
Abstract
To describe the process of engagement in information seeking behavior for individuals with type 1 and type 2 diabetes.
Methodology
Constructivist grounded theory. The data was gathered through thirty semi-structured interviews of participants attending a wound care clinic in Southeast, Ontario, Canada. The waiting period taken to seek appropriate help varied from weeks to months.
Results
“The processes of engagement in information-seeking behavior about diabetes” are organized as follows: 1) discovering diabetes, 2) reactions to the diagnosis, and 3) engaging in self-directed learning. For most participants, the diagnosis of diabetes was unexpected and usually confirmed after a long period of experiencing a diversity of symptoms. The terms used mostly by participants were “I started to wonder” and “Something was wrong with me.” After being diagnosed with diabetes, participants sought information to learn about it. Most of them engaged in self-directed learning to acquire knowledge about their illness.
Conclusion
Although the Internet is often used to seek information, healthcare providers and support network also played an important role in supporting participants information-seeking behavior learn about diabetes. The unique needs of people with diabetes must be taken into consideration during their diabetes care journey. These findings call for the need to provide education about diabetes from the time they are diagnosed and direct them to reliable resources of information.
Introduction
Diabetes mellitus (DM) is a complex, chronic condition that requires high-quality clinical care.1,2 Its prevalence has been increasing progressively over the years: in 2014, an estimated 422 million adults worldwide had DM; and in 2019, approximately 1.5 million people worldwide lost their lives to the disease. 3 Consequences of DM include blindness, kidney failure, heart disease, stroke, and lower limb amputation. 3
Nonetheless, people with diabetes play an important role in preventing its poor outcomes by performing daily self-management practices such as monitoring blood sugar and making good decisions about diet to regulate their glycemia.4–6 Additionally, they also need to inspect their feet and keep them clean, hydrated, and dried to avoid foot ulcers. To be able to implement such practices, those with diabetes must acquire knowledge about their illness, how to manage it, and develop the ability to seek and search out correct information 7 to self-manage appropriately and confidently. They must learn how to include some sources and channels of information and discard others. 8 Moreover, seeking good information is paramount to improving their ability to cope with early diagnosis and the impact of diabetes on their daily routine. Finally, the ability to find and apply information can help patients to improve their knowledge and confidence about the complexity of diabetes.
While information-seeking behavior is defined as the different ways individuals seek, interact with, and utilize information,8,9 investigators have proposed diverse models for characterizing various aspects of information-seeking behavior.9,10 A well-known model called Wilson's model explains four different types of information-seeking behavior: 1) passive attention, 2) passive, or 3) active searching, and 4) ongoing exploration. Passive attention is when individuals obtain information without anticipating looking for it (e.g., social media ads). In contrast, passive searching is when individuals find pertinent information while looking for other areas of the source. This type of information-seeking behavior frequently leads the individual to active searching, ‘the principal mode’ in the process of seeking more information. Therefore, this type also engages the individual as an active information seeker.
The ongoing search for information about a disease is usually performed during a need to reach satisfaction and to update or expand current information. 9 A recent systematic review identified five types of information-seeking behavior among people with diabetes that included passive and active search. 11 Researchers have highlighted the central role of information seeking and acquisition in enabling individuals to cope with early diagnosis and the ongoing impacts of disease in many areas of their life. 12 However, the number of studies examining information-seeking behavior among individuals with diabetes is scarce.8,13 Also, a search of current literature does not reveal published studies of information-seeking behavior in individuals who developed a diabetes-related complication.
While a few qualitative studies have explored the information-seeking behavior of individuals with diabetes, 11 none of them have investigated the process by which these individuals engage in information-seeking behavior. This investigation would be relevant to inform clinicians, diabetes educators, and other professionals on how to support individuals with diabetes to cope with and learn the skills they need to manage diabetes and prevent its complications. Therefore, the objective of the present study was to examine the process of engagement in information-seeking behaviors for individuals with Type 1 and Type 2 diabetes who developed diabetic foot ulcer.
