
Abstract
Objective
The aim of this study was to assess the feasibility and potential effectiveness of an 8-week virtual EMG biofeedback intervention for patients with CLBP.
Methods
Patients with CLBP completed validated baseline and post-intervention assessments of pain intensity and interference (Brief Pain Inventory), back pain-related disability (Oswestry Disability Index), anxiety and depression (Hospital Anxiety and Depression Scale). Participants underwent a series of Quantitative Sensory Testing (QST) procedures assessing responses to mechanical stimuli during two separate visits (baseline and post-intervention). In addition, we assessed, using surface EMG, the muscle tension in the trapezius, latissimus, and low back muscles at each session. Patients were randomized into the EMG biofeedback intervention or usual care group. Factorial analysis of variance including the interaction between treatment group and time was used to analyze the changes in pain intensity (primary outcome), pain interference, disability (secondary outcomes), anxiety, and depression (secondary outcomes).
Results
Compared to the treatment as usual comparison group, patients in the EMG biofeedback group reported lower pain intensity after completing the intervention (mean group difference 0.9, 95% CI −1.07, −0.32; p≤0.01). Compared to baseline, participants in the EMG biofeedback group demonstrated statistically significant reductions in pain interference (mean difference 1.3, 95% CI 0.42, 2.1; p≤0.01), disability (mean difference 4.32, 95% CI 1.2, 7.3; p≤0.01), and significant increases in low back pain thresholds (mean difference 0.5, 95% CI −0.87, −0.05; p≤0.01), assessed by QST. However, no significant group by time effects were observed for secondary outcomes: pain interference, disability, and low back pain thresholds. In addition, significant changes were observed in muscle tension for the trapezius, latissimus, and low back muscles in the EMG biofeedback group (p<0.001).
Conclusions
Virtual EMG biofeedback shows promise as a potential therapy for reducing pain and disability in individuals with chronic nonspecific low back pain.
Introduction
Low back pain (LBP) adversely affects the majority of adults at some point, causes disability for many, and is a common reason for seeking treatment. LBP is the most common musculoskeletal condition affecting the adult population, with a lifetime prevalence of up to 84%. 1 Chronic LBP (CLBP) is a chronic pain syndrome in the lower back region, lasting for at least three months. 2 To date, a number of non-pharmacologic interventions have been found to be beneficial in the management of CLBP patients; one such treatment approach is biofeedback. 3
Biofeedback is a treatment method that uses displays of physiological data to help participants develop the ability to modify involuntary processes consciously. It is frequently used for pain management and as part of the interdisciplinary treatment approach in pain centers. The aim of biofeedback therapy is to develop increased awareness of and control over biological processes. Various biofeedback modalities are widely used for chronic pain management, including autonomic nervous system measures (hand temperature, skin conductance, and heart rate), central nervous system measures (electroencephalography), and biomechanical measures (force and pressure). 4 Surface EMG is one of the oldest biofeedback modalities 5 which was used in clinical research as early as the 1920s, by Edmond Jacobson, the developer of interventions such as progressive muscle relaxation (PMR). 6
The general approach to biofeedback starts with utilizing non-invasive equipment to assess a specific physiological parameter. Such physiological signals (e.g. heart rate, muscle tension) are usually displayed directly or into a visual, auditory, or tactile feedback signal. Biofeedback training often involves incorporating a stress reduction rationale for the treatment. Since stress causes the muscles to tense, it can increase levels of pain. In addition, stress increases cortisol levels and causes inflammation and pain over time. 7 Biofeedback-assisted relaxation training is a generalized manualized treatment that has been used over the past 40 years to help reduce chronic pain and anxiety levels. The benefits of manualized treatment are the promotion of evidence-based practice, the enhancement of treatment integrity, the facilitation of staff training, and the potential replicability of treatment. 8
For the past 50 years, electromyographic biofeedback (EMG-BF) therapy has been identified as a potential therapy for decreasing muscle tension and reducing CLBP. 9 EMG-BF therapy has shown evidence to result in a greater reduction in muscle tension compared to using relaxation training alone. In a representative study, patients who received 90 days of EMG-BF compared to relaxation training or an educational program demonstrated a larger reduction in pain intensity, and a larger proportion remained symptom-free at four years post-follow-up. 10 Similar results were shown by Keefe and colleagues, where patients attended six training sessions with EMG-BF along with relaxation training. 11 Participants demonstrated significant decrease in daily ratings of muscle tension at the one-year post-follow-up. In a similar study, Vlaeyen and colleagues demonstrated that using an operant-respondent treatment approach including EMG-BF compared to an operant cognitive approach can produce broad positive outcomes on biopsychosocial factors including pain catastrophizing. 12 Interestingly, the majority of clinical trials of biofeedback for pain were performed in the 1980s and 1990s. Few clinical outcome studies that focus on EMG-BF for CLBP have appeared in the scientific literature since that time. In this study, we aimed to assess the effects of a virtual 8-week EMG-BF intervention on pain in patients with CLBP. Our hypothesis was that patients in the EMG-BF group will demonstrate significant changes in pain intensity, pain interference, disability, anxiety, and depression compared to the control comparison group.
