
Abstract
Introduction
Internet use disorder is a disorder of the digital age and presents a growing problem worldwide. It appears that due to structural and personal barriers, many persons affected (PA) and Concerned Significant Others (CSO) do not reach the health care system so far and thus a chronification of the pathology can proceed.
Methods
A telemedicine counseling service for PA and CSO of PA unwilling to enter treatment with two webcam-based sessions of 60 minutes for each group was created with the aim of reaching out to PA and CSO to provide a low-threshold support and refer the participants to the local health care system. Motivational interviewing for PA and CRAFT (Community Reinforcement and Family Training) for CSO were used as methods. Participants answered questions about their Internet use and sociodemographic data and six months after participation, participants were asked via email if they entered the local health care system. CSO answered the questions for themselves and in a third-party rating for PA unwilling to enter treatment.
Results
107 PA (34 years (SD = 13.64), 86% male) and 38 CSO (53 years (SD = 6.11), 28.9% male) participated in the two telemedicine sessions. After participation, 43.9% of the PA and 42.1% of the CSO reached the health care system. When there was consistency between the location of telemedicine consultation and treatment locally, over 90% of participants arrived (PA: 92.3%, CSO: 100%).
Conclusion
The results from this study reveal that telemedicine services could be a promising approach to address PA and CSO and build a bridge to the local health care system. Future studies should verify if these results can be replicated in randomized controlled trials.
Keywords
Introduction
Internet Gaming Disorder was included in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) in 2013 1 and 2018 Gaming disorder (GD) was designated as “disorder due to addictive behaviors” in the 11th edition of the International Classification of Diseases (ICD-11 2 ). GD is characterized by excessive or poorly controlled gaming behavior, increased priority given to gaming, and continuation of gaming despite the occurrence of negative consequences, and the gaming pattern must be so pronounced that it causes marked distress or functional impairment in daily life. 2 In addition to GD, the category of hazardous gaming is defined in the ICD-11. Hazardous gaming refers to a pattern of gaming that increases the risk of harmful physical or psychological consequences to the individual or others around the individual. 2 Differences between the two categories GD and hazardous gaming are seen by less severe or not at all developed diagnostic criteria in the category of hazardous gaming and that in the case of hazardous gaming significant impairments in personal, social, occupational, or other important areas of functioning are not yet developed. 2
Besides GD, other specific Internet use behaviors should be considered as addictive behaviors, such as the excessive or poorly controlled use of online pornography, social networks, or online shopping. 3 Therefore, the term “Internet Use Disorder” (IUD) is used frequently as an umbrella term for the pathological use of various Internet applications. 4
The Interaction of Person-Affect Cognition Execution (I-PACE) model is one model which outlines the development and maintenance of GD and specific IUD. The I-PACE model posits that diminished cognitive control influences the decision-making process, resulting in the decision to use the Internet. 9 Existing treatment methods may not only help identify ambiguities and increase motivation to change behavior, but also help modify maladaptive cognitions that underlie Internet use and generate distress.10,11
Prevalence rates of GD and IUD vary worldwide depending on assessment tools, sample size, -type, and year of data collection.12,13 Systematic reviews show a global prevalence for IUD of 7.02% on average. 13 Global prevalence rate for GD is 3.05% and 1.96% when only studies that met more stringent sampling criteria (e.g. stratified random sampling) are considered. 12 Women use social networks more frequently, while men predominantly use games.12,14
Higher prevalence rates are reported for younger compared to older individuals, as well as for hazardous Internet use compared to IUD.14,15 Considering the ongoing digitalization together with the reported prevalence rates, an appropriate health care system with specialized treatment structures for person affected (PA) and Concerned significant others (CSO) is essential. Health care system is used as an umbrella term for different types of treatment on-site, like addiction counseling facilities, outpatient clinics, and inpatient clinics.
