
Abstract
A ubiquitous healthcare (UH) system of multiple 3D printing facilities is established in this study for making dentures. The UH system receives orders from dental clinics, and then distributes the dentures to be printed among 3D printing facilities to save time. Compared with existing systems for similar purposes, the UH system has two novel features. The first is the consideration of the possibility of reprinting in formulating the plan to avoid replanning. The other is the cooperation with home delivery services that have gradually become popular during the COVID-19 pandemic to save transportation time. The new features are subject to considerable uncertainties. To account for the uncertainties, both printing time and transportation time are modelled using interval type-II trapezoidal fuzzy numbers. Subsequently, an interval type-II fuzzy mixed integer-linear programming (FMILP) model is formulated and optimized to plan the operations of the UH system. A case study has been conducted to illustrate the applicability of the proposed methodology. According to experimental results, the proposed methodology was able to shorten the order fulfillment time by up to 9%.
Introduction
Ubiquitous healthcare (UH) (or smart healthcare) is the application of smart technologies to assist medical and health care.
1
Smart technologies are based on miniaturized (or unobtrusive) smart devices that can transmit the collected data over wireless networks, thus supporting remote or mobile users.
2
Common smart technologies that support UH include wearable devices,
3
body area networks,
4
smart phones,
5
three-dimensional (3D) printing,
6
cloud computing,
7
telemedicine,
8
mobile web services or apps,
9
etc. This study aims to discuss the application of 3D printing technologies in dentistry
10
because of the following reasons:
Compared with other smart technologies that support UH, the economic benefits of 3D printing applications to dentistry, such as the reduction of denture production costs and production time, are clear and significant.6,11 Compared with other smart technologies, the applications of 3D printing to dentistry are quite diverse, including making drill guides for dental implants, building physical models for prosthodontics, orthodontics and surgery, making dental, craniomaxillofacial and orthopedic implants, and fabricating copings and frameworks for implant and dental restorations.
10
A UH system of multiple 3D printing facilities is established in this study. These 3D printing facilities print denture parts collaboratively to deliver to users (i.e. clinics) as soon as possible.
Some relevant references are mentioned below. Chen and Lin
12