Methods
We recruited 81 patients with CLBP (pain duration at least 6 months but no longer than 10 years), aged 18–65 years old and with minimum pain intensity score of >3 on a visual analog scale (VAS). Out of those 80 participants, 50 provided complete data before and after the intervention. Participants were randomly assigned to either the JOGO Digital Therapeutics EMG-BF or a treatment as usual control group following a 3:2 ratio randomization. Our study was registered on clinicaltrials.gov (Identifier: NCT04607460).
All patients were asked to complete self-report questionnaires assessing demographics, pain intensity (primary outcome), pain interference, negative affect, and disability (secondary outcomes) and underwent Quantitative Sensory Testing (QST) prior to and after completing the intervention. The intervention consisted of eight weekly sessions during which participants practiced various EMG-BF exercises with a trained biofeedback instructor. Study procedures received approval by the Institutional Review Board (IRB) of Brigham & Women's Hospital (Boston, MA, USA). Upon request, and subject to certain criteria, conditions, and exceptions, access to individual deidentified participant data can be provided.
Eligibility criteria
EMG-Biofeedback intervention
EMG-BF facilitates neuromuscular retraining and muscle relaxation by using visual stimuli using an EMG surface electrode-based biosensor and a software installed on a tablet or smart phone. During the weekly sessions participants were instructed on how to use the device and practiced various EMG-BF exercises with a trained biofeedback instructor. EMG electrodes were placed across the shoulder (trapezius muscle), underneath the shoulder blade (latissimus muscle) and at the lower back (paraspinal muscles). The EMG signal was visible on the tablet screen, which was also visible to the therapist. Each biofeedback session consisted of a series of exercises, during which the participants were taught to identify and reduce the level of tension they are feeling. Additionally, in each session, participants learnt ways to further reduce their muscle tension including relaxation techniques (e.g. PMR) while wearing the EMG-BF device. Further, one session was dedicated to posture training using the EMG-BF device. In each session participants had the opportunity to discuss possible difficulties using the device. Sessions lasted 40–45 min and were all conducted virtually (on BWH encrypted Zoom platform). Patients were instructed to practice the exercises they learnt during the session at least 30 min three times a week and keep track of their home practice.
Measures
Demographic Questionnaire. The baseline questionnaires collected basic demographic information following the existing recommendations for the minimum dataset in CLBP clinical trials.
The Brief Pain Inventory (BPI 13 ). This self-report questionnaire is a well-known measure of pain intensity and interference. The questionnaire provides information about pain history, intensity, and location as well as the degree to which the pain interferes with daily activities, mood, and enjoyment of life. Scales (rated from 0 to 10) indicate the intensity of pain on average (average of the four items): at its worst, at its least, and pain “right now.” The BPI has excellent validity and is among the most frequently-used outcome measures in chronic pain trials. 13
The Hospital Anxiety and Depression Scale (HADS 14 ). The HADS is a 14-item scale designed to assess the presence and severity of anxious and depressive symptoms. Seven items assess anxiety, and seven items measure depression, each scored from 0 to 3. The HADS has been used extensively in clinics and has adequate reliability (Cronbach's α = 0.83) and validity, with optimal balance between sensitivity and specificity. 15 It has been translated into many languages and is widely used around the world in clinical and research settings. Anxiety and Depression were calculated irrespectively as subscales and explored in separate analyses.