A systematic review and meta-analysis indicate that cognitive behavioral therapy (CBT) contributes to symptom reduction of GD in a direct comparison before and after treatment, but the long-term effects of CBT need to be systematically assessed in further studies.16,17 Additional treatment approaches (medication, family therapy, and other specialized treatment interventions) for GD have already been examined in initial studies, but due to methodological limitations, conclusions can only be drawn cautiously about their effectiveness. 18 Motivational Interviewing (MI) techniques are often used in counseling individuals with addictions to identify ambiguities and increase motivation for behavior change. 11 Efficacy of MI techniques has already been demonstrated in the treatment of substance abuse19,20 as well as in treating PA with IUD. 21 MI techniques work in traditional treatment and counseling settings as well as in Internet- and telephone-based counseling sessions.5,6
In addition to the PA, the CSO also suffer strongly from the consequences of the disorder with an increased risk of physical and mental illness resulting from financial difficulties and/or interpersonal conflicts. CSO often find themselves in a conflict between providing support for the PA on the one hand and suffering from the consequences of the disorder on the other hand.7,8 Community Reinforcement and Family Training (CRAFT) is a communication training program for family members of PA who are not willing to enter treatment, with the goal of simultaneously improving CSO well-being and motivating the PA to enter treatment. 22 The effectiveness of CRAFT has been demonstrated especially in the work with CSO of alcohol abusers23–25 and in counseling CSO of PA with problematic gambling.26,27
Demand for specialized interventions for PA with IUD and CSO is steadily increasing,28,29 but there is still a lack of evidence-based guidelines and a comprehensive care structure for PA and CSO.30–33
Telemedicine interventions in addictive behaviors
The number of telemedicine services for individuals with substance abuse (e.g. alcohol abuse, smoking cessation) and behavioral addictions (e.g. gambling disorder) has increased in recent years34–36 and telemedicine is becoming more and more accepted by practitioners and PA.37,38 A systematic review identified 27 articles of telemedicine interventions for problematic gambling with one-to-one counseling by a trained therapist as the most common form of intervention with a variety of methods including videoconferencing, telephone, email, and chat. The results show that telemedicine interventions were effective in reducing problem gambling scores and gambling behaviors, but little comparison with face-to-face interventions and a lack of diversity in samples (recruitment via existing gambling help sites) were identified that require further investigation. 35
There are still few telemedicine services for PA with IUD 39 and, to our knowledge, none for their CSO. An interactive step-by-step Internet-based intervention based on MI techniques for the treatment of IUD for college students in china was created and showed a reduction of symptom severity for all three experimental groups (laboratory environment, natural environment, and using a non-interactive program) in comparison to the control sample. 40 Another study demonstrated comparable results in symptom reduction of IUD for a Virtual Reality Program as well as for CBT group therapy (8 sessions each) in a direct pre-post comparison. 41 Two randomized controlled trials of telemedicine interventions for individuals with IUD are currently ongoing. A guided Internet- and mobile-based intervention for individuals with IUD with pre-defined sessions and individualized feedback after completion of each session 42 as well as a four-week manualized webcam-based motivational intervention in a one-to-one setting with a personal consultant by our research group. 43 Although systematic reviews across various disorders show that primarily women use telemedicine services and health applications,44,45 the samples of existing telemedicine services for individuals with IUD are primarily defined by men. 39 Only one Internet-based intervention for the treatment of IUD for college students in china reports a primarily female sample. 40
Study aims
Although epidemiological data suggests that a significant proportion of the population should be affected by IUD,12–14 only a certain percentage of affected individuals (primarily male, pathological use of online computer games) and CSO reach the local health care system.17,30 In Germany, where the present study was conducted, a prevalence study was carried out with the result that 1% of the German population (16–64 years; around 550,000 Germans) is probably affected by an IUD. 14 An online survey of counseling and treatment providers for PA with IUD and CSO in Germany (n = 228) indicated that around 3500 PA and CSO each (approximately 3361 PA and 3491 CSO; sumscore self-calculated based on published sub-scores) in 2015 arrived at counseling and treatment providers. 30 Relating the results of these two studies, it can be assumed that approximately 0.64% of probably affected by an IUD reached the German health care system. This discrepancy suggests that the existing health care system does not provide adequate access to treatment options. Barriers to treatment include personal factors (e.g. wanting to manage on their own, shame, fear of stigmatization) and structural barriers such as distance, specialized treatment options, time problems, and responsibilities.46,47 Based on existing research indicating the efficacy of MI techniques for (telemedicine) programs in counseling and treatment of individuals with mental disorders and (behavioral) addictions,34,48,49 a low-threshold, location-independent telemedicine motivation-based program for individuals with IUD and CSO following the street-working approach50,51 was created.
The primary aim of this study was to conceive a short-term telemedicine motivation-based program with the aim of reaching out to PA and CSO to motivate them to seek treatment regarding their IUD and enter the local health care system. Due to the low organizational effort for continued treatment by the participants as well as the existing connection to the institution, it was hypothesized that an affiliation between telemedicine- and treatment institutions would promote the transfer to the local health care system. Secondary aim was to explore the profile of participants with the research question if PA and CSO who have not yet reached in the local health care system (women, different specific types of internet use, not in treatment so far, different stages of symptom severity) could also be addressed.
