
Abstract
Introduction
Short messaging service has the potential to improve participation in physical activity in individuals with long-term health conditions. However, successful implementation relies on participant engagement with such programmes. The aim of this study was to undertake a systematic review of qualitative literature exploring participant perspectives of short messaging service-based interventions designed to promote physical activity for people with long-term health conditions.
Methods
CINHAL, MEDLINE, SPORTSDiscus, Scopus and Web of Science were searched up to 15 February 2021 looking for participants’ perspectives on short messaging service programmes designed to promote physical activity in people with long-term health conditions. Included studies were analysed using thematic synthesis.
Results
Eight studies involving 533 participants were included and analysed using the principles of thematic analysis and 10 descriptive themes were identified. These descriptive themes were further refined to develop five final analytical themes: taking control of my own health, from information to action, relationship with the programme, perfection required for success and increased expectations.
Discussion
The findings agree with published work on the factors which influence behaviour. The findings from this synthesis demonstrate that automated short messaging service programmes to increase physical activity are generally acceptable. People report that these interventions support and encourage physical activity. The novel finding of this study was that having more regular and long-lasting contact has the potential to increase the expectations people have of healthcare services. This is a finding which needs to be considered and managed but should not discourage the use of automated short messaging service.
Keywords
Introduction
Healthcare resources cannot keep pace with consumer expectation, particularly in the area of long-term conditions.1,2,3 Information and communication technologies (ICTs) have created an opportunity for healthcare to adapt, supplement or even replace face-to-face contact. This has the potential to increase access, decrease costs and reduce the burden on clinicians. 4
In a recent bibliometric review, Müller and colleagues identified an increase in research using ICT to promote physical activity. 5 Mobile phones provide an accessible form of ICT with the number of phones exceeding the current global population. 6 Short messaging service (SMS) is ubiquitous, and SMS-based interventions have been shown to prompt behaviour change and improve health outcomes in many healthcare settings.7,8 This suggests that SMS has the potential to improve participation in physical activity in its broadest definition, 1 including in specific exercise programmes, in a variety of populations. However, successful implementation relies on participant acceptance of, and engagement with such programmes.
The aim of this study was to undertake a systematic review of peer-reviewed qualitative literature exploring participant perspectives of SMS-based interventions designed to promote physical activity for people with long-term health conditions.
Methods
Design
