
Abstract
Pregnancy is a critical period. Pregnant women need to perform healthy lifestyle behavior in order to ensure good fetal development. During COVID-19 pandemic, Augmented-Reality (AR) media may be used in pregnant women health education. However, there is a lack of research that investigated the effect of AR media use in pregnant women health education. Therefore, this research aimed to investigate the impact of AR media use on healthy lifestyle knowledge, attitude, and behaviors among pregnant women during COVID-19 pandemic. This cohort-longitudinal study involved 86 pregnant women aged 18–45 years. The subjects who participated in this research received health education interventions using AR media for 5 months. The data collection was performed at the pre–post-intervention through a survey with questionnaire. Changes in subjects' healthy lifestyle knowledge, attitude, and behaviors were analyzed by using t-test. The research results show that the AR media use in health education significantly improved the subjects' scores for healthy lifestyle knowledge (5.0 ± 10.9; p < .05) and behaviors (9.7 ± 17.5; p < .05). However, the subject score for attitude was not significantly improved (0.3 ± 7.1; p ≥ .05). This research results provide evidence of the importance of using AR media in health education for pregnant women during COVID-19 pandemic.
Introduction
One of the health education that need serious attention is health education for pregnant women. This is due to the important role of pregnant women health conditions in supporting fetal growth and development. 1 Pregnant women health condition also affects the chance of stunting in children. 2 In Indonesia, specifically, health education for pregnant women is important to be conducted considering the following concerning facts. First, the maternal mortality rate in Indonesia remains alarming. In 2017, the rate reached 177 per 100,000 live births, making it the highest in Southeast Asia. 3 Second, the nutrient intake of pregnant women in Indonesia is also quite concerning. This can be seen from the 2018 Basic Health Survey results, which indicated that the prevalence of anemia among pregnant women reached 48.9%. 4 A study conducted by Mulyani et al. 5 found that even among well-educated mothers, 68.3% were still classified under the dehydration group. Third, the prevalence rate of stunting in Indonesia remains high. In this regard, the results of the 2021 Indonesia Nutritional Status study conducted by the Ministry of Health of the Republic of Indonesia and the Central Bureau of Statistics show that the prevalence of stunting still reaches 24.4%. 6
During the COVID-19 pandemic, pregnant women health education is also increasingly important considering that a person's immunity and health condition are needed to prevent being exposed to COVID-19.7–9 On the other hand, the handling of pregnant women who are affected by COVID-19 will tend to be more complex. 10 In Indonesia, from April 2020 to April 2021, there are 536 COVID-19 cases of pregnant women. 11 From 536 cases, 48.1% cases are COVID-19 cases with the symptom. 11 Furthermore, the mortality rate is 3%. 11
The COVID-19 pandemic has changed the activities that were originally carried out by relying on physical meetings and have turned into activities based on online meetings by utilizing digital technology,12–14 including health education. 15 One of the pregnant women health education models that can be carried out during the COVID-19 pandemic is the Augmented-Reality (AR) mobile learning application-based maternal education model. AR media is one of the media that can be used in providing learning education, 16 including health education. 17
In the context of health education, several studies have attempted to examine the impact of AR use on health behavior, for instance, in the pediatric patient for anesthetic injections, orthopedic patient rehabilitation, and kidney and prostate cancer patient.18–20 Several studies explain the positive benefits of using AR technology in the health sector to change knowledge, attitudes, and behavior. 17 However, there is a lack of studies that examined the impact of AR use in the context of health education among pregnant women. More clearly, there is no research that investigates the impact of AR use on pregnant women health education during the COVID-19 pandemic. Considering that pregnant women health education focuses on changing healthy lifestyle knowledge, attitudes, and behaviors of pregnant women, to fill the gaps in the literature, this study examines the impact of AR mobile learning application-based health education on healthy lifestyle knowledge, attitudes, and behaviors of pregnant women in Indonesia, a developing country, during the COVID-19 pandemic.
