
Abstract
Purpose
This pilot study evaluated how the content design of a nonpharmacological digital therapeutic intervention influenced therapeutic targets (self-regulation and impulse control) in children with ADHD. Examining the link between content-design features and target constructs clarifies the importance of design choices in digital intervention content. Typically, digital therapeutic intervention content is structured in a question-and-answer format that incorporates multiple therapeutic objectives. Evaluation involves tracking changes in the user's accuracy rate, which is then used to link target elements to the intended therapeutic goals. This makes it challenging to present elements that precisely align with specific therapeutic goals.
Method
Self-regulation and impulse control were the therapeutic objectives, with 30 children divided into experimental and control groups. The former performed content designed to target self-regulation and impulse control; the latter content focused on general cognitive elements. Both groups were evaluated using K-CBCL and FAIR.
Findings
For K-CBCL, statistically significant differences were observed between the two groups in the rate of change in internalizing (t = 2.34, p = 0.031) and externalizing (t = 2.39, p = 0.026) behaviors. For FAIR, significant differences were observed in the P-percentile (t = 2.40, p = 0.024), Q-percentile (t = 2.52, p = 0.022), and C-percentile (F = 4.42, p = 0.045).
Conclusion
These findings preliminarily indicate that ADHD digital intervention content aligned with assessment instrument targets may be associated with improvements in the intended therapeutic domains. Confirmatory evaluation in larger, longer, multisite studies, including teacher ratings and academic and social functioning outcomes, is warranted.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a psychiatric condition characterized by a persistent pattern of inattention, hyperactivity, and impulsivity that interferes with daily social functioning. 1 The etiology of ADHD is considered multifactorial and involves genetic, biological, and environmental factors; however, the exact cause has not yet been clearly identified. 2 From a medical perspective, ADHD is classified as a neurodevelopmental disorder, often associated with an imbalance or immaturity in brain function, particularly in the prefrontal cortex, leading to difficulties in attention and self-regulation. 3 The prevalence of ADHD in school-aged children ranges from 5% to 13%, indicating that this disorder primarily affects the pediatric population.4,5 Therefore, careful attention should be paid to diagnosis and treatment.
The treatment of ADHD includes both pharmacological and nonpharmacological approaches. 6 Pharmacological treatment involving central nervous system stimulants and nonstimulant medications is effective for managing symptoms and improving social behavior. 7 Among children, pharmacological interventions have been reported to yield positive responses in approximately 70–80% of cases.8,9 However, the side effects must be considered. Although they may vary depending on the type of medication, common adverse effects include loss of appetite, nausea or vomiting, headaches, dizziness, and insomnia. 10 These side effects can reduce the long-term effectiveness of pharmacological treatment and limit a child's ability to adapt positively to social settings. As a result, growing concerns among caregivers about the side effects of medication have led to an increased demand for nonpharmacological interventions, either as alternatives or in combination with medication.11,12 Accordingly, there has been rising interest in the use of digital content as a diagnostic and therapeutic training tool for children with ADHD. In particular, digital therapeutics have shown potential benefits for enhancing cognitive function in children with ADHD.13,14
The self-regulation function of therapeutic support content used as a training tool for children with ADHD is designed to help them learn to control themselves in distracting environments to successfully complete their final tasks.15,16 In impulse-control training, the content adapts mission scenarios based on the user's responses to various environmental stimuli such as color cues, character movement, size, sound intensity, and attention-diverting events, which are unrelated to the game's objective.17,18 Therefore, the digital therapeutic content intended for such interventions must be designed in clear alignment with the therapeutic goals, enabling users to train themselves not to react to irrelevant environmental stimuli.
The digital content used in digital therapeutic interventions for children with ADHD generally falls into two structural categories: a unidirectional question-and-answer format or a problem-solving format, in which the child actively engages in the task of finding the correct answers.19,20 A representative example of the problem-solving format is game-based digital content. Game-based content, initially designed to enhance motivation, can facilitate active participation during therapeutic training by promoting emotional engagement with various characters and allowing for the contextualization of scenarios, thereby increasing children's interest. 21 Such engaging content can serve as a powerful source of motivation for children with ADHD.