provided a literature review of the feasibility of collaborating multiple 3D printing facilities on order fulfillment, and discussed how to optimize the overall performance. In Chen and Wang,
13
customers on the move placed their orders through smartphones. These orders were distributed among multiple 3D printing facilities. A mixed integer-quadratic programming (MIQP) problem was solved to balance the loads on 3D printing facilities and plan the shortest delivery path through all the 3D printing facilities. A branch-and-bound algorithm was also designed to help solve the MIQP problem. Following their study, Wang et al.
6
derived the slack for each 3D printing facility, so that a 3D object could be reprinted if the printing process was terminated before the slack. In existing models, the transportation vehicle departs for a 3D printing facility while the printing process is still in progress to avoid waiting. As a result, orders are usually distributed to distant 3D printing facilities, resulting in unbalanced loads on 3D printing facilities. To address this issue, Chen and Lin
14
evaluated the suitability of a 3D printing facility in terms of the closeness to just-in-time (JIT). Chen (2019) defined the printing time with a fuzzy number to account for its uncertainty. Then, a fuzzy mixed integer linear programming (FMILP) model
15
and a fuzzy MIQP (FMIQP) model were optimized respectively to balance the loads on 3D printing facilities and plan the shortest delivery path. Most existing systems of 3D printing facilities are managed centrally. Vatankhah Barenji et al.
16
applied the blockchain technology to transform such systems, allowing 3D printing facilities to communicate with each other and manage the system by themselves. Existing methods have the following shortcomings:
If a printing process is terminated after the slack, it cannot be resumed and the system needs to be re-planned. The surge in demand for transportation services owing to the COVID-19 pandemic has magnified the uncertainty of transportation time. The popularity of home delivery services during the COVID-19 pandemic has eliminated the need to plan a route through all 3D printing facilities. The possibility of reprinting dental parts is considered when optimizing the UH system to avoid re-planning. The expected transportation time and the estimated printing time are represented as interval type-II trapezoidal fuzzy numbers (TrFNs).
17
Unlike may past studies that have subjectively designated the lower membership function (LMF) and upper membership function (UMF) of a type-II TrFN. This study clearly explains the rationale for specifying type-II TrFNs. Subsequently, an interval type-II FMILP model is optimized to balance the loads on 3D printing facilities. In addition, the shortest path problem no longer needs to be solved. Both printing time and transportation time are taken into account in the same model.
