
Abstract
Digital health represents a research field dedicated to realising digital technologies’ potential and developing knowledge about their feasibility and impacts. Yet, drawing on a critical review of the articles in the most prominent multidisciplinary digital health journals, this paper argues that the digital health field has not profoundly engaged with its core subject, namely technology. The features of digital technologies remain in the background, and research is disconnected from the complexities of healthcare settings, including multiple technologies, established practices and people. Instead, the overarching focus in the digital health literature is the processing capabilities of digital technologies and their posited impacts. This paper proposes a research direction in digital health where technology and the context of use take a more prominent role. It argues that realising the potential of digital health requires intensive investigation drawing on different disciplines, grounded on understanding healthcare processes, related informational needs and the concrete features of digital technologies.
Introduction
We can understand digital health as a response to a health landscape becoming more uncertain and complex on a global scale (Benis et al. 1 ). On top of the rising threat of non-communicable diseases like diabetes and hypertension, there is an upsurge of adverse health impacts resulting from pollution, climate change, and migration. 2 Global and national health reform efforts, such as Sustainability Development Goals, Universal Health Coverage, and One Health, engage with these global challenges, including antimicrobial resistance and novel infectious diseases. These reforms come with new informational needs, requiring, amongst others, sharing of information between different stakeholders and enhanced service delivery models based on person-based care.3,4 Digital technologies, such as the internet of things, smartphones, social media, and digital platforms, also lead to the generation of new and diverse forms of data, such as big data and biodata, and opportunities to do new ways of analytics, such as those based on machine learning (see, for example, L’Heureux et al. 5 ) However, while these new digital technologies create new possibilities for their users to address health concerns, they also pose inherent risks arising from the unknown nature of their impacts, such as digital inequities, 6 given the rise in the complexity to which they contribute.
With the proliferation of digital technologies in healthcare, there is an urgent need to understand their impacts. 7 The features of novel digital technologies let users do things they could not before, but they also come with their limitations. When technologies offer new possibilities, the users’ tasks and roles may change, it may introduce shifts in forms of collaboration, and the way work is organised may change.8,9 To overcome the limits of technologies and unwanted organisational changes that may come with them, users may also engage in counter activities such as workarounds.
Digital technologies have three defining characteristics, making them unique and different from other technologies. 10 First, digital technologies are programmable and reprogrammable. Thus, digital technologies are not single-purpose appliances but can perform different functions, and they can be changed and repurposed. Second, the basis of digital technologies is the digital representation of data, allowing for a decoupling of data from devices. Digital data further supports connectivity, allowing the exchange of data and services between different digital components. Third, digital technologies are central to an ongoing virtuous circle of increasing access to digital devices, digital content production, and digital innovation on a global scale. The pervasiveness of digital technologies and their malleable nature facilitate innovation and accelerate further diffusion of digital technologies.
The potential impact of digital technologies is wide-ranging (see, for example, Hund et al. 11 ). First, they allow the interlinkage of devices and components across organisational borders and user groups. Second, the combination of ubiquitous Internet access, miniature sensors, large-scale computing, and powerful end-user devices can generate, process, and make vast amounts of data readily available. 12 Third digital platform architectures allow broad participation in innovation and rapid development of user apps based on a relatively stable underlying infrastructure. 13 Fourth, digital technologies enable new linkages across organisations and between people and thus potentially influence the way we collaborate and interact.
Digital technologies have already made a substantial impact in healthcare. 14 We can observe the increasing use of big data analytics, machine learning algorithms, remote monitoring, and consumer devices in health planning, preventive care and personalised treatment. At the same time, we see changes in the roles of caregivers and patients, where digital technologies are essential drivers. 15 For example, social media platforms allow for informed patients regarding their own health and possible treatments. Individuals can access their health data through apps, data commonly considered as owned by them. There is also an expectation that patients participate in their treatment actively and the patient on their side expects healthcare services to be coordinated and integrated.