Methodology
Study design
We followed a constructivist grounded theory (CGT) study research informed by Charmaz and symbolic interactionism. CGT was chosen because it aligns with the authors’ philosophical assumptions that view individuals in society as active subjects working collectively and sharing experience to reconstruct their world and realities. Additionally, CGT denies the existence of objective reality and acknowledges subjectivity as inseparable from social existence.14,15 Another reason for using CGT is that it provides a flexible guideline for data collection and analysis to develop a theory grounded in data 16 and allows researchers to be in constant involvement in the construction and interpretation of data by stressing social contexts, interaction, sharing points of view, and interpreting understanding.14–17
Our CGT was rooted in symbolic interactionism, 18 which offers to grounded theorists an open-ended theoretical perspective that can inform grounded theory studies. 16 Symbolic interactionism assumes that interaction is inherently dynamic and interpretive and therefore addresses how people create, interpret, endorse, and alter meanings and actions in their life.16,19 This framework facilitated our understanding of how participants’ present experiences (i.e., having an active diabetic foot ulcer [DFU]) are informed by interpretations of the past (e.g., receiving the diabetes diagnosis and seeking information to learn about it).
Study participants
Thirty individuals with diabetes who developed diabetic foot ulcers and were attending a wound care clinic in southeastern Ontario, Canada, were invited to participate in individual interviews from April to August 2017. Table 1 provides a summary of participants’ demographic characteristics.
Socio-demographic characteristics of study's participants.

Participants were selected through purposive and theoretical sampling. Purposive sampling was used to identify participants who met the following criteria: 1) a confirmed medical diagnosis of a DFU for a minimum of two months, which ensured adequate experience to reflect on the process of taking care of DFU; 2) age 18 years or older; 3) able to speak and read in English comfortably and articulate their experience of having DFU; 4) willing to engage in active self-reflection and self-disclosure about their experience of living with and managing DFU. Ethics approval was obtained from the Queen's University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (TRAQ IRB#6020520) before recruitment, as was informed consent by participants. We ensured confidentiality by using pseudonyms instead of participants’ real names.
Procedures
Data collection involved a variety of methods (i.e., intensive interviews, memo writing, field notes, and the researcher's journal) to provide robust and reliable data to develop this theory. Semi-structured interviews were conducted until no new properties of the patterns emerged. Interview lengths ranged from 36 min and 41 s to one hour and 42 min. Interviews were entered into N-Vivo© (Version 11.4.1), and audiotaped interviews were transcribed verbatim by a professional transcriptionist and verified for accuracy by the first author. Table 2 provides a few samples of the questions used in the interview guide.
Overview of questions and prompts used in the interview guide.

Data collection and analysis
In our study, data collection and analysis occurred concurrently in a cyclic research process that began with initial coding and continued to focused coding. The coding phase involved the following hierarchical phases: 1) an initial phase (open) line-by-line coding, and 2) a focused phase (selective and conceptual coding). The initial phase generated a total of 529 codes identified by action or in vivo words as recommended. We used focused coding (second phase) for the second stage of analysis to explain more substantial segments of data. During this phase, some redundant codes were collapsed into categories. Therefore, about 120 codes were grouped into the three phases/categories and three concepts of the theory. We used memo-writing and field notes to support coding, description, and interpretation of date and the development of categories/phases toward generating a substantive theory. We finished data collection when theoretical saturation was accomplished. In our study saturation occurred when themes and sub-categories in the data became repetitive and redundant such that no new information could be gathered by further data collection. To ensure the usefulness and quality of this grounded theory study, we followed the five criteria suggested by Charmaz 20 : 1) credibility (provided a transparent internal and external audit of the analytical methods); 2) originality (relied on the analytical insights grounded in data to develop the substantive theory); 3) confirmability/validity (followed up with each participant to confirm if the summary of findings was an adequate understanding of their experience); 4) resonance (included what is meaningful about the substantive area and described the fullness of participants’ perception about the impact of DFU on their lives); and 5) usefulness (identified key messages drawn from participants’ experiences useful to clinical practice and policy).
Results
The components of the theory are comprised of three phases, their respective categories, and a set of concepts (Figure 1). The three phases of the theory titled “The processes of engagement in information-seeking behavior about diabetes” are organized as follow: 1) discovering diabetes, 2) reactions to the diagnosis, and 3) engaging in self-directed learning. After being diagnosed with diabetes, participants had different reactions and engaged mostly in active and ongoing searching to learn about a disease they knew nothing about. Participants engaged in three types of self-directed learning approaches that became concepts of the theory: 1) searching on the Internet; 2) Learning from support networking; 3) learning while living with the disease. Table 3 depicts an outline of the categories (phases of theory), concepts, and notable quotes.
