
Abstract
Background
Digital testing services for sexually transmitted and blood-borne infections (STBBI) are becoming more common in Canada. There is little evidence supporting the assumption that these services reduce healthcare system burden. To explore this further, we described patterns of provider-based testing among repeat users of a digital STBBI testing service, and their association with access barriers.
Methods
We conducted a cross-sectional survey in November 2022 of repeat GetCheckedOnline.com users (≥2 tests, with 1 test between April and October 2022). We stratified participants into three use patterns of GetCheckedOnline for testing, using ordinal logistic regression to examine associations with barriers reflecting availability, accessibility, acceptability and appropriateness of health services (applying weights to adjust for non-responders).
Results
Of 798 participants (17.2% of 4633 eligible), 52.6% only and 35.8% mostly tested through GetCheckedOnline; 14.5% tested more often/equally through healthcare providers. Availability was associated with greater use of GetCheckedOnline (e.g., not having a primary care provider, OR 2.03, 95% CI [1.52–2.73]), and appropriateness with lower use (getting tested part of clinical care, OR 0.07 95% CI [0.05–0.11]). Participants < 25 years, high school educated or less or born outside Canada reported greater use of GetCheckedOnline for testing while 2S/LGBTQ+ and full-time employed participants reported lower use. Most participants (88.0%) would have tested through a provider if GetCheckedOnline were not available.
Conclusion
GetCheckedOnline use was associated with barriers to the availability of provider-based testing. Digital STBBI testing services may improve access to testing and reduce demands on healthcare providers for testing.
Introduction
The current Canadian primary healthcare access crisis affects both patients and healthcare providers and urgently requires solutions. In 2022, 44% of Canadians reported it difficult or impossible to access non-emergency care. 1 Workforce shortages and rising service demands are leading to increasing workload, overtime and burn-out among Canadian healthcare providers. 2 Digitally enabled health services are considered solutions for improving healthcare access in Canada and are valued by patients and providers alike.3,4 Such services may facilitate patient access to healthcare providers directly (e.g., virtual visits) and support greater patient engagement in their own healthcare (e.g., patient access to health records). However, high-quality evidence of the health system impacts of digitally enabled health services is generally lacking, including examining whether services reduce demand on healthcare providers as well as inequities in service access.5,6
Testing for sexually transmitted and blood-borne infections (STBBI) is a case in point, given rising rates of infections, 7 demand on existing services, 8 and access barriers similar to other health services and specific to STBBI testing (e.g., long wait-times for appointments, distance to services, fearing discrimination or judgement from healthcare providers, embarrassment or shame about getting tested).9–11 Digital STBBI testing services are an established way of providing STBBI testing in many countries12,13 and are becoming more common in Canada. 14 Typical models for these services include online ordering of home self-test kits, online ordering of kits for self-collection of specimens returned to a laboratory for testing or generating an online lab form to take to a lab. 14
In British Columbia, Canada, the BC Centre for Disease Control operates GetCheckedOnline.com, a digital STBBI testing service that was designed according to clinical best practices to complement provider-based testing (described elsewhere). 16 Prior research has demonstrated that GetCheckedOnline is acceptable,17,18 used by people facing barriers accessing STBBI testing, 9 has equivalent rates of treatment and partner notification compared to usual care, 19 and that service utilization increased as a result of the COVID-19 pandemic. 20 The service involves four steps: i) visit the website and create an account using an email address; ii) complete a risk assessment questionnaire and generate a lab form, iii) go to a local laboratory to provide blood, urine and/or self-collected throat and rectal swabs (tested for HIV, hepatitis C, syphilis, chlamydia and/or gonorrhea); and iv) receive results online if negative, or from a nurse if positive to arrange treatment and follow-up. After creating an account, people receive reminders to test and can test repeatedly. GetCheckedOnline is free, does not verify demographic information provided, and users are asked to consent to be contacted for evaluation purposes. As of July 2024, GetCheckedOnline is available in eight communities in BC. In 2022, 16,223 people used the service generating 22,443 tests with 55% of tests among repeat users (Figure 1).