The increasing complexities and uncertainties of both digital technologies and health and their interactions make the landscape of digital health a relatively uncharted territory in terms of research. In many ways, digital health is a new research area. Therefore, we need systematic research to understand better the various questions concerning how we can effectively harness the digital technology to enable improved access to healthcare services and provide informational support to engage with emerging health challenges. This paper argues that to help engage with these and related questions, the field of digital health could usefully learn from Information Systems (IS) research. Inspired by the focus on strengthening the value of digital technologies to emerging health challenges in situated contexts, the aim is to answer the following research question: How does existing digital health research conceptualise the nature of digital technologies and understand their relation to the context of use?
This paper analyses publications from the journals engaged with interdisciplinary digital health research to explore gaps in the literature and discuss them in the light of learnings from information systems research. Two critical gaps are identified, where arguably such cross-disciplinary learning can take place: (i) how to be more explicit about digital technologies, not treating them as ‘black boxes’, to understand better how their nature influences health-related processes; and, (ii) how to be more explicit about the context to understand better the challenges in effectively implementing and using digital technologies in real-world and complex settings. The paper further discusses how information systems research has tried to address these concerns over more than three decades of research before turning to an analysis of the current digital health literature, identifying gaps and providing recommendations on how to fill them.
Learnings from information systems research
Opening the ‘black-box’ of digital technologies
Information systems research is concerned with understanding the dynamic and complex relationship between digital technologies and processes of organisational change, viewed as deeply contingent, complex, interwoven and dynamic. While the specificity of digital technologies is now recognised as a critical contributing element in shaping this relationship, technology is often taken for granted and presumed to be unproblematic once it is built and installed, resulting in it disappearing from view. 16 This neglect leads to simple-minded, linear and deterministic accounts of how digital technologies generate (primarily positive) change, which, as research has emphatically demonstrated, is not always the case. An underlying reason for this is the fact that we are not ‘specific about technology’ 17 and do not focus on understanding in more intimate detail how digital technologies can have both restricting and enabling implications. 18
Over time, information systems research has matured and brought in novel theoretical means to conceptualise digital technology and its relation to organisational change processes and complexity. This includes actor-network theory 19 and information infrastructures (see, for example, Hanseth et al. 20 ). More recently, digital platforms and architectures have received much attention (see, for example, De Reuver et al. 21 ). This literature conceptualises platforms as a particular type of digital technology, with features of being reprogrammable, malleable and flexible, contributing to digital representations of data as combinable and re-combinable. 10 These features also enable layered architectures of different components, raising particular challenges of sharing data across these layers. This and related research have emphasised how the specific nature of digital technology shapes, enables and constrains organisational change processes by different mechanisms, which also has implications for the users and institutions involved. For example, Constantinides and Barrett 22 provide an exciting example of how a new digital tool enabled the exchange of health data between GPs and cardiologists, shaping their collaborations and allowing them to develop new and shared means for making diagnoses. In combination with ECG devices, the system rendered symptoms to the cardiologist, thus influencing the way they made diagnoses. However, the GPs considered the system too slow during emergencies because they needed to type on the computer. Such examples lead to the conclusion that digital technologies are anything but neutral, and buried deep in the ‘technical’ details are inscribed anticipations of individual, organisational and inter-organisational behaviour. 17 It thus becomes essential to understand the impact of technical features, how to use is envisioned, and how powerful digital technologies’ role is in healthcare practices. 18 These aspects of technology profoundly influence organisational processes.
Being explicit about the context of use
Context matters, as it actively shapes processes of IT design, implementation and use. 23 Failure to be specific about the context leads to building ‘one size fits all’ kind of solutions, which have historically not worked because they lead to a significant gap between those that design and those that use it. 24 Digital technologies on their own can do little unless they are linked with their context, involving multiple heterogeneous relationships, including users, practices, institutional rules, industry standards, and other technologies. The context in digital health is complex, multifaceted and interconnected, involving the disease, the patient, the health system, the informational flows and artefacts in use, and existing institutional conditions. Understanding how these conditions interact with the technology and their implications on health processes becomes an important object of research.