A systematic review with thematic synthesis of qualitative data was undertaken. The systematic review was conducted in accordance with the PRISMA guidelines (Figure 1). 9 No protocol was registered for this review.
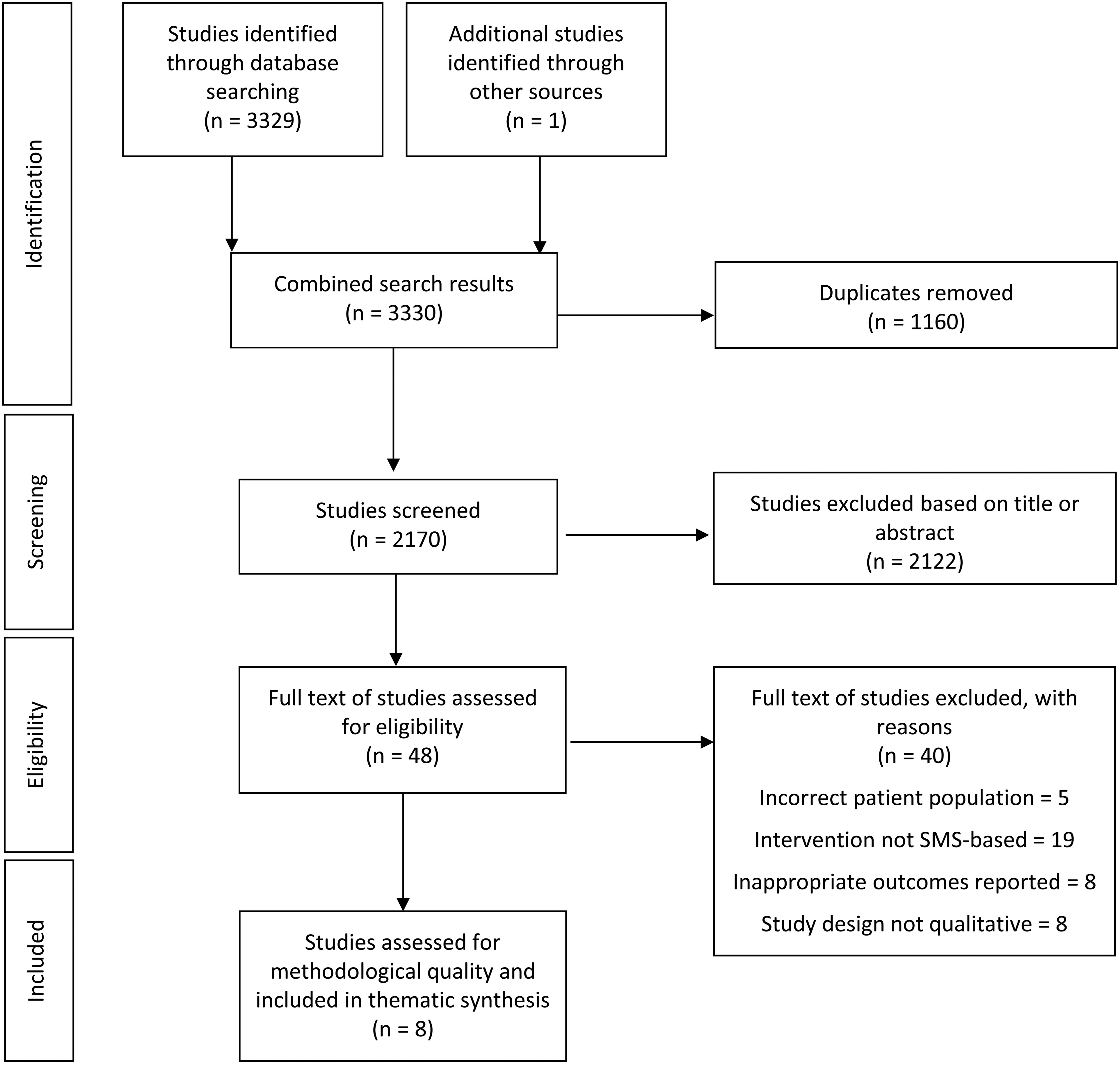
PRISMA flow diagram.
Identification of studies
A search was undertaken up to 15 February 2021 using CINHAL, MEDLINE, SPORTSDiscus, Scopus and Web of Science, with no restrictions placed on publication date. The search strategy combined terms for study design (qualitative), population (long-term condition, elective surgery), intervention and mode of delivery (physical activity, exercise, SMS and m-health) and participant experience (acceptability, experience). A full list of search terms can be found in online Supplemental material. Reference lists of final articles were manually screened to identify relevant studies missed in the primary search.
Study inclusion criteria
Studies were included if they met the following inclusion and exclusion:
Study design and reporting: Included studies were qualitative, mixed methods with an independently reported qualitative component, available in full text, and published up until 15 February 2021. Those that were not in English, not peer-reviewed, or that were conference proceedings were excluded.
Population: Included studies involved adults with a long-term condition, and those who accessed an inpatient or outpatient service. Physical activity programmes are an important component of recovery after surgery, so this population was also included. Studies involving participants who were overweight or obese, without other long-term conditions, were excluded.
Intervention: Studies investigating intervention delivery using automated SMS to participants with a standard mobile connection, and those promoting physical activity-based rehabilitation were included. Those that did not deliver messages directly to participants (e.g. only delivered messages to family members) were excluded.
Outcome: Studies were included if they contained direct quotations of participant perspectives, experiences, suggestions and opinions concerning the intervention, or if the survey studied had free text responses expressing opinions. Studies were excluded if they reported results from closed question surveys, health-related quality of life or screening questionnaires, or the perspectives were from participants’ family members, caregivers or healthcare professionals.
Study screening and selection
Articles were downloaded and imported into Endnote X8 ® software. Duplicates were removed in Endnote X8 ®. Initial screening of titles and abstracts was completed by JG and KH (research assistant) using the inclusion criteria. Disagreements were discussed until a consensus was reached. Where this was not possible, NS acted as arbitrator. Full texts of all remaining studies were read by JG and KH independently and discussed. Again, NS acted as an arbitrator when consensus could not be reached.
Study quality assessment
There is little consensus on whether the quality of qualitative literature can or should be assessed. 10 For the current study, as suggested by Majid and Vanstone, 11 the CASP qualitative appraisal tool was used. 12 Regardless of quality, all studies meeting the inclusion criteria were included in the analysis; allowing readers to draw their own conclusions.