Digital therapeutic design should be grounded in a systematic design–evaluation framework that emphasizes content–goal alignment, use of user feedback, adaptive design, engagement, and stimulus management.22,23 However, many existing serious games remain oriented toward engagement, repetition, and immediate rewards, with unclear implementation of goal alignment, stimulus control, and delayed reinforcement.24,25 Moreover, baseline-adjusted, comparator-controlled evidence demonstrating how design elements and therapeutic targets relate to ADHD outcome measures remains limited.26,27
This study focused on the design aspects of game-based digital content that contribute to its therapeutic effectiveness. Rather than serving as a standalone pharmacological treatment, such content is intended to be used as an adjunctive therapy within a multidimensional, cognitively integrated intervention approach.28,29 This study thus examined how the design of digital content, when used as a supplementary therapeutic tool, can effectively support two core treatment objectives in children with ADHD: self-regulation and impulse control. Training methods for self-regulation are primarily based on cognitive self-awareness, behavioral reinforcement, and emotional control. Operationally, this requires the application of digital content that strengthens attention through self-monitoring. 30 Training methods for impulse inhibition are mainly grounded in response inhibition tasks; the operational definition involves applying content that provides real-time feedback through self-monitoring, delayed rewards, and distraction management. 31 The question of whether the design of digital content aligns with therapeutic goals must be addressed with high specificity. In particular, the connection between the therapeutic purpose and the choice of characters, their movements, and the methods and types of learning, as well as the assessors and assessment methods, should be clearly articulated. While games are often designed to capture attention through visually appealing, entertaining features, it is essential to consider in more detail what types of attention and cognitive processes are being targeted. This consideration is especially important when the children involved are engaging with the training not merely for entertainment but for therapeutic or rehabilitative purposes.
Therefore, customized design tailored to the characteristics of the target children is required to apply content that aligns precisely with the intended therapeutic goals. This involves identifying and integrating various auxiliary elements such as task structures, characters, background environments, and response components, which correspond to a single, well-defined therapeutic objective. Designing content based on these elements is likely to be more effective for achieving targeted treatment outcomes.
This study utilized digital intervention content currently used as adjunctive therapy for the pharmacological treatment of children with ADHD. For comparative validation, two types of content were employed: a question-and-answer format designed to assess performance and improve general cognitive abilities and game-based content redesigned specifically to target self-regulation and impulse control as therapeutic objectives.
This study provides quantitative evidence supporting the hypothesis that digital content for children with ADHD should be designed according to the specific therapeutic objectives of the target population. Moreover, there is a need to evaluate the impact of purpose-built, engagement-oriented content design and to advance design research that aligns with children's psychological relatedness and therapeutic objectives.32,33
Therefore, the aim of this pilot study was to explore, via baseline-adjusted comparisons with an active control, the effects of a game-based digital content design explicitly aligned with the core therapeutic targets for children with ADHD (self-regulation and impulse control) on clinical outcomes (K-CBCL, FAIR).
Methods and materials
This study was a prospective, parallel-group pilot comparative trial conducted in the Department of Psychiatry at K University Hospital. Children with a DSM-5 diagnosis of ADHD were allocated to either a story-driven, game-based digital therapeutic intervention targeting self-regulation and impulse control or a question-and-answer–based training control, both delivered via tablet over a 4-week period. The primary outcomes were parent-reported emotional and behavioral problems on the Korean Child Behavior Checklist (K-CBCL) and performance on a standardized attention test (FAIR), assessed at baseline and post-intervention. The following subsections describe the study setting, participants and recruitment, intervention protocol, outcome measures, and statistical analyses in detail.
Study participants and recruitment
This study was conducted prospectively over a 3-month period, from January 3, 2023, to April 7, 2023, in the Department of Psychiatry, Keimyung University Dongsan Hospital. Prior to data collection and assessment, ethical approval was obtained from the Institutional Review Board (IRB no. 2022-12-020) in accordance with ethical considerations for the research participants. The informed consent form and explanation included information on the study's purpose, participation procedures, potential risks and benefits, and confidentiality, as well as assurances that the collected data would not be used for purposes other than this study. The data collection and experimental procedures began after written consent was obtained from all participants and their legal guardians. Participants were selected based on a comprehensive review of clinical interviews conducted by board-certified psychiatrists, along with psychological assessments, including attention and intelligence tests. All data were stored and securely protected in accordance with the Bioethics and Safety Act.
This study included 30 children aged 6–13 years who were diagnosed with ADHD based on the criteria in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). 34 The inclusion criteria were as follows: voluntary written consent from the legal guardian and assent from the child to participate in the clinical study, ability to comply with the investigator's instructions and study procedures, and normal intellectual functioning, as determined by the Korean version of the Wechsler Intelligence Scale for Children, Fifth Edition (K-WISC-V). 35
Concurrent medication use was permitted under controlled conditions: Participants were allowed to continue their preexisting ADHD medications, but initiation of any new medications during the intervention period was not permitted. The concurrent medications included methylphenidate-class and atomoxetine-class drugs, all of which were maintained at stable doses as prescribed prior to study enrollment.
The exclusion criteria included the following: children diagnosed with disorders or conditions other than ADHD (e.g., post-traumatic stress disorder, psychosis, severe obsessive-compulsive disorder, or major depression), individuals with physical conditions that could affect the use of the experimental product (e.g., physical deformities of the hands or arms, prosthetic limbs), those with a history or suspicion of substance abuse or dependence within the past 6 months, participation in another ADHD-related study within 90 days prior to screening, individuals with color blindness, those with a family member currently enrolled in or participating in the same study, and any other condition deemed by the investigator to make the participant unsuitable for the study.