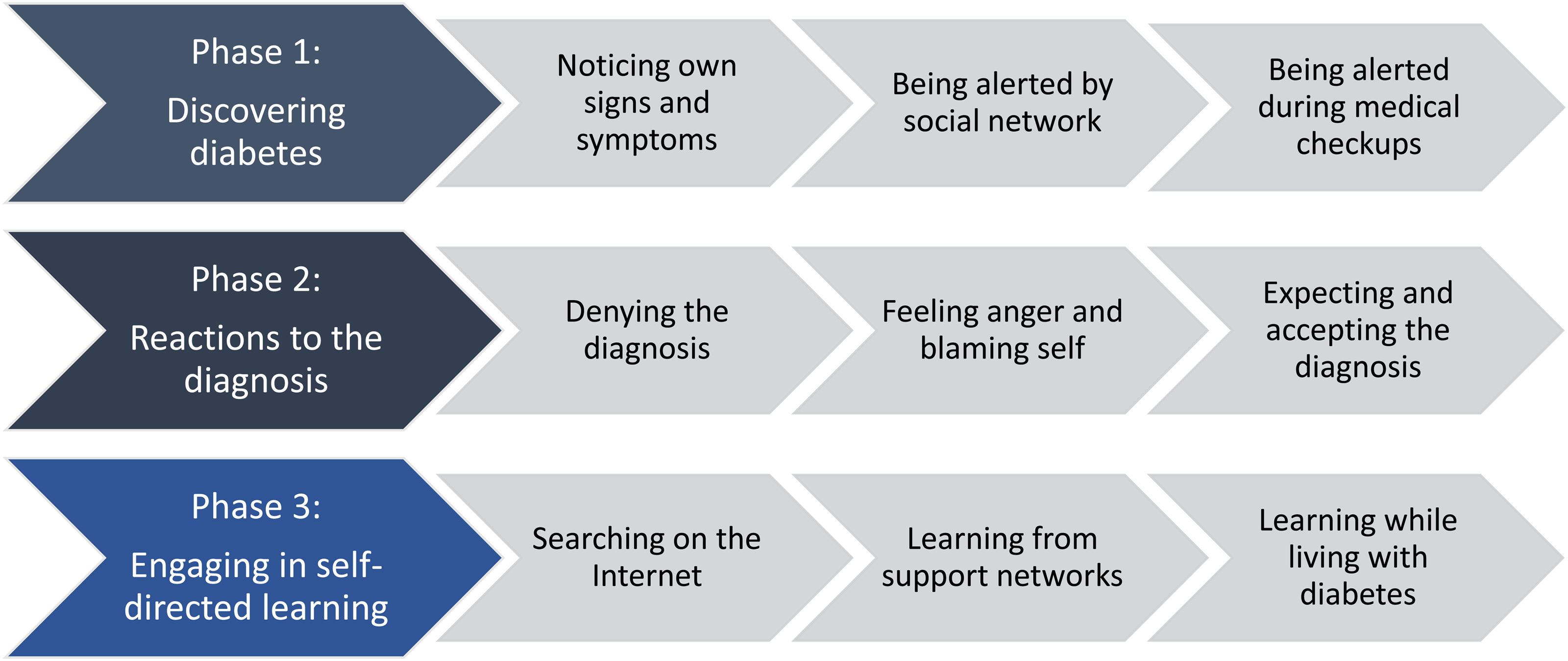
Theoretical model representing the processes of engagement in information seeking behavior for individuals with diabetes who developed DFU.
Summary of phases, categories, concept and supporting quotes.

Phase 1: discovering diabetes
The discovery of diabetes through a formal diagnosis was the first phase of the process of engagement in information-seeking behavior (Figure 1). The majority of participants were living with diabetes before being aware that they had the disease. Three concepts emerged in this phase: Noticing one's own signs and symptoms of diabetes, being alerted by a social network, and being alerted during medical checkups.
While some participants presented a variety of symptoms such as increased thirst and hunger, dry mouth, frequent urination, unexplained weight loss, fatigue, blurred vision, tiredness, and insomnia, others did not present any symptoms and continued to live with their regular routines and lifestyle. The terms that participants mostly used were “I started to wonder” and “Something was wrong with me.” For instance, before doing blood work to confirm the diagnosis of diabetes, Anita was wondering why she was often thirsty and urinating frequently at night: I started to wonder about it a little bit because I found out I was getting up to the bathroom at night and I was thirsty and I thought, ‘I wonder.’ So, when I went to see my family doctor, I said, “‘You know, let's do a random blood sugar and see what it is. ‘ Well, it wasn’t too bad then, but when I went back the next time, it was higher and that was three months…So, that was I’m gonna say, probably six years ago when I was first diagnosed. And in my family, there are … My one brother has it.