Information systems research has focused on understanding context and how it mutually interacts with implementations of digital technologies. Four decades ago, Kling and Scacchi 25 introduced the ‘web model’ of computing in contrast to the dominantly used ‘discrete-entity’ model, which represented a decontextualised analysis of computing. The web model saw IT as being more than just the tools deployed on the desktop or the factory floor, but as an ensemble or ‘web’ of equipment, techniques, applications, and people that define a social context, which further contributed to the conceptualisation of IT as social systems. The social context is dynamic and multi-level, representing various cultural, social, technical and cognitive forces. 23 Markus and Robey 26 presented different ways of studying the relationship between digital technologies and organisational change – as an independent variable, a dependent variable, or as an outcome of an emergent process of contextually situated change, often indeterminate and dynamically contingent. By understanding the context, we can further open the ‘black-box’ of technology and learn how and why technologies are designed and used in particular ways. 27 Understanding that no two contexts are exactly similar helps to go beyond making technology-deterministic assertions and encourages us to analyse unexpected, unintended and multiple consequences of technology. Barley 28 demonstrated this phenomenon by analysing similar CT scanner technologies used in two hospitals in Massachusetts, which produced very different outcomes. Barley's analysis depicted how different contextual conditions, particularly the relationship between doctors and radiologists, shaped the impacts of the same technology in very different ways.
Methods
Our research aim was to understand how the publications in journals focusing on digital health and drawing on multiple disciplines have considered the particular features of digital technologies and related to the context of use. Thus, a critical review 29 was conducted to synthesise the digital health literature along the dimensions of the role of technology and context. Furthermore, taking stock of the existing body of research in the emerging field of digital health, the aim was to highlight critical gaps and suggest ways to address these.
The starting point was that digital health is an emerging discipline. While a variety of journals are dedicated to applying information technology in healthcare (such as health informatics), the aim was to take stock of research contributing explicitly to establishing digital health as a discipline. Further, one assumption was that taking the nature of digital technologies and context into account and addressing the complexity of scientific challenges in digital health requires drawing on multiple disciplines. Therefore, the focus was on journals positioning themselves explicitly as digital health journals and with multiple disciplinary scopes, transcending the disciplinary borders of health, computer sciences and others.
The journal databases UlrichsWEB (http://www.ulrichsweb.com) and Pubmed (https://pubmed.ncbi.nlm.nih.gov/) were searched using the string ‘digital health’ and limiting the results to academic/scholarly contents. The search resulted in six unique journals, as shown in Table 1 below (sorted to show similarities and differences in the results from the two databases).
Search results for digital health journals.
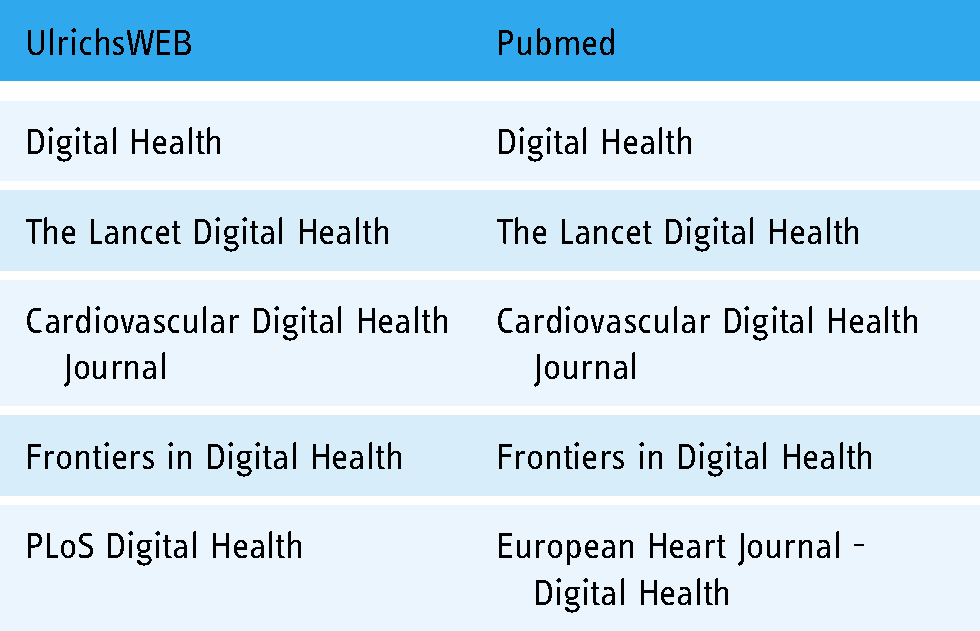
Six journals were screened for relevance related to our purposes. PLOS Digital Health was just launched when conducting the review and thus excluded (only one article was published). Both Cardiovascular Digital Health Journal and European heart journal - Digital health are journals not focused on digital health in general but dedicated to cardiovascular and heart medicine, respectively. From the description of their scope and mission, these two journals are multiple disciplinary only to the degree that they involve different disciplines within medicine. Thus, the screening resulted in three relevant digital health journals with multiple disciplinary scopes (described in Table 2).
