
Abstract
Objective
The objective of this study was to investigate the risk of acute kidney injury in elderly patients compared with nonelderly patients undergoing AngioJet rheolytic thrombectomy for treatment of acute deep vein thrombosis.
Methods
A retrospective review of all patients who underwent AngioJet rheolytic thrombectomy for the treatment of acute deep vein thrombosis between November 1, 2014 and August 1, 2022 was conducted. Their baseline demographics, comorbidities, clinical characteristics, procedural details, and postoperative course were reviewed.
Results
A total of 105 eligible patients were reviewed; 45 patients were in the elderly group, and 60 were in the nonelderly group. Except for age (p < 0.001), no significant differences regarding demographics were detected (p >0.05). Transient macroscopic hemoglobinuria occurred in all patients during the first 24 h post-AngioJet rheolytic thrombectomy. The overall morbidity of acute kidney injury in the two groups was 11.4%, and the nonelderly group had a similar rate of acute kidney injury (8.3%) to the elderly group (15.6%). None of the 12 patients progressed to dialysis within the postoperative period, and the mean acute kidney injury recovery time of the elderly group was 5.86 ± 1.57 days, which was longer than the 3.60 ± .89 days of the nonelderly group (p = 0.017).
Conclusion
The use of AngioJet rheolytic thrombectomy for the treatment of patients with acute deep vein thrombosis is associated with a potential risk of acute kidney injury, which seems to have a comparable rate in elderly and nonelderly patients. acute kidney injury in the elderly group tends to need a longer recovery time, which requires postoperative vigilance for this population.
Keywords
Introduction
The population in the world is ageing rapidly, and people all over the world are living longer, but the elderly's chances of spending their later years in good health and well-being vary compared with the general adult population. 1 Deep vein thrombosis (DVT) is the third most common vascular disease, and its prevalence increases with age.2,3 Without prompt treatment, DVT in elderly patients is at a higher risk for developing pulmonary embolism (PE), which is more likely to lead to death than in the general population, partly due to higher rates of coexisting comorbidities. 4 Postthrombotic syndrome (PTS), another common and burdensome sequela of DVT, has proven to affect 23%–60% of patients who have received conservative anticoagulation therapy alone, further increasing health care costs and the financial burden on families and society.2,5 Hence, a trend of more aggressive endovascular therapies, such as percutaneous pharmacomechanical thrombectomy (PMT), has been recommended by some clinical guidelines and it has achieved superiority when compared with conservative therapy.2,6–9
AngioJet rheolytic thrombectomy (ART), which represents a modality of PMT, is mainly based on PMT with pulsatile lytic delivery, mechanical fragmentation, and rheolytic aspiration of the clots. 8 It has been proven to facilitate rapid thrombus burden removal, reduce further severe PTS, decrease the dosage of lytic agents and lower the risk of lysis-dependent bleeding complications,8,9 especially for elderly patients who are associated with a potentially higher bleeding risk induced by the high prevalence of multiple comorbidities or relatively poor vascular pathophysiology. Although the high-pressure jet spray of ART can benefit clot dissipation, it may also lead to the destruction of normal blood cells, intravascular hemolysis and hematuria. 10 Shen et al. 11 reported that acute hemolysis could definitely increase the odds of acute kidney injury (AKI) in 22.8% of patients during ART. In view of the fact that elderly individuals have weaker kidney function recovery competence in response to a health insult, the risk of AKI should be given more attention. Although postoperative AKI has been demonstrated in some patients, its influence on the elderly remains unclear, since the elderly are often excluded from clinical studies because of comorbidities, short life expectancies, and logistical difficulties.10,11
Advanced age is significantly associated with the presence of DVT.3,4 We wondered whether the use of ART increases the risk of AKI in elderly patients by increasing the extent of intravascular hemolysis. The purpose of this single-center retrospective cohort study was to assess whether the risk of AKI development in elderly patients who underwent ART (Solent catheter; Boston Scientific, Marlborough, MA, USA) for the treatment of DVT was affected compared with that of nonelderly patients.