To overcome these shortcomings, the following treatments are taken in this study:
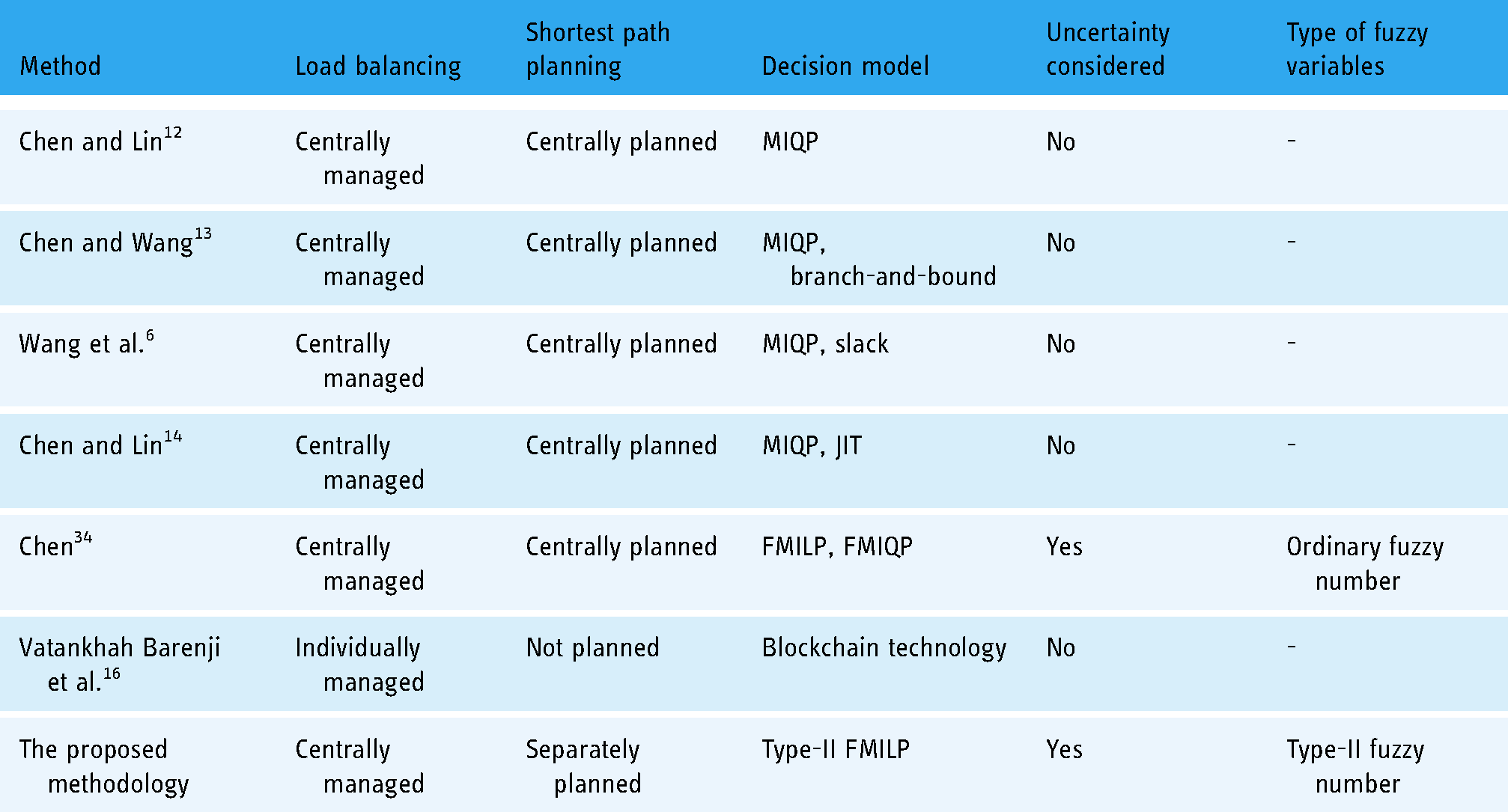
The differences between the proposed methodology and some existing methods are compared in Table 1.
Differences between the proposed methodology and some existing methods.
The remainder of this paper is organized as follows. Literature Review is dedicated to a literature review. Methodology introduces the UH system of 3D printing facilities for making denture parts developed in this study. Case Study details the application of the UH system to a regional experiment in Nantun District, Taichung City, Taiwan amid the COVID-19 pandemic. Conclusions provides the conclusions of this study as well as some possible topics for future investigation.
Literature review
Uh
Body area networks are an important UH (or smart) technology that places tiny wireless sensors on various parts of a human body to monitor vital signs. 4 The monitored signals can be processed by a mobile web service and then transmitted to distant caregivers or hospitals. 9 However, the size, precision, operating time, and reliability of sensors are difficult to balance. 4
Another prevalent UH technology is wearable devices including smart bracelets, smart clothes, smart glasses, etc. Lee and Chung 3 designed a smart shirt that can measure electrocardiogram (ECG) and acceleration signals using wireless sensors. Once the user falls or his/her heartbeat is abnormal, an emergency distress signal can be automatically sent out.
Smartphones are undoubtedly the most commonly used smart device to aid UH. There have been many studies summarizing and comparing smartphone applications to UH, such as Milošević et al. 5 and Weisel et al. 18 Milošević et al. 5 also claimed that smartphone applications allow users to take more active care of their physical conditions.
Most past studies have used wireless sensors to monitor the physical conditions of users. In contrast, Mohr et al. 19 translated sensor-collected data into behavior and state markers related to the user's mental health. For example, a user's movement can be used to deduce his/her activity type and movement intensity that reflect the user's fatigue level.
Wireless sensors collect a user's vital signs at short intervals, generating a huge amount of data. The large number of users of a UH system further amplifies the amount of data. As a result, most of the UH systems face the problem of big data analysis. To solve this problem, some algorithms have been proposed or applied. For example, Shin et al. 20 proposed an integer signal processing algorithm for digitally filtering electrocardiogram (ECG) and photoplethysmogram signals. Hsiao et al. 21 applied several machine learning methods, including multiple layer perceptron (MLP), random forest (RF), support vector machine (SVM), and naive Bayes (NB), to process ECG signals to recognize hybrid arrhythmia patterns.