The Oswestry Disability Index (ODI). It is one of the most commonly used outcome measures for individuals with LBP. The ODI has 10 items that assesses how LBP affects common daily activities.16,17 The ODI has a range of 0% “no disability due to LBP” to 100% “completely disabled due to LBP,” with higher scores indicating higher disability from LBP. The ODI has been found to have sound psychometric properties 17 with a minimal clinically important difference reported to be 10 percentage points.
Muscle tension assessed by EMG biofeedback. The therapist collected logs on muscle tension (amplitude of surface EMG signal) assessments pre- and post-treatment for each session and each muscle group for every patient receiving the intervention group for the trapezius, latissimus, and low back muscles.
Quantitative Sensory Testing (QST)
QST is a non-invasive method for measuring pain sensitivity and pain modulation.
Our QST testing protocol will measure mechanical pain sensitivity (pain threshold) and temporal summation of pain (reflecting pain-promoting processes). These protocols have been used in various studies we conducted by our lab.18–23
Mechanical pain and temporal summation of pain
Data analysis
Statistical analyses were performed using the SPSS 26.0 for the Social Sciences (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used for demographic and clinical characteristics of the study sample. Baseline differences between groups were assessed by an unpaired t-test. For categorical variables, chi-square tests were used. Analyses were carried out on a “per protocol” (PP) basis, which covered patients who entered the intervention (n = 27) and control group (n = 23) after randomization and presented values at the follow-up point.
Based on previous investigations, a sample size of 18 subjects in each group was required to detect a decrease of 25% in pain equal to the difference of one standard deviation (effect size = 0.08) with a power of 80% and α of 0.05. Factorial analysis of variance (ANOVA) including the interaction between treatment group and time was used to analyze the changes in pain intensity (primary outcome), pain interference and disability (secondary outcomes), anxiety and depression (secondary outcomes). In addition, two-way repeated measures ANOVA was used to analyze the changes in low back and trapezius pressure thresholds (secondary outcome). Muscle tension changes were tested in the intervention group using paired t-tests.
Results
The majority of participants in both groups were female, white, and non-Hispanic. Chronic pain was characterized as moderate in intensity and of long duration. Less than 16% of the sample was using as-needed opioids in either group (see Figure 1). Participants’ baseline characteristics are given in Table 1, which demonstrates no significant differences between the two groups with a randomization 3:2. Participants (n = 27) attended an average of 6.8 ± 1.2 (range 4–8) of the eight sessions in the EMG-BF based intervention.

Consort flow diagram.
Sociodemographic variables and baseline scores.

Note. SD: standard deviation; BPI: Brief Pain Inventory; ODI: Oswestry Disability Index; PCS: Pain Catastrophizing Scale; HADS: Hospital Anxiety and Depression Scale.
Primary outcome
A two-way repeated-measures ANOVA performed for pain intensity demonstrated a significant time effect (p<0.001) and a group time interaction (F = 6.45, p =0.01), showing a change in pain intensity scores based on time and group assignment (Table 2). The results of the final analyses are presented in Table 3. Compared to baseline, participants in the EMG-BF group demonstrated statistically significant improvements in pain intensity (p<0.01) whereas TAU participants did not demonstrate any significant changes.
Questionnaire scores by assignment group.

Note. M: mean; SD: standard deviation; ppth: pain threshold; BPI: Brief Pain Inventory; ODI: Oswestry Disability Index; PCS: Pain Catastrophizing Scale; HADS: Hospital Anxiety and Depression Scale.
Changes in muscle tension before and after sEMG biofeedback sessions.