The efficacy of the telemedicine program in terms of symptom reduction, increase in motivation to change, and reduction in Internet use time has already been published separately. 52
Methods
Requirements for participation
The telemedicine study “Online-Ambulatory Service for Individuals with Internet Use Disorder and Concerned Significant Others” (OASIS; 52) addresses two different independent groups of individuals. On the one hand, PA who are dissatisfied with their Internet use and seek support and on the other hand CSO of PA who are not willing to enter treatment. The PA unwilling to enter treatment did not participate in the telemedicine consultation of the CSO.
All PA and CSO older than 18 years and with access to the Internet, webcam and an e-mail account could participate in the OASIS study. Exclusion criteria for PA and CSO were current psychotic disorders and/or primary substance-related disorders and/or suicidal ideations. The PA unwilling to enter treatment in the group of CSO had to be at least 14 years old.
Procedure
The telemedicine OASIS study was carried out from September 2016 to December 2019 in Germany, funded by the Federal Ministry of Health (ZMVI1-2516DSM207). Recruitment for study participation took place via social networks as well as participation at the largest computer game convention. The project was also presented to health care professionals. Interested persons had the opportunity to fill out a self-test on the project homepage (CSO in a third-party rating for the PA unwilling to enter treatment). The self-test consisted of the nine DSM-5 criteria of a gaming disorder 1 formulated as questions and should be answered on a 5-point Likert scale. Immediately after answering the questions, the interested persons received feedback if an Internet use behavior at-risk might be present and participation in the OASIS program was recommended. Once interested persons created a user account, agreed to the informed consent, and confirmed that they met the inclusion criteria (see above), they were able to book an appointment for the first telemedicine session. Before the first and after the second session participants were asked to fill out some questionnaires (see below) via the study portal. Six months after the last telemedicine session participants received a request via email, if the PA, CSO, and/or PA unwilling to enter treatment (reported by the CSO) entered the local health care system (see Figure 1).

Overview of the number of participants in the different steps of the OASIS study. Number of participants are listed separately for persons affected (PA) and concerned significant others (CSO).
For both groups of participants, the OASIS program consisted of two webcam-based sessions (60 minutes each; software: La-Well Systems GmbH) with their personal counselor. A detailed data protection concept was developed and implemented by the Competence Centre of Healthcare Telematics. Consultants were psychologists, psychiatrists, and experts in the field of counseling PA with IUD and CSO.
During the first telemedicine session, a detailed anamnesis of the Internet-, social- and family-history of the PA and two additional structured interviews to assess mental disorders and ensure exclusion criteria (M.I.N.I) and the presence of an IUD were carried out. In the group of CSO an estimation of the Internet use of the PA unwilling to enter treatment in a third-party rating based on the descriptions of the CSO took place and rules of positive communication (CRAFT; 22) were presented. In the second telemedicine session (approximately two weeks after the first session) increase in motivation for change among PA and communication training for CSO were focused as well as individual treatment options for PA, CSO, and/or the PA unwilling to enter treatment were presented and discussed (see Table 1).
Structured guidelines for the two online consultation sessions listed separately for person affected (PA) and concerned significant others (CSO).

The underlying manuals were developed separately for PA and CSO within the project. The manual for PA was created on the basis of MI- techniques 11 and the manual for CSO was on the basis of the CRAFT approach. 22 Both techniques are already established and validated techniques in the treatment of PA and CSO. The manuals were created by combining the above-mentioned established techniques with the comprehensive experience of the project management (senior physician of the outpatient clinic and expert in the field of treating PA and CSO).
Measures
Structured interviews
Internet use disorder
As basis for the self-developed guideline to diagnose an IUD the DSM-5 criteria for IGD 1 were used. An IUD was diagnosed if at least five of the nine DSM-5 criteria were present over a 12-month period. Hazardous Internet use was diagnosed if at least three criteria were met and subjectively burden Internet use if less than three criteria were present.
Mental disorders and comorbidities
M.I.N.I.—international neuropsychiatric interview
To verify the inclusion/exclusion criteria and identify mental disorders covered by DSM-IV and ICD-10 the structured diagnostic interview M.I.N.I. was used. 53 The M.I.N.I. covers different mental disorders (affective disorders, anxiety disorders, post-traumatic stress disorder, substance dependence, psychotic disorders, eating disorders, and suicidality).
ADHD screening
To determine if a suspicion of attention deficit hyperactivity disorder (ADHD) might exist the screening test V1.1 54 was conducted. Six questions were answered on a 5-point Likert scale from 1 “never” to 5 “very often.” If four of the six responses are in the pre-defined range (Questions 1–3: at least “sometimes” (3) selected; Questions 4–6: at least “often” (4) selected), it indicates a possible adult ADHD.
In addition to mental disorders covered by the M.I.N.I., ADHD is a frequent comorbidity of an IUD or GD. 55 Therefore, ADHD screening was conducted.