Multiple disciplinary scope and mission of the selected journals.

The original research articles published in the three journals Frontiers in Digital Health, Digital Health and Lancet Digital Health were reviewed. The 342 articles published from the inception of the journals and until the time of the review (July 2021) were interpretively analysed to understand how they addressed the features of digital technologies and the context. To aid the review and analysis, the review drew upon the meta-categories developed by Orlikowski and Iacono
30
to categorise research in the way it conceptualises technology, which included:
(i) nominal view, where there is little or no focus on the digital, or is only presented in passing more as a motivation rather than the subject of analysis; (ii) computational view, which focuses only on the technical capabilities of the digital, while ignoring the interactions between the technical and social, within situated contexts; (iii) proxy view, which assumes that critical aspects of the digital can be captured through specific abstract measures, such as user perceptions or investments in technology; (iv) ensemble view, which recognises the features of digital technologies and the complex and dynamic context in which they inherently are enmeshed in their design and use; (v) tool view assumes technology is designed to do something, and it does what it is intended to. The technology is independent of the context and treated as stable and settled ‘black boxes’. (i) disciplinary: author(s) in the same research discipline (ii) multiple disciplines: authors from different research disciplines (iii) interdisciplinary: authors from different research disciplines and explicit on disciplines working jointly in the research (identified by searching for ‘discipline’ and ‘disciplinary’ in the articles) (iv) transdisciplinary: authors from different research disciplines and explicit on transcending boundaries of disciplines including health, technology and the social sciences in the research (identified by searching for ‘discipline’ and ‘disciplinary’ in the articles).
The review categorised 342 papers based on the above framework and we classified them according to the research methods used in five broad groups: randomised control trials, computations on datasets, quantitative, qualitative and mixed methods. Based on the institutional affiliation of the authors and how they describe the role of multiple disciplines in research, we finally categorised the papers into the following four groups:
These results are presented next.
Results
The categorisation of the original research articles (n = 342) is summarised in Table 3.
Classification of the 342 articles according to the conceptualisation of digital technologies.

The tool view accounting for 40% of the articles was the most common conceptualisation. These publications see digital technologies as discrete and stable artefacts while focusing on independent variables influenced by the technology, such as productivity, information processing and social relations. The digital only appears in the background, delivering what it is intended to do independently of social and organisational arrangements. For example, Benhamou et al. 31 reported on a study of patients who received insulin via a hybrid closed-loop system, comprising a patch-pump, a glucose sensor and a hybrid closed-loop regulation algorithm in addition to remote monitoring features of patients. Benhamou et al. 31 showed that the proportion of time that the glucose concentration was within the target range was significantly higher with this solution compared to the control group using more conventional and sensor-assisted insulin pumps. This paper has a tool view by reflecting how the technology enhanced the ability of diabetic patients and their caretakers to regulate glucose concentrations. While the authors discuss the human and ethical implications of the technology, they pay scant attention to the concrete features of the technology. Further, the research did not consider what it takes to put the concrete technology into wider use. Thus, research treats digital technology by large as decontextualised and as a ‘black-box’. Such a conceptualisation restricts our ability to understand the features of the technology that made it work. How the technology can be adapted to multiple contexts with positive implications for improved glucose management and better care of diabetic patients remains an open issue.