Methods
Patients and study design
This was a retrospective cohort study including consecutive confirmed acute DVT patients (onset of symptoms was less than 14 days) who underwent ART as the first-line treatment at a single academic center from November 1, 2014, to August 1, 2022. The data were retrospectively derived from the medical database system and paper records. This data collection protocol was approved, and a waiver of informed consent was allowed by our Institutional Review Board owing to a span of approximately 8 years; obtaining patient consent would likely not have been possible. The baseline demographics, comorbidities, thrombotic risk factors, time from onset, procedural details, and related hematological examination data were recorded and reviewed. There were 166 potentially eligible patients, 61 of whom were subsequently excluded because they were treated with a large-bore catheter, had preoperative AKI, had a history of end-stage renal disease, or lacked perioperative creatinine values (the study flowchart is shown in Figure. 1). Of the remaining 105 included cases, based on age, 45 patients were divided into the elderly group (aged over 65 years), and 60 cases were in the nonelderly group (aged under 65 years old). Although periprocedural details slightly varied in different cases depending on individual therapy needs, the treatments were similar, and the approach to renal protective measures in both groups was comparable.

Study flowchart. DVT: deep vein thrombosis; ART: AngioJet rheolytic thrombectomy.
Management strategy details
Duplex ultrasonography and/or CT venography were initially performed for all patients to confirm the diagnosis and to assess the DVT extent. Anticoagulant treatment was initiated immediately when DVT was identified with the use of subcutaneous low-molecular-weight heparin (LMWH) at a bolus dose of 100 units/kg twice daily. ART was performed for suction mechanical fragmentation and thrombus aspiration based on a 6F ART catheter (Solent catheter; Boston Scientific). For patients without contraindications for thrombolysis or when it was left to the discretion of the endovascular operators, 3 mg of rt-PA (Actilyse; Boehringer Ingelheim; Ingelheim, Germany), with a total injected volume of 250 mL, was intraclot injected under the Power Pulse® model. After 20 min of dwell time, with the pump unit active during slow catheter passages (3–5 mm/s), runs were performed across the thrombotic segment in a distal-to-proximal manner under fluoroscopic guidance. Each device activation run lasted at less than 20 s with breaks of 30 s between the runs to avoid arrhythmia, and the total run times were monitored and kept at no more than 240 s. A maximum of 250 mL of suction fluid was used in patients receiving ART. If a residual clot was found following ART, alternative conjunction with catheter-directed thrombolysis (CDT) could be applied through a multiple-side hole thrombolytic catheter (Uni*Fuse; AngioDynamic; Latham, NY). Then, reduced-dose thrombolytic therapy of rt-PA was administered at an infusion rate of 0.01 mg/kg/h; the maximum rate was no more than 1.0 mg/h. Routine blood tests (including hemoglobin), renal function and fibrinogen level were conducted at least once before the operation and once a day for 3 consecutive days after the operation. Once AKI was identified, renal function was monitored until the serum creatinine (sCr) level began to decline. PTA and/or stent placement were encouraged for lesions that caused over 50% diameter narrowing of the iliac and/or common femoral vein, robust collateral filling, and/or a mean pressure gradient of more than 2 mmHg. At the end of LMWH, oral rivaroxaban was given for at least 6 months.
Renal protective measures details
Except for contrast agent, other potentially nephrotoxic drugs were not used during the course of hospitalization. Hydration measures during the perioperative period were empirically added during the perioperative period, 500 mL of 0.9% saline was administered intravenously to all patients 2 hours after the ART procedure, and 100 mL bicarbonate was administered intravenously. Once postoperative AKI occurred, renal protective drugs and even hemodialysis were adopted when necessary.