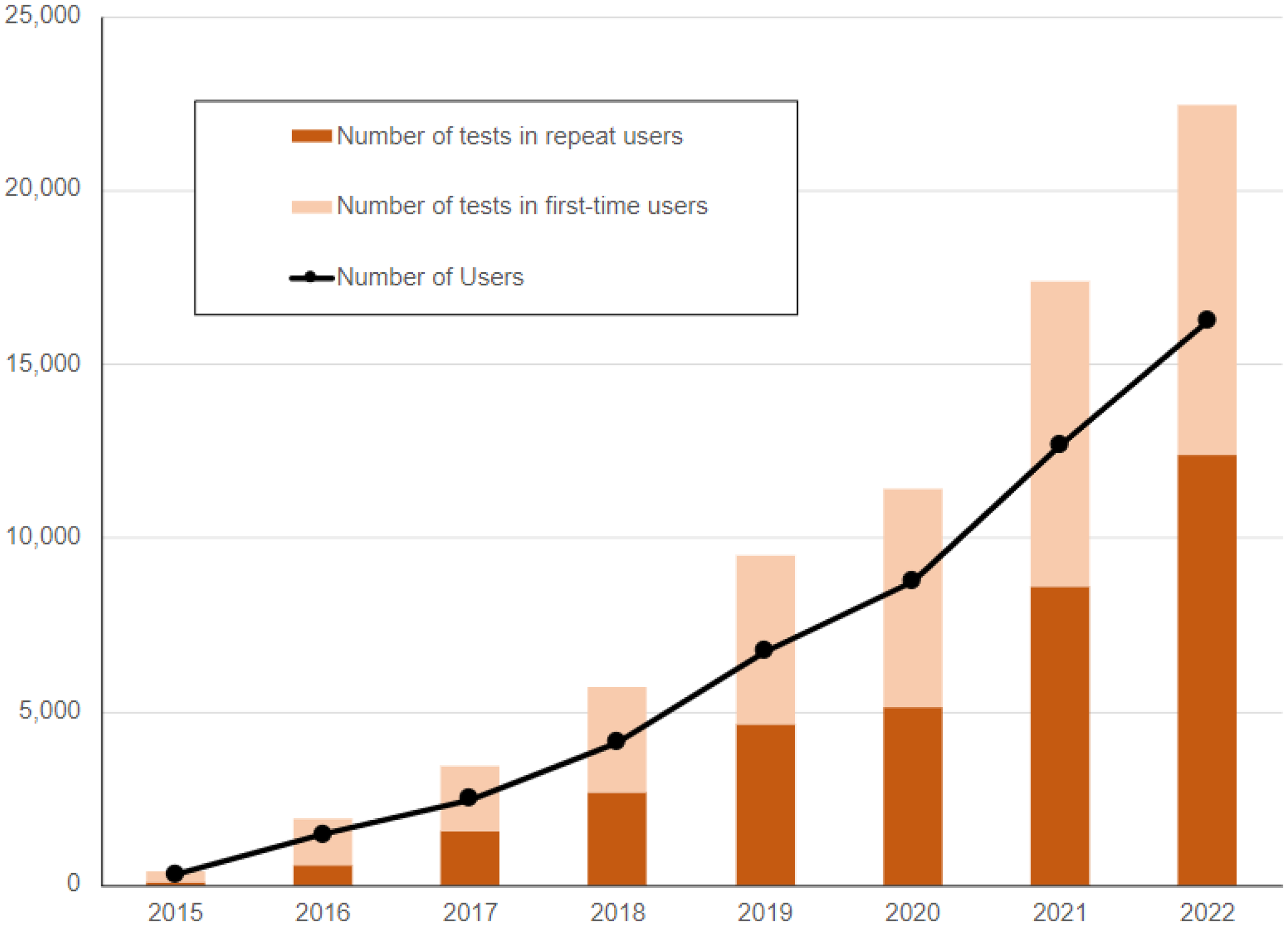
GetCheckedOnline program outcomes, 2015 to 2023.
Digital STBBI testing services like GetCheckedOnline are assumed to decrease health-care system burden by shifting asymptomatic, routine testing away from provider-based clinical testing services to online. However, there is little evidence supporting this assumption and limited understanding of how service users use both digital and provider-based testing services. The primary objective of our exploratory study was to describe patterns of use, and perceptions of, digital and provider-based testing services among GetCheckedOnline users. As a secondary objective, we determined whether barriers accessing provider-based testing were associated with these patterns. We hypothesized that individuals with these barriers would be more likely to report greater use of GetCheckedOnline for testing.