Similarly, Finn also experienced some diabetes symptoms and thought something was wrong with him and decided to contact his practitioner:
I started urinating very frequently. Then I thought there was something wrong. I couldn’t go about two hours without having to urinate, so I ended up calling the doctor. I came in and they did a test and determined that I was diabetic. By the time I was, I think I was 46 or 47 years old when I got diagnosed with it, which didn’t seem to be a surprise with the family because so many of them had it.
The lack of knowledge about diabetes may have prevented these participants from taking immediate actions to prevent health issues related to unregulated diabetes. For example, Pretty Lady received her diagnosis and continued having the same lifestyle that eventually affected her blood sugar level. She only came to realize that the diagnosis of diabetes was true only after three months from time her blood sugar was checked for the second time and showed a higher level than before.
In some cases, signs and symptoms of diabetes were noticed by a lay person such as a neighbor or family member as evidenced in Charlette's retelling: Well, first of all, I was going to the washroom constantly and then, my neighbor said,‘Let me check your blood sugar.’ Her husband was a diabetic and she checked my blood sugar and it was 29, and she said, ‘You know what? I think you should go to the hospital.’ I said, ‘Man …’ and she said, ‘No, I’m serious.’ So I got in the car and drove to the hospital. My urine was black and they took my blood sugar there and it was 31. That's how I was diagnosed with diabetes.
Pretty Lady recalled that a family member noticed signs and symptoms of diabetes:
I was sleeping all the time and drinking water. Then, I’d get up and, not even an hour later, I felt so tired I had to go and lay down again. I was just really tired a lot. My husband at the time, his grandmother, her husband had it. She said, ‘You better go see a doctor,’ because that's what she thought it was, too, because her husband had diabetes and that was one of the signs.
There were also situations in which participants experienced no symptoms until a healthcare provider diagnosed diabetes during check-ups or hospitalizations for treatment of a different health issue. For example, Grumper was having medical check-ups during his military career when his diabetes was diagnosed: Okay, I was in the military at that time so I was in my 50 s I guess. I can’t remember why I ended up … Well, we have medical check-ups every year so I was diagnosed, I guess, that I had diabetes from military doctors.
Toby was diagnosed accidentally during a medical assessment for acquiring his driver's license: Well, I just went for my physical (referring to the medical assessment) for truck driving. And they do my blood sugar and urine tests and whatever, and there was sugar in my urine. That's how that was. In such cases, participants having no obvious symptoms of diabetes were diagnosed accidentally.
As noted in this phase, diabetes symptoms showed up progressively for most participants. Anita and Finn perceived some changes in their body and quickly looked for medical help to confirm the expected disease. However, Charlette and Pretty Lady were not able to link the signs and symptoms they were experiencing to diabetes. In their cases, a social network (e.g., friends or family members) played an important role in warning them about diabetes and led them to seek medical assistance. On the other hand, some asymptomatic participants such as Grumper and Toby did not receive a warning from the body signaling them that something was wrong and that they should react to it immediately. These asymptomatic individuals accidentally discovered they had diabetes only during a medical appointment for different health concerns.
Phase 2 - reactions to the diagnosis
The second phase of the theory was reaction to the diagnosis (Figure 1). In this phase participants described a variety of feelings and reactions after discovering they had diabetes that coincide with some stages of Kübler–Ross's grief theory. 21 The following concepts emerged from their reactions: Denying the diagnosis, feeling anger and blaming self, and expecting and accepting the diagnosis. (Table 2)
Many participants described their reaction as surprise, anger, and confusion. For instance, Grumper showed anger, blamed himself, and questioned the Lord: What I didn’t understand is how I got it. And I’ll never know really how … it was my lifestyle, I think, and drinking and eating habits. I really question why do I have it, but why me Lord?
Although Grumper has had diabetes for over 25 years, he still faces the challenge of accepting his disease. Grumper's mind constantly spins around questions to help him to understand why he has diabetes. His big question to which he does not know the answer is: Why do I have it, but why me, Lord?