Method
This study is a cohort-longitudinal study conducted in August 2020-December 2020 at Public Health Centre of Kebon Jeruk District, Jakarta, the capital city of Indonesia. The location selection was determined based on the number of antenatal care visits, around 150 visits per day, and the status of the public health center as a pilot and a reference health center. This research has received ethical approval from Universitas Esa Unggul, Health Research Ethics Commission, Jakarta in the form of Ethical Approval Statement with number 0162-20.153/DPKE-KEP/FINAL-EA/UEU/V/2020 dated May 30, 2020.
Subject
The subjects of this study were pregnant women who came to have their pregnancy checked in the study area during the study period. Since the number of pregnant women who came to have their pregnancy checked in the area was not fixed and fluctuated as the nature of pregnancy number in an area is also not fixed and fluctuate, the sample size was decided based on two considerations. First, the sample size should fulfill the minimum requirement of the statistical analysis tool this research used. More specifically, in order to achieve normality assumption, the minimum sample size should be 30.21–23 Second, several experimental studies involving pregnant women during COVID-19 pandemic used 29–30 samples in their intervention group.23–26 Therefore, this research decided the minimum sample size should be 30.
Subjects were picked using the purposive sampling method. The use of the purposive sampling method in the context of research on the behavior of pregnant women was also carried out by Nurlaily et al. 27 The entry criteria for the subjects were: (1) pregnant women getting their antenatal care at the public health center, (2) healthy (not suffering from secondary infections) based on the medical examination, (3) never gave birth to a low birth weight and short babies, (4) 18–35 years old, (5) have a body height of 150–165 cm, (6) have a BMI between 18.5 and 25.0 kg/cm2, (7) signed the informed consent, and (8) are willing to comply with research procedures. This research did not put education level as a subject criterion due to two considerations. First, the public health center provides health services for pregnant women without any education level requirement. Second, health education was normally designed for pregnant women without any education level requirement. A subject was excluded from the study if she fulfilled at least one of the exit criteria of this study. The exit criteria of this study were as follows: (1) The subject discontinued the utilization of antenatal care services at the public health center designated as the study location, and (2) the subject was incapable of fully following all of the mandatory procedures and treatments specified in the study.
At the screening stage in the second trimester, 100 pregnant women subjects were identified, and then 86 pregnant women subjects were willing to take a part in the media education activity until it was finished. Moreover, 14 pregnant women subjects were not willing to join the study because 10 people returned to their hometowns and four of them were moved to another examination location. The sample size fulfilled the minimum requirement of sample size this research previously decided. Figure 1 shows the data collection flow.

Data collection flow.
This research selected second-trimester pregnant women due to the rapid fetal development during this phase. 28 In the second trimester, the vital organs of the fetus continue to develop, and the fetus’s sex can be determined.29,30 On the other hand, pregnant women are in a more comfortable condition compared to the first trimester that still have depression. 31 Therefore, health education is expected to be effectively provided during this trimester phase.
Intervention overview
The subjects were given an intervention in the form of health education based on AR mobile learning application for five months. Ten AR Cards were designed in order to deliver the information of healthy lifestyle behavior for pregnant women. The design of AR mobile learning application as follows. There are four sections on the main menu of the AR mobile learning application, each of which will direct the user to the sub-menu according to the flowchart in Figure 2. The scan menu (first button) contains camera features to analyze image markers on cards, while the tutorial (second button) and about (third button) menus contain information on how to use the application and application developer information. The exit (fourth button) menu will take the user out of the application. Image 1 shows the main menu of the application, the AR scan features, and the AR card.

AR mobile learning application flow.