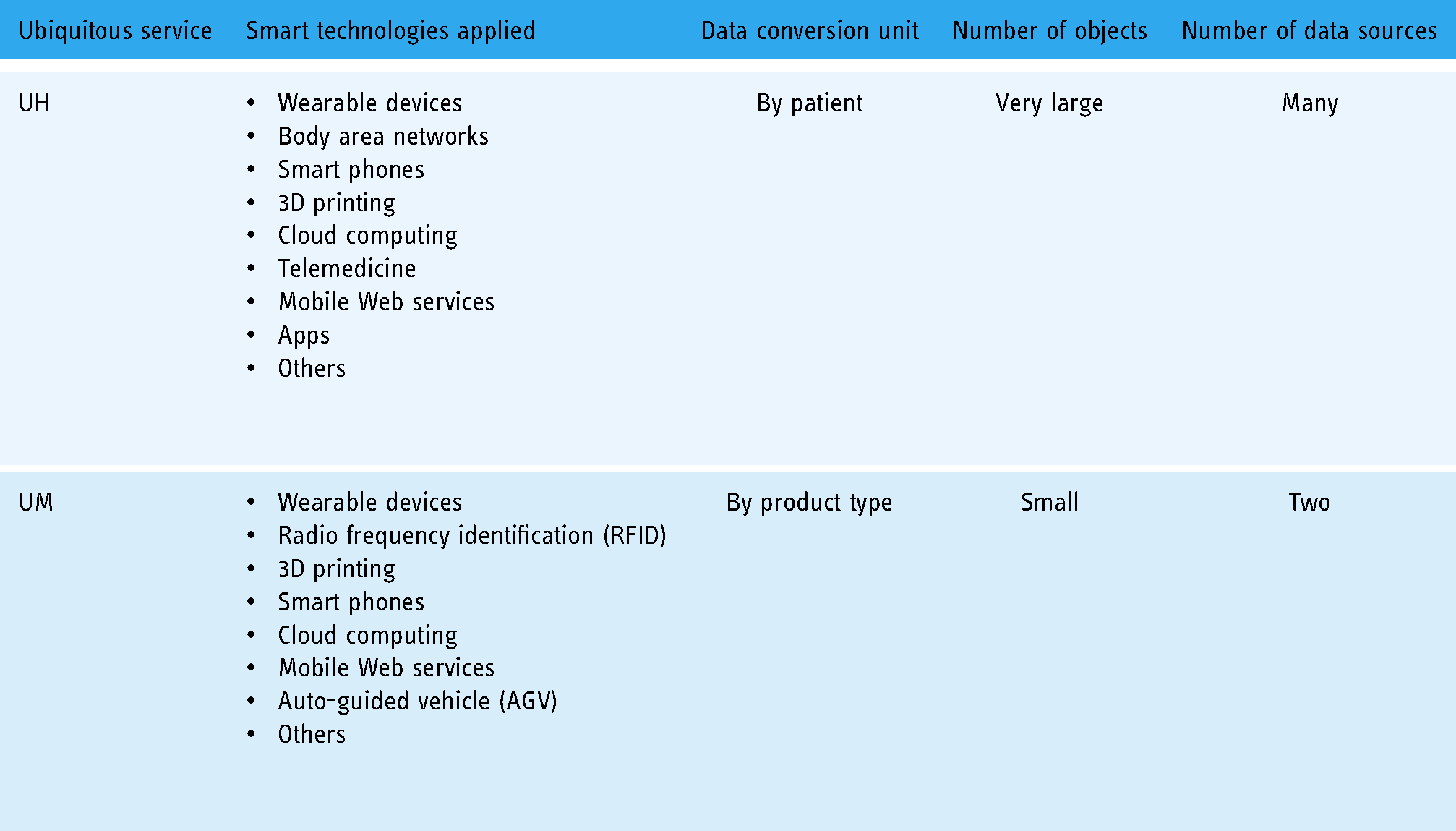
Inconsistencies in medical standards make it difficult to integrate data from various UH systems, which calls for the conversion of data formats. A similar problem can also be observed in ubiquitous manufacturing (UM), 22 in which recipes are converted between two manufacturing execution systems. 23 However, the former is more complicated than the latter, as compared in Table 2. To addressed this difficulty, Satti et al. 24 established a UH profile system, in which the data from various UH systems were reorganized and stored under a relatively flat/denormalized data structure.
Comparing UH and UM.
3D printing applications to dentistry
3D printing has been applied to dentistry since the late 1990s. 10 Many earlier studies had fairly high expectations for the widespread application of 3D printing to dentistry, while some scholars thought it is hype. After years of development, practical applications appear to be much slower.
Dawood et al. 10 introduced the application of 3D printing to dentistry in detail, including commonly used 3D printing technologies and commonly printed dental parts. They concluded that the application of 3D printing in dentistry also promotes the further development of 3D printing technologies.
Whether 3D printed dental parts are suitable for use and whether their quality is not inferior to those manufactured using traditional methods have always been concerned by dental practitioners and patients. Therefore, some studies have conducted comparative, long-term experiments to explore this issue. For example, Jeong et al. 25 compared the precision of tooth models constructed by 3D printing with those constructed by traditional milling methods. Experimental results showed that 3D printing was three times more precise than milling methods in building tooth models.
Tunchel et al. 26 followed up on 110 patients with 3D-printed titanium dental implants. The results showed that after 3 years, the 3D-printed titanium dental implants of 94% of the patients were still intact.
Pillai et al. 11 reviewed the evolution and current trends in 3D printing applications to dentistry, and highlighted the advantages of 3D printing over traditional methods in the manufacture of dental parts as full automation, personalization, improved accuracy, and lower costs. 10
