
Abstract
Background
Despite its benefits, cardiac rehabilitation (CR) participation rates remain subpar. Telehealth lifestyle interventions have emerged as modalities to enhance CR accessibility. Virtual-world (VW) technology may provide a means to increase CR use.
Objectives
This pilot study assessed the feasibility and acceptability of a VW-based CR program as an extension to medical center-based CR. Our goal is to apply the study results toward the design of a patient-centered VW platform prototype with high usability, understandability, and credibility.
Methods
Patients (n = 8, 25% women) recently enrolled in outpatient CR at Mayo Clinic, Rochester, Minnesota participated in a 12-week, VW health education program and provided feedback on the usability, design and satisfaction of the intervention at baseline and completion. A mixed-methods approach was used to analyze the participant perceptions of the intervention.
Results
Overall, there were positive participant perceptions of the VW experience. There was unanimous high satisfaction with the graphical interface appearance and ease of use. Participants placed value on the convenience, accessibility, and social connectivity of the remote program as well as the novelty of the simulation platform presentations, which aided in memorability of key concepts. Greater than 80% of participants reported that the program improved their health knowledge and helped to maintain better health habits.
Conclusions
Our pilot study revealed the feasibility and acceptability of an innovative VW-based CR program among cardiac patients. This novel delivery method for CR has the potential to influence healthy lifestyle change and to increase accessibility to vulnerable populations with higher cardiovascular disease burdens.
Keywords
Introduction
Despite an abundance of evidence demonstrating clear benefits of cardiac rehabilitation (CR) for patients with coronary artery disease and other cardiac diagnoses in improving cardiovascular fitness, cardiovascular disease (CVD) risk factors and quality of life, and reducing hospitalizations and cardiovascular mortality, it remains drastically underused.1,2 The reasons for this issue are multifactorial, inclusive of patient-, provider-, and systems-level factors. 3 The current CR model must undergo significant infrastructure changes focusing on increasing patient convenience through alternative delivery models. Approaches to “rebrand and reinvigorate” traditional CR programs through the integration of digital and mobile technologies are key to transforming the current paradigm toward a more patient-centered program to increase CR enrollment, participation, and completion.2,4–8
Fundamental strategies to integrate into CR programs include those that promote social connectedness, engagement, and quality of life. 9 Virtual-world (VW) environments offer a potential innovative technology to improve health outcomes through rehabilitation,10,11 disease self-management,11–13 healthy lifestyle change 14 and social networking. 9 VWs are immersive, three-dimensional environments that foster a more synchronous experience for experiential learning, skill-building, and socialization. 10 These inherent features are patient-centric and complementary to CR core components and competencies as outlined by national secondary prevention guidelines that aim to optimize cardiovascular risk reduction, foster healthy behaviors, and promote an active lifestyle for cardiac patients. 15 VWs may also represent a valuable tool to expand the reach of CR by increasing its accessibility to underserved groups.10,12,13
The aims of this pilot study were the following: (1) to assess the feasibility of implementation of a 12-week VW-based CR program as an extension to conventional CR, (2) to probe the acceptability, ease of use, utility, and satisfaction of a VW-based CR education program among cardiac patients, and (3) to examine the perceptions regarding the VW-based platform by cardiac patients. The information gleaned from the study will inform the design of a patient-centric, VW platform prototype with high usability, understandability, and credibility to apply within a broader comparative effectiveness study. 10
Methods
Study setting and participants
We recruited patients recently enrolled in outpatient CR at Mayo Clinic Rochester, Minnesota, through the assistance of CR staff. Among those recruited, the indications for CR were the following: recent hospitalization for acute coronary syndrome (ACS) (unstable angina, ST-segment elevation myocardial infarction, non-ST-segment elevation myocardial infarction), heart valve replacement, elective percutaneous coronary intervention (PCI), and stable angina. Eligible patients were required to continue with standard CR and have regular high-speed internet access (home, work or community). Patient exclusion criteria included < 18 years of age, lack of basic internet navigation skills and non-fluency in English. The feasibility study research protocol was reviewed and approved by the Mayo Clinic Institutional Review Board.
Upon informed consent completion, each participant received hands-on instructional training by a study investigator (B.K.) on the VW platform (Second Life® account activation, avatar creation, basic navigational skills). Personal laptops installed with VW software and personal headsets were provided to each participant for use throughout the intervention.
