
Abstract
Background
Mobile health interventions have emerged as a promising strategy in the global effort to enhance maternal and newborn care practices. In this study, we aimed to develop and test a context-tailored short message service (SMS)-integrated web-based application to improve maternal and newborn health in Ethiopia.
Methods
We conducted a system development and pilot usability testing study. We followed the stages of the waterfall model. Initially, we collected and systematically analyzed requirements from stakeholders to understand the desired outcomes of the application. During the development phase, we wrote the code to build application components, modules, and features. Finally, we tested the application through unit, prototype, and pilot testing to identify and resolve any defects before deployment.
Result
The system sends 78 key messages to pregnant women between 16 and 20 weeks of gestation, covering 10 thematic areas during pilot testing. The application features an interface for scheduling and automatically tailoring text messages based on the last menstruation period. Message delivery success was 97.4%, security and privacy features functioned at 100%, and network connectivity resilience was 98% in field simulations. User requirements and acceptability were evaluated through pilot testing with healthcare providers and end users, with high endorsement for message dispatch flexibility (96.4%) and distinct messaging features (92.9%). Usability test yielded a mean score of 92.3.
Conclusion
The application has been successfully developed and tested. It offers organized SMS scheduling and effectively tailors messages based on the pregnant mother's last menstruation period. The system provides timely health information, tracking pregnancies, facilitating remote consultations, and connecting women with local support groups. These findings indicate that mobile health is a viable strategy for improving maternal and newborn health.
Trial registration
Clinical trials PACTR202201753436676, 4 January 2022.
Background
Improving maternal health continues, nonetheless, to be one of the major global challenges. Indeed, maternal mortality rates remain extremely high, especially in low-income and lower-middle-income countries. Globally, the estimated maternal mortality ratio (MMR) stands at 223 maternal deaths per 100,000 live births. 1 In 2023, the MMR in Ethiopia was estimated at 195 maternal deaths per 100,000 live births. 2 Although efforts have been directed towards reducing maternal mortality over the past two decades, hundreds of thousands of women continue to die every year from pregnancy-and childbirth-related complications that could have been prevented, while the majority of such deaths still occur in resource-poor settings.3,4 Low literacy rates, widespread misinformation, and the need to travel long distances to reach health facilities place quality care well out of reach for many women.5,6 Despite efforts to improve the status quo, progress in maternal health remains hindered by numerous obstacles.7,8 One promising strategy to address challenges in maternal health care services is the utilization of mobile health (mHealth) to extend access to essential health information and quality services for pregnant women and their families.9–11
mHealth is a medical and public health practice supported by mobile devices, including mobile phones, patient monitoring devices, personal digital assistants, and other wireless tools.12–14 By leveraging mHealth technologies, it is possible to expand coverage of basic services such as prenatal care education, nutrition guidance, exclusive breastfeeding support, and other health-related information, enabling access to health resources anytime and anywhere. Moreover, the integration of mHealth into maternal and newborn health services can improve not only access to care but also communication and health information management, ultimately contributing to better health outcomes for mothers and newborns.15,16 mHealth also serves as an effective tool for sending short message services to track pregnancy progress, increase access to experienced providers, improve obstetric outcomes, enhance the quality of emergency services, strengthen capacity for direct client care, and reduce unscheduled visits.15,17
The effectiveness mHealth interventions depends on context, especially in low- and middle-income countries (LMICs) like Ethiopia, where limited network connectivity, intermittent power, low digital literacy, language diversity, and weak health system capacity hinder uptake; rural users often have basic phones, and studies in sub-Saharan Africa and Ethiopia report usability issues, language barriers, low awareness, and infrastructural constraints that make many tools designed for high-income settings unsuitable.18–20 To address this, our intervention was tailored to the Ethiopian context by using short message service (SMS) (not requiring internet or smartphones), creating simple content in Afan Oromo and Amharic, testing gain- and loss-framed messages, including key family influencers, and embedding data privacy and security safeguards appropriate for resource-limited settings, positioning it to overcome documented barriers and improve relevance and scalability.