Wang et al. 6 established a collaborative UH system composed of multiple 3D printing facilities for making dental parts. The system distributed the required dental parts of an order among 3D printing facilities to minimize the makespan (i.e. the time it takes to print all the dental parts), for which a MIQP model was formulated and optimized. They also derived a slack for each 3D printing facility, based on which the 3D printing facility could decide whether to resume a printing process that was early terminated.
Researchers continue to experiment with different materials, such as polyether-ether-ketone (PEEK), carbon fiber reinforced PEEK, and antibacterial stereolithography resins (SLR) (with Ag-carrying halloysite nanotubes), to print dental parts and test the strength, antibacterial ability, and biocompatibility (or cytocompatibility) of the printed dental parts.27,28
According to MarketsandMarkets, 29 the global market for 3D printed dental parts will reach $7.9 billion by 2027. Compared with the current market size, which is $3.2 billion in 2022, the compound annual growth rate (CAGR) is up to 20.2%, showing an obvious trend in the dental industry. The main materials used to print dental parts are plastics and metals, while the main 3D printing technologies applied include vat photopolymerization, fused deposition modeling (FDM), selective laser sintering (SLS), and polyjet.
Methodology
Problem statement
This study aims to address the following problem. A dental clinic wants to use 3D printing to make dental parts for patients. Therefore, the 3D-scanned tooth models will be transmitted to 3D printing facilities. However, it will take a long time if all the dental parts are made by a single 3D printing facility. A better approach is to print the desired dental parts simultaneously by multiple 3D printing facilities. The problem is how to determine the number of dental parts made by each 3D printing facility, so as to minimize the makespan, as illustrated in Figure 1.
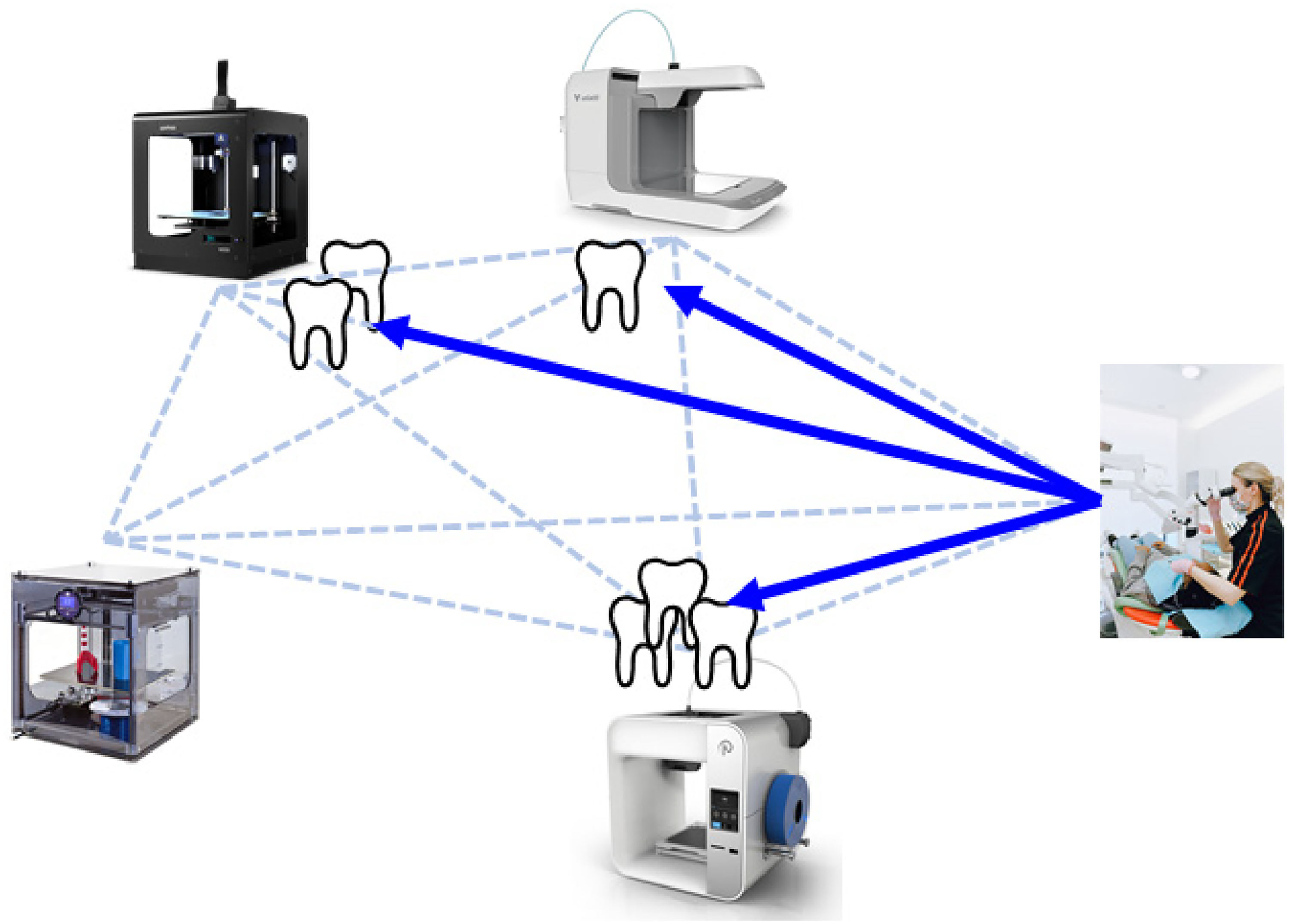
Uh system of 3D printing facilities for making dental parts.
In making this decision, the following concerns are critical:
More dental parts should be allocated to earlier available and faster 3D printing facilities. Distant 3D printing facilities should be avoided to reduce the transportation time to the clinic. In past studies, a freight vehicle visits all 3D printing facilities to collect printed dental parts.
12
The ubiquity and affordability of home deliver services emerged during the COVID-19 pandemic
30
has changed that. It is now more convenient and economical for every 3D printing facility to transport printed dental parts to the clinic directly using a home delivery service, as illustrated in Figure 2.