Intervention
Intervention development
The study investigators engaged with two community-based, cardiac patient-led groups in intervention development. One group, One Voice, is a patient/family advisory council within the Mayo Clinic Department of Cardiovascular Diseases, which provides input on any aspect of practice, education, research, policy, and procedure development to ensure responsiveness to individual patient values and preferences. The other group, the Rochester Coronary Club, is a local support group for CVD survivors. Three community presentations detailing the feasibility study proposal were delivered by the study team (L.B., B. K., S.K.) with integrated VW (Second Life®) platform demonstrations from January 2014 to February 2015. The proposal was well received by both groups and the study team gleaned excellent feedback on recruitment strategies and intervention refinement.
Self-determination theory 16 informed the development of the VW platform and education curriculum to foster healthy behavior change given its focus on an individual’s beliefs and effectiveness in performing behaviors (competence), connection with others (relatedness), and perceived control over behaviors (autonomy). In addition, the intrinsic features of the intervention are to encourage healthy lifestyle behaviors by participant avatars with the goal of transferring these behaviors to the real world (i.e. Proteus effect 14 ).
Intervention delivery
Virtual world education session topics.


Peer social support group, concluding education session 12.
Measures
A comprehensive electronic pre-intervention survey assessed participant sociodemographics, social support, 17 digital health information access, and prior VW experience. The post-intervention survey included 18 questions probing participant perceptions of the VW intervention on several domains (overall experience, usability, logic of information, and utility) through both closed and open-ended questions from previously validated tools.18–22 Participants rated each domain on a five-point Likert scale (very unsatisfied to very satisfied or strongly disagree to strongly agree). We aggregated responses into “satisfied/very satisfied,” “neutral,” “strongly disagree/disagree,” and “agree/strongly agree” as a percentage of the total participant group. Participant education session series attendance and presentation feedback (style, content, etc.) statistics were also collected.
Data analysis
Quantitative data
For normally distributed variables, simple arithmetic means and standard deviations were calculated. Frequencies and proportions were calculated for categorical variables. Analyses were performed using commercial software (SAS, version 9.2; SAS Institute).
Qualitative data
Qualitative analysis was conducted by an independent analyst (K.S.) of the participant post-intervention open-ended responses that was informed by both ethnomethodology 23 and structural narrative analysis 24 approaches. Ethnomethodology is a descriptive approach to understanding behaviors among individuals within groups and how they use social interaction to maintain an ongoing sense of reality in situations and environments. This framework facilitated the systematic review of the narrative responses according to their structure and conveyed meanings. Initially, a comprehensive catalog of aggregated major themes of likes, dislikes, and suggestions for improvements to the VW platform was created. Subsequently, a form of structural narrative analysis was used to examine how each respondent connected themes into a sequence to convey meaning about what mattered most or least or in relation to another feature of the VW platform.
Results
Sample description
Baseline characteristics of study participants (N = 8) a .

A total of eight participants enrolled into the study; one participant withdrew before the start of education session series.
Social support is represented as an average of a total score sum of seven items from each participant. 11 (Items 1–6, Scale 1–5: 1 [“None of the time”] through 5 [“All of the time”] and Item 7 scored 4 for “yes” and 2 for “no.”; score range: 8–34).
Intervention acceptability
Virtual world-based cardiac rehabilitation acceptability (N = 7).

Frequencies not adding up to post-intervention total (N = 7) indicate missing data.
Virtual world-based education session series feedback.