Methods
We used the STROBE statement for reporting on cross-sectional studies to organize our results. 15
Study design, population and setting
We conducted an online, cross-sectional survey of repeat users of GetCheckedOnline, who we considered most likely to have established a pattern of use of GetCheckedOnline and provider-based testing services.
Survey instrument
We developed a survey for people who repeatedly use GetCheckedOnline for testing (repeat users). The maximum survey length was 81 questions across five domains including participants’ use and perception of GetCheckedOnline, socio-demographic characteristics, access to and use of provider-based STI testing, sexual behaviour and use of healthcare and technology. Survey questions were informed by prior research findings about GetCheckedOnline mapped to single constructs of the Theoretical Domains Framework,9,18,20 and selected based on the feedback of program implementers and our Community Advisory Board comprising people from populations affected by STBBI across BC. The survey was pilot-tested with 10 community members familiar with GetCheckedOnline and subsequently modified to enhance language accessibility (for survey instrument, see Appendix).
Recruitment and data collection
Eligible repeat users of GetCheckedOnline met the following criteria: i) had previously consented to be contacted for evaluation purposes; ii) having ≥2 tests through GetCheckedOnline, with ≥1 test between April 7, 2022, and October 7, 2022; iii) created an account prior to this period; and iv) 16 years of age or older. Invitations to the online survey were sent to eligible participants on 21 November 2022, with email reminders at 2, 4 and 7 days until the survey closed on December 6. The survey landing page described the purpose of the study, additional eligibility criteria (able to complete the survey in English) and offer of a $20 honorarium, with proceeding to the survey taken as provision of informed consent. We collected survey data using REDCap electronic data capture tools hosted at the BC Children's Hospital Research Institute. 21 Ethics approval for this study was obtained from the UBC Behavioural Research Ethics Board.
Statistical analysis
Survey data was imported into R version 3.5.2 (2018-12-20) for analysis 22 and participants who reported testing <2 times through GetCheckedOnline were excluded. Our primary outcome of interest was patterns of use of GetCheckedOnline and provider-based testing, based on the question ‘What best describes your current way of getting tested for STIs?’ which was collapsed into a three-level ordinal variable (ranging from least to most use of GetCheckedOnline compared to testing through healthcare providers): i) test more often through healthcare providers or test equally through GetCheckedOnline and health care providers; ii) mostly test through GetCheckedOnline, sometimes through a healthcare provider; and iii) only test through GetCheckedOnline. For barriers related to accessing testing, we grouped survey variables according to the following health policy context categories from the Health Equity Measurement Framework. 23 Availability, or the infrastructure and organization for provision of services, included the variables having a primary care provider, and having a usual place where comfortable getting tested by a healthcare provider for STIs. As availability of providers for testing may have been lower for participants creating their accounts during the COVID-19 pandemic we also included reported time since account creation as an availability variable. Accessibility, or an individual's ability to use services when needed, included the variables ease of seeing a provider for STI testing when needed and feeling anxious in clinic waiting rooms when testing for STIs. Acceptability, or provision of respectful and responsive services regardless of social location, included the variables comfort discussing sexual history with healthcare providers, and worry about being judged by healthcare providers when providing a sexual history. Appropriateness, or providing suitable, evidence-based health services balanced with individual needs and preferences, included the variable for requiring STBBI testing as part of routine clinical care for HIV treatment, HIV pre-exposure prophylaxis or contraception (i.e., where offer of STBBI testing by providers to participants would be routine).
To adjust for non-response bias, we applied post-stratification weights based on program data for age, gender identity and number of GetCheckedOnline tests performed by all repeat users eligible for the study (weighted percentages presented below). 24 We conducted bivariate analyses between our outcome of interest and barriers related to accessing testing and key socio-demographic characteristics using ordinal logistic regression weighted using the same post-stratification weights. We also described reasons for use of healthcare providers for testing among participants reporting using both digital and provider-based testing services.
Results
Of 4633 eligible repeat users of GetCheckedOnline, 798 (17.2%) were included in our final analysis, or 44% of the 1798 eligible repeat users who had previously consented to be contacted for research and invited to this survey (Figure 2). The median age of participants was 33 years, 59.3% were White, 48.0% were women, 66.7% had a sexual identity other than straight/heterosexual and 58.8% had a Bachelors’ degree or higher (Table 1). A minority had been homeless or unstably housed in the past year (1.2% and 6.8%, respectively), and 33.6% of participants reported an annual income <$40,000. One-eighth (11.9%) of participants were recent immigrants to Canada.