Comparison of transportation plans made in different studies. (a) Past studies (b) This study.
However, printing time and transportation time are subject to considerable uncertainty, as discussed in the next section.
Type-II fuzzy logic for modelling transportation time and printing time
First, the definition of an interval type-II fuzzy set is given.
Definition 1. 31
An interval type-II fuzzy set

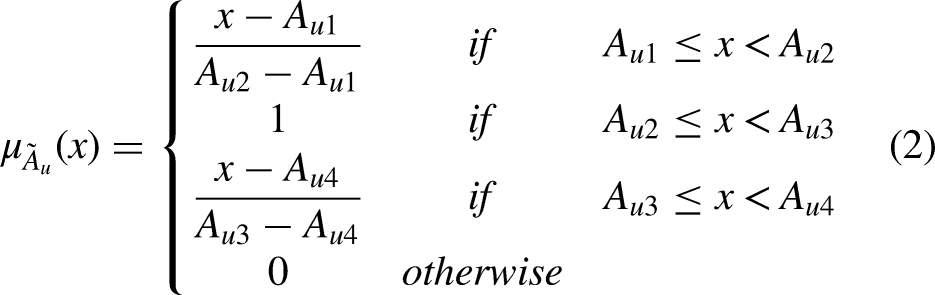

An interval type-II trFN.

Theorem 1. (Arithmetic Operations on interval type-II ITFNs)
Fuzzy addition: Fuzzy subtraction: Fuzzy product (or multiplication): Fuzzy division:
Continuous changes in road conditions and uneven transportation speed lead to uncertainty in transportation time. To account for this, representing the estimated transportation time as a (ordinary) fuzzy number is a common treatment.
33
During the COVID-19 pandemic, the surge in transportation demand has increased the unavailability of transportation services. As a result, the required delivery service may not start immediately after a request is made, which is modelled by representing the estimated transportation time as an interval type-II TrFN, as illustrated in Figure 4, in which the interval type-II fuzzy transportation time from location (i.e. 3D printing facility or clinic) i to location j, denoted by 