Although no direct adverse effects were expected in the children participating in the study, owing to the nature of digital devices, potential side effects such as frustration, headaches, or dizziness could occur. To minimize such risks, a usage monitoring system was incorporated into the program to limit device usage to less than 30 min per session. 36
Participants were randomly assigned in a 1:1 ratio to the intervention or control group. Randomization was performed without stratification, and allocation concealment was managed by an independent researcher; the general study staff was not informed of the allocation sequence. The randomization list was generated by the biostatistics team, participant enrollment was conducted by a single on-site investigator, and group assignment notifications were issued by an independent researcher. Outcome assessors were blinded to group allocation. In total, 38 participants were screened and enrolled, with 19 assigned to the EYAS-Focus DTx (question-and-answer–based training) plus medication and 19 to the NeuroWorld DTx (story-driven, game-based self-regulation/impulse-control training) plus medication. During follow-up, four participants in each group (eight total) withdrew for scheduling reasons, leaving 30 participants (15 per group) for analysis. An overview of the study design is shown in Figure 1.

Flow diagram of study participants.
Content design
The design and development of content aimed at improving self-regulation and impulse control in children with ADHD prioritized the identification and integration of design elements that respond to a child's stimuli and reactions. The analysis revealed that the characteristics and task environments selected by the participants were directly related to the therapeutic training processes targeting self-regulation and impulse control. Accordingly, the design approach began by structuring screens adapted based on how the selected characters responded to the given environment. We designed the procedure and feedback flow such that, regardless of the user's path, it converged on the same objective (mission).
The digital content used as the experimental tool was NeuroWorld (V2.1) DTx, developed by Woorisoft Co., Ltd (Republic of Korea, 2022), which was applied to the experimental group in accordance with the research design and implemented as a modular program. For the control group, typical Q&A-based digital therapeutic content, EYAS Focus (V1.4) DTx, developed by InTheTech Co., Ltd (Republic of Korea, 2024), was used. Both products were designed as training content and digital therapeutic interventions to support the pharmacological treatment of children with ADHD. In both programs, users could select content tailored to their individual levels within the program, thereby minimizing variability in the experimental results due to individual differences. The digital content used in the experiment was delivered through smart devices (tablet PCs).
Stimulus intensity was modulated using a design approach that encouraged users to actively regulate the task environment during the performance process. As shown in Figure 2, different types and levels of external stimuli were presented sequentially to introduce increasing levels of difficulty in controlling the stimuli.

Example of content with stimulus intensity modulation. (a) A general task scenario without surrounding stimuli. (b) A scenario in which the user focuses on the selected character and successfully completes the task without being affected by changes in the surrounding environment or stimulus intensity. (c) A scenario in which the user is exposed to external stimuli and exhibits behavior that deviates from the intended objective.
The intensity of external stimuli was modulated by combining vivid colors and sounds. It entailed repeated selective-response training in which participants responded to goal-relevant stimuli while suppressing responses to goal-irrelevant stimuli to promote impulse control. During the task, rewards such as points or in-game events were provided to reinforce self-regulation and impulse-control training. This approach reflects one of the most traditional methods of cognitive training. However, it was adapted to a game-based format favored by contemporary children, as illustrated in Figure 3. Accordingly, digital content applied a selective control design in which users responded to training commands generated during the performance process.
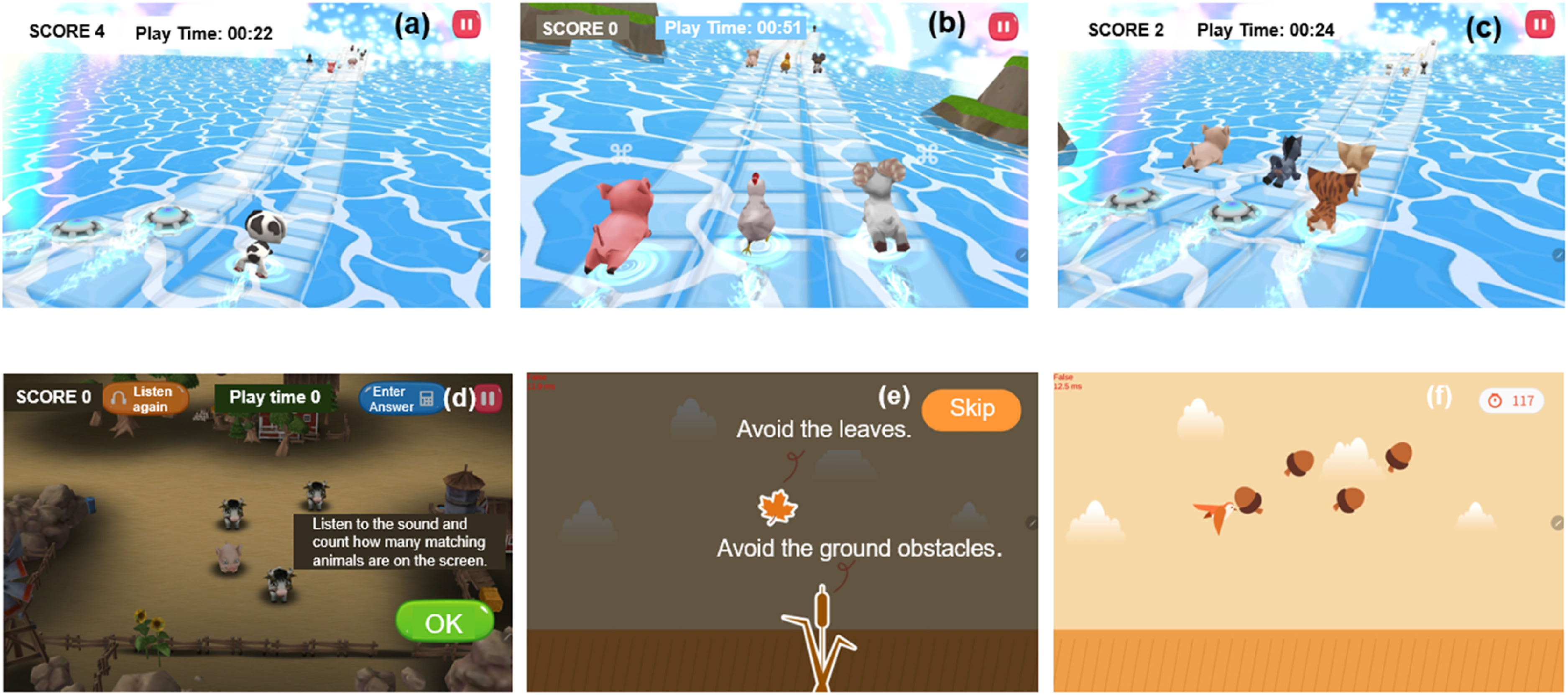