The second-largest group, accounting for 18% of the articles, represents the nominal view, which Orlikowski and Iacono argue does not consider technology nor the context. For example, Hyppönen et al. 32 assessed possible associations of high body-mass index (BMI) with multiple disease outcomes in a hypothesis-free, data-driven phenome-wide association study (PheWAS). Based on a population of U.K. Biobank participants, they analysed data from 17 different disease categories and identified diseases possibly influenced by high BMI. The only mention and consideration of technology and context in their paper is the comment that the actual effects of the technology are complex and would vary with life stages.
The third-largest group of articles represented the proxy view, accounting for 18% of the articles. The proxy view has its basis in assuming that we can capture technology characteristics by measures such as users’ perceptions. For example, Stiles-Shields et al. 33 studied the use of smartphones for behavioural interventions for depression. They aimed to identify perceived barriers to mobile app use (the proxy), and they used card sorting tasks performed by potential end-users. The research identified several perceived barriers, including concerns about intervention efficacy, the app's functioning, the privacy of recorded data and costs. While the barriers identified and the design recommendations made may be relevant inputs to app design, they are out of context and not linked to the particularities of any technology. For example, they suggest addressing the most important identified barrier of perceived high costs of use by providing a choice of using cellular data packages or Wi-Fi. This approach is sensible but may have little if any effect on use because use happens in a context where a range of other factors will be at play.
The fourth-largest group, accounting for 14% of the articles, represents the computational view, focusing on the processing capabilities of the technology. For example, Stanitsas et al. 34 envision the augmentation of clinicians’ capabilities to describe malignant regions in breast cancer image data. While mammography is widespread in use, interpreting images based on manually segmenting data to consider whether a lesion is cancerous or not remains time-consuming. Computer-aided diagnostics has the potential to assist medical experts in doing their job more efficiently and supporting them in their most recurrent tasks, resulting in faster diagnostics. In their research, Stanitsas et al. 34 suggest the Covariance-Kernel Descriptor (CKD) and derive the Weakly Annotated Image Descriptor (WAID). They show how CKD outperforms other descriptors and how WAID outperforms other descriptors using the Breast Cancer Histopathological database (BreakHis) in terms of classification accuracy. They conclude by proposing that CKD and WAID can support medical experts to be more accurate and work faster. This represents an argument based on the computational capabilities of technology to support human activity in healthcare. The authors argue that automation of medical diagnosis is more timely, eliminates human errors, and allows medical experts to focus on treatment and patient consultations. However, the basis for the research was running new models on existing datasets and did not involve the use of the computational capabilities in the complex and dynamic context of clinical practices, interconnection with other technologies and the ethical sides of automated decisions.
The smallest group, accounting for 10% of the articles, represented the ensemble view. The research based on the ensemble view addresses the particular features of digital technologies and as embedded in a larger context. As an illustration, Martin et al. 35 evaluated the preventability and effect of health IT failures based on analysing patient safety incidents in England and Wales. They described IT failures as complex, contributed to by the interactional effects of the technology, people and the broader context. Another example is the work of Mount-Campbell et al. 36 on the value of a widely used paper-based artefact, the Kardex, for collaboration among nurses. Comparing the aspects of this ‘historical’ artefact to how existing digital solutions support nursing practices, they draw implications for digital designs.
Looking at the different journals separately, we also observe that the prevalence of the conceptualisations varies (as illustrated in Figure 1). For example, in Digital Health, the proxy view accounts for 29% of the papers. In the Lancet Digital Health, the tool view accounts for 70% of the papers, none of the papers is based on the proxy view, and only 1% represents the ensemble view.

Classification according to conceptualisation of the digital across the different journals.