An interval type-II fuzzy transportation time.
Equation (9) quantifies the delay caused by the unavailability of transportation services. For example, in Figure 4, the membership of 15 min is [0.47, 1], meaning that it is not very likely (with a membership of 0.47) to take 15 min to transport the printed dental part before the COVID-19 pandemic. However, during the COVID-19 pandemic, considering the possible unavailability of transportation services, the possibility of taking up to 15 min to transport the printed dental part may become very high (with a membership of 1). Therefore, the possibility can be appropriately represented by the range between these two memberships.
Both the setting of a 3D printer and the finishing of a printed 3D object require manual work, which results in the uncertainty of printing time. Therefore, past studies adopted a (ordinary) fuzzy number to represent the printing time of a 3D object.
34
In the proposed methodology, the UM system is planned on the premise that the printing process at each 3D printing facility may resume once after failing. As a result, the printing time of a 3D object may be doubled, which is modelled as a type-II TrFN, as illustrated in Figure 5, in which the interval type-II fuzzy printing time at 3D printing facility i is 
In Figure 5, without reprinting, the membership that the printing time is 95 min is only 0.35. However, if the dental part has to be reprinted once, the membership that the printing time is up to 95 min increases to 1. In this way, the possible reprinting can be incorporated into the optimization model to avoid re-planning.
Interval type-II FMILP model
In the literature, various interval type-II fuzzy mathematical programming models have been formulated and optimized. For example, Srinivasan and Geetharamani
35
solved a fuzzy linear programming (FLP) problem with interval type-II fuzzy coefficients and right-hand sides. They split the problem into two subproblems. Each subproblem was solved under the premise that the degree of credibility (satisfaction level or possibility degree) of the constraints was higher than a threshold. Finally, the optimal objective function values of the two subproblems determined the lower and upper bounds of the optimal objective function value of the original problem. Kundu et al.
36
considered a FLP problem with interval type-II right-hand sides. They also split the problem into two subproblems solved separately. Furthermore, an additional FLP model was optimized to combine the optimal solutions to the two subproblems into the optimal solution to the original problem. The interval type-II FMILP model proposed in this study is optimized in a similar manner. However, the defuzzification approach is applied instead of the credibility approach in converting constraints.
An interval type-II fuzzy printing time.
The interval type-II FMILP model for planning the UH system of 3D printing facilities is formulated as follows. Assuming 


In Equation (11), 

First, considering the LMFs of all interval type-II TrFNs, a goal is established for the objective function as 


A goal for

















Case study
Background
To validate the effectiveness of the proposed methodology, an experiment has been conducted in Taichung City, Taiwan. The experimental region is shown in Figure 7, which had an area of 56 km2. There were fifteen 3D printing facilities in the experimental region, as shown by red pins in this figure. Not all of them had 3D printers suitable for making dentals or were willing to participate. Therefore, the willingness of each 3D printing facility was confirmed case by case. In the experiment, a 3D printing facility should respond to a printing request in 30 min.

Experimental region.
A clinic wanted to make the dentures of six patients using 3D printing, with the aid of three 3D printing facilities, as shown in Figure 8. After a patient had a tooth extracted, a vertebral beam CT was done to obtain 3D root data. The data were transmitted to a 3D printing facility, in which a 3D printer was used to print the denture using titanium alloy or Zirconia. It took half a day to a day to print a titanium alloy tooth, or 3 to 4 h to print a Zirconia tooth. In contrast, with the traditional dental implantation technology now used, a patient had to wait for three months after tooth extraction. These dentures were similar in size and could be printed in the same amount of time. However, the printing times at different 3D printing facilities were not the same.

Case of a clinic.
Application of the proposed methodology
The available time of each 3D printing facility, the printing time of a denture at the 3D printing facility, and the transportation time from the 3D printing facility to the clinic have been estimated and are summarized in Table 3.
Data of the illustrative case.

