
Abstract
Case summary An 8-year-old, male neutered domestic shorthair cat was presented with acute onset of ataxia, apathy, hypersalivation and anorexia. Clinical examination revealed a swollen, bluish tongue tip, neurological deficits, hypothermia, hypotension and a left-sided systolic heart murmur with arrhythmia. Blood pressure was initially low but normalised after dobutamine therapy. Thoracic radiographs revealed cardiomegaly, and echocardiography confirmed a hypertrophic cardiomyopathy (HCM) phenotype with severe left atrial dilation, spontaneous echo contrast and suspected thrombus formation. MRI of the head showed absent contrast enhancement in the rostral two-thirds of the tongue and signal changes consistent with lingual infarction. Doppler ultrasound confirmed absent blood flow in the affected tongue region. Based on imaging, cardiac findings and clinical signs, a lingual artery thromboembolism was considered the most likely diagnosis. The patient was treated with anticoagulant therapy and supportive care, but because of worsening tongue swelling, functional impairment and underlying advanced heart disease, euthanasia was elected.
Relevance and novel information To the authors’ knowledge, this case represents the first reported case of feline arterial thromboembolism affecting the lingual artery. Although HCM was the presumed cause, other thromboembolic risk factors, such as hyperthyroidism, could not be definitively excluded. This case emphasises the need to consider atypical thromboembolic presentations in cats with cardiac disease and highlights the diagnostic value of advanced imaging modalities in identifying uncommon sites of arterial obstruction.
Plain language summary
An 8-year-old, male neutered domestic shorthair cat was examined because of a sudden onset of poor coordination, lethargy, excessive drooling and refusal to eat. On clinical examination, the tip of the tongue was swollen and blue in colour, suggesting poor blood supply. The cat also had low body temperature, low blood pressure, abnormal heart rhythm and a heart murmur. Imaging of the chest and heart showed severe heart disease consistent with hypertrophic cardiomyopathy, including marked enlargement of the left atrium and changes suggesting an increased risk of blood clot formation. Advanced imaging of the head demonstrated a lack of blood supply to the front portion of the tongue, consistent with tissue death (infarction). Doppler ultrasound confirmed the absence of blood flow to the affected area of the tongue. Based on the clinical signs, imaging findings and underlying heart disease, a blood clot blocking the lingual artery was considered the most likely cause of the tongue infarction. Despite treatment with anticoagulant medication and supportive care, the tongue swelling progressed, leading to severe functional impairment. Given the poor prognosis associated with both the tongue injury and the advanced heart disease, euthanasia was elected. This case is the first reported instance of an arterial thromboembolism affecting the lingual artery in a cat. It highlights that blood clots in cats with heart disease can affect unusual locations and demonstrates the importance of advanced imaging techniques in identifying uncommon sites of arterial obstruction.
Keywords
Case description
History
An 8-year-old, male neutered domestic shorthair cat was presented to the emergency service with an acute onset of staggering gait, apathy and anorexia, beginning a couple of hours before presentation. Intoxication could not be ruled out as the cat had free access to the outside and was known to prey on mice. According to the owners, there were no known pre-existing conditions and the cat was fed a commercial diet.
Clinical presentation
On initial presentation, the cat showed pronounced hypersalivation and a swollen, bluish discoloured tip of the tongue with an inability to fully retract the tongue into the oral cavity (Figure 1). The general physical examination showed tachypnoea of 88 breaths/min, hypothermia with 37.1°C and a heart rate of 196 beats/min. Auscultation revealed a left apical systolic heart murmur (grade III/VI) and arrhythmia detectable on both auscultation and pulse assessment at the femoral artery. Pulse was weak, but clearly palpable in both hindlimbs. To ensure the patient’s comfort, analgesia with buprenorphine 0.01 mg/kg IV q8h was given. 1 Complete neurological examination, performed after administration of opioids, showed mild ataxia, bilateral reduced vision with mydriasis, bilateral absent menace response and absent pupillary light reflex, both direct and indirect. The remaining cranial nerve functions were physiological and swallowing reflex was present. Postural reactions, spinal reflexes and nociception were within normal limits. The complete neurological examination is provided as Table S1 in the supplementary material. Fundoscopic examination revealed no abnormalities.