Recruitment outcomes.
Description of survey participants who were repeat users of GetCheckedOnline in BC and tested between April 7 and October 7, 2022 (N = 789).

Missing responses excluded.
Percentages shown are weighted percentages (post-stratification weights based on age, gender identity, and number of times tested through GetCheckedOnline).
Four (7%) Indigenous participants identified as Two-Spirit.
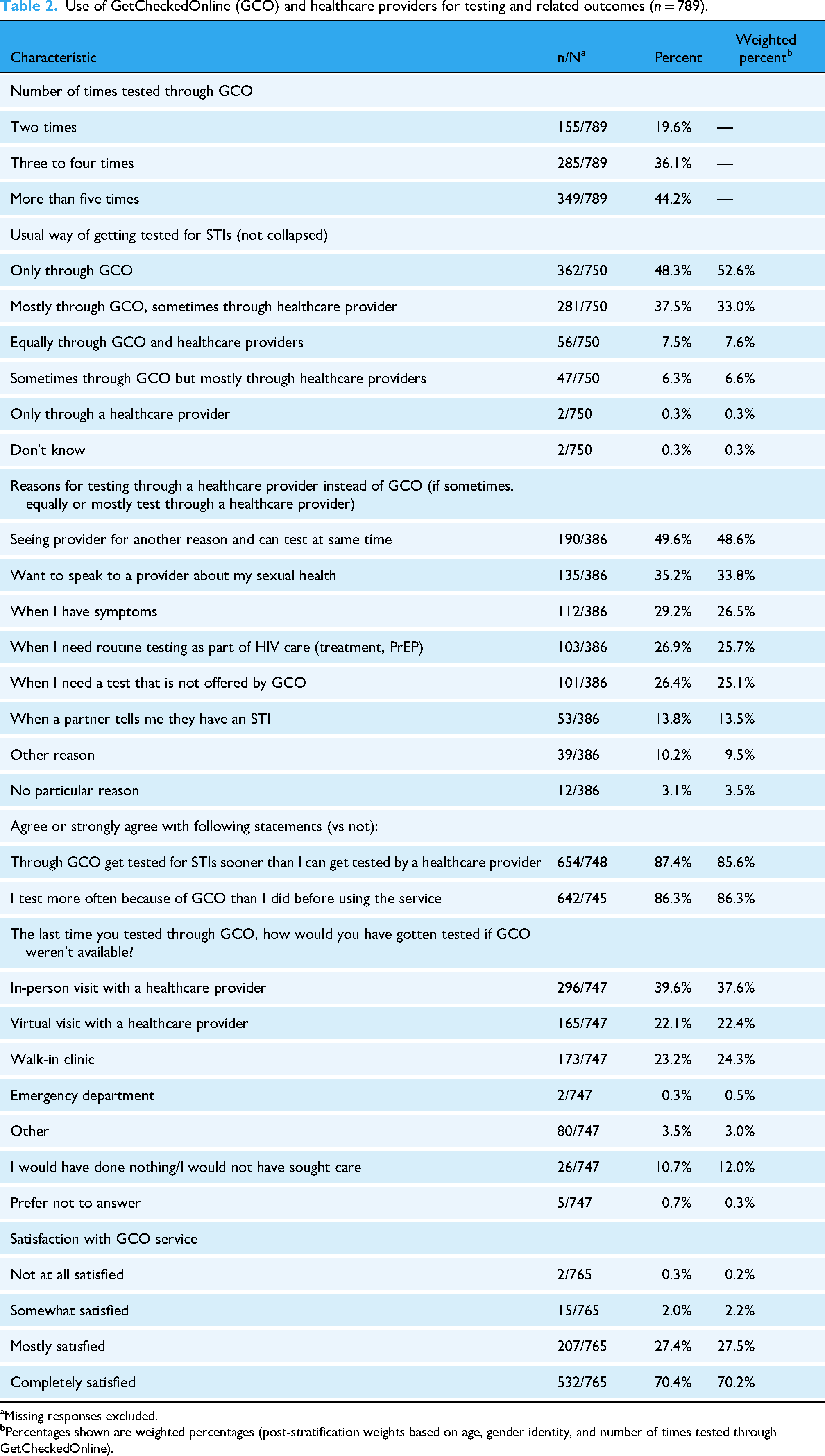
Most participants had tested three or more times through GetCheckedOnline (80.3%), creating accounts in the past year (14.8%), past 1–2 years (48.0%) and ≥3 years ago (35.8%) (Table 2). Most participants agreed or strongly agreed that they tested sooner through GetCheckedOnline than through a provider (85.6%) and were testing more often than before using GetCheckedOnline (86.3%). While most participants reported that they would have tested through a healthcare provider if GetCheckedOnline had not been available, 12.0% reported they would have done nothing/would not have sought care. Overall, 97.7% of participants reported being mostly or completely satisfied with GetCheckedOnline.