Questionnaires
Prior to the first online telemedicine consultation, participants completed online questionnaires regarding sociodemographic data, treatment history, and specific Internet use (CSO answered the questions for themselves as well as for the PA unwilling to enter treatment in a third-party rating).
After the second telemedicine consultation, participants answered questions about the technical implementation and evaluation of OASIS on a 5-point Likert scale and rated their satisfaction with the OASIS program on a scale from 1 "dissatisfied" to 10 "very satisfied."
Response transfer to local health care system
Six months after the second online consultation, participants were asked via email if the PA, CSO, and/or PA unwilling to enter treatment (reported by CSO) had entered the local health care system. Responses from participants were received via email and were assigned to one of the following categories: addiction counseling facilities, outpatient clinics, inpatient clinics, and others (see results section).
Statistical analysis
All analyses were conducted with IBM SPSS statistics for windows, version 26.0 and Microsoft Excel. Descriptive statistical analyses were calculated using percentages for categorical variables and means, standard deviation for continuous variables. One-way between-groups analysis of variance for continuous variables and Chi-squared tests for nominal variables with post-hoc comparison (Bonferroni) were conducted to compare the different groups.
Cramer's V was calculated for the Chi-squared test with V = 0.1 indicating small, V = 0.3 medium, and V = 0.5 large effects. 56
Eta-square was used as effect size indicator for the one-way between groups analysis with η2 = .01 indicating small, η2 = .06 moderate and η2 = .14 large effects and the effect size indicator f 2 was calculated for the binary regression analysis with f 2 = .02 indicating small, f 2 = .15 moderate and f 2 = .35 large effects. 57
Binary logistic regression was used to investigate the impact of the different variables on the likelihood that PA reaches the local health care system.
A post-hoc power analysis was performed for the binary logistic regression with G*Power V3.1.9.7.
57
With the effect size of Cox and Snell R2 = 0.358/Nagelkerkes R2 = 0.478 for the feedback regarding transfer to local health care system with n = 98 and the alpha error probability (
Ethics
The study was carried out in accordance with the Declaration of Helsinki. The Institutional Review Board approved the study (16-5734). All subjects were informed about the study procedure and all provided informed consent.
Results
Study participants
383 people created a user account (PA: n = 284, CSO: n = 99) and 187 participated in at least the first online consultation (PA: n = 140, CSO: n = 47). At the second online consultation, 107 PA and 38 CSO attended. Feedback after six months, if PA, CSO, and/or PA unwilling to enter treatment (reported by CSO) have entered the local health care system, was given by 50 PA and 18 CSO (see Figure 1).
After the second online consultation, participants (PA n = 67, CSO n = 30) answered questions about the technical implementation of and overall satisfaction with the OASIS program. The webcam-based conversation was perceived as comfortable by 93.1% (n = 62) of the PA and 96.7% (n = 29) of the CSO (PA: M = 4.54, SD = 0.77, Range = 1–5; CSO: M = 4.47, SD = 0.57, Range = 3–5). The overall satisfaction with the OASIS program was rated on average with 8.63 by PA (SD = 0.94, Range 6–10) and 8.27 by CSO (SD = 1.76, Range 2–10).
Table 2 shows sociodemographic data listed separately for PA, CSO, and PA unwilling to enter treatment (reported in a third-party rating by CSO) as well as treatment history and specific Internet use patterns including diagnosis of IUD for PA and assessment of Internet use for the PA unwilling to enter treatment based on the descriptions of the CSO.
Sociodemographic data, treatment history, specific Internet use, and diagnosis of Internet use disorder (IUD) and comorbidities listed separately for person affected (PA), concerned significant others (CSO), and PA unwilling to enter treatment (reported by the CSO in a third-party rating).

Note: aPA unwilling to enter treatment: suspicion, no diagnosis given; bn = 36; cPA: streaming (n = 8), online-shopping (n = 1), online-gambling (n = 1), general internet use (n = 6); PA unwilling to enter treatment: online-shopping (n = 1).
Specific internet use patterns
Differences in sociodemographic data, duration, and type of Internet use between the three groups (PA with IUD, hazardous -, subjectively burden Internet use) are listed in Table 3. The majority of participants were male throughout all three groups. Bonferroni-adjusted post hoc tests reveal that more women than expected based on the predicted values of the Chi2 test are in the hazardous Internet use group and fewer than expected based on the predicted values of the Chi2 test in the IUD group (vice versa for men).
Sociodemographic, comorbidities, treatment history listed separately for person affected (PA) with Internet use disorder (IUD), hazardous Internet use and subjectively burden Internet use.