Definitions of outcomes
Elderly patients were defined as patients aged over 65 years or older, and those patients who were younger than 65 years were classified as nonelderly, as the World Health Organization has suggested. 1 Technical success was defined as the successful use of ART. The primary outcome studied was the development of postoperative AKI. The comparison between the baseline value and the highest value of sCr within 48 h after the intervention was chosen to determine the occurrence of AKI, which was defined as an absolute increase in sCr concentration of ≥26.4 μmol/L (0.3 mg/dL) or an increase ≥50% from baseline within 48 h following the operation and long-term renal impairment or recovery. The AKI recovery time was defined as the time from AKI occurrence to the return of baseline sCr. Hematuria was judged by visual inspection and urine occult blood test results.
Statistical analysis
The SPSS statistical software package (version 23.0; SPSS statistical software, Chicago, IL, USA) was used to perform all statistical analyses in the present study. When data were compared between the elderly group and the nonelderly group, an unpaired t test was used. When assessing the correlation between preprocedural and postprocedural variables, a paired t test was used. The significance of the qualitative variables was tested with a chi-square test or Fisher's exact test Findings with a p-value less than 0.05 were deemed statistically significant.
Results
Baseline demographics and clinical characteristics
A total of 105 eligible patients were finally included in the present study (the study flowchart is shown in Figure 1), with 45 patients in the elderly group (mean age, 72.9 ± 12.9 years; 46.7% male) and 60 patients in the nonelderly group (mean age, 44.1 ± 6.2 years; 38.3% male). The onset of DVT symptoms at presentation was mainly within the acute stage, with a mean of 5.9 ± 4.2 days, and the clots were all in the iliofemoral vein. Inferior vena cava thrombosis was implicated in 34.3% (36/105) of patients, and 27.6% (29/105) were identified with PE. Demographic, presentation, lesion characteristics, comorbidities, and DVT risk factors for these patients are summarized in Table 1. Except for age (p < 0.001), no significant differences regarding sex, onset time, thrombus segments or limbs, comorbidities or risk factors were detected between the elderly group and the nonelderly group (p >0.05).
Demographics, presentation, lesion characteristics, comorbidities and risk factors of DVT patients.

DVT: deep vein thrombosis; PE: pulmonary embolism; CAD: coronary artery disease.
Continuous data are presented as the means ± standard deviations; categorical data are given as the counts (percentage).
*Fisher exact.
aOne patient with previous isolated distal deep vein thrombosis included in Non-elderly Group.
ART seemed not to increase the hazards of postoperative AKI in elderly patients
All patients successfully underwent the ART procedure, and the technical success rates were 100% in both groups. The intraoperative procedures and treatment details are shown in Table 2. The models (including the PP model and/or clot aspiration) of the AngioJet device used in both groups were equivalent (p = 0.529). An average aspiration volume of 143.56 ± 48.69 mL was observed in this study, and the elderly group seemed to have a slightly reduced mean aspiration volume compared with the nonelderly group (136.65 ± 49.48 mL vs. 150.48 ± 47.64 mL), but no significant difference was noted (p = 0.151) (listed in Table 2). The proportion of patients who needed adjunctive CDT and the overall duration of CDT was not significantly different (p >0.05), but the agent dosages seemed slightly lower in the elderly group than in the nonelderly group (22.30 ± 7.80 vs. 29.18 ± 8.14; p = 0.064).
Procedure induced characteristics by ART treatment.