Use of GetCheckedOnline (GCO) and healthcare providers for testing and related outcomes (n = 789).
Missing responses excluded.
Percentages shown are weighted percentages (post-stratification weights based on age, gender identity, and number of times tested through GetCheckedOnline).
Regarding patterns of use, over half of participants described their usual way of testing for STIs as being only through GetCheckedOnline (52.6%), with 33.0% reporting mostly testing through GetCheckedOnline and sometimes through a healthcare provider, and 14.5% reporting testing more often or equally through healthcare providers. We found greater use of GetCheckedOnline was associated with factors related to availability of provider-based testing including not having a primary care provider and not having a usual place where comfortable getting tested for STIs by a provider (Table 3). Creating an account three or more years earlier (i.e., pre-COVID pandemic) was associated with less use of GetCheckedOnline. Variables related to accessibility and acceptability of provider-based testing were not associated with patterns of use; however, appropriateness of testing through a provider was associated with lower use of GetCheckedOnline for testing (getting tested for STI as part of clinical care). Among 386 participants who reported using a combination of GetCheckedOnline and providers, the most common reasons for testing through a provider instead of GetCheckedOnline included when seeing a provider for another reason (48.6%), when wanting to speak to a provider about sexual health (33.8%) and when having symptoms (29.2%) (Figure 3).
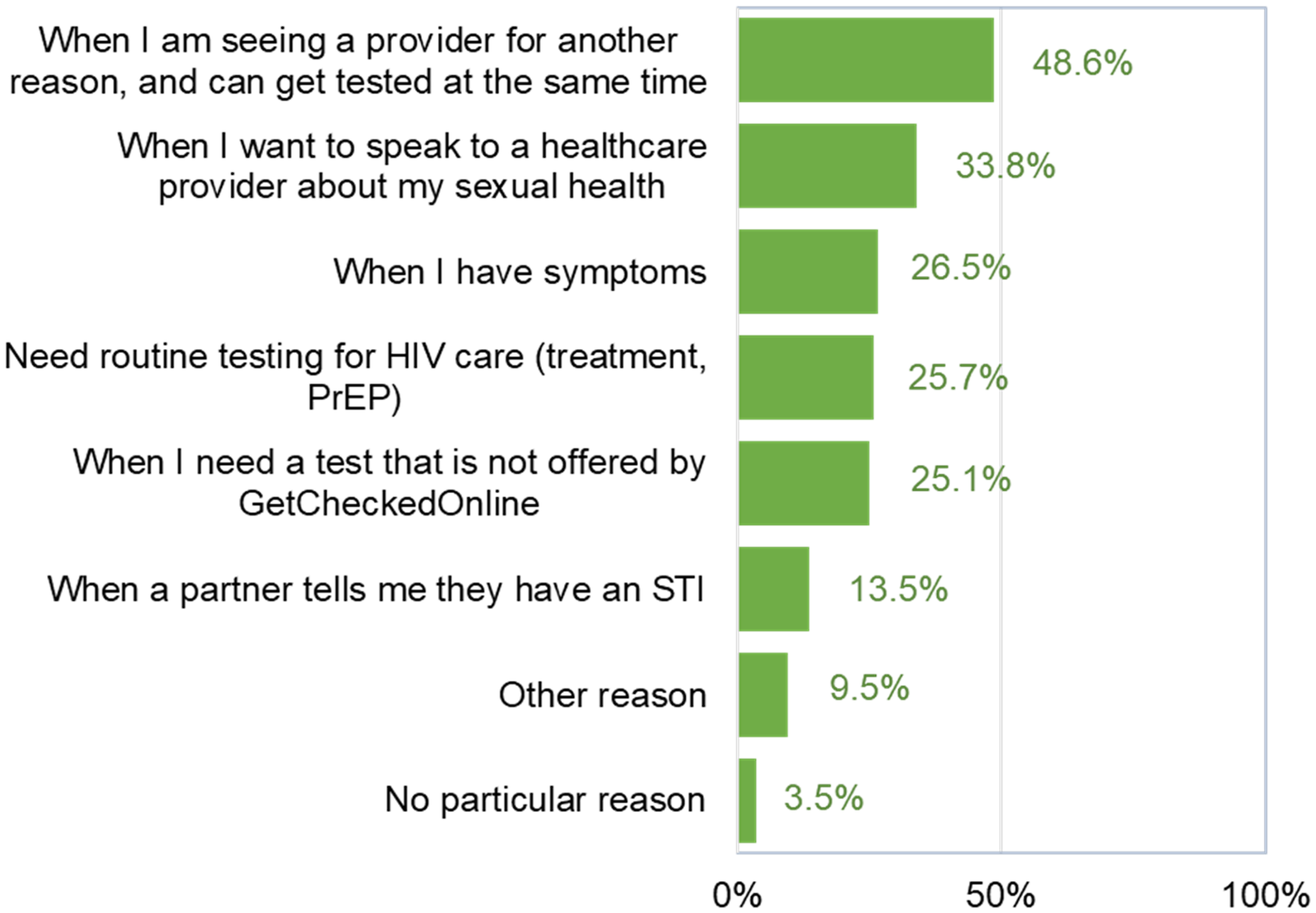
Scenarios for testing through healthcare providers instead of GetCheckedOnline (N = 386 participants reporting testing through a combination of both modalities; multiple responses possible).
Results of bivariate analysis of patterns of use of provider-based testing and explanatory variables (n = 742; 732 for weighted analyses).

Notes: Participants with missing data or ‘Prefer not to say’ responses excluded from analyses of each variable. Percentages are weighted percentages (N = 732).
GCO: GetCheckedOnline; HCP: Healthcare Professional; OR: weighted odds ratio (OR > 1 indicates greater use of GCO).
Bold values indicate statistical significance.