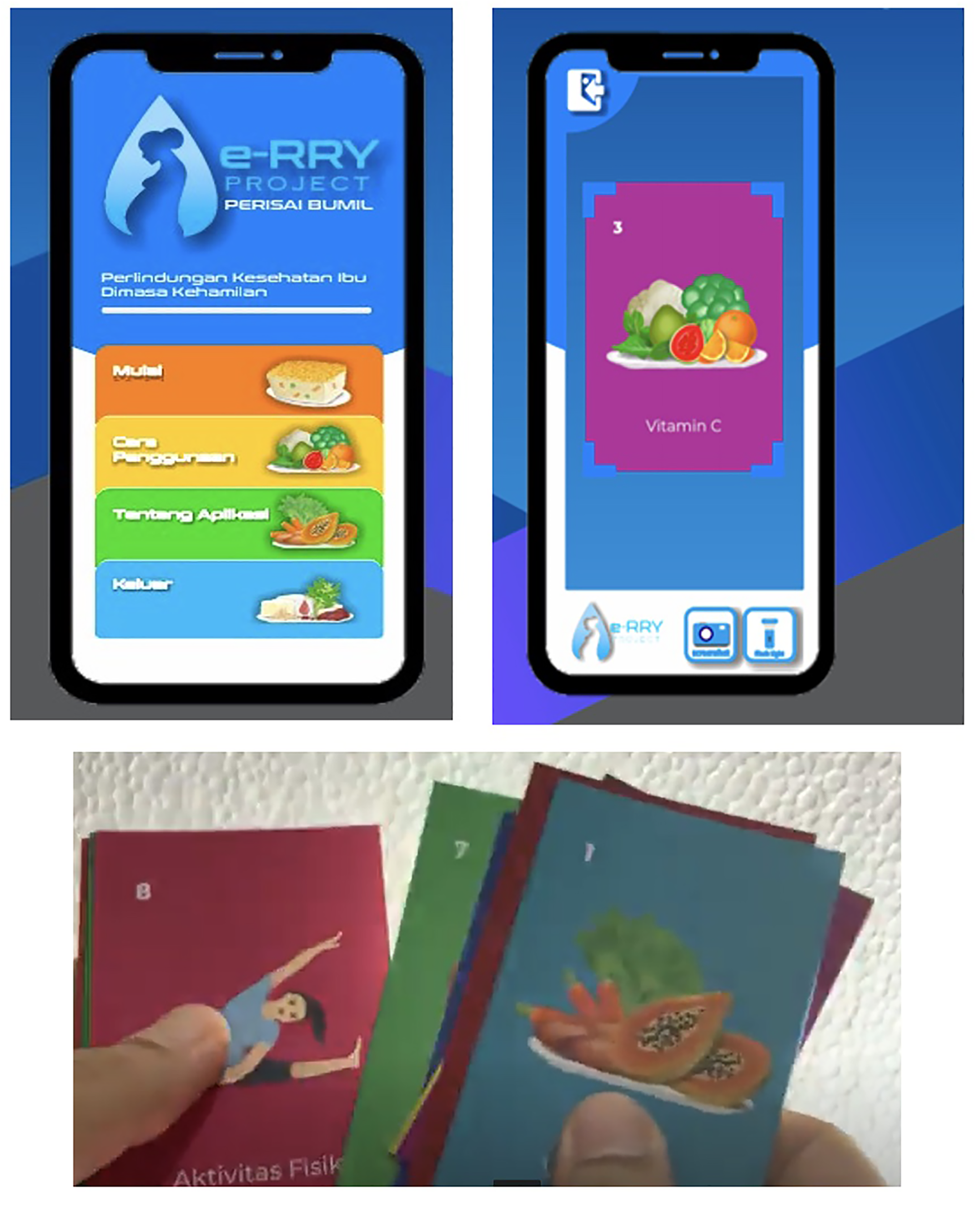
AR Application.
The scan menu of the application consists of four features. First, the frame scan feature can be used to scan the AR Cards. The feature will display a short, animated video of the scanned image from the AR cards. Second, the back button (top left corner button) will direct the user to the main menu. Third, the screenshot button is used to save photos from the smartphone layer. Fourth, the flashlight button can be used to turn on the flash on the smartphone in order to clarify the scan results in low light conditions. From these features, it can be stated that the AR cards are the input needed by the application so that health education can be performed.
The intervention process is as follows. The subjects were included in a WhatsApp group. They first downloaded the AR mobile learning applications. Then, 10 AR cards were delivered to them. Once a week the subject is given nutrition education for 2 h (education and discussion) with the help of AR card. The team involved in providing the material is a nutritionist with a minimum education background of undergraduate nutrition.