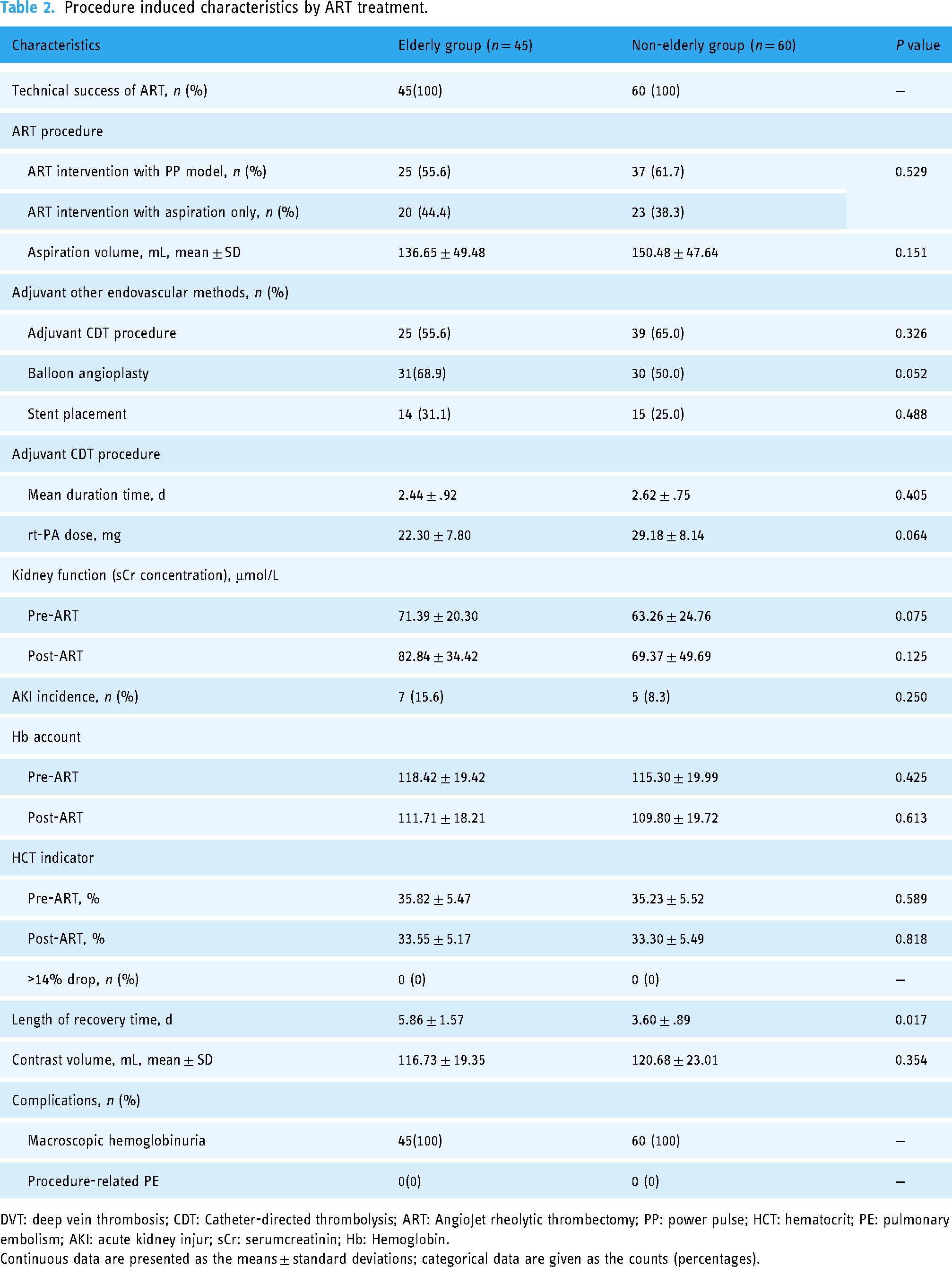
DVT: deep vein thrombosis; CDT: Catheter-directed thrombolysis; ART: AngioJet rheolytic thrombectomy; PP: power pulse; HCT: hematocrit; PE: pulmonary embolism; AKI: acute kidney injur; sCr: serumcreatinin; Hb: Hemoglobin.
Continuous data are presented as the means ± standard deviations; categorical data are given as the counts (percentages).