For the past few decades, one of the major challenges in addressing maternal and newborn health through mobile phone-based messaging interventions has been the lack of effective messaging applications. In response, several messaging systems have been developed and implemented. For instance, Text4baby in the United States, 21 MomConnect in South Africa, 22 mMitra in India, 23 WeCare in Bangladesh, 24 the Technology for Maternal and Child Health (T4MCH) project in the Sawla-Tuna-Kalba district of the Savannah Region in Ghana, which implemented a mobile application known as Societe Generale de Surveillance (SGS) Collect to deliver weekly SMS and voice messages in local languages to increase maternal and child health services utilization, 25 and the Mobile Alliance for Maternal Action (MAMA) in countries such as South Africa and Afghanistan.26,27
The development and testing of mobile phone messaging applications have shown significant potential in improving maternal health outcomes through strategic message framing. This approach enhances women's knowledge, positively influences their attitudes, and boosts their self-efficacy. Strategic framing of text messages promotes greater engagement with healthcare services, leading to improved adherence to recommended practices and reductions in maternal morbidity. Testing has demonstrated that such applications not only enhances service utilization but also empower women with the knowledge and confidence to make informed health decisions, ultimately contributing to healthier pregnancies and lower maternal health risks.28,29
Several studies on the development and testing of mobile phone messaging applications for health interventions have commonly employed iterative and agile development methodologies commonly employed iterative and agile development methodologies, such as Scrum or Rapid Prototyping, which emphasize flexibility, frequent revisions, and ongoing user feedback.30,31 However, for the development of the application, the Waterfall Model was chosen due to its structured, linear approach, which is particularly effective when project requirements are well-defined and stable from the outset. This method ensures that each phase of development—from requirements analysis to design, implementation, testing, and deployment—is completed thoroughly before moving on to the next, reducing the risk of overlooking critical components. The Waterfall Model was suitable for this application because it allowed for careful planning and documentation, ensuring that the software was developed with a clear focus on its primary goal: enhancing maternal and newborn health through precise, well-monitored messaging interventions. 32
Despite extensive efforts worldwide, there remains a notable absence of effective mobile phone messaging applications specifically designed for maternal and newborn health in Ethiopia, particularly within the Jimma Zone. The primary objective of this article is to describe the design, development, and technical testing of the SMS—integrated web-based application—not to evaluate its clinical or public health effectiveness, which was rigorously reported in a separate article. 33
Method and materials
We conducted a system development and pilot usability testing study to design and evaluate a context-tailored mobile messaging intervention for maternal health in rural Ethiopia. This study was part of a large cluster randomized controlled trial. The proposed system is an interface solution based on mobile phone-based messaging. The application was designed locally by software programmers, and it manages scheduling and automatically dispatches messages. The application allows sending of previously developed 78 messages with gain framed or loss framed.
Mobile phone messaging application development process
We followed the waterfall model, which encompassed six distinct phases. At the outset of the project, we conducted a comprehensive requirements gathering and analysis by consulting a total of 28 stakeholders, including 12 healthcare providers, 10 pregnant women and their partners, four maternal and child health (MCH) experts, and two local ICT/telecom experts.
The local ICT/telecom experts were experienced professionals with extensive knowledge of mobile network operations, SMS/MMS delivery protocols, and Ethiopian telecom regulations. They were included to ensure the local feasibility of the messaging system by addressing network-related constraints, such as coverage limitations and message size capacity, optimizing delivery protocols for local networks, and resolving compatibility and reliability issues within the user environment. These experts played a pivotal role in providing technical input on software feasibility and integration with the local telecom infrastructure; however, they were not involved in the health-related components of the software.
This stage was used to define the scope and functionalities essential to the end-users, thereby informing the subsequent design and development process. In the second stage, we developed a detailed application design, including the architecture, user interface, database structure, and other technical components. This stage specified how the application would function and appear, ensuring that it met end-user requirements, was user-friendly, and adhered to technical constraints. The third stage involved implementing the design by writing code and building the application components using the Symfony framework.
The web application ulfamijuu was built with the Symfony PHP web framework (Symfony 7.4), which is a contemporary open-source framework for creating maintainable and scalable web applications using a modular, component-oriented approach. Symfony 7.4 is a long-term support (LTS) version, which requires the use of PHP 8.2 or later versions and is still supported for bug and security fixes. Therefore, based on our implementation of the core modules, backend organization, and database setup for ulfamijuu, the Symfony 7.4 framework enables structured backend programming, optimized routing, and secure database interaction through its library of reusable components and best practices. In the fourth stage, comprehensive testing, including unit testing, prototype testing, and pilot testing, was performed to verify that the application met the requirements and worked as expected, ensuring its reliability and intended operation.
During the unit-testing phase, individual components of the application were rigorously tested to ensure their functionality and performance. Five software engineers carried out the unit testing. The testing team assessed the functionality of specific features, such as message scheduling, SMS delivery, data encryption, and user interface elements, by isolating each component and validating its expected behavior against predefined criteria.
The prototype-testing phase, conducted after the initial design input, involved a partially overlapping but significantly broader group of stakeholders. While the initial design phase drew input from key stakeholders, the prototype testing group was expanded to include healthcare providers, software developers, Ethio Telecom experts, IT professionals, and health extension workers for a comprehensive system evaluation. This deliberate choice to use a broader and more representative group was justified on the grounds that it improves the external validity of the usability testing, reduces potential design-team bias by incorporating feedback from individuals not involved in the initial conceptualization, and simulates the eventual real-world use of the system more accurately by incorporating the perspectives of the primary end-users. Initial testing featured hands-on engagement and scenario-based assessments of key functions like message scheduling and SMS delivery. Feedback was collected through structured sessions, surveys, and discussions, identifying usability issues and areas for improvement. These insights guided technical refinements and re-testing until the prototype met performance standards, concluding with a final evaluation and approval from all stakeholders to ensure alignment with user needs.
