become a social problem. 16 Appropriate smartphone use by older individuals enables them to search for and use various types of information, such as correct health, economic, and weather information, resulting in an increased life satisfaction among this population. 17 However, the digital capacity required for these activities reduces social participation, and the low level of social participation among older individuals with high digital competency cannot be overlooked. Such online activities lead to a reduction in social activities and a deterioration of offline relationships. This problem can increase the likelihood of depression, social isolation, and inactivity among the older population. 18 Such low health promotion participation affects active aging.
Third, more active health promotion participation had a stronger correlation with active aging. In fact, previous studies reported that older individuals who actively participate in the society are mentally and physically healthy.19,20 The results of this study also showed that more active health promotion participation led to more active aging. This suggested the need to actively encourage health promotion participation. Recently, South Korea has launched a digital government and is preparing for an aging society using the digital platform. In particular, programs and information for older individuals are produced and provided through digital platforms, with increasing frequency. For example, South Korea's Central Dementia Relief Center provides programs to older individuals through tablet personal computer (PC) and virtual reality (VR) devices to improve their cognitive function and encourage their participation.
Due to the acceleration of aging, the digital divide has become an important societal issue in worldwide. Especially according to previous research, the digital divide is known to be closely related to disparities in elderly health. 21 Furthermore, we identified a connection between the digital divide and healthy aging. To address this digital disparity among the elderly, solutions are needed from various perspectives, including national-level interventions, combined efforts of medical services, and the local community.
This study has some limitations. First, this was a cross-sectional study, which cannot establish the causal relationship. Although the analysis has been conducted using the structural equation, further investigation of the causal relationship through a panel survey should be conducted in future studies. Second, this study only included older individuals living in rural areas; therefore, its results cannot be generalized to the entire population of South Korea. Therefore, future studies should select and analyze a group of participants that can represent the population nationwide to enhance the generalizability of the study results of older individuals in South Korea. Third, this study is a face-to-face survey, with the possibility of non-sampling surveys occurring during the survey. In particular, since different surveyors conducted the survey in the two regions, non-sampling error between the two regions may have occurred. Fourth, this study was conducted to the digital capabilities by collecting the survey. In Korea, where the smartphone usage rate is very high among OECD countries, it is necessary to focus on the research of smartphone capabilities for the elderly in the future. Finally, there are areas where the model does not fit perfectly. The RMSEA value of 0.146 is higher than the preferred threshold of 0.05 or 0.08, suggesting that the model could be improved in terms of its ability to explain the variance in the data. Additionally, the NFI value of 0.795, while acceptable, is below the commonly recommended threshold of 0.90, indicating room for improvement in the model's incremental fit. The our model demonstrates a good fit in indices; the areas of less-than-perfect fit are invaluable in identifying opportunities for further research and model refinement.
Conclusions
This study investigated the correlation between the digital capacity of older individuals aged 65 years or older living in rural areas of South Korea and health promotion participation and active aging, as well as the influencing factors. As a result, active health promotion participation had a positive effect on active aging, and older individuals with higher digital competency had lower health promotion participation and active aging index. In other words, a higher digital competency leads to lower social participation and, consequently, a lower active aging index. Higher digital competency has positive effects, such as easier access to quality information and active online communication, but it also has negative effects, such as smartphone addiction causing depression. In the digital era and super-aged society, various programs are provided to older individuals to enhance the utilization of smartphones, such as strengthening digital literacy and digital capacity training. However, education and programs for strengthening digital capacity should be organized to explain the advantages of digital use and inform of the dangers of addiction to ensure healthy aging through social participation and exchange both online and offline.
Footnotes
Acknowledgements
The authors would like to thank DIHAC Global Research Team for his assistance and guidance in this research.
Contributorship
H.L., M.N.A., and E.W.N. researched literature and conceived the study. H.L., H.K.N., B.Z., M.N.A., Y.K., and E.W.N. were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. H.L. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of Juntendo University approved this study (REC number: E22-0057-M01).
Funding
This research was supported by “Regional Innovation Strategy (RIS)” through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (MOE) (2022RIS-005) and the Japanese Ministry of Education, Culture, Sports, Science and Technology, Grant-in-Aid for Scientific Research (21H00795), Digitally Inclusive, Healthy Ageing Communities (DIHAC).
Guarantor
E.W.N.
Appendix 1. Exogenous/endogenous variables

| Exogenous/endogenous variables | Questions | Scales |
|---|---|---|
| Mobile Internet skills | I know how to download and install applications on mobile devices. | 1–5 |
| I know how to keep track of the costs of mobile application use. | 1–5 | |
| Information navigation | I think it is hard to decide on the best keywords to use for online searches. | 1–5 |
| I find it hard to find websites I’ve visited before. | 1–5 | |
| I get tired when looking for information online. | 1–5 | |
| Sometimes I end up on websites without knowing how I got there. | 1–5 | |
| I find the way in which many websites are designed confusing. | 1–5 | |
| Communication/SNS skills | I know which information I should and should not share online. | 1–5 |
| I know when I should and should not share information online. | 1–5 | |
| I am careful when making comments and only show behaviors that are appropriate to the situation I find myself in online. | 1–5 | |
| I know how to change who I share my content with (e.g., friends, friends of friends, or public). | 1–5 | |
| I know how to remove friends from my contact lists. | 1–5 | |
| Health promotion participation | Have you participated in social or cultural activities at least once in the past week at your own choice? | 1–5 |
| Active aging | Please rate how active you consider yourself regarding physical activity and social participation. | 1–10 |