Transient macroscopic hemoglobinuria occurred in all patients during the first 24 h post-ART (typical changes within the first 24 h are shown in Figure. 2). The average contrast volume given was 116.73 ± 19.35 mL in the elderly group compared with 120.68 ± 23.01 mL in the nonelderly group (p = 0.354). The overall morbidity of AKI was 11.4% (12/105). AKI developed in 7 of 45 patients in the elderly group and in 5 of 60 patients in the nonelderly group, but the overall sCr concentrations pre-ART and post-ART were not significantly different (p >0.05). The incidence of AKI in the elderly group was similar to that in the nonelderly group (15.6% vs. 8.3%; p = 0.250). All AKI patients could be recovered to baseline sCr. In regard to hematological loss, the Hb account and HCT indicator were similar (p > 0.05). In AKI patients, none of the 12 patients progressed to dialysis within the postoperative period, but the mean AKI recovery time of the elderly group was 5.86 ± 1.57 days, which was longer than that in the nonelderly group (3.60 ± .89 days) (p = 0.017).

Images of urinary excretion collection bag from a 60-year-old male patient suffering from transient macroscopic hemoglobinuria during the first 24 h post-AngioJet rheolytic thrombectomy (ART). (a) Immediate after ART procedure. (b) 6 h. (c) 12 h. (d), 18 h. (e) 24 h.
At completion, 68.9% (31/45) of the patients in the elderly group underwent PTA, which was slightly higher than that in the nonelderly group (50.0%; p = 0.052). The 31.1% (14/45) rate of stent use in the elderly group had a trend to be higher than that in the nonelderly group (25.0%, 15/60, p = 0.488). The use of antithrombotic treatments and renal protective measures were not significantly different between the two groups (p > 0.05).
Discussion
The risk of venous thrombosis soars with age; the incidence is less than 5/100000 individuals per year in people younger than 15 years but approximately 500/100000 individuals per year among those aged 80 years. 3 Around 60% of thrombotic events present after the age of 60 years.3,4 In the past two decades, approximately 600 million people have passed the age of 60 years worldwide, and this number will skyrocket to 1.2 billion in 2025 and 2 billion in 2050.1,10 However, an exact cut-off to define “the elderly” has not reached a consensus; various researchers have used 60, 65, 70, and even 80 years.1,12 In our study, we adopted an age over 65 years as a standard. For people aged 70–75 years, they are expected to live for at least 14 more years, and those aged 80–85 years are expected to live at least 8 additional years. The CaVenT study 5 and ATTRACT trial 9 indicated that CDT or PMT could lower the morbidity of PTS during the follow-up; hence, aggressive therapies such as ART and thrombolysis for DVT have been applied to elderly patients, aiming to achieve the same expected safety and good prognosis as nonelderly patients.
In addition to several case reports,13–15 postoperative dysfunction of the kidney after ART has also been noted in some cohort studies.10,11,16 Escobar et al. 10 reported that the ART procedure is an independent risk factor for AKI and postulated that ART-induced hemolysis could trigger the development of AKI. Shen et al. 11 and Morrow et al. 16 subsequently found that ART as a treatment for arterial or venous thrombosis increased the risk of AKI when compared with CDT alone. Salem et al. 17 carried out a study in a population that underwent ART and found that patients with bilateral extensive DVTs are at a higher AKI risk, which may progress to chronic renal failure in a small fraction of affected patients. However, less attention is given to the influence of ART on kidney function in elderly patients in the literature.
Regarding the definition of postoperative AKI, different studies had various standards. AKI was detected by evaluating a rise in sCr concentration rather than a glomerular filtration rate (GFR) reduction in Shen et al. . 11 One reason could be that no direct measurement of GFR was conducted. In addition, according to the calculated formula for GFR, the sCr concentration is the only variable that changes within 48 h. Hence, the sCr concentration was chosen for detecting postoperative AKI. In our study, we also chose this criterion to indicate AKI. Patients who developed AKI within 48 h had an increase in sCr compared with preoperation. Another kidney function test was then conducted between 48 and 72 h to confirm the diagnosis of AKI.