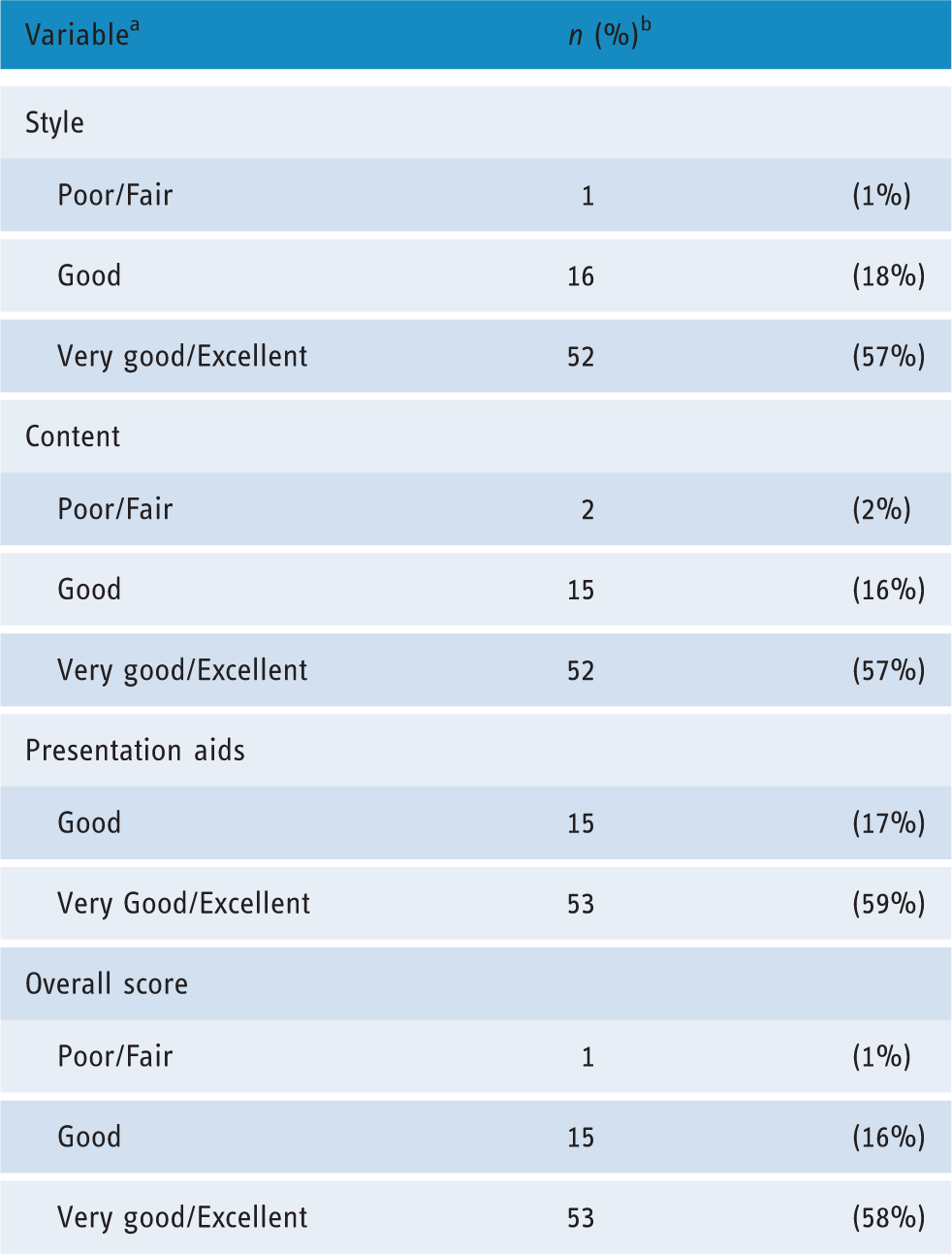
For each variable, percentages not adding up to 100% represent missing data or participant lack of attendance of particular sessions.
Note frequencies represented as composite of all participants (N = 91 responses).
Intervention qualitative perceptions
Post-intervention survey responses revealed several themes regarding likes, dislikes, and suggestions for improvement of the intervention and education program. These responses coalesced into three valued priorities among the participants including: (1) time/space flexibility, (2) memorability, and (3) post-intervention concept reinforcement.
Time/space flexibility
Participants specifically liked that the program could be accessed anywhere, even while traveling, and did not require preparation. One individual noted: “It is interactive with visuals yet can be done from home and without having to take the time to comb my hair (or other embarrassments of face time) …it’s easier to pick up a computer for an hour at home than to get dressed, get in the car and go somewhere for an hour session somewhere away from home which ends up taking two hours when it is all done.” “One of the best parts of Second Life was the ability to interact, ask questions, to participate. Without the distraction of evaluation that comes with seeing another person. Or the self-consciousness of being seen.” “Some speakers started to rush through as the talk went along as if they thought the audience had quit listening. They might have had better presentations with eye contact.”