On the other hand, Maverick blamed himself and his lifestyle. His family history of diabetes associated with a lack of information about disease management led him to think that diabetes was inevitable no matter what he did to avoid it and therefore he did not try to adopt a different lifestyle to avoid it:
My reaction? I think I thought it was inevitable because my grandfather had it and my father had it. I thought that, no matter what I did, I would probably get it. However, that's probably not true, the lifestyle I led, the extra weight, everything else, because my siblings don’t have it. They have different lifestyles than I do. Though I thought it was probably inevitable and didn’t work hard enough to avoid it, now I wish I would have.
Similarly, the diagnosis of diabetes did not surprise Barbara as she was expecting it because her mother had diabetes, which made it easy for her to accept the disease. However, Barbara's misunderstanding of diabetes also led her to think that it would be unavoidable for her to get diabetes, which made her not make any effort to avoid or delay its onset. I knew I was going to get it, because my mom had diabetes. When I was a kid, I didn’t bother taking it seriously, because I understood that my mom had diabetes very badly and I would end up having it probably, too. I didn’t bother paying attention to that. It's almost like I grew up some.
Participants such as Maverick and Barbara who knew about their family history of type 2 diabetes were expecting the diagnosis and more prepared to accept it than others. They thought that having a close relative with diabetes would lead to the unavoidable diagnosis. However, after understanding how to prevent diabetes, Maverick showed regret for not changing his lifestyle to avoid or delay diabetes. By contrast, Barbara seemed comfortable with the fact of having diabetes because she grew up watching her mother who had the disease. In this study participants such as Maverick and Barbara who had a family history of diabetes perceived it as something inevitable and therefore ignored adopting a healthier lifestyle even after getting the formal diagnosis.
Bob's lack of knowledge about diabetes led him to think that diabetes was not a “big deal” and to compare it with an infectious disease that could be cured:
Well, I said, ‘I have no idea what they’re talking about. I still didn’t really know what it was. Just, ‘So I got diabetes, big deal. No different than a cold or a flu or something like that.’ You know? ‘It’ll go away in a couple days.’ Didn’t go away in a couple days.
Other participants had different reactions. Barbara was upset about her diagnosis because she thought she needed to give up eating things she likes: I wasn’t too happy about it, because I love chocolate and I love Coca-Cola and I thought I’d have to give it up. I was really upset over that idea.
Other participants engaged in a fighting against diabetes and had difficulty accepting the diagnosis. It was difficult for Dave and Pretty Lady to accept their diagnosis because they were young when they were diagnosed with type 1 diabetes and suddenly needed to learn how to take care of themselves: It's hard to accept because you’re different than you’re used to. I wasn’t used to being … having to look after myself. I was used to doing what I wanted to do, but then I had to start a diet, I had to watch what I was doing. I had a … for 11 years old, and it's hard to accept that when you’re 11 years old because you can’t do the same things as your friends (Dave).
It was like, back then, you didn’t know anything about it, where it's more open now. I’m aged, but back then I was 19. I didn’t know anything about it. Well, it was very uncomfortable. You’re just like, “What kind of disease is this?” They put me in the hospital right away to put me on insulin to get things under control. After learning about it I was shocked, because nobody in the family ever had it. It was kind of shocking (Pretty Lady).
Participants with type 1 diabetes, such as Dave and Pretty Lady, discovered diabetes when they were still young. Therefore, it was difficult for them to understand the disease, make changes, and adapt to a new lifestyle to control diabetes. How much did this discovery affect their life? It was not easy for them! Pretty Lady was young and wondering about this “kind of disease.” After learning about it she was “shocked” because she thought there was no family history associated with diabetes. While Dave needed to watch everything he was doing, he felt controlled by diabetes and had difficulty in accepting his diagnosis.
Phase 3 - engaging in self-directed learning
The last phase of the theory describes the information-seeking behavior after participants realized they needed to learn more about diabetes (Figure 1). Most participants shared that they received limited information from their healthcare providers or had limited access to formal diabetes education. After perceiving the need to acquire information to learn more about diabetes, participants engaged in three self-directed learning approaches that comprise the concepts of this phase (Table 2): 1) searching on the Internet, 2) talking to support networks, and 3) learning while living with diabetes.