Our study supports the findings of previous studies that PMT is associated with acute renal dysfunction.2–5 The incidence of postprocedural AKI after ART in the present study was 11.4%, which seemed to be slightly lower than that of the 21%–22% in previous reports.11,17 Two potential reasons may be associated with this reduced incidence. First, there were obvious differences between the 6F Solent Omni catheter used in the present study and the 8F ZelanteDVT catheter used in a previous study. 17 An 8F catheter has a larger catheter lumen and a stronger high-pressure pulse/suction effect, 18 which might jeopardize more red blood cells and lead to severe intravascular hemolysis. Under this condition, the release of free hemoglobin can overwhelm binding proteins. Free hemoglobin is filtered into the glomerulus and can cause acute tubular injury, thus elevating the risk of AKI. Second, the degree of hemolysis is thought to be proportional to the duration of ART. A relatively lower mean aspiration volume of 143.56 ± 48.69 mL in the present study was observed compared with 175 ± 92 mL in previous studies. 16 This increased volume indirectly indicated a longer pulse/suction time and potential devastation of intravascular hemolysis, 11 which can cause a heme pigment-induced burden on the kidney and increase the hazards of AKI to some extent.19,20 Prompt recognition of intravascular hemolysis earlier in the clinical course may have been implemented, and intravenous crystalloid fluids remain the mainstay of treatment for the prevention of AKI. However, there is a paucity of data on the best choice of fluids (i.e., alkalinization vs. normal saline). 21
In the present study, the data revealed that the rate of the development of postprocedural AKI between the two groups was similar, which showed safe ART procedures in the elderly and nonelderly populations. Although there was no statistically significant difference in AKI when comparing the two groups (p = 0.250), among the 12 patients who developed AKI, the average length of time until return to their baseline creatinine values in nonelderly patients was 3.60 ± .89 days, which was faster than the elderly patients, which may be attributed to elderly patients having a reduced ability to compensate and recover from health insults due to underlying diseases. Once AKI has been established, treatment was largely supportive in our study. The PEARL registry 8 showed that 4 out of 283 patients required dialysis after ART. Fortunately, none of our patients progressed to dialysis-dependent AKI within the same admission.
Our study had several limitations. First, the present study used a 6F Solent Omni catheter for AngioJet ART rather than an 8F ZelanteDVT catheter; thus, whether the lumen would affect postprocedural AKI was difficult to evaluate, and this notion should be addressed in future studies. Second, we acknowledge that we chose the sCr concentration as the indication of AKI instead of GFR reduction because no direct measurement of GFR was conducted. Third, this study was limited to an early short-range observation during hospitalization, but any available long-term follow-up data will be recorded in the future. Moreover, the present study was a single-center, nonrandomized controlled, retrospective study. The conclusions of the present study were limited as a result of the small number of cases, lack of logistic regression analysis, and other undefined risk factors and should be interpreted with caution. In the future, a prospective, randomized controlled study with a longer follow-up period to overcome these limitations should be designed to validate the conclusions.
Conclusions
The application of ART for the management of patients with proximal DVT confers a potential risk of AKI, which seems to have a comparable rate in elderly and nonelderly patients. Elderly patients tend to have a longer recovery time, so a shorter run time of rheolytic thrombectomy may be preferred for this population.
Footnotes
Guarantor
Jianping Gu
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number 81871463) and Xinghuo Talent Program of Nanjing First Hospital.
Ethical approval
The study protocol was reviewed and approved by the institutional review board (IRB) of the Nanjing First Hospital, Nanjing Medical University (Nanjing, China). In addition, the study was performed in accordance with the Declaration of Helsinki and the Ethical Guidelines for Clinical Studies.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available, as the experimental data are related to other experiments that are progressing but are available from the corresponding author upon reasonable request
Authors’ contributions
MFG contributed to this project development, manuscript writing/editing. GQF, ZLL contributed to data collection, manuscript associated editing. YYZ and JK contributed to data analysis. BXZ and XH contributed to manuscript editing. JPG contributed to project development, manuscript editing. All authors contributed to the article and approved the submitted version.