Note: Bonferroni post-hoc: ap < .008, bp < .003. Printed in bold type: significant Bonferroni post-hoc test. cincluding multiple diagnosis; n = 2 no M.I.N.I. conducted.
As seen in Figure 2 in the IUD group 46% used the Internet to a pathological extent for playing online computer games and 35% for using pornography. In the group of hazardous Internet use, the Internet was used to a problematic extent for information search (29%), others (e.g. streaming, generalized Internet use; 27%), gaming (23%) and in the group of subjectively burden Internet use the most frequent applications which were indicated to use in a problematic extent was information search (30%; X2(8) = 31.117, p < .001, V = 0.381). Bonferroni-adjusted post-hoc tests reveal that online pornography occurs more frequently than expected based on the predicted values of the Chi2-test in the IUD group and information search less frequently than expected based on the predicted values of the Chi2-test.
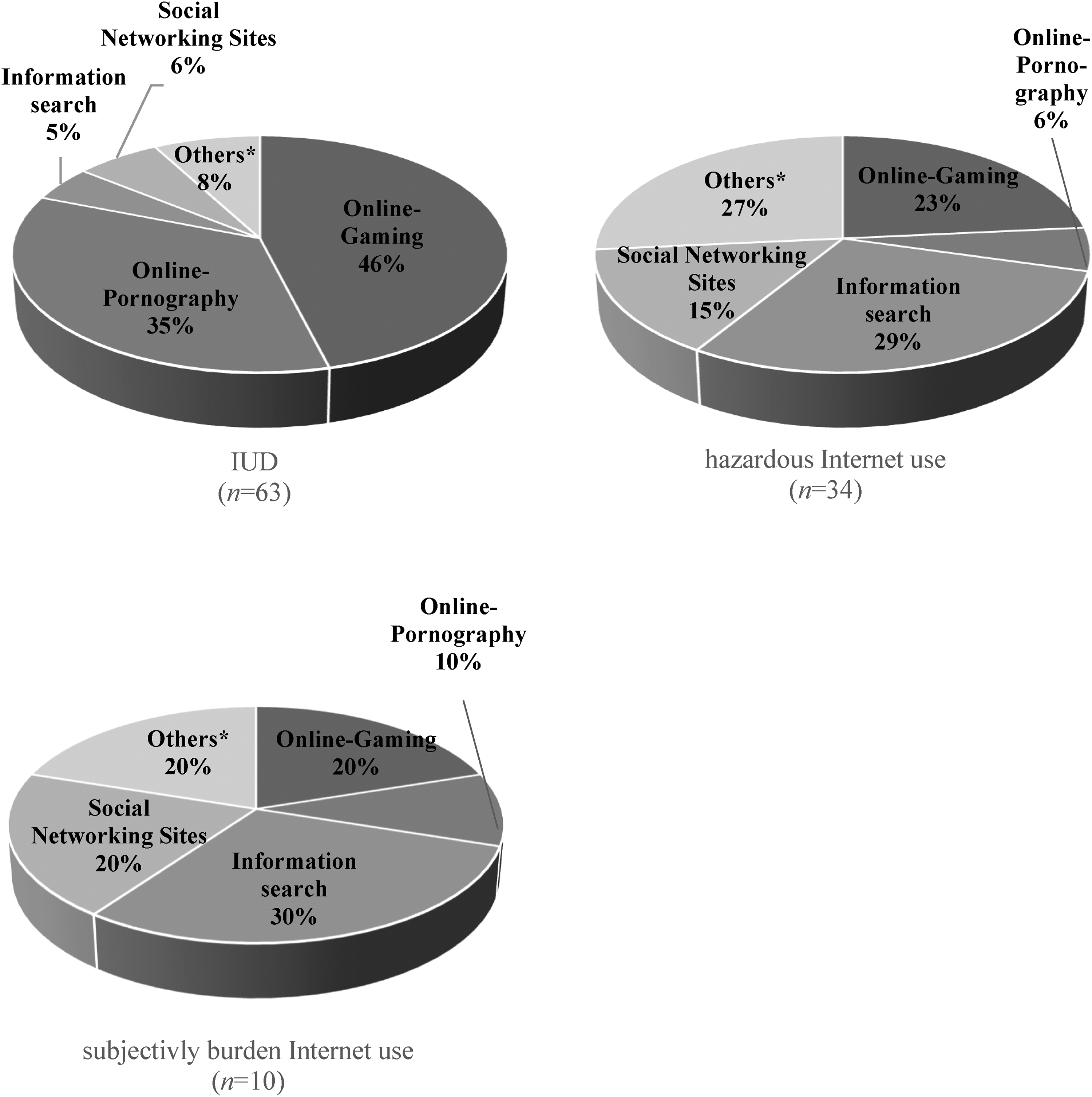
Specific Internet applications used to a problematic extent, listed separately for PA with Internet use disorder (IUD), hazardous internet use and subjectively burden Internet use. *IUD: streaming (n = 1), online-shopping (n = 1), online-gambling (n = 1), general Internet use (n = 2); hazardous Internet use: streaming (n = 6), general Internet use (n = 3); subjectively burden Internet use: general Internet use (n = 1), streaming (n = 1).