Impulse-control design. (a) Task execution process is aimed at achieving the intended goal. (b) A scenario in which the user follows a character identical to their own; when the target character changes, the user must quickly switch, training self-regulation based on character recognition. (c) A process in which identical characters create confusion and path interference, making it more difficult to achieve the goal. (d) A process in which irrelevant missions and distracting stimuli (e.g., sounds and colors) interfere with the user's ability to accomplish the original objective. (e) A screen where the user must choose among various distractions designed to prevent the completion of the initial mission. (f) A training process that guides the user on how to manage confusion and interference by responding with inhibition and control through their selected character.
The content was designed to consist of a main screen for performing self-regulation training and presenting the results, and an auxiliary screen providing explanations of the self-regulation training process. This structure allows for simultaneous access to both the training and evaluation phases while also promoting motivation for new challenges. The main screen, as shown in Figure 4(a), presents an analysis of the training results through direct feedback following the evaluation. This corresponds to direct or indirect assessments of the user's behavior by others and includes both qualitative and quantitative evaluations of the results presented after the game. The auxiliary screen, shown in Figure 4(b), guides the user's self-regulation process through empathetic emotional engagement. Both approaches enable simultaneous access to the performance and evaluation processes, thereby sustaining motivation and reinforcing learners’ self-awareness.

Design of the self-regulation training approach (evaluation example). (a) Main screen: After the game is completed, performance is evaluated, and quantitative results (e.g., attention, working memory, executive function) are presented along with encouraging feedback for the next training session. (b) Auxiliary screen: Rather than providing quantitative scores, this screen presents stage-by-stage evaluation feedback obtained during gameplay, offering information, self-reflective cues, and motivational messages to support the progress of use toward the next stage.
Finally, as illustrated in Figure 5, a game-based format was designed to enhance self-regulation and impulse control by providing reward-driven external events during the performance process. Rather than the immediate, predictable rewards typical of conventional games, rewards are granted after a defined period following the verification of performance criteria. This approach aimed to train users to suppress impulsive behaviors during a task to obtain rewards based on factors such as time, score, or interval, thus reinforcing self-regulation. Traditional designs often provide frequent event-based rewards to reduce errors or maintain user engagement. However, these systems allow users to predict reward patterns, leading them to focus more on repetitive task completion rather than on impulse suppression or genuine self-regulation. Accordingly, this design was developed as training content aimed at promoting sustained attention and strengthening self-regulation.

Delayed gratification training. (a) A stage in which the participant achieves rewards through waiting by regulating time during the execution process. (b) A stage that maintains game continuity by offering bonuses in the next level based on evaluation scores. (c) A stage where intermediate rewards are given for accurate performance and rule-compliant actions during gameplay, enabling training in self-regulation and impulse control through sustained concentration.
Experimental methods
As shown in Figure 6(A), the digital content used by the experimental group incorporated a story-based game format specifically designed to enhance self-regulation and impulse control. By contrast, as illustrated in Figure 6(B), the content used in the control group was primarily based on answer-guided modules originally developed from traditional apprenticeship-style teaching methods. Both types of content functioned as digital therapeutic interventions to support treatment but differed in their initial content-design approaches. Accordingly, 15 participants were assigned to each group (experimental and control) to evaluate the effects of the respective content formats.