Participants who attended diabetes class were usually passive subjects when it came to learning about controlling blood glucose levels as they struggled to adhere to a diet and maintain regular exercise. For example, Allan explained that when he was diagnosed, he did not have enough access to information about appropriate diet, drinking, and exercising, a lack that led him to make many mistakes. Back then, when I was diagnosed, I guess I was semi-taking care of a diabetic diet. I got information, okay? Stay away from sweets. They never talked about … I don’t recall them talking about exercise or the importance of exercise, which … How can I put it? To be a successful diabetic, you have to walk a fairly narrow path that is just generally good for staying healthy as a normal human being. Diet, exercise, sleep, drinking, all of that other stuff, and controlling blood sugar. The best way to put it is, when I was first diagnosed, I didn’t get much information and I made a lot of the mistakes just simply through ignorance.
Similarly, Pretty Lady stated that when she was diagnosed with (type 1) diabetes she needed to be hospitalized for about two weeks where she just learned a few things about diabetes monitoring and treatment.
Well, it was very uncomfortable. You’re just like, Diabetes? What kind of disease is this? They put me in the hospital right away to put me on insulin to get things under control. I was there for about two weeks, where I think that a lot of times now, I think they do just home visits and stuff to teach you all that stuff, where, back then, it was different. As I say, it seemed like it was something new. Well, it was totally new to me.
She also attended diabetes class in the beginning but stated that what they highlighted was to pay attention to what she ate: Nothing else, in the diabetes class they just said, ‘Watch what you eat.’ That was about it. As I say, I haven’t seen a dietician in years.
Participants’ narratives showed evidence that they were not prepared to live with and manage diabetes. They did not know what diabetes was; therefore, they did not know how to manage this multifaceted chronic condition from the beginning. Most importantly, they did not know that unregulated diabetes could lead them to complications and disability such as DFU and amputation. How could they have avoided such poor outcomes of diabetes? Pretty Lady's mind was constantly spinning around the question: What kind of disease is this? She was admitted for four weeks to the hospital to control a disease that she did not know anything about, and therefore that hospitalization did not make sense to her.
Janet explained that she is always on her computer and she would use the Internet to find information about diabetes or medications prescribed for her:
I am on the computer usually every day and I learned most about diabetes on the Internet. If I wanna know something about diabetes, about my symptoms or about my medications…for example if they put me on a new prescription, I Google it, because I wanna know like can it react with my heart meds?
The main source of information about diabetes for participants such as Finn and Paul who had a college and university level of education was the Internet.
I have cousins who have been diabetic for a long time and type 2 as well so we chatted a bit on the … Well, the one girl was worse than I was, and she's very, very good. She watched everything she ate, I swear to God. So, yeah. She was a good resource. I could call her and she lives in Montreal, of course.
Bob recalled that he did not know anything about diabetes at the time he was diagnosed. Thus, he had a friend explain it to him and alert him about his blood sugar and the need to take insulin:
I knew nothing about them and then a friend of mine said, ‘You need insulin. Your diabetic sugar level must be pretty high, because you got them sores all over you.’ He said, ‘I had the same thing, went to a doctor and he said it's ‘cause my sugars were too high.’ And he's diabetic. I said, ‘What’d you do?’ He said, ‘You’ve got to adjust your insulin until you get it cleared up.’ I said, ‘I ain’t got no insulin. I can’t get in to see my family doctor.’ He said, ‘You don’t need to see your family doctor. You go to the pharmacy and you say by law they have to give you insulin.’ I said, ‘Is that right?’ So I went and see them and, ‘Yeah, we’ll give you some insulin.’ And, they gave me insulin, and it went that way.
For participants such as Anita and Bob a family member or close friend provided some advice and explanations about diabetes. Having a cousin who controlled diabetes strictly served as a role model and good resource for Anita. Bob, on the other hand, had a close friend who had had similar signs of diabetes complications and therefore was able to warn him about it and direct him to find services and resources. These findings showed that sometimes family members or friends who have dealt with the disease can be helpful and good resources for understanding diabetes. Social support from family and friends can make living with diabetes easier.
Maverick stated that he has learned from his own experience that led him to be conscious about his limitations: Experiment with it. Then you know your limitations. I have to be very conscious of how much exercise I’m doing with my insulin. If I exercise too much and take a full dose of insulin, my sugars will crash. That happens on occasion.
Overall, most of the information participants acquired came from the Internet, healthcare providers or a support network. Yet, participants such as Duke and Maverick believed they learned most by living with diabetes and learning about their limitations.