Measures
The data collection was performed at the pre-post-intervention. A survey with questionnaire and anthropometry collection was performed. The pre-pregnancy weight and body weight were measured using a digital weighing scale (OMRON) with an accuracy of 0.1 kg and mid-upper arm circumference (MUAC), using a meter line with an accuracy of 0.1 cm. Height was measured using a microtoise with an accuracy of 0.1 cm. All this measurement was executed by well-trained nutritionist under closed supervision of the researcher.
The constructs of healthy lifestyle knowledge, attitudes, and behaviors were assessed through a survey with questionnaire. Knowledge was measured by using 15 indicators. Healthy lifestyle behavior was measured by using 10 indicators. Attitude was measured by using 10 indicators. The indicators are shown in Appendix 1. In order to ensure the validity and reliability of the instrument, we performed the following procedures. The validity of the instrument was ensured by using the existing instrument that has already proved to be valid in our study context. The instrument of this research was previously used by Mulyani et al., 32 who also studied pregnant women in Jakarta, Indonesia. The reliability of the instrument was ensured through Cronbach Alpha (CA) analysis. The CA analysis showed that all CA coefficients of the constructs were higher than 0.5, namely 0.710 (knowledge), 0.707 (behaviors), and 0.513 (attitudes). In other words, knowledge and behaviors have high reliability, while attitude has moderate reliability. 33
The indicators of knowledge were measured using nominal scale (false; true). More clearly, the subject was required to evaluate the knowledge indicator/statement, whether it was false or true. The knowledge score was calculated as follows. The answer of the subjects on the knowledge indicator was valued 1 if the answer was right and 0 if the answer was wrong. Since knowledge was measured by using 15 indicators, the knowledge score was obtained by dividing the total value of the subject obtained with the maximum value the subject may obtain and then multiplying the result with 100. The maximum knowledge score is 100 with the total of all indicator is true (15 indicator).
The indicators of attitude were rated using a scale from 1 to 5 (1 = Very Disagree; 2 = Disagree; 3 = Neutral; 4 = Agree; 5 = Very Agree). More clearly, the subject was asked to provide his/her agreement regarding the attitude indicator/statement by selecting the scale. For example, if he/she very disagrees with the indicator, he/she selects the option of 1 (very disagree). The scale of the indicators of healthy lifestyle behaviors ranges from 1 to 5 (1 = never; 2 = rarely; 3 = sometimes; 4 = often; 5 = very often). Specifically, the subject was required to express his/her real experience regarding healthy lifestyle behaviors. For example, if a subject never performs a healthy lifestyle behavior indicator, he/she selects option of 1 (never).
The attitude and behaviors scores were calculated using the method employed by Mulyani et al. 32 More specifically, the attitude and behaviors scores were calculated as follows. The mean value of each indicator was calculated. Then, the indicator was re-categorized into two categories based on the mean value as a cut-off. Attitude categories were agreed and disagree, while behaviors were rarely and often. The answer of the subject was categorized as agree (often) was valued 1 and 0 if the answer of the subject was categorized as disagree (rarely). The attitude and behaviors scores were obtained by multiplying the total value of the subject obtained with 100.