The system has been pilot-tested in selected health facilities of Jimma Zone, Oromia Region, Ethiopia, with 30 pregnant women attending the ANC services in order to test the delivery capability of the mobile messaging application. This test, therefore, focused on the assessment of whether the system delivers the scheduled SMS messages on time, correctly in Afan Oromo and Amharic languages, and without technical problems in supporting multilingual messages. This involved real-time monitoring of dispatch, delivery success rate, and system error tracking. The fifth stage included the deployment of the application to a real environment, where training and support were provided to users for effective and efficient use. The sixth and final stage was maintenance, with sustained support through bug fixes, optimization of performances, and updating to meet the evolving requirements. This would guarantee that the application remains functional and reliable over time (Figure 1).

Development process flow diagram (waterfall model).
Software description
We developed and tested a short message service (SMS) integrated, web-based application. This web-based application facilitates timely, targeted communication with pregnant women m. The application is accessible for further information and updates at https://ulfamijuu.com/.
Modules of the application
The application features an interface for entering participant details, including name, gestational week, mobile phone number, message type, category, and language options, along with capabilities for report generation and feedback. The application also allows midwives or health workers to provide feedback on whether pregnant women received the advised services.
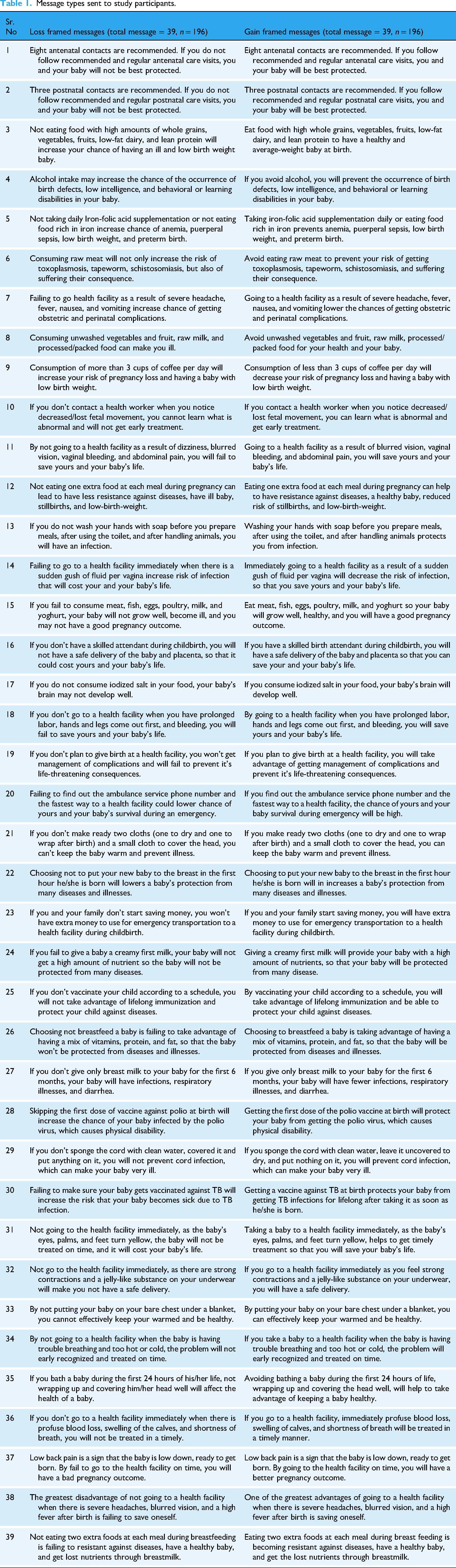
On the homepage of the application, accessed through an internet protocol (IP) address, users are presented with a user interface featuring a login option. The dashboard provides real-time activity metrics, including registered customers, scheduled messages, reminders, message types, and total users. The customer list functionality allows for the addition of new customers with their mobile numbers and last menstruation period, and users can categorize women into message types, choosing between loss frames or gain frames. In this study, we used message framing as a behavioral science strategy to communicate health information. Gain framing involves the focus on benefits or positive outcomes associated with the promotion of maternal health behavior (e.g. “If you visit ANC on a regular basis, you and your baby will have a chance to stay healthy”), while loss framing involves the focus on negative aspects or costs of failing to adopt a maternal health behavior (e.g. “Failure to visit ANC may result in complications for you and/or your baby”). Message categories enable the listing and scheduling of 11 primary message categories for educating pregnant women, while message subcategories facilitate the listing of subcategory messages within each category, linking them accordingly. Message types allow for further categorization of the 78 messages into gain-framed and loss-framed messages. The message list functionality enables scheduling based on the last menstruation period and utilizes Google Calendar techniques to identify appropriate messages for the targeted gestational age. The customer follow-up feature enables midwives to provide services and specify received services, while the customer attendance index tracks services provided by health facilities to the pregnant women under study.