Differences in content according to the design approach. (A) Individually tailored design for therapeutic purposes (experimental group). (a) Content that responds to external stimuli such as sound. (b) User input results based on the task performance process. (c) Content modified through quantitative evaluation. (B) Complex cognitive design (control group). (d) Screen presenting a problem. (e) Screen for selecting an answer. (f) Screen where the user performs tasks and matches the correct answer.
All participants completed the digital content training program over a period of 4 weeks, totaling 20 sessions, with five sessions per week, each lasting approximately 25–30 min per day. While individual variation was allowed, the program was designed to prevent continuous use exceeding 1 hour per day.
Evaluation tool
Korean version of the child behavior checklist (K-CBCL)
The child behavior checklist (CBCL) was developed in 1983 by American psychologists Achenbach and Edelbrock. 37 This is a standardized instrument completed by caregivers to assess social adaptation, emotional functioning, and behavioral problems in children and adolescents. It is widely used as a benchmark for behavioral assessment. This tool provides T-scores based on age and gender, making it particularly suitable for evaluating children and adolescents in their developmental stages. The Korean version of the CBCL (K-CBCL) has been standardized for the Korean population, with two versions available: one for young children aged 1.5–5 years and the other for children and adolescents aged 6–18 years. 38 The tool consists of two major domains: an adaptive functioning scale and a syndrome scale for problem behaviors. The former includes eight subscales related to social functioning and five subscales related to academic performance. The latter comprises 10 subscales and two DSM-oriented subscales, which are combined into a total problem behavior score. Each item is rated on a four-point scale (0–3), with higher scores indicating more severe problems. In particular, the K-CBCL is completed by the child's parents, with the adaptive scale measuring domains such as sociality and academic performance; the problem behavior syndrome scale consists of 107 items across nine subscales, including withdrawal, attention problems, and aggression. A T-score of 64 or above (92nd percentile) is considered to meet the clinical threshold. 39
In addition to the syndrome scales, the CBCL provides indices for internalizing and externalizing problem scales. The internalizing problem score is derived by summing subscales such as anxiety/depression and withdrawal, whereas the externalizing problem score is based on subscales related to rule-breaking and aggressive behaviors. 40 Accordingly, this study tracked total problem behavior scores, internalizing and externalizing scores, and their rates of change using the K-CBCL. As such, the digital content used in this study was designed to help identify both adaptive functioning and problem behaviors. These elements can be applied stepwise throughout the gameplay and execution processes. This design framework may also be applicable to the development of future digital therapeutic interventions.
FAIR attention test (FAIR; Frankfurter Aufmerksamkeits-InventaR)
The FAIR Attention Test, developed in 1995 by Moosbrugger et al. in Germany, is a psychological assessment tool used to measure attention over a wide age range from 8 to 85 years. 41 The ability index (P) indicates the number of test items completed by the participants, reflecting the amount of information processed within a given time. The Control Index (Q) represents the proportion of correct responses among all responses, indicating the accuracy of performance. The persistence index (C) evaluates the degree and consistency of attention over time. Hence, it is a measure of attentional persistence. 42 The Korean version of the FAIR Attention Test has demonstrated high internal consistency, with Cronbach's alpha coefficients ranging from 0.90 to 0.95 across all items.
Accordingly, this study applied the ability index (P), which indicates the number of items accurately processed during the attention task, and the control index (Q), which reflects response accuracy as the proportion of correct responses among all responses. The persistence index (C) was also used to assess the consistency and continuity of attention during the given task. Through this test, digital content was evaluated for its effectiveness in training attention by measuring selective attention in response to visual stimuli and its ability to sustain attention. This included the assessment of self-regulation skills, such as impulse control, maintaining focus despite distracting stimuli, and responding appropriately to relevant cues.
Analysis methods
The evaluation results for children with ADHD were statistically analyzed based on the type of content provided to the study participants. The analysis was performed using the original data without any data substitution. All statistical analyses were conducted using SAS software (version 9.4; SAS Institute, Cary, NC, USA). Descriptive statistics included the number of participants, means, standard deviations, medians, and minimum and maximum values.