This research transformed the knowledge, attitude, and behaviors scores to 100 due to three reasons. First, the scale of the constructs is different. Second, the score transformation makes the interpretations of the knowledge, attitude, and behaviors of raw data calculation results easier and clearer. 34 Third, several studies on health education and/or health behaviors also transformed the scores to 100.32,35–38
Data analysis
The data analysis was performed using Microsoft Office Excel and IBM SPSS Statistics. Subject characteristics data were analyzed descriptively and presented in the form of mean, standard deviation, and total (percentage). A t-test was performed to analyze the changes in subjects’ healthy lifestyle knowledge, attitude, and behaviors score before and after intervention. Data were analyzed at a 95% confidence level and significance level p < .05. This research used t-test due to two reasons. First, t-test is suitable to analyze data from two related groups, namely pre–post-intervention.39,40 Second, previous studies on health context that used pre–post-intervention data also used t-test.41–45
This study did not analyze the relationship between knowledge, attitude, and behavior due to two considerations. First, it is well known that knowledge, attitude, and behavior changes were the objectives of health education. Second, previous studies on health education that used experimental design and analyzed the impact of health education on knowledge, attitude, and behaviors also did not analyze the relationship between knowledge, attitude, and behavior.41,46,47
Results
Subject characteristics
Table 1 shows the characteristics of the subjects. Most of the subjects were aged 27.9 ± 5.1 years, which can be categorized as a productive age according to WHO. 48 The gestational age of the subjects is in the second-trimester category, namely 27.2 ± 8.5. 49 The pre-conception body weight of the subject was normal, 58.0 ± 10.9 kg with a mean body weight in the second trimester of 65.5 ± 11.2 kg. The increase in body weight from the average value is approximately 7.5 kg in normal circumstances.
The characteristics of the subjects.

N (%).
Generally, the subjects have high school education background (55.8%) and work as housewives (57.0%). Based on educational background, the average subject has an educational background in accordance with the government's recommendation of 9 years of compulsory education. 50 The average per capita household expenditure per month is Rp. 743,601.0. It was included in the category higher than the average per capita expenditure in urban areas (>Rp. 637,132/month). 51
Knowledge, attitude, and healthy lifestyle behavior of pregnant women
Each subject in this study received health education interventions using AR learning media, which was given for 5 months with 10 messages related to healthy lifestyle behaviors on the AR card. Then an evaluation is carried out at the end after giving the material is complete (post-test). Table 2 shows the results of the assessment of knowledge, attitude and behaviors scores of the subject before and after the education.
The knowledge, attitude, and behavior scores of subject pre- and post-intervention.

*p < 0.05.
Table 2 shows that there is a statistically significant improvement in the subject's healthy lifestyle knowledge and behavior scores. This shows that health education through AR-based learning media, which is carried out on a scheduled and consistent basis, is effective in increasing the healthy lifestyle knowledge and behavior of pregnant women.
Table 2 also shows that there is no statistically significant improvement in the subject's attitude score. In our research, the subjects already have a high value of attitude scores on the pre-intervention (mean = 97.3 ± 5.4). In other words, there is only a small room for improving the attitude score. Therefore, it can be understood the a non-significant change in the attitude score.
Discussion
Pregnancy is a natural physiological condition that requires attention because it can affects the outcome. 52 One of the important factors in fetal development is the health behavior of the mother during pregnancy. 52 This condition shows the importance of health education for pregnant women, especially during a pandemic. Pregnant women health education during a pandemic can be done by using AR as a media education. Unfortunately, empirical evidence showing its effectiveness is difficult to find in the literature.
This study fulfilled the gap in the literature by examining the impact of the use of AR media in health education on healthy lifestyle knowledge, attitudes, and behavior of pregnant women during the COVID-19 pandemic. The results of this study indicated that AR use in health education significantly improves the health lifestyle knowledge and behavior of pregnant women. However, AR use in health education does not significantly improve the attitude toward a healthy lifestyle of pregnant women.
The previous studies revealed that the use of AR positively influences knowledge and behavior in various health behavior contexts.17–20 It is argued that the use of AR facilitates experiential learning. 17 In experiential learning, the health education participant learns the health behavior through self-reflectiveness. 17 The use of AR makes self-reflectiveness easier to be performed since it can produce a sense of presence and increase emotional engagement. 17 Our findings strengthen the findings of previous research. Furthermore, our findings generalize the applicability of AR use in the context of health education for pregnant women. In other words, it can be stated that AR use in health education facilitates the experiential learning of pregnant women on health behavior needed during their pregnancy in the COVID-19 pandemic.