The essential elements of system architecture
The system integrates multiple components, with the central element being a mobile phone messaging application that incorporates a Layer 3 Virtual Private Network (VPN), an SMS modem pool, a wireless adapter for desktop ping, short codes, message hunting, and central server components for secure communication. The Layer 3 VPN ensures secure communication between system components by linking customer-edge (CE) routers to provider-edge (PE) routers through peer routing. The SMS modem pool improves efficiency and reliability by managing message distribution across multiple modems, providing redundancy in case of modem failure. A wireless adapter installed on the desktop enables network communication, with the ping command used to test network reachability. Short codes, which are integral to the system, facilitate scalable message delivery, customer opt-ins, and quick information dissemination (Supplemental File 1).
Development and structure of text message interventions
The study utilized a total of 78 distinct text messages (39 pairs), which were equally distributed across the messaging approach into
Message types sent to study participants.
Data analysis procedure
All statistical analyses were conducted using IBM SPSS Statistics. For binary outcomes (e.g. success/failure in test scenarios, user requirement endorsements), we used SPSS's One-Sample Proportions and Binomial Test procedures to estimate proportions, confidence intervals, and significance tests. Proportions were computed as the number of positive responses or successful cases divided by the total sample size for each indicator. To quantify the uncertainty around each proportion, we obtained 95 % confidence intervals. In SPSS, confidence intervals for one-sample proportions and binomial tests were specified via the proportions procedure with exact methods of Clopper–Pearson using testtypes = exact and specifying confidence level. The Clopper–Pearson interval is based on the binomial distribution and inverts the exact test, providing exact confidence limits for proportions that do not rely on large-sample normal approximations. We also performed one-sample binomial tests in SPSS to compare each observed proportion against a predefined benchmark value of 0.90. This test evaluates whether the observed success rate differs significantly from the benchmark, generating an exact two-sided p-value when SPSS considers the sample size sufficient for exact inference. Both asymptotic and exact p-values were provided; where possible, we reported the exact (Clopper–Pearson) test p-values for greater accuracy in small samples. For scale-based usability measures such as the System Usability Scale (SUS), we computed mean scores and standard deviations (± SD). We also derived a 95 % confidence interval for the SUS mean using the standard error of the mean (SD/√n) to reflect uncertainty in usability estimates.
Data security and privacy
Personally identifiable information (PII), such as pregnant women's identities and contact numbers, is handled with strict security measures. Specifically, all PII is stored in an encrypted form on secure servers, and access is rigorously restricted only to authorized health personnel. Furthermore, all data transmission between the application and the servers utilizes secure communication protocols, such as HTTPS (Hypertext Transfer Protocol Secure), to prevent interception. These security protocols ensure the system's compliance with relevant ethical and data protection guidelines, as approved by the institutional review board.
Result
The development of the application took eight months and followed the steps outlined in the Waterfall model. Each phase of development-requirement analysis, development, and testing (unit, prototype, and pilot) was systematically completed, with findings from each stage carefully integrated into the subsequent phases.
Socio-demographic data
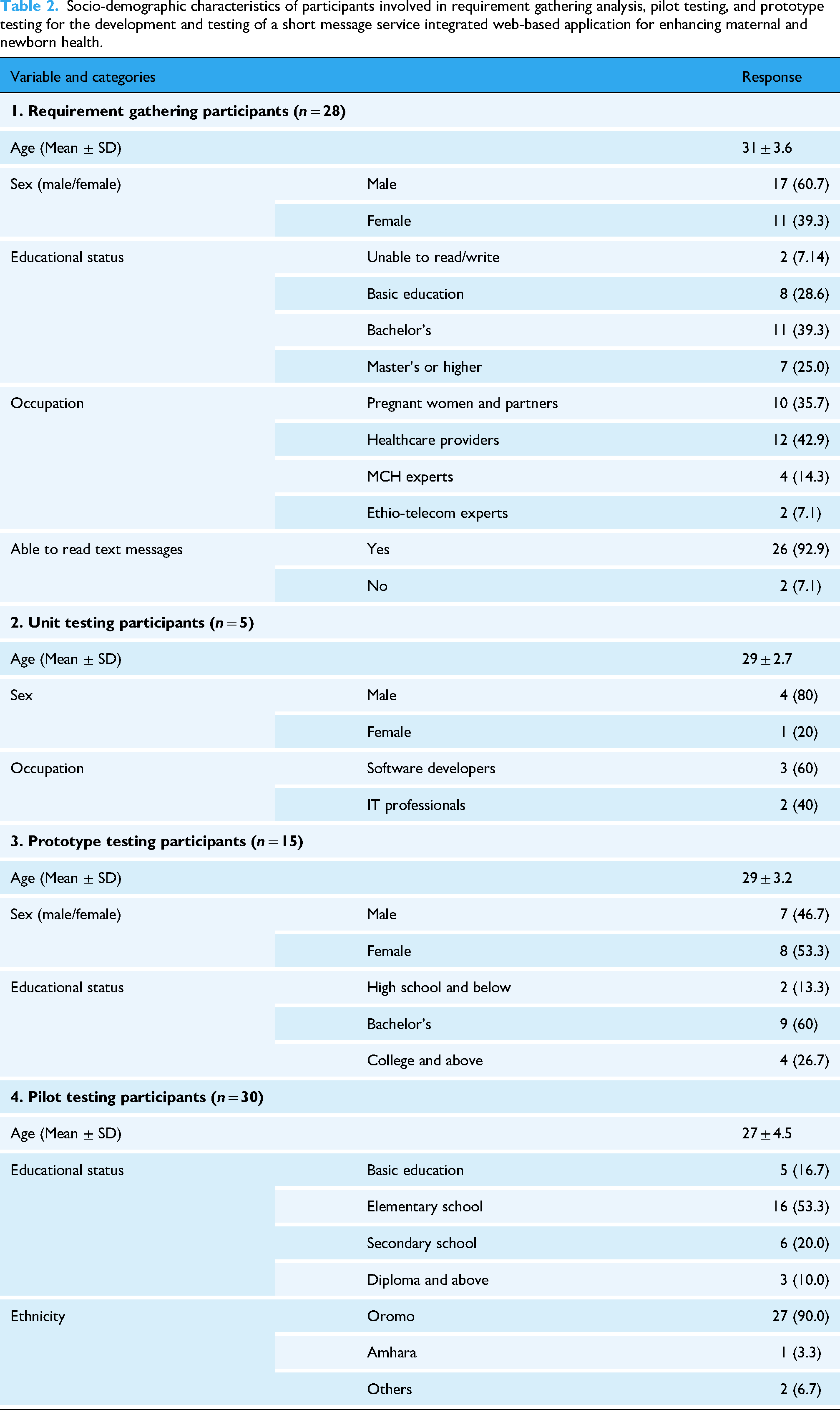