For between-group comparisons, if normality was satisfied, an independent two-sample t-test was conducted; otherwise, the Wilcoxon rank-sum test was used. Changes in the experimental and control groups before and after the intervention were analyzed using paired t-tests. For comparisons among more than three groups, one-way ANOVA was applied. 43
To evaluate the differences in the changes between groups after the intervention, ANCOVA (analysis of covariance) was performed, adjusting for baseline scores as covariates. 44 This allowed for the correction of potential group differences at baseline and enabled the accurate evaluation of intervention effects. Participants’ general characteristics are presented using frequencies, percentages, means, and standard deviations. The homogeneity of the general characteristics between the experimental and control groups was tested using Fisher's exact test. 45
All statistical tests were two-tailed and performed at a significance level of 0.05. 46 Given the pilot scope, we did not apply any multiplicity correction, and p-values are presented as unadjusted (nominal) values. Interpretation prioritized an estimation-based approach grounded in effect sizes. Numeric values, such as means, standard deviations, and percentages, were rounded to two decimal places (nearest third decimal place), and p-values were reported to three decimal places. In addition to statistical significance, effect sizes have also been reported. For paired t-tests, Cohen's d was calculated, with interpretation thresholds of 0.2 (small), 0.5 (medium), and 0.8 (large). 47 In the ANCOVA analyses, partial eta squared (η2) was used to estimate effect size, with thresholds of 0.01, 0.06, and 0.14 interpreted as small, medium, and large effects, respectively. 48
Results
Characteristics of the study participants
Participants’ characteristics are listed in Table 1. In the experimental group, there were 13 boys (81.3%) and three girls (18.7%), whereas in the control group, there were 11 boys (68.7%) and five girls (31.3%). In both groups, there were fewer girls than boys. However, there was no statistically significant difference in gender distribution between the groups (p = 0.683). The mean age was 8.63 ± 1.86 years in the experimental group and 9.02 ± 0.56 years in the control group, with no significant difference between groups (p = 0.68). No comorbid conditions that could interfere with the study were identified during the individual interviews.
Information on the participating children.

* Fisher's exact test, ** Student's t-test (p > 0.05).
K-CBCL score analysis
The total, internalizing, and externalizing problem behavior scores from the K-CBCL, along with their respective change rates, are presented in Table 2 and Figure 7.

Rate of change in K-CBCL final scores. (a) K-CBCL Total Behavior Problems. (b) K-CBCL Internalizing Disorders. (c) K-CBCL Externalizing Disorders. (d) K-CBCL Rate of Change.
Changes in K-CBCL indicators of self-regulation and impulse control.

*Student's t-test, **baseline vs. 4 weeks paired t-test, ***baseline-adjusted ANCOVA, #Cohen's d, ##partial η2.
In the control group, the total problem-behavior score decreased significantly from baseline to week four (t = 2.45, p = 0.024). However, in the experimental group, the change from baseline to week four was not significant (t = 1.61, p = 0.122). There were no significant differences between the two groups in terms of baseline scores, week four scores, or rates of change (t = 0.94, p = 0.177; t = 1.30, p = 0.204; t = 1.03, p = 0.313, respectively).
However, after adjusting for baseline as a covariate, the between-group effect size (partial η2 = 0.085, 95% CI [0.007, 0.353]) was of at least medium magnitude. Although statistical significance was not achieved, we interpret this as an exploratory, estimation-based signal that warrants further confirmation. There was a significant difference in internalizing problem scores between the two groups at week four (t = 2.34, p = 0.031). After adjusting for baseline as a covariate, the between-group difference in the 4-week scores was statistically significant (F = 6.82, p = 0.015, partial η2 = 0.105, 95% CI [0.002, 0.381]). As this was a pilot study, we prioritize an estimation-based interpretation, and the reproducibility of these effects should be confirmed in larger, longer studies.
Regarding externalizing problem scores, a significant difference was observed between the groups at week four (t = 2.39, p = 0.026), and the experimental group showed a significant reduction from baseline to week four (t = 2.16, p = 0.046). However, given the 4-week intervention period and the limited sample size, the clinical interpretation should be made with caution. After adjusting for baseline scores, the between-group differences remained significant (F = 5.64, p = 0.025, partial η2 = 0.094, 95% CI [0.005, 0.366]). A significant difference in the rate of change was observed between the two groups (t = 2.33, p = 0.033). The externalizing problem behavior score for the experimental group decreased by −16.00%, which was nearly twice as large as that for the control group (−8.75%). However, considering the 4-week intervention and the limited sample size, clinical interpretations should be made with caution.
Frankfurter Aufmerksamkeits InventaR (FAIR)
The FAIR assessment was used to analyze the attention indices, including the Ability Index (P), Control Index (Q), and Persistence Index (C), before and after treatment, as shown in Table 3 and Figure 8.

Rate of change in final FAIR scores. (a) Performance value (P-standard score). (b) Quality value (Q-standard score). (c) Continuity value (C-standard score).
Rate of change in FAIR indices related to self-regulation and impulse control.

*Student's t-test, **baseline vs. 4 weeks paired t-test, ***baseline-adjusted ANCOVA, ##partial η2.
Analysis of the Ability Index revealed a significant difference in the P-percentile between the experimental and control groups after 4 weeks (t = 2.40, p = 0.024). In addition, the P-standard score showed a statistically significant increase in the control group from baseline to 4 weeks (t = 2.24, p = 0.042).
For the Quality Index, the Q-percentile showed a statistically significant increase in the experimental group from baseline to week four (t = 2.52, p = 0.022). After adjusting for baseline scores as a covariate, a significant difference in the Q-percentile was observed between the groups at week four (F = 5.53, p = 0.027, partial η2 = 0.092, 95% CI [0.005, 0.363]). Similarly, the Q-standard score also showed a significant increase in the experimental group from baseline to week four (t = 2.33, p = 0.034).