Memorability
Participants felt that the VW simulations and range of physical environments (restaurant, exercise facilities) intensified the emotional experience and, thus, enhanced the memorability and retention of the subject matter on healthy lifestyles. One participant mentioned that he or she had developed an emotional connection to their avatar, noting that the VW technology created a sense of really “being there,” of “humanity,” and being “person-to-person”: “I would miss that in a way that would not be true in any other online interaction.” “Everyone getting to know each other and speaking up … to communicate with the presenter, staff and fellow participants and hearing other participants’ stories and opinions.”
Post-intervention concept reinforcement
Participants expressed a desire to connect the series to real life; that is, to reinforce learning from the education sessions to life beyond the program. Several expressed a strong desire to build community beyond the workshop, with use of the VW platform for forums to mentor and support each other. An illustrative comment promoting social support is as follows: “Invite me back! Teach me how to be a support layperson counselor so that I can help others be more comfortable with this virtual world experience.”
Beyond the aggregated three priorities, additional comments highlighted the novelty of the VW delivery method for CR: “I cannot think of any other application or situation that offers all these things, making it unique … I think there are endless possibilities for this format.”
Discussion
Capitalizing on telemedicine advances toward creating alternative CR delivery models is paramount to increasing CR access and participation. 2 Our study results suggest the potential use of VW technology as a feasible and acceptable means for promoting CR participation and delivering cardiovascular health education. Participants reported overall positive perceptions of the VW-based CR program due to its ease of use, innovative graphics and simulations, and novel education delivery approaches. Many participants felt that the interactive simulations and real-time VW education sessions aided in their memorability of key concepts of secondary CVD prevention, which prompted adoption of healthy behaviors in the real world—the ultimate objective to improve health outcomes (i.e. Proteus effect). 14 Participants reported a minimization of distractions within the VW environment in comparison to the face-to-face environment of center-based CR that allowed them to focus on the CR education content and develop supportive, virtual interactions with other participants. Participants particularly gravitated to the social connectivity and sense of camaraderie afforded by the VW experience in coping with shared experiences of heart disease.
We recognize that our pilot study is a small, single-site feasibility trial that limits generalizability. We also acknowledge that our participants were largely of high socioeconomic status; however, the majority lacked prior experience with VW technology. VW technology has also been successfully used within a socioeconomically disadvantaged group (of variable digital literacy) engaged in a diabetes self-management program with high user satisfaction and retention. 13 Nonetheless, it is the first study to our knowledge evaluating the use of VW-based technology for CR, particularly through a designated medical center of excellence. Our study indicates an openness and perceived utility toward a VW environment for home-based CR among cardiac patients that has been further supported by similar groups. 25 Participant engagement and retention were excellent as the education sessions were well-attended and all but one participant completed the entire program. Future studies using VW in CR should emphasize social support and networking to promote participant cohesiveness and relationship-building. It is also of utmost importance to assess the acceptability of VW in CR among underserved groups with the lowest CR utilization, including ethnic minorities, rural residents, the elderly, and the economically disadvantaged. Thus, recruitment is underway for the next phase of the VW in CR trial by the study investigators with an aim of prioritizing this patient demographic.
Footnotes
Acknowledgements
We are grateful to the Mayo Clinic outpatient cardiovascular rehabilitation program staff members for assistance with participant recruitment. The authors would also like to show gratitude to Mayo Clinic faculty/staff for volunteering their time as speakers for the education session series.
Contributorship
All authors participated intellectually or practically in this work including the conception (SK, BK, LB), and design (LB, BK, KK, RS, RT, SK) and analysis (LB, KS, SK). LB wrote the initial draft of the manuscript. All authors have made substantive contributions to this study and endorse its data and conclusions. All authors have reviewed, edited, and approved the final submitted manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board for Mayo Clinic, ID: 14-005945.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Mayo Clinic Center for Clinical and Translational Science, the Mayo Clinic Department of Cardiovascular Diseases, and the American Medical Association Foundation Seed Grant Research Program.
Guarantor
LB
Peer review
This manuscript was reviewed by Sally Singh, Coventry University UK, Konstantinos Antypas, University Hospital North Norway, and one other individual who has chosen to remain anonymous.