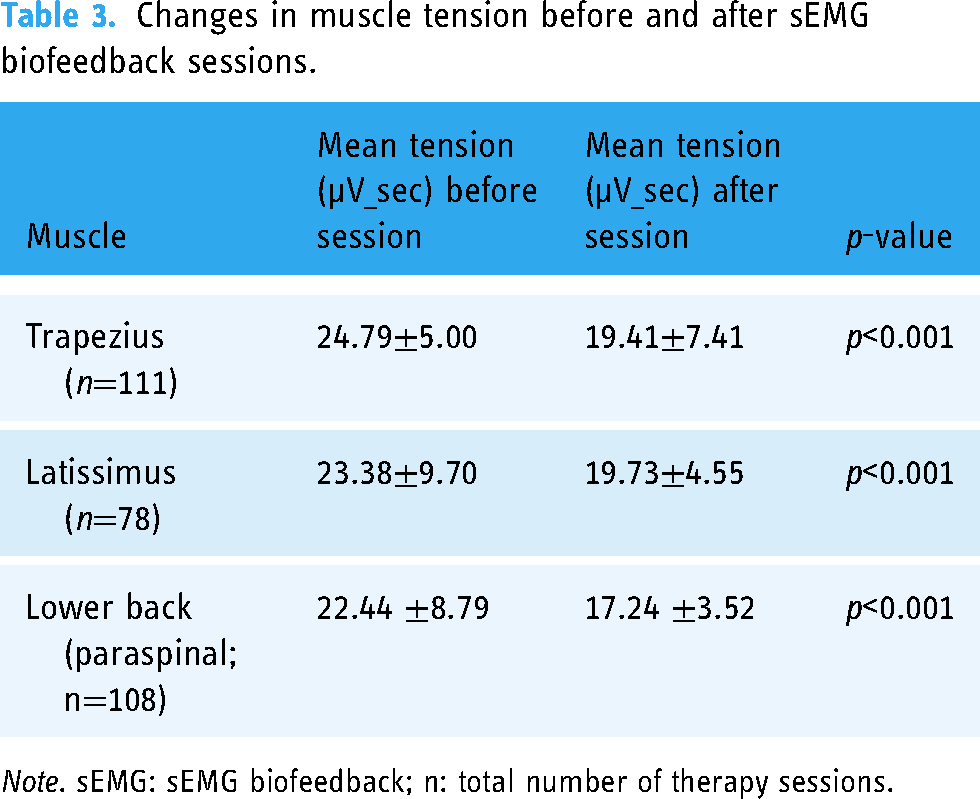
Note. sEMG: sEMG biofeedback; n: total number of therapy sessions.
Secondary outcomes
A two-way repeated-measures ANOVA performed for pain interference demonstrated a significant time effect (mean difference 1.3, 95% CI 0.42, 2.1; p≤0.01) but not significant group time interaction (F = 1.53, p =0.22), demonstrating a change in pain interference scores over time but not as a function of group.
A two-way repeated-measures ANOVA performed for disability demonstrated a significant time effect (mean difference 4.32, 95% CI 1.2, 7.3; p≤0.01), but not significant group time interaction (F = 0.17, p =0.6), demonstrating a change in disability scores over time but not as a function of group.
A two-way repeated-measures ANOVA performed for LBP thresholds (assessed by the QST) demonstrated a significant time effect (mean difference 0.5, 95% CI −0.87, −0.05; p≤0.01), but not significant group time interaction (F = 2.45, p =0.1), demonstrating a change in LBP threshold scores over time but not as a function of group (Table 2).
A two-way repeated-measures ANOVA performed for HADS-anxiety and HADS-depression, trapezius pain thresholds, and temporal summation demonstrated no significant time effect nor significant group time interaction (p>0.05).
Paired t-tests demonstrated significant reductions in muscle tension for the trapezius, latissimus, and low back muscles in the EMG biofeedback group (p≤0.01). Table 3 shows the mean muscle tension before and after each exercise and each muscle group.