Finally, analysis of the Persistence Index revealed a significant difference between the experimental and control groups in the C-percentile at week four after adjusting for baseline scores (F = 4.42, p = 0.045, partial η2 = 0.108, 95% CI [0.002, 0.385]). For the C-standard score, a statistically significant difference between the groups was confirmed after adjusting for baseline scores (F = 5.29, p = 0.028, partial η2 = 0.095, 95% CI [0.004, 0.368]). Given the limited sample size and the 4-week duration, these findings should be interpreted exploratorily, with an emphasis on effect sizes and their 95% confidence intervals.
Discussion
Principal findings
In this pilot study, children who received the story-driven, game-based digital therapeutic intervention showed more consistent improvements in parent-reported emotional and behavioral problems and in selective aspects of attention performance than those who engaged in the question-and-answer–based training. The game-based intervention was associated with reductions in both internalizing and externalizing symptoms, as well as gains on attention indices that reflect more efficient and regulated task performance, whereas the control condition demonstrated more limited or inconsistent changes. Taken together, these patterns provide preliminary evidence that explicitly aligning the design of digital therapeutic content with self-regulation and impulse-control constructs may yield short-term clinical benefits beyond those achieved by structurally similar but less content-aligned training.
Theoretical contribution
Similar to our research, another study employed a narrative-centered, game-based intervention for adolescents with ADHD. While that research focused on reducing risky alcohol use, both studies share the common goal of enhancing self-regulation through theory-driven digital interventions. 49 In this study, a DTx designed to target self-regulation and impulse control produced, after 4 weeks, reductions in K-CBCL internalizing and externalizing scores and improvements in selected FAIR indices (P, Q, C), suggesting that narrative-/game-based approaches may translate into measurable clinical improvements.
Previous studies have reported that interventions such as video games, specialized physical exercise programs (e.g., taekwondo, cycling), and music activities are effective for improving attention and complex cognitive abilities in children with ADHD.40,50,51 Such findings can be interpreted as cases in which programs developed to intervene in hyperactivity and attention deficit in children with ADHD were used as training tools. Our finding of reduced externalizing scores together with improvements in FAIR accuracy (Q) and consistency (C) suggests that, rather than merely optimizing item-level correctness, task and feedback structures explicitly aligned with the constructs of attentional control and impulse inhibition may be more effective.
In this study, self-regulation and impulse inhibition were set as the primary targets, and the basic design of the content was developed based on factors derived from ADHD-related assessment tools, such as the K-CBCL and FAIR. These assessment tools incorporate both qualitative and quantitative elements that allow the implementation of content in a variety of formats.
By analyzing the determinants identified by such training and assessment tools, it is possible to provide digital content that corresponds to these factors. Children with ADHD may engage with training tools embedded with these factors through digital content, often without direct awareness of the intervention.
The qualitative components of the content were related to individual psychological characteristics and were used to minimize the performance variability that may have arisen depending on the participants’ choices during gameplay. Quantitative components refer to numerical outcomes such as final scores, which can be integrated into the content by assigning different weights based on the score achieved. Our findings provide preliminary support that these design choices—minimizing answer-driven drills, emphasizing mission success with delayed rewards, and incorporating inhibitory-choice loops—may translate into improvements in clinical outcome measures.
Practical implications
Traditionally, digital therapeutic interventions aim to improve complex cognitive abilities, including attention, by training users with stepwise changes in accuracy rates. By contrast, for game-based content that deviates from this traditional framework, the weighting of individual correct answers is reduced, and scores are assigned according to the success rate of sequential performance missions. This approach enables the quantification of qualitative variability, thereby allowing for a more consistent quantitative evaluation.
The digital content design used in this study was intended to promote self-regulation by guiding users to act with clear goals during mission tasks. The stepwise feedback provided (reinforcement elements) was structurally linked to goal-setting and mission completion, supporting users in inhibiting impulses and successfully completing tasks. Therefore, the future development of digital therapeutic interventions for children with ADHD should consider the elements highlighted in relevant assessment tools during the content-design process.
In the present study, the K-CBCL-Total score, which was used as a measurement tool, reflected the overall level of cognitive and behavioral regulation and broadly captured difficulties in self-regulation. Although the difference was not statistically significant, the effect size was moderate or high. This is interpreted as an exploratory, estimation-based signal requiring further confirmation. The K-CBCL-Internalizing subscale assesses problems related to self-expression, such as anxiety and depression, while the K-CBCL-Externalizing subscale measures impulsivity in outward behaviors, such as aggression, defiance, and rule-breaking, thereby indirectly reflecting the level of impulse control. 52 In this pilot study, the experimental group demonstrated significantly greater improvement than the control group in both the internalizing (K-CBCL-Internalizing) and externalizing (K-CBCL-Externalizing) domains. This may be interpreted as reflecting the influence of the content-design model implemented for children with ADHD; however, given the limited sample size and the 4-week duration, clinical interpretations should be made with caution.