The MILP Model I was formulated and optimized using Lingo 16.0 × 64 on a PC with an i7-7700 CPU 272 3.6 GHz and 16 GB RAM. The goal was established as 






Optimal objective function value of the interval type-II FMILP model.
According to the plan,
The order could be most possibly delivered to the clinic at 568–606 min. However, the order could be fulfilled in as little as 445 min. Even if the printing process at each facility failed once or the transportation from each 3D printing facility was delayed, the order could still be delivered at 1236 min. The number of dentures to be printed by all 3D printing facilities ranged from 4 to 7. Therefore, the administrator of the UH system should continuously monitor the progresses at all 3D printing facilities and stop making additional dentures when 6 dentures have already been printed.
The execution results are summarized in Table 4. Despite a printing failure, the order was completed and delivered to the dental clinic at 665 min. It was noteworthy that the early terminated printing process was resumed at the same 3D printing facility without replanning, because such events had already been considered in making the printing plan. In contrast, using existing methods, the administrator had to re-plan and assign the denture to another 3D printing facility, which required further negotiation with 3D printing facilities.
Execution results.

Comparison with existing methods
The planning results using two existing methods were simulated for comparison. The first existing method was the MIQP method proposed by Chen and Lin,
12
in which printing time and transportation times were set to their defuzzified values using COG:

The second existing method compared in the experiment was the FMILP and FMIQP method proposed by Chen,
34
in which both printing time and transportation time were modelled using ordinary fuzzy numbers:

Obviously, the proposed methodology outperformed the two existing methods in shortening the order fulfillment time by 6–9% due to the following reasons:
Re-planning was not required when a printing process was early terminated. Printed dentures were transported to the clinic from the 3D printing facilities separately and simultaneously.
The proposed methodology takes into account the possibility that a dental part may be printed twice. A dental part can be printed more times, but that is rare. In this case, the UMF of the printing time can be further expanded to three to four times that of printing once, while the LMF remains the same.
Managerial implications
In Taiwan, although the National Health Insurance covers some dental treatments, it does not cover dentures. Therefore, the cost of a denture is extremely expensive, and the profit for the dental clinic is also high. Therefore, there is no incentive for a dental clinic to switch to offering cheaper 3D printed dentures, unless the majority of dental clinics already do so. By then, the low cost of 3D-printed dentures can be expected to lead to a surge in demand for dentures. People who were reluctant to buy dentures will no longer hesitate. The methodology proposed in this study will be able to efficiently meet this large demand.
In this experiment, as expected, the dental part printed by one of the 3D printing facilities failed and had to be reprinted. The lack of stability of the 3D printing process remains a concern for the development of related services.
On the other hand, the home delivery service that emerged during the COVID-19 pandemic can be expected to remain popular after the pandemic is over. Therefore, more and more ubiquitous healthcare services, like the one designed in this study, are expected to appear.
Conclusions
3D printing is a smart technology that has been widely applied to medical and health care. The applications of 3D printing in dentistry are even more diverse. This study establishes a UH system based on multiple 3D printing facilities, which allocates the dental parts to be printed to multiple 3D printing facilities for simultaneous printing to shorten the overall completion time. Compared with similar studies in the past, the methodology proposed in this study considers the possibility of reprinting in advance when formulating the plan and cooperates with home delivery services that have gradually become popular and economical during the COVID-19 pandemic to save transportation time.
The proposed methodology has been applied to a regional study to validate its effectiveness. Compared with two existing methods, the proposed methodology shortened the order fulfillment time by 6–9%. In addition, the proposed methodology has the following advantages over existing methods:
Using the proposed methodology, there is no need to re-optimize the production plan when a 3D printing process is terminated early. The operations at different 3D printing facilities can be separated using the proposed methodology. In the proposed methodology, 3D printing facilities deliver the printed dental parts to the clinic in parallel, thereby speeding up the delivery. A 3D printing facility reprints an early terminated dental part without communicating with the system administrator or other 3D printing facilities. As a result, there may be too many dental parts printed by the end. Estimating the possible delay in the shipping service may not be easy.
However, the proposed methodology also has disadvantages:
It is not impossible that a printing process fails more than once, which can be addressed in a future study by modifying the proposed methodology. In addition, the quality levels of dentures printed by different 3D printing facilities may not be equal, which needs to be considered in improving the practicability of the proposed methodology. These constitute some topics for future research.