The methods used in the papers were also captured. There was a wide variety of methods used, and we categorised them into five broad groups: randomised control trials, computations on datasets, quantitative, qualitative and mixed-methods as shown in Table 4.
Classification of the 342 articles according to methods used.

The largest group accounting for 39% of the articles was based on the collection of quantitative data from databases and surveys. The second-largest group, accounting for 30% of the papers, developed new methods, algorithms and scientific knowledge based on data from existing clinical registries, databases, datasets, and population-based studies. The third-largest group accounting for 14%, was based on qualitative methods, including interviews and focus groups. The fourth largest group was a mix of the methods in the other groups accounting for 9% of the articles. Finally, the smallest group representing 8% of the articles was randomised control trials. Thus, the basis of 77% of the papers originate from outside the context of use, and through trials, computations, reviews and surveys.
Looking at the different journals separately, we also observe that the prevalence of the research methods varies (see Figure 2). For example, qualitative methods account for 25% of articles in Digital Health, while computations on datasets accounts for 69% of the articles in the Lancet Digital Health.
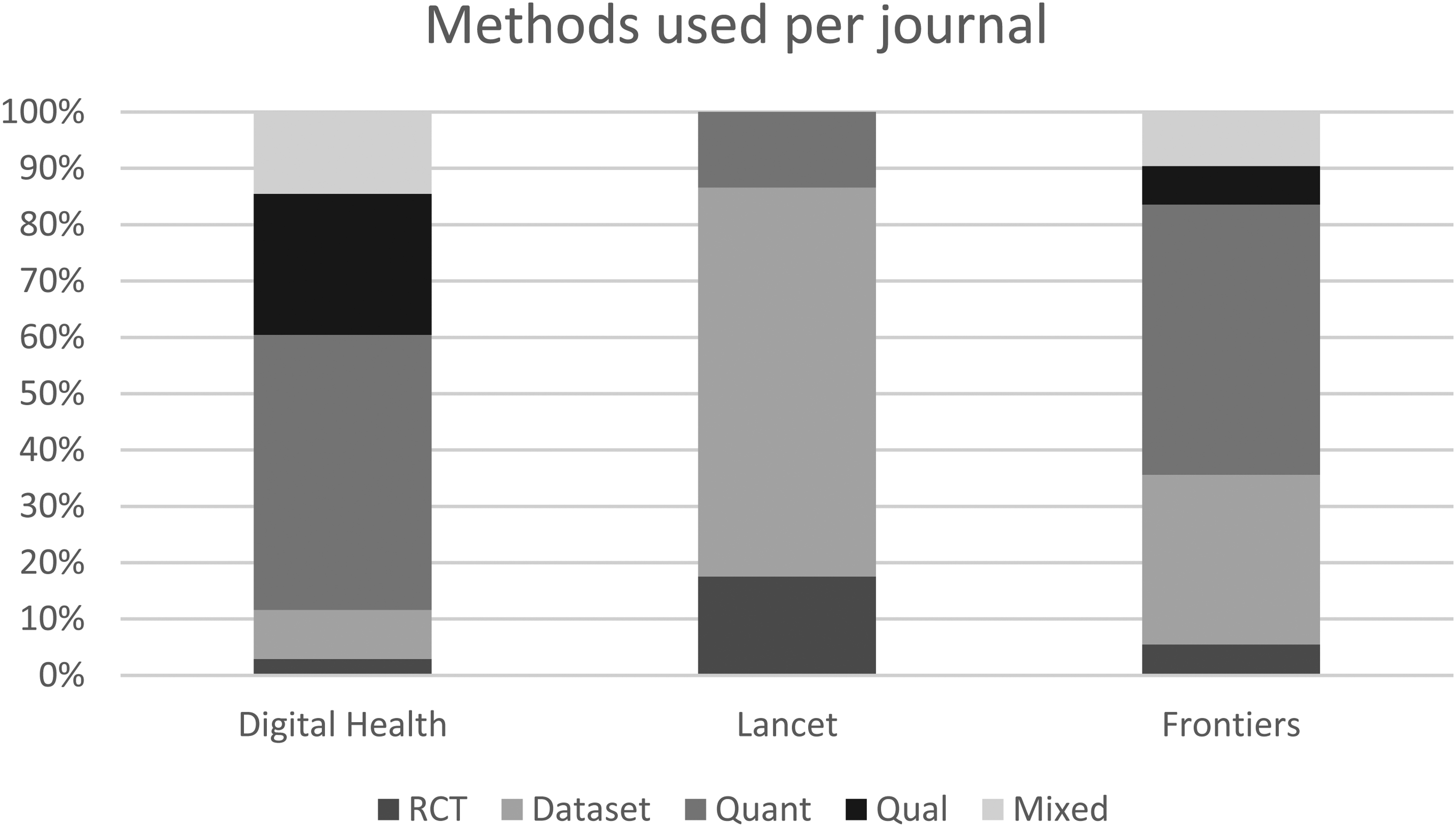
Methods used across different journals.