Referral to local health care system
Of the 107 PA (n = 38 CSO) who participated in the second online telemedicine session, 98 PA (n = 38 CSO) received recommendations for treatment options in the local health care system. In consultation with the respective consultant, nine participants decided to apply the strategies developed to reduce their Internet use during OASIS on their own. Half of the PA (51%, n = 50) and 47.4% (n = 18) of the CSO provided feedback after six months if they (or the PA unwilling to enter treatment (reported by CSO) in the group of CSO) have reached the local health care system after OASIS participation. In total, 43.9% (n = 43) of PA and 42.1% (n = 16) of CSO gave feedback that they had at least a first appointment for further treatment in the local health care system. In the group of CSO, nine of the 16 CSO gave the feedback that the PA unwilling to enter treatment (reported by CSO) reached the local health care system, in four cases the CSO and in three cases the PA unwilling to enter treatment (reported by CSO) and CSO reached the local health care system. When the affiliation of the telemedicine consultation was the same as for treatment in the local health care system, 92.3% (n = 12) of PA and 100% (n = 2) of CSO and PA unwilling to enter treatment (reported by CSO) arrived (see Figure 3).

Response rate of reaching the local health care system reported separately for person affected (PA) and concerned significant others (CSO)/PA unwilling to enter treatment (reported by CSO) in relation to treatment recommendation nationwide and the study location as a treatment recommendation.
Table 4 shows what type of treatment PA, CSO and/or PA unwilling to enter treatment reached in the local health care system. The majority of PA reached outpatient settings (62.8%) followed by addiction counseling facilities (23.3%) in the local health care system and the majority of CSO reached addiction counseling facilities (71.4%) followed by outpatient clinics (28.6%).
Type of treatment in the local health care system separately listed for person affected (PA), Concerned Significant Others (CSO), and PA unwilling to enter treatment (reported by the CSO).

Note: an = 3 CSO and PA unwilling to enter treatment in treatment; bn = 1 psychotherapy because of another mental disorder; n = 1 ADHD diagnostic; n = 1 autism diagnostic; cn = 1 autism diagnostic; dn = 1 mindfullness class; eOASIS participation.
A binary logistic regression was performed to assess the predictive value of the different independent variables on the referral rate (see Table 5). The entire model was statistically significant (X2(18) = 36.94, p = .005, n = 98) and explained between 31.4% (Cox and Snell's R2) and 42.1% (Nagelkerke's R2) of the variance of the referral-rate and classified 76.5% of the cases correctly with an effect size of f 2 = .724. As seen in Table 5 the independent variable treatment recommendation “study location” was significant. This means that the chance of being placed in analog help services is about 19 times higher when the recommended treatment location is the same where the telemedicine intervention took place.
Binary logistic regression for the likelihood of transfer to local health care system for person affected (PA).