Data extraction and analysis
The included studies were imported into NVivo 12 Plus ® software and analysed using principles from an established protocol of thematic analysis and thematic synthesis by Thomas and Harden. 10 Any text pertaining to participant perspectives of automated SMS-based interventions to promote physical activity were identified. Two researchers (JG, KH) independently completed line-by-line coding of relevant data and developed initial codes to summarise ideas presented in the text. These were then compared, and new collated codes were created to capture the agreed meaning of the portions of text, referring each time to their meaning in the context of the original study. Final codes were grouped into descriptive themes to summarise the original findings of the data. Descriptive themes stayed close to the original context and data of the original studies. The final stage of data analysis required a process of developing themes not wholly grounded in the data from individual studies. The process of developing higher-order analytical themes was initially undertaken by JG and KH. These were then presented to a group of more experienced researchers (NS, VS). The data were interrogated for insights which would answer the original question and inform clinical practice. Online Supplemental material demonstrate the process of moving from initial codes through descriptive themes to analytical themes. This process was unavoidably linked to the background and experience of the team. The iterative process included researchers with a range of experience which helped to ensure generalisability of the results. 10 KH was a final year physiotherapy student and JG a junior physiotherapist. They were supervised by NS who is a physiotherapist with extensive clinical experience with this patient population, and expertise in this research methodology. VS also has considerable clinical experience as a physiotherapist and is part of the research team.
Results
Search results
The search of electronic databases identified 3329 publications; one further publication was identified from screening reference lists of relevant articles. After removal of duplicates, 2170 studies remained, 2122 of which were excluded after the review of titles and abstracts. The full texts of the remaining 48 articles were screened, of which 40 were excluded with reasons. Eight articles were identified for inclusion in the thematic synthesis.13–20
Study characteristics
Study designs included mixed methods,13,15 a qualitative component as part of a randomised controlled trials (RCTs),16,19,20 and primary qualitative studies.14,17,18 Participants had low back pain, 18 non-small cell lung cancer, 15 breast cancer, 16 hypertension, 17 heart disease13,19,20 or underwent elective joint arthroplasty. 14 Studies were completed in six countries and in a range of socio-economic environments.
The eight studies collected data from 533 participants. Fewer than half (159) participated in face-to-face interviews or focus groups the remaining participants (374) provided feedback either via phone interviews or surveys allowing free text responses.13–20 All included RCTs collected qualitative data from only a sample of participants.13,15–17,19,20 Studies used the following methods to analyse data: thematic,13,16,17,19 content, 15 constant comparative, 20 phenomenological analysis with systematic text condensation, 18 and descriptive presentation of satisfaction data with participant quotes. 14 Further details of the included studies are presented in Table 1.