A total of 28 participants were involved in the requirements-gathering phase, with a mean age of 31 ± 3.6 years. Regarding educational attainment, 7.14% could neither read nor write, while 39.3% held a bachelor's degree. In addition, 92.9% reported that they were able to read text messages. Among these participants, 35.7% were pregnant women, 42.9% were healthcare providers, 14.3% were maternal and child health (MCH) experts, and 7.1% were Ethio Telecom experts.
Unit testing involved five participants with a mean age of 29 ± 2.7 years; 60% were software developers and 40% were IT professionals. Prototype testing was conducted with 15 participants, with a mean age of 29 ± 3.2 years, of whom 60% held a bachelor's degree. Pilot testing included 30 participants with a mean age of 27 ± 4.5 years. More than half of the participants had completed elementary school (53.3%), and the majority were Oromo (90.0%) (Table 2).
Socio-demographic characteristics of participants involved in requirement gathering analysis, pilot testing, and prototype testing for the development and testing of a short message service integrated web-based application for enhancing maternal and newborn health.
Application requirements analysis
Stakeholder needs analysis identified core functional and non-functional requirements for the SMS/MMS-based web application aimed at enhancing maternal and newborn health. Requirements were retained if ≥50% of respondents highlighted them, resulting in nine key requirement categories (Table 3). These guided system specification and design priorities.
Application requirement analysis from stakeholders for the development and testing of a short message service integrated web-based application for enhancing maternal and newborn health.

System design and implementation
The application was developed to automate the delivery of 78 maternal and newborn health messages, categorized by gain-framed versus loss-framed messaging. It includes features for participant information entry, message scheduling based on gestational age, report generation, and feedback capture by midwives and health workers. Implementation employed the Symfony 7.4 PHP framework, ensuring a maintainable, scalable backend with multilingual messaging support and integration with SMS/MMS delivery protocols.
Testing
The application passed three sequential tests. Each phase improved the functionality of the software, user experience, and reliability mutually to ensure that it would be fully ready to be deployed.
Unit testing
Unit testing evaluated the application across eight key dimensions—messaging capabilities, contact management, security features, network connectivity, system performance, database integrity, user interface consistency, and error handling and logging—selected to represent the critical functional and non-functional requirements of the system (Table 3). For each dimension, objective success metrics were predefined and assessed through repeated test scenarios, including success rates expressed as percentages of test cases passed, counts of errors per 100 test cases, response time thresholds in milliseconds for performance evaluation, and binary pass/fail outcomes for data integrity checks, thereby providing a rigorous and quantifiable measure of system reliability and robustness across all major functional components. Messaging capabilities, including SMS sending with delivery confirmation and error-handling mechanisms, were robust, which achieved 99% success rate in 100 test cases. It also supports message threading, sorting by time and topic, and it's able to handle a great volume of messages. Contact management features of the application performed perfectly, with a 100% success rate across 50 tests, allowing for the addition, editing, and deletion of contacts, as well as grouping by attributes such as last menstruation period (LMP), expected day of delivery (EDD), and postnatal schedules. Encryption, password protection, PIN lock, and even hiding messages from the lock screen were some of the security features vigorously tested with a perfect 100% success rate in 100 test cases. Network connectivity was reliable, keeping the flow of messages in 98% of the time without having any impact on network switching. The user interface was functional, thus easy to use. The application's performance under stress (e.g. high load) was also excellent, with 99% of tests passing successfully (Table 4).