Regarding the non-significant effect of AR use on attitude toward health behavior in our research, this finding is different from the previous studies on the effect of digital health education on attitude.41,46 This may relate with the context of our research participant. In our research, the subjects already have a high value of attitude scores on the pre-intervention (mean = 97.3 ± 5.4 of 100). Therefore, the opportunity to significantly improve the attitude score is low. Another explanation of this finding may relate with the nature of attitude. Attitude is formed not only by cognitive evaluation but also by affective evaluation.53–55 In other words, attitude involves the emotional feeling of the participant.53–55 Furthermore, attitude represents the assessment of the accumulative experience. 54 These conditions make attitude improvement needs additional health education duration time to compare to knowledge and behavior improvement. In other words, in order to change their attitude toward the health behavior, the participant needs to evaluate the effectiveness of the health behavior based on her experience. 56 The time needed to perform this evaluation may not be covered by our research design.
Practical implications
Based on the previous explanation, it can be stated that the innovation of our study is empirical evidence on the impact of the use of AR media in health education on healthy lifestyle knowledge, attitudes, and behavior of pregnant women during the COVID-19 pandemic. Based on this innovation, several practical implications can be derived.
Our research shows that the use of AR in the health education of pregnant women significantly increases their knowledge and healthy lifestyle behavior during the COVID-19 pandemic. This finding provides several practical implications for health education practitioners, health education institutions, and the government. For health education practitioners and institutions, it is important to use AR-based media in providing health education for pregnant women during the COVID-19 pandemic. Health education practitioners and institutions can design an experiential learning-based health education by utilizing AR-based media.
For the government, there are several implications. First, the government needs to develop a health education policy that involves AR-based media. Second, the government needs to promote the use of AR media in health education. Third, the government needs to support AR use in health education by providing AR media-based health education material that can be easily accessed and other resources that are needed for performing AR media-based health education.
Limitation and implications for future research
Although this research provides interesting and important findings, there are several limitations that encourage future research. This research was performed in Jakarta, which represents a context of urban society. Urban society may have different views and acceptance of technology, such as AR media, with rural society due to the possibility of the digital divide between urban and rural society.57,58 Therefore, the effectiveness of AR use on health education for pregnant women also needs to be studied in the context of rural society.
This research found a non-significant effect of AR use on attitude toward health behavior for pregnant women. However, as previously discussed, this research was performed in the context of pregnant women with a high score of attitudes toward health behavior. Therefore, it is important to test the effectiveness of AR use in health education for pregnant women with low and middle scores of attitudes toward health behavior.
AR media-based health education for pregnant women is a type of health technology. In order to ensure that a technology is accepted by the organization that is supposed to use it, it is important to develop an efficient and easy-to-use technology. This research only involved one design of AR media-based health education for pregnant women. Future research should develop more various designs of AR media-based health education for pregnant women and evaluate the efficiency and easy to use of the technology so that it can be found the most efficient and easy-to-use design of AR media-based health education for pregnant women.
This research was performed during the COVID-19 pandemic. The pandemic makes the limited number of participants that involved in this research. This condition caused this research did not employ a control group that can be used to evaluate the health lifestyle knowledge, attitude, and behavior changes more comprehensively. Although there are also previous studies on the effect of digital media use in health education that also did not employ a control group to evaluate the health knowledge, attitude, and behavior changes,59,60 future research should consider to employ a control group.
Conclusion
This research investigated the impact of AR use in pregnant women health education during COVID-19 pandemic. The subjects of this study were women at the second-trimester pregnancy with normal weight. It was found that there was a significant increase in the health lifestyle knowledge and behavior of pregnant women after the intervention of AR media-based health education. Therefore, AR media-based health education can be used as an alternative approach in improving health lifestyle knowledge and behavior of pregnant women during the COVID-19 pandemic.
Footnotes
Acknowledgements
The views in this study were expressed by researchers and did not reflect the views of the Ministry of Research, Technology and Higher Education of the Republic of Indonesia. We also would like to thank the staff of the Accredited Laboratory and Public Health Centre of Kebon Jeruk District, West Jakarta, who helped in the data collection process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
EYM and IJ who conceived and designed the studies oversaw its implementation and contributed to the writing of the manuscript. SS supported the acquisition of data and contributed to the revision of the manuscript and data analysis. All authors contributed to the interpretation of data and approved the final manuscript.