In terms of socio-demographic factors, age < 25, having up to high school education, earning less than $20,000 per year and being born outside Canada were associated with greater use of GetCheckedOnline for testing (Table 3). 2S/LGBTQ+ identity and full-time employment were associated with less use of GetCheckedOnline for testing. Race/ethnicity, gender identity variables and being underhoused were not associated with greater or lesser use of GetCheckedOnline for testing.
Discussion
Approximately 85% of our sample tested mostly or only through GetCheckedOnline, with greater use of GetCheckedOnline associated with barriers related to the availability of provider-based testing, suggesting GetCheckedOnline is improving access to STBBI testing for some repeat users of the service. However, 89% of the sample said they would have tested elsewhere (i.e., through a healthcare provider) if GetCheckedOnline had not been available the last time they tested. These findings support the assumption that digital STBBI testing services like GetCheckedOnline reduce the demand on the healthcare system by shifting testing away from provider-based clinical testing services. As expected, testing through providers as a routine part of ongoing clinical care such as HIV pre-exposure prophylaxis was associated with lower use of GetCheckedOnline for testing, and participants commonly reported testing through providers for these and other scenarios where provider-based testing would be recommended.
Few other studies have explored patterns of use of both digital and provider-based services for STBBI testing, and these have been primarily focused on sexual health clinic settings.25,26 Other surveys have suggested that patient use of digital technologies may reduce demands on healthcare providers (e.g., access to own electronic health information leading to avoided clinic or emergency room visits) 27 or overcome gaps in access to primary care (e.g., telehealth users having lower access to primary care). 28
While our study suggests that digital STBBI testing services like GetCheckedOnline may decrease the demand on healthcare providers for testing, another common rationale for these services is their impact on health equity, reaching populations facing disparities in resource access. 29 We did find that lower income, lower education, younger age and immigrant status were associated with greater use of GetCheckedOnline for testing, suggesting equitable improvements in access for these groups. While participants identifying as 2S/LGBTQ + had lower use patterns of GetCheckedOnline for testing, this may be related to greater existing access to testing or use of HIV PrEP in this group.