We finally looked at how the articles relate to multiple research disciplines. We categorised the articles according to the institutional affiliation of their authors and how the articles addressed the links and boundaries between research disciplines, as shown in Table 5.
Classification of the 342 articles and how they relate to research disciplines.

Seventeen percent of the articles had authors from only one discipline, which was due to a single author in most cases. The largest group of papers, accounting for 80%, involved authors from different disciplines, such as pharmacy, nursing, various medical professions, public health, biomedical informatics, biostatistics, health informatics, orthopaedics, justice, phycology, social sciences, etc. However, only 3% of the articles explicitly described research to be interdisciplinary and as joint endeavours of different disciplines. Only one article, 37 less than 1% of the papers, showed an explicit and profound focus on researchers transcending disciplines by working together, combining different bodies of knowledge across disciplines, and working towards a common purpose.
Discussion
Digital technology comes with the promise of improving healthcare services. Today’s changing, uncertain and complex health landscape is increasingly dependent on ubiquitous and interconnected digital technologies spanning practices, institutions, as well as national and international borders. However, our scientific knowledge on how to succeed in this emerging territory is by large arguably unchartered.
The first 342 original research articles published in the three interdisciplinary digital health journals Lancet Digital Health, Digital Health and Frontiers in Digital Health show little discussion on digital technologies’ features. Further, there is a general lack of focus on the context of use, raising questions about the relevance of the results for real-life settings. 90% of the articles take a proxy, tool, computational or nominal view on digital technologies emphasising their computational capabilities in controlled environments. The basis of 77% of the papers was largely decontextualised data, originating in databases, surveys, controlled and idealised population datasets or reviews of research publications (see Table 4). This represents a significant gap in research related to fundamental questions of how digital technologies can advance healthcare delivery in the real world. To help address this gap, this paper provides three recommendations that digital health can implement.
Advancing transdisciplinary research
From the critical review, we observe that the perspective on technology features and context and the research methods used vary significantly among the digital health journals. From this, the argument is that digital health is not one field of research or discipline but represents a broad interest in digital technologies within disciplines. Research drawing on multiple disciplines can be categorised into multidisciplinary, interdisciplinary and transdisciplinary research. 38 The articles in the digital health journals reviewed stay largely multidisciplinary by bringing together different disciplines. However, the representatives of the different disciplines still work on tasks within their usual expertise areas. There is very limited research of interdisciplinary nature explicitly building links between disciplines and even less transdisciplinary research integrating technology, health and social sciences by purposefully transcending their boundaries. We need editorial policies to encourage more transdisciplinary research, as most papers are authored by medical or data science experts who favour randomised control trials or retrospective data analysis as the research method. While these studies are indeed relevant for establishing scientific feasibility in controlled settings, they do not shed much light on how these interventions can be effectively translated to real-world settings. Scientific knowledge developed in a controlled setting will be made relevant in discovering why things work when combined with other methods.39,40 This requires bringing in other disciplines, including social sciences, psychology, economy, computer science and information systems. There are several areas where transdisciplinary approaches can bear fruit. For example, information systems research could explain how digital interventions can sustain and scale in real-world settings. Anthropology can help develop an intimate understanding of the relationship between healthcare workers and technology to explain whether, for whom and in which contexts particular technology is likely to be relevant.