Unit testing results for the development and testing of a short message service integrated web-based application for enhancing maternal and newborn health.

Prototype testing
Prototype testing indicated that the application was user-friendly and performed well across key areas, achieving a 99% success rate in usability, messaging, health tracking, security, and communication. Registration and scheduling for pregnant women were straightforward, although some healthcare providers experienced minor navigation challenges. Messaging and communication functions performed reliably with only slight delays. Health tracking and alert features were effective, although several users requested additional customization options. The application demonstrated high performance in status communication, error recognition, with a 98% success rate. However, there remains room for improvement in help and documentation, as well as multilingual support, which showed a relatively lower success rate of 80%. We recommend adding a personalized dashboard to track progress and milestones, enhancing system compatibility, and expanding multilingual support to further improve accessibility and overall user experience (Table 5).
Prototype testing result for the development and testing of a short message service integrated web-based application for enhancing maternal and newborn health.

Usability was measured using the SUS, which yields a standardized score from 0 to 100 with higher scores indicating better usability and a score of ≥70 considered acceptable based on established benchmarks; navigation efficiency was assessed by the task completion rate—the percentage of users who successfully completed predefined tasks (target ≥90%); messaging accuracy was measured as the proportion of correctly delivered messages during the prototype evaluation (target ≥98%); and language clarity was quantified using a post-task comprehension quiz, with the percentage of correct responses serving as the metric (target ≥85%) (Table 6).
Usability and functionality test result.

Pilot testing
The application was designed to send 78 key messages to pregnant women between 16 and 20 weeks of gestation, covering 10 thematic areas: nutrition, lifestyle modification, danger signs, birth preparedness, breastfeeding, labor, newborn care, immunization, and antenatal/postnatal care. Over a two-week period, the system was planned to deliver 78 messages, with each message sent every 3 days. The pilot testing of the mobile messaging application indicated high performance through various indications. Of the scheduled 78 messages for delivery, 76 were delivered at a delivery rate of 98%. User satisfaction was high, with 92.9% of the participants distinguishing the messages from promotional ones due to clarity and specificity. The application was also supportive in messages with multiple languages, such as Afan Oromo and Amharic, at a 100% rate. Although there were minor delays affecting 2% of messages due to network issues, the application maintained a 100% success rate in message frequency and coverage across 10 thematic areas. Overall, the pilot test indicates that the system is ready for broader implementation, with only minor enhancements recommended (Table 7).
Pilot test result for the development and testing of a short message service integrated web-based application for enhancing maternal and newborn health.

Summary of performance results
The system performed very well across key technical domains, with 99% success in messaging capability, 100% in contact management and security features, 98% in network connectivity, and 99% in performance under load, indicating high reliability and robust overall performance in pilot testing (Figure 2).

Summary of system performance results and success rates.
Behavioral outcomes
The effectiveness of the message content in driving behavioral change was rigorously reported in a separate manuscript. This dedicated study found that the SMS-based intervention—using both gain-framed and loss-framed messages—significantly improved key maternal health service utilization indicators compared to the control group. Specifically, utilization of Antenatal Care (ANC) increased significantly in both intervention arms. The gain-framed arm had an odds ratio (OR) of 5.40 (97.5% CI: 1.95–14.94), and the loss-framed arm had an OR of 7.14 (97.5% CI: 2.40–21.26) compared to the control. Similarly, utilization of Skilled Birth Attendance (SBA) rose substantially in the gain-framed arm (OR: 7.53 (97.5% CI: 2.20–25.79)) and the loss-framed arm (OR: 7.31 (97.5% CI: 2.13–25.09)). Postnatal care (PNC) also improved significantly, with the gain-framed arm showing an OR of 4.83 (97.5% CI: 1.71–13.67) and the loss-framed arm showing an OR of 4.07 (97.5% CI: 1.46–11.39). The intervention also significantly improved maternal health knowledge and reduced maternal morbidity. This robust evidence confirms that the message content and framing employed by the system were effective in promoting desired behavioral outcomes and improving key health indicators among participants.
Discussion
This study describes the development and testing of a mobile phone messaging application designed to improve maternal and newborn health through the use of message framing, an evidence-based communication strategy that emphasizes either the benefits of recommended health behaviors (gain-framed) or the risks associated with not adopting them (loss-framed) to influence health decision-making. The application delivers key messages on prenatal and postnatal care, nutrition, and other important maternal health topics to pregnant women to support informed health decisions and facilitate pregnancy tracking.