Additionally, we used the FAIR P-percentile, Q-percentile, and C-percentile as indicators of impulse inhibition and self-regulation. 41 Significant increases were observed for some indices, suggesting conceptual alignment between the content-design components and the treatment-oriented assessment measures. The observed effect sizes were generally of moderate magnitude; however, given the pilot scope, the clinical implications should be interpreted exploratorily. Confirmation of reproducibility and clinical validity will require larger, longer, multisite studies.
These findings suggest that, in the future, the development of digital therapeutic content aimed at replacing pharmacological treatment for ADHD should be guided not only by therapeutic objectives but also by criteria that ensure sustained effects and adaptability to user changes. Furthermore, as demonstrated by the results of this study, it is crucial to recognize the need for personalized content tailored to user states and therapeutic goals. If, as hypothesized in this study, the design of digital intervention content can influence therapeutic effectiveness, further research is warranted to advance both development and clinical validation in this field.
Limitations
This study has several limitations. The relatively small sample size and implementation of the intervention as an adjunct to pharmacological treatments may restrict the generalizability of the findings. Furthermore, this study focused exclusively on self-regulation and impulse inhibition without extending the therapeutic objectives to other relevant domains, which should be addressed in future studies.
In addition, the assessment of social functioning in this study relied on the caregiver-reported K-CBCL and was therefore indirect and limited in scope.
Accordingly, future studies should incorporate long-term follow-up (at one year) and expand outcomes by adding teacher reports, academic achievement, behavior records, and social functioning to evaluate sustained improvement. The present study also has certain cultural limitations related to being conducted within a single country and a single institution. There are, moreover, potential constraints stemming from the regional familiarity of characters and task procedures. Therefore, future research should consider more globalized characters and task methods, as well as research designs based on multiple institutions.
Based on the findings of this study, the future development of digital therapeutic content should be grounded in the theoretical background of assessment tool components that align with therapeutic objectives. In addition, elements such as character design and task environment should be systematically structured based on quantitative evidence to optimize treatment outcomes. The further development of diverse digital content incorporating a wide range of components suitable for use as an adjunctive therapy to medication will likely be necessary. 53
Conclusion
This study suggests that a story-driven, game-based digital therapeutic intervention, whose content is aligned with self-regulation and impulse-control constructs, may produce more consistent short-term improvements in emotional and behavioral problems and selective aspects of attention performance in children with ADHD than a structurally similar question-and-answer–based program. By demonstrating added benefit beyond the commonly used training format, this study highlights the potential value of moving from generic digital training toward content-centered interventions that more directly target the processes they aim to change.
Beyond the clinical outcomes, this work contributes a content-centered design framework for digital therapeutics. We systematically mapped self-regulation and impulse-control constructs onto in-game situations, response options, and feedback rules and embedded opportunities to practice self-monitoring, delay of gratification, and response inhibition within a narrative-driven, game-based environment. This approach could inform the development of future digital interventions that seek to balance engagement with therapeutic specificity, providing a practical example of how theory-driven content design can be operationalized in a pediatric ADHD context.
Future research can build on these preliminary findings in larger, adequately powered, more diverse samples to evaluate the robustness and generalizability of the observed patterns. Beyond simply replicating the effects, it will be important to examine whether content-centered digital therapeutics can drive meaningful change in everyday functioning across home, school, and peer contexts. Comparative studies that vary the degree and nature of content alignment, incorporate objective digital behavioral markers, and explore personalization based on baseline profiles could further clarify how to design digital therapeutics in combination with pharmacological and psychosocial treatments for children with ADHD.
Footnotes
Ethical considerations
Approval was obtained from the Institutional Bioethics Review Committee before data collection and evaluation (Keimyung University Dongsan Hospital; Institutional Review Board no. 2022-12-020, approval on January 2, 2023).
Consent to participation
Participants and their guardians provided written consent to participate in the study.
Consent for publication
All authors are aware of and agree to the publication of this manuscript.
Author contributions
Conceptualization, S.-C.K.; formal analysis, S.-C.K.; writing—original draft preparation, S.-C.K.; writing—review and editing, S.-C.K. and H.L.; data curation, S.-C.K.; software, S.-C.K.; project administration, S.-C.K.; investigation, H.L.; resources, H.L.; methodology, H.L.; validation, H.L.; supervision, H.L. Data curation, S.-Y.L.; Formal analysis, S.-Y.L.; Investigation, S.-Y.L.; Methodology, S.-Y.L.; Resources, S.-Y.L.; Visualization, S.-Y.L.; Validation, S.-Y.L.; Writing—review & editing, S.-Y.L.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was prepared as part of the project “2024 AI-Based Brain Disease Digital Medical Device Demonstration Initiative,” which was selected by the National IT Industry Promotion Agency (NIPA) under the Ministry of Science and ICT. It was conducted under the auspices of Daegu City, with support from the Daegu Digital Innovation Promotion Agency (DIP) as the lead organization.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.