Treating the digital as different from other technologies
One particular trait of the digital is that it is more flexible, malleable, and rapidly circulating across multiple time-space contexts than medical equipment and technologies. These digital features allow for a high degree of interpretive flexibility, implying that digital technologies are understood differently and thus produce different outcomes in varying settings. 16 Furthermore, digital technologies are typically not designed, developed, and commissioned as a one-time exercise but involve recurrent and ongoing design, redesign and update cycles in a different time, space, and use context. This requires us to focus on understanding the dynamic and evolving relationship between the digital and its use. New architectures such as platforms and apps are also on the increase, with implications on technology delivery models and forms of IT governance. There is thus the need to broaden the scope of publications beyond just testing digital technologies as any other technology and as an independent variable in a controlled environment. We should also include longitudinal research that focuses on the evolution of the technology together with processes of design, redesign, implementation, governance and use.
Paying attention to context to anticipate unintended consequences of the digital
Digital technologies can improve quality and support equity in health. However, quality from digital technologies will not come without integration with and rationalising existing systems and processes. Digital technologies can also reinforce existing inequities by adding yet another layer of digital inequity. Access, ownership, evolution and use of digital technologies are shaped by particular social, political and economic relationships, raising the possibility of digital inequities playing out in various ways in different contexts. The digital health research analysed here focused primarily on testing the feasibility of technologies in controlled settings. This research does not leave open the space to understand how the digital can have multiple consequences, including adverse ones, deviating from what was envisaged by the designers. Building such understanding requires research that focuses on examining the consequences of the digital in different contexts and from different perspectives (healthcare workers, patients, health managers, etc.). Developing our understanding of digital technologies in context can only be based on contextualised data. While the methods used in 25% of the articles in Digital Health are qualitative and well equipped to capture the context, none of the papers in Lancet uses qualitative methods. The bases of all the papers in Lancet are decontextualised data. Our recommendation is thus to encourage research to go beyond trials, computations, reviews and surveys and bring in the context with appropriate methods.
In conclusion, this paper tries to answer the question of how does existing digital health research conceptualise features of digital technology and their context of use? This question was approached by reviewing the original research papers published in multiple disciplinary digital health journals. Lancet Digital Health, Digital Health and Frontiers in Digital Health were found as exemplary, and venues where we should expect to find the state of the art research on digital health. However, based on the findings and discussion, the answer is that the papers published on digital health do not pay the required attention to the features of digital technologies, and the research is by large disconnected from the contexts of use. Motivated by learning from three decades of information systems research which has sought to address similar gaps in other domains, the hope is that the recommendations provided here can support digital health research to further the scientific and societal impacts of research to address the emerging field of digital health.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076221109554 - Supplemental material for A critical review of the role of technology and context in digital health research
Supplemental material, sj-docx-1-dhj-10.1177_20552076221109554 for A critical review of the role of technology and context in digital health research by Petter Nielsen and Sundeep Sahay in Digital Health
Supplemental Material
sj-docx-2-dhj-10.1177_20552076221109554 - Supplemental material for A critical review of the role of technology and context in digital health research
Supplemental material, sj-docx-2-dhj-10.1177_20552076221109554 for A critical review of the role of technology and context in digital health research by Petter Nielsen and Sundeep Sahay in Digital Health
Supplemental Material
sj-docx-3-dhj-10.1177_20552076221109554 - Supplemental material for A critical review of the role of technology and context in digital health research
Supplemental material, sj-docx-3-dhj-10.1177_20552076221109554 for A critical review of the role of technology and context in digital health research by Petter Nielsen and Sundeep Sahay in Digital Health
Footnotes
Contributorship
PN conceived the study and reviewed the literature. PN and SS developed the manuscript and approved its final version.
Acknowledgements
None
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
PN.
Informed consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial registration
Not applicable, because this article does not contain any clinical trials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.