Summary of studies included in thematic synthesis of automated short messaging service (SMS) interventions.

n, number of participants; RCT, randomised controlled trial.
Methodological quality
When the CASP criteria was applied, all studies had included study aims, justified use of the methodology, collected data appropriate to the research question, and clearly presented findings. Only four studies satisfied all elements of the CASP criteria.13,15,16,18 One criterion, the relationship between researchers and participants, was inadequately discussed in three of the studies.14,17,20 There was generally a lack of clarity as to how study findings contributed to existing knowledge, the impact on clinical settings and the generalisability of results to other populations. Further details can be found in online Supplemental material.
Results of analysis
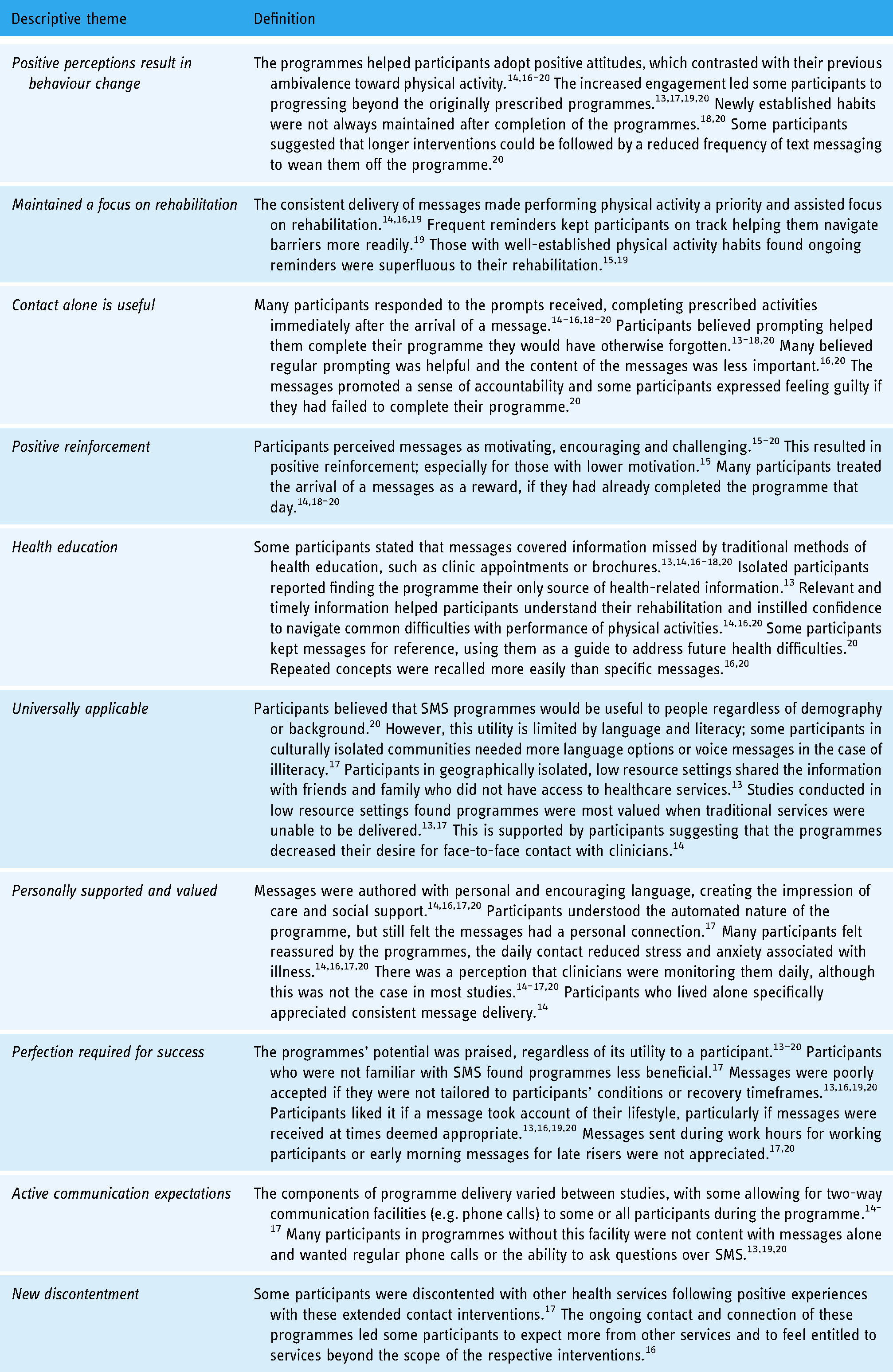
Initial analysis yielded codes that were then collated to create 10 descriptive themes. These are defined in Table 2, using examples from the included studies.
Descriptive themes and definitions.
The descriptive themes were then used to derive five analytical themes (Table 3). A detailed diagram of the derivation of each analytical theme can be found in online Supplemental material.
Link between descriptive and analytic themes.

Analytical theme 1:
From information to action
Participants noted being overwhelmed by information presented to them during the treatment process, making understanding and remembering information difficult, specifically regarding exercise and physical activity. Receiving the same information in manageable portions, in a familiar environment, via SMS messages, allowed participants to remember and apply the advice to their everyday life. The added advantage of being able to refer to SMS messages allowed participants to undertake activity with increased confidence, increasing the likelihood of physical activity becoming habitual.
Analytical theme 2:
Taking control of my own health
Practical and psychosocial elements of the programmes seemed to encourage participants to adopt a more positive mindset, helping participants recognise that successful rehabilitation required taking ownership of their own health. Incremental adaptation of physical activity-related behaviour resulted in decreased reliance on the programmes, as physical activity became a valued and important component of participants’ lifestyles. Participants reported having a greater commitment to personal goal setting and increased engagement with physical activity programmes. Occasionally this commitment went beyond basic engagement, with some participants planning their schedules around physical activity or investing in gym memberships to progress their programmes. Once these behaviours had been integrated into everyday life, participants noted less difficulty overcoming barriers that previously limited their engagement in physical activity, such as forgetfulness and indifference.
Analytical theme 3:
Relationship with the programme
Many participants spoke about the messages as if they were from a trusted friend, rather than from an automated programme. This perception may have stemmed from the interaction with clinicians or researchers when the programme was commenced, and the personable language used in many of the messages. Messages were seen as a proxy for regular contact with a clinician and provided a similar sense of reassurance about recovery. This included explaining to the participant that occasional setbacks are likely, however, they are not a reason to stop physical activity.