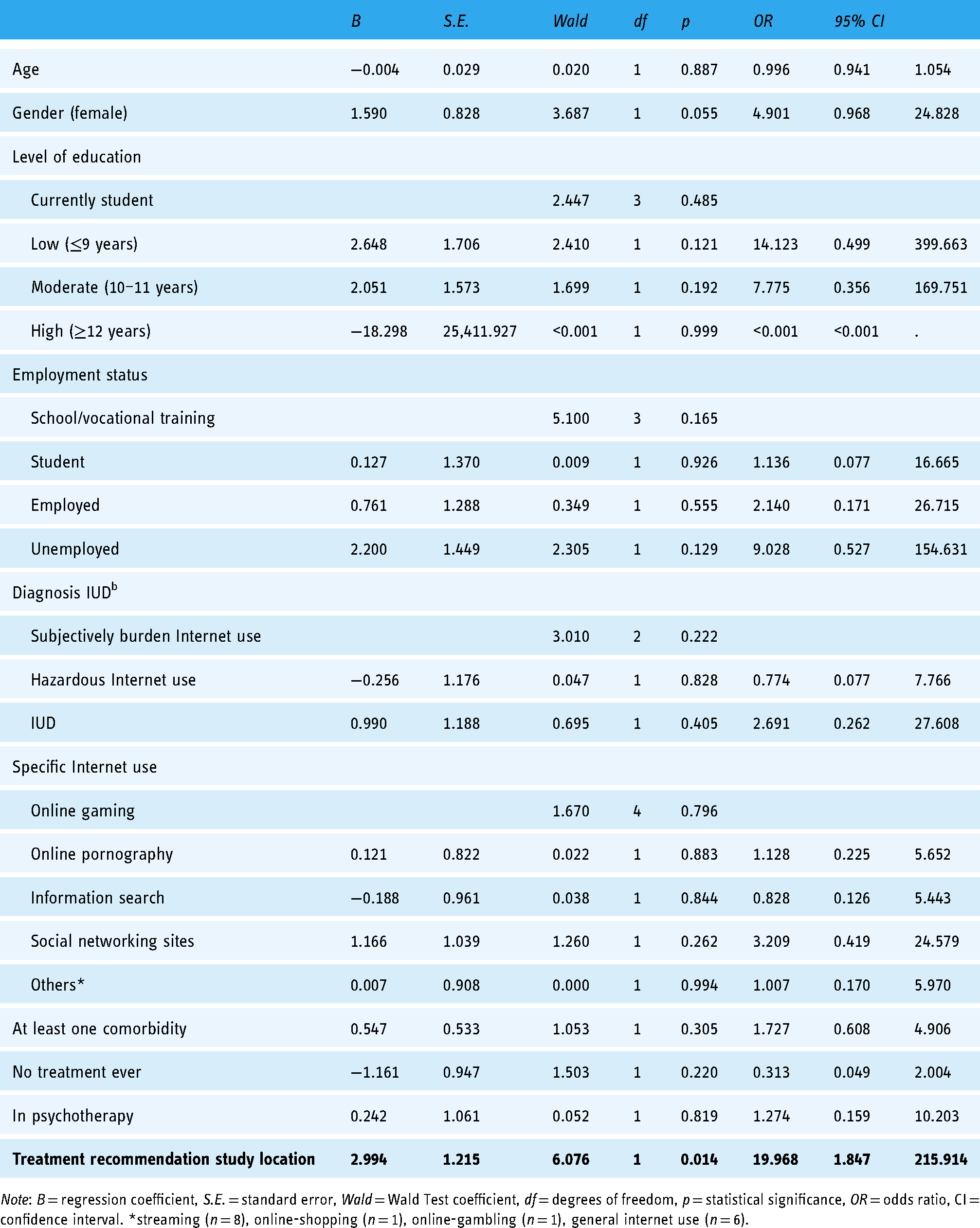
Note: B = regression coefficient, S.E. = standard error, Wald = Wald Test coefficient, df = degrees of freedom, p = statistical significance, OR = odds ratio, CI = confidence interval. *streaming (n = 8), online-shopping (n = 1), online-gambling (n = 1), general internet use (n = 6).
Discussion
To date, this is the first telemedicine webcam-based counseling service for PA with problematic Internet use and CSO with the aim of transferring the participants to the local health care system. Other telemedicine services for PA with problematic Internet use are primarily defined by pre-designed modules that individuals complete independently with the primary aim of symptom reduction.39,42 A randomized controlled trial to evaluate the efficacy of four-week webcam-based one-to-one counseling for individuals with IUD was initiated by our research group and is ongoing. 43 To the best of our knowledge, no telemedicine services specifically for CSO of PA with IUD (not preventive programs) have been published so far.
The main result of this study is that a referral to the local health care system through a short-term telemedicine consultation was successful for more than 40% of the participants. More than 90% of the PA and CSO arrived in the local health care system when there was an affiliation between telemedicine intervention and the local treatment institution. Regardless of sociodemographic characteristics and/or symptom severity, the affiliation of the telemedicine consultation and the local health care system as well as the smooth and simplified transition to the local health care system seem to be crucial factors for the effectiveness of the referral.
Other important findings are that OASIS was used primarily by individuals who had not yet entered the health care system (majority of participants not in treatment) and a high proportion of PA with pathological Internet pornography use in comparison to traditional treatment settings 30 utilized the program. The assumption that telemedicine intervention may be particularly attractive to women with IUD could not be confirmed.
The results found in this study are in line with systematic reviews which have already shown that MI techniques support motivation to change and treatment adherence across different disorders19,20 and that online MI-based interactive messages had significant effects on treatment initiation for individuals at risk for gambling disorder and substance use.58–61 Therefore, a validation of the promising results found in this study seems to be appropriate.