Discussion
The aim of this pilot study was to assess a pilot 8-week virtual EMG-BF intervention for patients with CLBP. In addition, the purpose of using EMG-BF was to improve patient's muscle and posture awareness and to support muscle relaxation in an effort to bring pain relief. Our results demonstrated that this virtual EMG-BF is an effective therapy for reducing pain intensity in individuals with chronic nonspecific LBP, therefore satisfying our primary endpoint.
Our results come in agreement with recent studies on the use of real-time muscle monitoring of neck and shoulder muscles using a portable EMG device with promising results. In three randomized control trials, portable EMG biofeedback was found to be effective for reducing muscular tension and associated pain and perceived disability in females with chronic neck/shoulder pain.24–26 Our results are also in line with a recent meta-analysis reporting small-to-medium effect sizes for reduction of pain intensity, disability, and muscle tension in patients with CLBP. The increase of LBP threshold by 25% in the lower back alongside with the improvement of reported pain intensity suggest that the observed changes in experimental pain sensitivity may translate to improvements in chronic pain severity. 27 It is important to note though that there is additional, well-documented evidence for other nonpharmacologic therapies for non-specific LBP including acupuncture, 28 massage therapy and yoga,29,30 cognitive-behavioral therapy, 31 and spinal manipulation. 32 Other effective non-pharmacological therapies include exercise therapy which seems to be a good option for pain relief and improved functional ability. 33
Among other advantages, our study is one of the first to systematically assess the use of a portable EMG-BF device for reducing CLBP. Although EMG-BF is the most widely used and widely reported method of biofeedback in chronic pain management, few clinical EMG-BF training protocols have been scientifically tested before. 4 Another advantage of this intervention was the use of a virtual therapy for pain management. The remote technologies enable people to try different treatment modalities out safely and for their behavior to be modified in a way they wouldn’t necessarily be able to achieve in the “real world.” Especially, during the COVID pandemic, more and more virtual therapies are becoming more popular for pain management. Therefore, our study is novel in many ways including the accessibility and usability of the device and therapy delivery model.
A number of limitations must be considered when interpreting the present findings. First, we were not able to include a sham EMG-BF comparison group which limits the comparison between groups. However, there is significant difficulty of designing studies with credible sham EMG-BF, which can be compared with real EMG-BF, in assessing the efficacy of a defined biofeedback training protocol. Second, we utilized only two timepoints to assess changes in outcomes which might limit the observation of long-term therapy effects. Multiple endpoints could potentially have allowed the exploration of long-term effects of our virtual EMG-BF program. In addition, we were not able to demonstrate Minimal Important Clinical Difference (MICD) for Pain Interference. Since this was a pilot study, we are hoping to be able to conduct a future RCT that will include a bigger sample size. Another limitation includes not being able to include a diverse ethnic and socioeconomic group in our sample. It is indeed true that the Boston Metropolitan area includes 4.5 million people, with the majority being Caucasians with higher socioeconomic backgrounds. Last, surface EMG is effective in assessing contractile activity of the superficial multifidus muscle but it might not be able to accurately assess activity in deep multifidus. However, surface EMG is convenient and offers the possibility to be practiced at home although it can only assess part of the muscle. Intramuscular EMG which can get at the deeper structures requires a laboratory-based assessment. 34 Despite these limitations, we demonstrated that eight weeks of EMG-BF significantly reduced pain intensity, disability, and muscle tension in patients with CLBP. These results of this study demonstrated the feasibility of a digital intervention for CLBP and set the basis for conducting a future, larger scale randomized controlled trial to confirm these preliminary findings.
Footnotes
Contributorship
AL performed the analysis, drafted the manuscript, and supervised the study. MP delivered the virtual therapy and drafted the manuscript. RE served as scientific advisor and critically reviewed the study design and analysis. EV, JS, AK, and DB were involved in the study design and data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Study procedures received approval by the Institutional Review Board (IRB) of Brigham & Women's Hospital (Boston, MA, USA).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JOGO Health Inc.
Guarantor
AL