The app also facilitates involvement of family members by allowing pregnant women to optionally include additional phone numbers (e.g. husband or mother/mother-in-law) so that trusted family members can receive the same health messages and support discussion and care decisions within the household—a mechanism designed to leverage social influence and reinforce good maternal and newborn health behaviors with consent. Having family members who can share SMS information has been shown to be an important determinant of intention to use mHealth interventions in similar settings. 34
The study identified several key requirements, including the app to support SMS and MMS messaging, to have Afan Oromo and Amharic language options, to have message delivery tracking, health service tracking, advanced encryption, distinct messaging to avoid confusion, and for midwives to be able to report services provided. Compared to other studies, our consultation process yielded results that align with global best practices and local needs, especially in maternal and newborn health interventions through mobile technology. Localization of language increases accessibility and cultural relevance, as seen in the mHealth program in Bangladesh, where messaging in local languages was found to be crucial for adherence to maternal health advice. 35 Moreover, studies in South Africa showed that data privacy is essential to gain the trust of participants, especially in rural settings where concerns about confidentiality can significantly impact participation. 36
Some of the features the app has are adding, deletion, and grouping of contacts to facilitate easy sending of tailor messages to groups based on common attributes such as LMP, EDD, and postnatal schedules. The application is embedded with a search functionality within the application to help the user in finding a particular contact within a very long contact list of pregnant women. It is important to note that several messaging application software exists at the market, which comprises of various features and functions, such as an improved contact management system. 37 This article defines the feature of grouping in messaging applications as that which will enable segmentation of the contact list based on shared attributes. The search Allows searching contacts using keyword or other search criterion.
The application was local developed; this ensured that it is culturally and linguistically tailored to the needs of Ethiopian women. This localized approach enhances the potential for scalability and long-term sustainability, as systems developed within national contexts are more likely to integrate with existing health system workflows and be maintained using local technical capacity. Similarly, global interventions such as the Mobile Midwife program in Ghana have successfully integrated localized, stage-specific content to increase acceptance and relevance among users. 38 Unlike many global systems, however, the present application incorporates a structured feedback loop from health workers, enabling midwives to confirm message receipt and reported service uptake—an important feature for sustaining program effectiveness and accountability at scale.39–41 When compared with large-scale African mHealth initiatives such as MomConnect in South Africa and mMitra in India, several similarities and distinctions emerge. Like MomConnect, the present system relies on SMS-based delivery, enabling broad reach among women with basic mobile phones and limited internet access, and supports multilingual communication, which has been critical to MomConnect's national scale-up. However, unlike MomConnect, which primarily delivers standardized national messages, our application incorporates experimentally framed gain- and loss-based messages and enables optional family level message sharing, allowing more tailored behavioral influence within households. Similarly, mMitra delivers time-specific maternal health messages; however, our system uniquely integrates bidirectional reporting from midwives and localized contact grouping by LMP and EDD, enhancing continuity of care and system responsiveness in decentralized health systems.
From the current study, the utilization of a dedicated domain, Layer 3 VPN, and short code for message dispatch availed from Ethio Telecom, symbolizes sound technology infrastructure—a feature identified to be pivotal for sustaining the mHealth intervention. These infrastructure choices reduce dependency on third-party platforms and enhance system reliability, data ownership, and long-term operational viability. Evidence from South African and Indian mHealth implementations similarly demonstrates that reliable and scalable telecommunications infrastructure is a cornerstone of sustainable digital health programs.42,43 This study emphasize that effective telecommunications infrastructure is essential for facilitating access to services.
The advanced integrated security features of the application include the encryption of messages, decryption, password protection, and a PIN lock feature, concealing messages from the lock screen. Indeed, there have been parallel reports in the past that issues related to encryption and other security features in messaging applications were major factors. In 2016, WhatsApp introduced end-to-end encryption that barred any person, including WhatsApp itself, from reading messages sent over the application. Telegram, meanwhile, have rolled out many security features to protect users’ privacy and security: besides offering secret chats, in which all messages can be end-to-end encrypted and self-destruct after a set amount of time.44–48
The application also demonstrated strong resilience to network instability by maintaining message delivery across variable network conditions, including during temporary interruptions. Such robustness is essential for scale-up in rural and hard-to-reach settings where network availability is unpredictable. Techniques such as network switching, error correction, and adaptive routing—previously explored in other studies.49,50 support reliable communication under challenging conditions, reinforcing the application's suitability for widespread deployment. Finally, the system efficiently manages large message volumes, supporting maternal education before, during, and after pregnancy. This scalability, combined with strong error-handling and rapid recovery mechanisms, supports sustainability by minimizing service disruption and data loss. Consistent with prior research emphasizing the need for resilient digital solutions in resource-constrained settings,51–54 these features help ensure that maternal health information remains accessible, reliable, and continuous even under adverse conditions.