Ethical approval
This research has received ethical approval from Universitas Esa Unggul, Health Research Ethics Commission, Jakarta, in the form of Ethical Approval Statement with number 0162-20.153/DPKE-KEP/FINAL-EA/UEU/V/2020 dated May 30, 2020.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Research, Technology and Higher Education of the Republic of Indonesia [grant numbers 3580/LL3/KR/2021]. The APC was partially funded by Universitas Esa Unggul [grant number 028/LPPM/Kontrak-INT/PEN/VIII/2022].
Guarantor
All authors are guarantors.
Appendix 1. The indicators of the variables
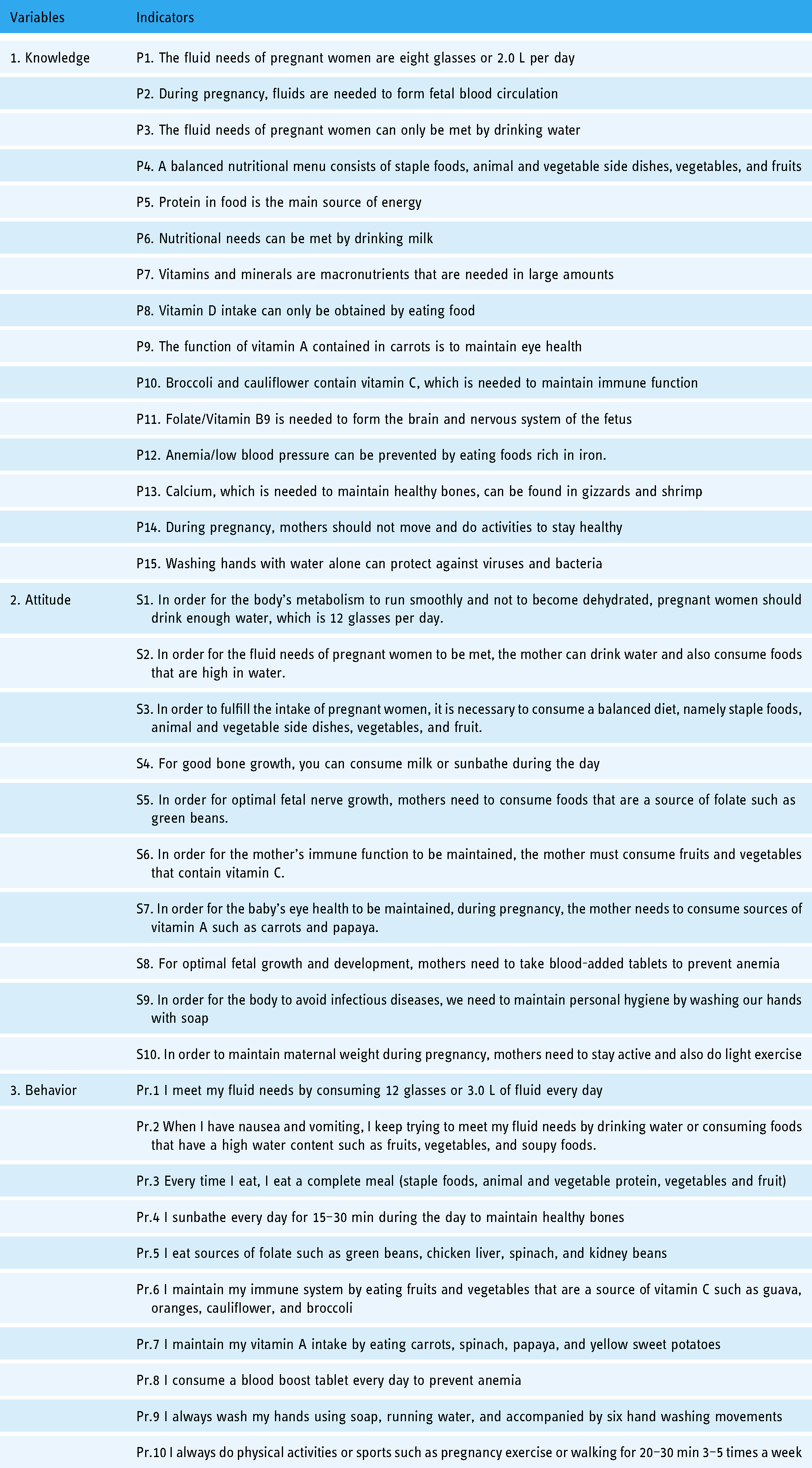
| Variables | Indicators |
|---|---|
| 1. Knowledge | P1. The fluid needs of pregnant women are eight glasses or 2.0 L per day |
| P2. During pregnancy, fluids are needed to form fetal blood circulation | |
| P3. The fluid needs of pregnant women can only be met by drinking water | |
| P4. A balanced nutritional menu consists of staple foods, animal and vegetable side dishes, vegetables, and fruits | |
| P5. Protein in food is the main source of energy | |
| P6. Nutritional needs can be met by drinking milk | |
| P7. Vitamins and minerals are macronutrients that are needed in large amounts | |
| P8. Vitamin D intake can only be obtained by eating food | |
| P9. The function of vitamin A contained in carrots is to maintain eye health | |
| P10. Broccoli and cauliflower contain vitamin C, which is needed to maintain immune function | |
| P11. Folate/Vitamin B9 is needed to form the brain and nervous system of the fetus | |
| P12. Anemia/low blood pressure can be prevented by eating foods rich in iron. | |
| P13. Calcium, which is needed to maintain healthy bones, can be found in gizzards and shrimp | |
| P14. During pregnancy, mothers should not move and do activities to stay healthy | |
| P15. Washing hands with water alone can protect against viruses and bacteria | |
| 2. Attitude | S1. In order for the body's metabolism to run smoothly and not to become dehydrated, pregnant women should drink enough water, which is 12 glasses per day. |
| S2. In order for the fluid needs of pregnant women to be met, the mother can drink water and also consume foods that are high in water. | |