Discussion
This study examined the process of engagement in information-seeking behavior for people with type 1 and type 2 diabetes. The constructivist grounded theory and symbolic interactionism helped us understand how individuals with diabetes engaged in the process of learning about their disease while living and adapting to a social world. The processes of engaging in information-seeking behavior include three phases: discovering diabetes, reacting to the diagnosis, and engaging in self-learning about diabetes, as well as three sub-concepts of searching on the Internet, talking to support networks, and learning from experience. (Figure 1) Participants shared that they engaged in self-learning about diabetes from the moment they began to recognize its symptoms until the time they had a confirmed diagnosis.
Between the process of discovering and learning about diabetes participants had a variety of reactions that are related to phase 2 of the theory. While some of them did not understand why they had the disease and questioned the Lord, others felt upset and uncomfortable because they did not know anything about it and needed to change their daily lives to manage diabetes. These findings are similar to those of previous studies that described a variety of reactions to the diagnosis of chronic disease that include anger, fear, anxiety, stress, depression, and disruption. 22 When many people find out that they have a chronic disease, their immediate response is to question God, the world, and pay attention to their role in their diagnosis. 23 Even for those able to accept their chronic condition, its trajectory is marked by repeatedly unstable periods of illness and wellness. 24
After they received confirmation of the diagnosis and passed the phase of questioning it, learning to live with and managing diabetes occurred progressively. When we asked directly about how they found about diabetes and learned how to manage it on a daily basis, it was clear that participants did not have much opportunity to engage in information-seeking behavior or in formal diabetes class. Unfortunately, of all participants, only a few had access to a diabetes class. Canadian research related to patient's attendance in diabetes classes is still scarce. However, investigators of previous studies have reported that just one in five patients newly diagnosed with diabetes attended a diabetes self-management education program. 25 Another Canadian study reported that fewer than half of primary care physicians referred all their diabetes patients to diabetes education programs. 26
Phase 3 described participants’ engagement in information-seeking behavior. They stated that after receiving the diagnosis and making diabetes meaningful they wanted to learn more about their condition. In our study, most of the information participants sought was from the Internet, healthcare providers or a support network. Research findings have shown that the Internet has become the primary source of health information in contemporary society, and diabetes is no exception. 27 In addition, individuals with a higher level of education use the Internet more than those at a lower level. 28 Individuals with a newer diagnosis of diabetes who reported having less access to information from their healthcare providers were more likely to use the Internet.29,30
Participants in our study also expressed receiving a paucity of information (and support) from healthcare providers, which led them to look for it from other sources. In a previous qualitative study, participants described how the scarcity of information received from healthcare providers after being diagnosed with diabetes 31 made them reach out to their social networks (e.g., family members, friends, etc.) whom they knew were living with diabetes. These findings showed that sometimes family members or friends who have dealt with the disease could be helpful and good resources for understanding and living with diabetes. Those who have experience in managing diabetes are important sources of information for those newly diagnosed to understand how to deal with their condition. 32 However, participants who did not have access to the Internet or diabetes education programs and did not have someone with diabetes in their social network were left without the option to learn about their condition. Learning about the disease from their mistakes can be very challenging and dangerous for their health. All study participants developed the diabetes complication of foot ulceration and some also faced having their toes amputated.
Besides limited access to a diabetes class, participants who attended it shared that most of the content was disease-focused (e.g., glucose-monitoring, medication regimen, diet, exercise, and weight loss), which is consistent with standard diabetes education programs in North America.33–35 As a result of not being taught about diabetes complications, many participants did not know that diabetes could lead to foot deformity, ulceration, and lower limb amputation. All of them confirmed when directly asked that they had never attended a formal foot care education class and that diabetes-caused foot disease was never mentioned in diabetes class or by their healthcare providers. These findings are consistent with Wounds Canada's report that highlights that fewer than half of all individuals with diabetes who had undergone amputation had received information on how to inspect and take care of their feet prior to the amputation. 36 Therefore, failure to emphasize the importance of foot care and to distinguish “teaching” from “telling” may result in poor communication, inadequate education, 37 and irreversible diabetes consequences for patients.