Our intervention was tailored to the real challenges of rural Ethiopia and similar LMIC settings, where limited network coverage, intermittent electricity, low digital and health literacy, and language barriers can impede uptake of conventional smartphone apps. mHealth research highlights these infrastructural, literacy, and language barriers as common impediments in Sub-Saharan Africa and LMICs, underscoring the need for context-specific design. By using SMS rather than internet-dependent smartphone apps and delivering content in locally preferred languages, we improved accessibility for women and families with basic phones.
Limitations of the study
This study has several limitations. First, the pilot involved a relatively small sample size and was conducted over a short period, which limits the generalizability and the ability to observe longer-term usability trends and impacts. Second, the geographic scope was limited, as the intervention was tested in a specific rural setting in Ethiopia, so findings may not be fully representative of other regions with different infrastructural, linguistic, or cultural contexts. Third, the intervention remains dependent on mobile network coverage and access to technology barriers that persist in many low-resource areas and may have affected participation and engagement. Additionally, this manuscript focuses primarily on the technical and operational development of the web-based application and its contextual design features, rather than on direct end-user outcomes; we did not assess clinical or behavioral outcomes such as improvements in antenatal care (ANC) attendance or other maternal health indicators within this article. While the clinical and behavioral effectiveness of the messaging content is the central focus of our companion manuscript, the absence of outcome measures in the current study limits conclusions about the intervention's impact on health service uptake.
Conclusion
The development and testing of the mobile messaging application for maternal and newborn health, was a comprehensive and iterative process that covered 8 months. The application successfully integrated critical user needs such as multilingual support, secure communication, health tracking, and the ability to send 78 crucial messages at key pregnancy stages. High success rates in unit, prototype, and pilot testing confirmed the software's reliability, user-friendliness, and effectiveness in delivering health messages. While minor improvements are recommended, the application's performance indicates it is well-prepared for broader deployment, serving as a model for similar digital health interventions. Looking forward, this application is well positioned for integration into Ethiopia's national digital health framework, such as the Digital Health Blueprint and strategic initiatives under the Ministry of Health's Health Sector Transformation Plan, where interoperable, scalable, and culturally tailored mHealth solutions are prioritized to support universal health coverage and strengthen health information systems in alignment with national goals.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261417862 - Supplemental material for Development and testing of a short message service integrated web-based application for enhancing maternal and newborn health in Jimma Zone, Ethiopia
Supplemental material, sj-docx-1-dhj-10.1177_20552076261417862 for Development and testing of a short message service integrated web-based application for enhancing maternal and newborn health in Jimma Zone, Ethiopia by Gebeyehu Bulcha, Hordofa Gutema, Tamirat Tanga, Asefa Getaneh, Mulusew Gerbaba, Demisew Amenu and Zewdie Birhanu in DIGITAL HEALTH
Footnotes
Acknowledgments
We would like to acknowledge Fuad Sabit and Munira AbaJihad who were involved in the process of software development in one way or other.
Ethical approvals and consent to participate
The study was approved by the Institutional Review Board of Jimma University (Ref. No. JUIH/IRB/316/23). Participation in this study was voluntary. All participants—including pregnant women, healthcare providers, MCH experts, and Ethio-telecom specialists—were informed about the study's objectives, procedures, and their roles in the development and pilot testing phases of the mobile phone messaging application. Each participant was given ample time to ask questions and receive answers before providing written informed consent.
The informed consent procedure, as described to the pregnant women participating in the pilot testing, included explanations of the type and frequency of SMS messages they would receive, the importance of the messages for maternal health service uptake, and their right to withdraw from the study at any time without affecting their access to health services. Health professionals and other stakeholders involved in prototype testing and the pilot provided informed consent, understanding that their feedback would be used to refine the system for broader implementation.
Authors contributions
GB drafted the article and was involved in planning the details of the software development process. HG contributed to the planning of the software development and reviewed the manuscript. TT and AM developed the software by writing the code. MG, DA, and ZB played crucial roles in the software development process; they conceptualized the development, outlining the steps required to create a functional and effective software solution. Finally, all participants reviewed and approved the article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was carried out with the support of small grants for postgraduate students from the Jimma University Innovation and Research Institute Directorate, as well as small grants from the Departments of Health, Behavior and Society and Obstetrics and Gynaecology. The views expressed do not necessarily reflect those of these organizations.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials statement
Software availability statement
The application can be accessed at ![]() for details on its features and future updates. Software detail for ulfamijuu is as follows:
for details on its features and future updates. Software detail for ulfamijuu is as follows:
Project name:
Operating system(s):
Programming language:
Other requirements:
License:
Any restrictions to use by non-academics:
Guarantor
I, Gebeyehu Bulcha, hereby confirm that I accept full responsibility for the integrity of the work presented in the study titled “Development and Testing of a Short Message Service Integrated Web-Based Application for Enhancing Maternal and Newborn Health in Jimma Zone, Ethiopia”. I affirm that:
I have made substantial contributions to the conception and design of the study as well as the analysis and interpretation of the data. I have reviewed and approved the final version of the manuscript (or report). I accept accountability for all aspects of this work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately addressed and resolved.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.