Given the importance of health system contexts, validation of these findings in other jurisdictions and with different service models is needed. Further studies should also better quantify the impact on primary care providers of digital STBBI testing services at scale, including modeling and economic analyses, 30 and understand healthcare provider perspectives on these services. Further work exploring the equity implications of our findings is also needed.
As a long-running digital STBBI testing service in Canada which has been scaled up to multiple geographic communities, our study was well positioned to look at how repeat users access both digital and provider-based testing and included long- and short-term repeat users of the service. Our findings may be generalizable to other Canadian jurisdictions and to similar models of digital STBBI testing services. We also acknowledge that only 17% of all eligible repeat testers during our study period participated in the survey. While we used post-stratification weighting based on the prevalence of key socio-demographic factors of all repeat testers, it is possible that selection bias may have affected our results (e.g., if repeat testers with access to providers were more likely to participate).
Conclusion
Our study suggests digital STBBI testing services improve equity in testing access and supports the assumption that they reduce healthcare system demands by shifting provider-based to digital testing services. Our findings have implications for scaling-up overall access to STBBI testing, as the majority of tests conducted through these services may be shifted from health care providers, avoiding costs to the healthcare system. However, further research using population-level testing and health utilization data is needed to more robustly understand the impact of digital STBBI testing services within the broader testing ecosystem. Furthermore, we caution that these patient and health system benefits of digital STBBI testing should not be a reason for replacing or reducing the availability of provider-based testing services – both as an appropriate route of testing and for populations with lower digital literacy. As digital STBBI testing services become more common in Canada, it will also be important to ensure that these services are of high quality, adapt to reflect changes in testing recommendations and provide clinically appropriate information – a challenge that is emerging elsewhere, particularly in relation to for-profit providers of these services. 31
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251339016 - Supplemental material for Use of GetCheckedOnline and testing through healthcare providers among repeat users of British Columbia's digital testing service for sexually transmitted and blood-borne infections: Findings from a cross-sectional survey
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251339016 for Use of GetCheckedOnline and testing through healthcare providers among repeat users of British Columbia's digital testing service for sexually transmitted and blood-borne infections: Findings from a cross-sectional survey by Mark Gilbert, Aidan Ablona, Hsiu-Ju Chang, Ihoghosa Iyamu, Rodrigo Sierra-Rosales, Heather Pedersen, Paul Flowers, Nathan Lachowsky, Daniel Grace and Catherine Worthington in DIGITAL HEALTH
Supplemental Material
sj-doc-2-dhj-10.1177_20552076251339016 - Supplemental material for Use of GetCheckedOnline and testing through healthcare providers among repeat users of British Columbia's digital testing service for sexually transmitted and blood-borne infections: Findings from a cross-sectional survey
Supplemental material, sj-doc-2-dhj-10.1177_20552076251339016 for Use of GetCheckedOnline and testing through healthcare providers among repeat users of British Columbia's digital testing service for sexually transmitted and blood-borne infections: Findings from a cross-sectional survey by Mark Gilbert, Aidan Ablona, Hsiu-Ju Chang, Ihoghosa Iyamu, Rodrigo Sierra-Rosales, Heather Pedersen, Paul Flowers, Nathan Lachowsky, Daniel Grace and Catherine Worthington in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions of the BC Centre for Disease Control Sexual Health Advisory Group which served as the Community Advisory Board for this study and provided feedback on survey design and interpretation of findings. The authors would also like to thank Dr Travis Salway, Faculty of Health Sciences and Simon Fraser University for his contribution to study design.
ORCID iDs
Ethical considerations
Ethics approval for this study was obtained from the UBC Behavioural Research Ethics Board (ethics #H18-00437).
Author contributions
MG led all aspects of this study. AA, HC, II, HP, PF, NL, DG and CW contributed to study design with AA, HC, II, and RSR contributing to data analysis. All authors contributed to interpretation of study findings and preparation of this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was supported by the Canadian Institute of Health Research (CIHR) [Implementation Science Team Grant: FR# CTW- 155387; PIs: MG, DG, CW].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.