A systematic review of the CRAFT approach for CSO of individuals with drug, alcohol, and gambling abuse showed the effectiveness of the method, 62 but to our knowledge, to date there are no studies published which have used the CRAFT approach to support CSO of PA with IUD. Comparable to the results found in this study, the majority of CSO in other studies are female and the majority of PA unwilling to enter treatment (reported by CSO) are male. 62 Compared to the results of CRAFT for CSO of gambling abusers (4 × workbook: 13.3–23%, 1 × individual: 12.5%), the referral rates of the OASIS study are higher with 31.6% for PA unwilling to enter treatment (reported by CSO) and 18.4% for CSO.
The results support the success of (online-based) MI- and CRAFT-interventions regarding the referral of PA, CSO, and PA unwilling to enter treatment (reported by CSO) to the local health care system. Due to the different disorders and types of interventions, further studies are necessary to classify and verify the results found in this study.
Since the majority of participants were not in treatment before participating in OASIS, the aim of creating a low-threshold counseling service for PA and CSO who have not yet reached the local health care system could be achieved. Comparable to clinical as well as telemedicine samples of PA with IUD, the group of OASIS participants is defined by primarily male participants with advanced education and an unemployment rate between 15–23%.16,17,63,64 Although epidemiological studies show that women are affected with IUD at the same rate as men,14,15 the majority of treatment-seekers are male,16,17 which is in line with the composition of the OASIS sample. Most of the female OASIS participants were in the group of hazardous Internet users. Based on initial studies, one possible explanation could be that women enter the health care system through other primary diagnoses, although an IUD is present. 65 Comparable to epidemiological studies, women primarily used the Internet for social networking sites and information searches, whereas men primarily used online computer games and online pornography to a pathological extent. In clinical as well as epidemiological studies, GD is the most common type of IUD.14,16,17 In the course of OASIS, the number of men with GD is comparable to the number of men with pathological online pornography use. Possible reasons for the high amount of participants with pathological online pornography use may be the shame-associated subject and that a low-threshold telemedicine program reduces barriers to seeking support and/or that there are only a few specific treatment options. 66 Unlike clinical and other telemedicine settings,16,17,39 OASIS participants are on average eight years older (mean age 34 years). Previous studies indicate a younger average age across the different types of an IUD,16,65,66 which may assume that a telemedicine intervention addresses in mean older PA with IUD than the traditional health care system.
Limitations
To verify the validity of the results of the study, it would be important to use a randomized controlled study design with equal sample sizes in the groups “treatment recommendation study location” versus “nationwide“ with follow-up measurements. Since the diagnosis of an IUD was made based on a self-developed guideline following the DSM-5 criteria for GD, 1 future studies should use already established and validated structured interviews for the diagnosis of an IUD. The results show that mainly male participants took part in the OASIS study, therefore it is only possible to outline initial tendencies of female affected individuals but no conclusions are feasible. Since epidemiological studies indicate that men and women are affected at the same rate,14,15 particular attention should be paid on how to reach affected women more effectively. There were high dropout rates during the course of the study. The rates are comparable to reported dropout rates of 23–50% in addiction treatment, 67 yet more attention should be paid to reducing dropout rates in future studies. To strengthen the commitment of the participants, brief contacts via webcam at the follow-up measurement and/or to obtain consent from participants that they are contacted via telephone (and not only via email), could be helpful.
Conclusion
To the best of our knowledge, this is the first study to investigate the effectiveness of a webcam-based short-term counseling service for PA and CSO with the aim of referral to the local health care system. Due to the increasing acceptance and use of telemedicine services in the health care sector, the results found are of particular relevance. Therefore, it is important to verify the efficacy of such telemedicine counseling services in randomized controlled study designs. If the efficacy of the telemedicine service can be replicated, the integration of such telemedicine services into existing care structures could be a promising next step.
Footnotes
Acknowledgments
We acknowledge support by the Open Access Publication Funds of the Ruhr-University Bochum. Our thanks go to the German Federal Ministry of Health for sponsoring the study and to the cooperation partners Centre for Telematics and Telemedicine (ZTG) GmbH and the German Fachverband Medienabhängigkeit e.V.
Contributorship
LB conducted literature research, created manuscript concept, ran the statistical analysis, interpreted the results and wrote the manuscript. JDH contributed to the manuscript concept and refinements. BTW conceived the study and acquired funding. LB, BTW and JDH conducted and coordinated the study. JDH, BTW, MB, SH, MP contributed to the style of reporting and writing and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Open Access Publication Funds of the Ruhr-University Bochum and the OASIS project was funded by the German Federal Ministry of Health under grant number ZMVI1-2516DSM207.
Ethical approval
The study was carried out in accordance with the Declaration of Helsinki. The Institutional Review Board approved the study (Nr. 16-5734). All subjects were informed about the study and all provided informed consent.
Guarantor
LB.