| S3. In order to fulfill the intake of pregnant women, it is necessary to consume a balanced diet, namely staple foods, animal and vegetable side dishes, vegetables, and fruit. | |
| S4. For good bone growth, you can consume milk or sunbathe during the day | |
| S5. In order for optimal fetal nerve growth, mothers need to consume foods that are a source of folate such as green beans. | |
| S6. In order for the mother's immune function to be maintained, the mother must consume fruits and vegetables that contain vitamin C. | |
| S7. In order for the baby's eye health to be maintained, during pregnancy, the mother needs to consume sources of vitamin A such as carrots and papaya. | |
| S8. For optimal fetal growth and development, mothers need to take blood-added tablets to prevent anemia | |
| S9. In order for the body to avoid infectious diseases, we need to maintain personal hygiene by washing our hands with soap | |
| S10. In order to maintain maternal weight during pregnancy, mothers need to stay active and also do light exercise | |
| 3. Behavior | Pr.1 I meet my fluid needs by consuming 12 glasses or 3.0 L of fluid every day |
| Pr.2 When I have nausea and vomiting, I keep trying to meet my fluid needs by drinking water or consuming foods that have a high water content such as fruits, vegetables, and soupy foods. | |
| Pr.3 Every time I eat, I eat a complete meal (staple foods, animal and vegetable protein, vegetables and fruit) | |
| Pr.4 I sunbathe every day for 15–30 min during the day to maintain healthy bones | |
| Pr.5 I eat sources of folate such as green beans, chicken liver, spinach, and kidney beans | |
| Pr.6 I maintain my immune system by eating fruits and vegetables that are a source of vitamin C such as guava, oranges, cauliflower, and broccoli | |
| Pr.7 I maintain my vitamin A intake by eating carrots, spinach, papaya, and yellow sweet potatoes | |
| Pr.8 I consume a blood boost tablet every day to prevent anemia | |
| Pr.9 I always wash my hands using soap, running water, and accompanied by six hand washing movements | |
| Pr.10 I always do physical activities or sports such as pregnancy exercise or walking for 20–30 min 3–5 times a week |