Analytical theme 4:
Well received when well delivered
When programmes did not meet participants’ expectations or were delivered using messages that were not personally relevant, message fatigue developed. This resulted in loss of engagement with the programme and a subsequent reduction in the amount of physical activity undertaken. Participants reported that a poorly administered programme was worse than having no programme.
Analytical theme 5:
Increased expectations
The regularity of the contact can set an expectation of a level of contact which may not be able to be sustained. Providers could be at risk of creating an expectation for extended contact that is neither practical to deliver nor helpful in encouraging patient autonomy. This has the potential to result in dissatisfaction if the scope and purpose of the programme are not clearly explained at the outset of the intervention.
Discussion
This thematic synthesis has proposed five analytical themes which reflect consumers’ perceptions of SMS messaging. It is clear from these themes that SMS messaging interventions to support physical activity has good acceptability. The themes give some insights into considerations for future development of automated rehabilitation interventions. These may support a change in behaviour allowing people to engage in physical activity, independent of health care professionals. The first four themes from this research can be mapped on to a framework proposed by Michie and colleagues that helps understand factors such as

Findings from current synthesis (white) mapped onto the COM-B model (grey).
The final theme from this synthesis
This does not discount the applicability of automated interventions in clinical settings, and their use can still contribute to effective and acceptable care. They can be used as an adjunct in mixed delivery services,22,23 or at a point in rehabilitation when patient needs can be managed remotely and the user is willing and capable of engaging. A recent systematic review and meta-analysis of remotely delivered physical activity interventions found sustained between-group increases in physical activity at long-term follow-up. 24 This demonstrates that automated minimal contact has the potential to support people in maintaining physical activity.
Implications for practice
Automated SMS messages provide connectivity which appears to have benefits beyond those associated with physical activity. People report an ongoing sense of connection with the healthcare provider, especially those who are socially isolated or living alone and may not have the ability to regularly access services outside their home. Other authors have found similar themes when investigating perceptions of automated interventions in people with long-term conditions. 25
When prescribing a programme, people need to be given choices and where possible it should be tailored to an individual and their lifestyle. However, the benefits of automating a programme to enable widespread dissemination have the disadvantage of making individualisation and tailoring more difficult. Another limitation of current automation options is that most do not allow for two-way communication which is another frequently requested feature.
Next steps for research
Adverse events in these automated interventions are frequently poorly reported. 24 However, when they are reported, the number of incidents is low, the severity mild and most are unrelated to the intervention.26,27 Given the high acceptability and apparent low risk, the next step would appear to be to embed this as part of clinical practice.
Validated physical activity outcome measures could be used by participants and this data could be collected to allow auditing of the interventions. Outcomes could be measured using commercially available activity monitors such as wearable devices and phones or self-report telephone administered measures. 28
Strengths and limitations
A comprehensive search was conducted to identify literature exploring and analysing personal perspectives after participating in SMS interventions. Studies included culturally and socioeconomically diverse populations, from a range of countries. A wide range of people with a broad range of health long-term conditions were included in data collection and synthesis which increased the generalisability of results. Coding was completed by authors with different backgrounds resulting in a rich interpretation of ideas which was reflected in the analysis. A thorough methodological critique and summary have been presented to ensure transparency.
Most of the included studies were multifactorial and did not deliver a purely SMS-based intervention to promote physical activity. This increased the complexity of coding, requiring robust discussion to decide which results were relevant to the intervention of interest for this study. Debate exists in the literature regarding the classification of obesity alone as a long-term condition. Physical activity and behavioural interventions intended to exclusively promote weight loss were outside of the scope of this study. This limits the generalisability of these findings to this group of people.
Conclusion
Participants’ perspectives of automated SMS interventions were positive regardless of demographics health condition, or country of residence. There is a clear theme of people feeling supported and encouraged despite the lack of human contact. However, this is dependent on recipients being willing, and capable, of engaging and having their personal preferences considered. Given the high acceptability and low risk, there seems little reason not to implement these programmes as part of usual care to increase engagement in physical activity beyond what is currently provided.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076221113705 - Supplemental material for Participant perspectives of automated short messaging service interventions to promote physical activity: A systematic review and thematic synthesis
Supplemental material, sj-docx-1-dhj-10.1177_20552076221113705 for Participant perspectives of automated short messaging service interventions to promote physical activity: A systematic review and thematic synthesis by J Stefanus Grobler, Verna Stavric and Nicola L Saywell in Digital Health
Footnotes
Contributorship
KH contributed to the design, data collection and analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The ethics for the included studies are described within their methods.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
NLS.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.