Implication for clinical practice and policy
This study uniquely addresses how the process of engagement in information-seeking behavior occurred after participants received the diagnosis of diabetes. It showed a profound lack of participant preparation to embark on the process of diabetes self-care and prevent complications such as diabetic foot ulcer. Although this process of engagement may seem familiar to most clinicians, our study's findings urge a change in this seemingly normal process, if those of us in healthcare expect to see improvements in diabetes outcomes in the future. In fact, the usual way of seeking information has not contributed to improve the uptake of diabetes knowledge, as we have witnessed the skyrocketing incidence and prevalence of DFU. Undoubtedly, clinicians need to develop a new process of engagement in information-seeking behavior that places the individuals at the center of care and allows them to participate as active subjects in the design of an effective pathway to acquire and implement information to achieve better outcomes. Recent systematic review of diabetes-related information-seeking behavior suggests that a more comprehensive way of sharing information is needed to help patients to identify reliable sources of information on the Internet. 8
Information and care must be designed along with patients's participation rather than directed to them and without their input. To this end, healthcare providers such as nurses, primary practitioners, diabetes educators, social workers, and dieticians need to engage individuals in developing diabetes education materials and programs. That kind of cooperative venture ensures that diabetes education programs address patients’ health and cultural needs, preferences, beliefs, gaps in knowledge, and physical, emotional, and social factors that influence their ability to meet the challenges of implementing diabetes self-management on a daily basis. 38 Policy makers need to develop policies that include the needs, values, and culture of individuals with diabetes. In doing so, educational programs should accessible for individuals and families from the time they are diagnosed, and developed to target the multiple needs of individuals from different backgrounds. Individuals with diabetes need support to manage this multifaceted disease that leads to potential physically devastating outcomes such as amputation and emotional despondency such as depression. 22
An effective pathway to learn about and manage diabetes includes educational strategies to equip patients and families with appropriate knowledge to manage this complex disease on a daily basis. Further, the cornerstone of self-management education includes involving patients in goal-setting, and helping them in developing problem-solving and decision-making skills to manage diabetes . 39 Healthcare professionals hold a pivotal position in advocating for a self-care management model that promotes patient autonomy and confidence to take responsibility for daily self-management. In summary, these findings support the need to ensure that patients and families have access to diabetes education, reliable diabetes information, services, support, and resources from the beginning of their diagnosis to make sure they develop the confidence and skills needed to regulate diabetes throughout the course of their illness.
Limitations
Participants in this study were recruited from one wound care clinic in the province of Ontario, Canada. We also included only individuals with one type of chronic wound (i.e., diabetic foot ulcer). We understand that the incorporation of participants from different wound care settings and with other type of wounds may have produced additional or different results. Another potential limitation was undertaking this study as a novice grounded theorist. To mitigate that, the principal investigator (I.C.G.) reviewed and carefully followed the step-by-step guide to develop a constructivist grounded theory described by Charmaz14,15 and consulted with supervisors as needed.
Conclusion
These findings revealed that although the Internet is often used to seek information, healthcare providers and support networks also played an essential role in supporting individuals’ information-seeking behavior to learn about diabetes. However, these were not enough to prevent participants from developing diabetes complications such as DFU. Thus, healthcare providers face an urgent need to develop an effective pathway for people with diabetes to learn about and manage diabetes and also to design diabetes education programs that focuses on individuals’ unique needs, preferences, concerns, and beliefs.
These findings highlight the need to change the current process of engagement in information-seeking behavior to one that is more beneficial to individuals and helps them to successfully cope with this life-long condition and prevent devastating outcomes. Individuals with diabetes should have access to reliable information from the beginning of their diagnosis. Reliable information will enable them to understand the progress of their disease, cope with and manage signs and symptoms, learn the self-management practices they will need to implement on a daily basis, and develop self-confidence to perform their role as self-care managers. This kind of active self-engagement also includes the ability to ask the right questions and seek the right answers from the right resources.
Healthcare providers need to be more proactive in providing essential information to patients in a way that makes sense to them by using lay language after their diagnosis. Secondly, they need to be more proactive in helping patients get onto the right pathway to learn how to become good self-care managers. Finally, they need to be aware of where individuals seek information to learn about their diabetes, and direct and connect them to reliable resources and community support.
Footnotes
Acknowledgements
The authors thank Drs. Deborah Tregunno, Elizabeth VanDenKerkhof and Dana Edge for their contributions in the thesis preparation that generated this paper.
Contributorship
IGC contributed to the conceptualization, acquisition, analysis and interpretation of data; drafted the first version of this manuscript and funding acquisition. PCP guided the research study, contributed to the design of the methodology, and revised the manuscript critically for important intellectual content. All authors reviewed and approved the final version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Obtained
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided by the Canadian Frailty Network to complete the many steps of this study Canadian Frailty Network.
Guarantor
I.G.C.