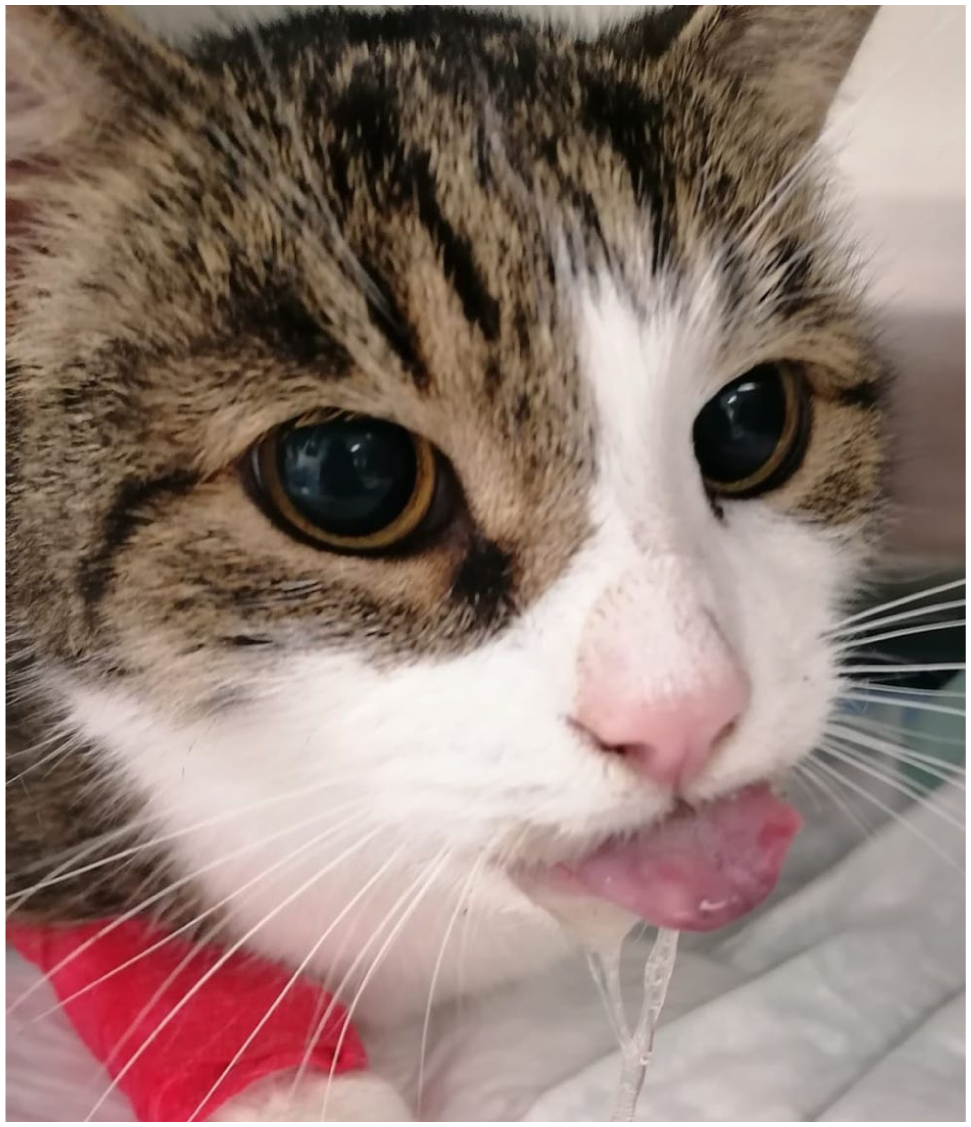
Photograph of the cat at presentation with bluish discoloration and swelling of the tongue. In addition, the described bilateral mydriasis can be seen
Initial systolic blood pressure (BP), measured by Doppler method on one forelimb, was 60 mmHg.
Cardiac focused point-of-care ultrasound (TE5 Vet; Mindray) revealed severe dilatation of the left atrium (LA) and auricle with spontaneous echo contrast. The ratio of the LA to the aorta (Ao) measured 2.6 (two-dimensional short axis). The left free wall showed marked thickening. A three-lead electrocardiogram (ECG) was attached to the cat for continuous ECG monitoring at the intensive care unit and showed various premature complexes with both narrow and broad morphology. Thoracic radiographs showed an enlarged cardiac silhouette and a mild interstitial lung pattern. As a local irritation with a toxic substance was initially considered, the tongue and the oral cavity were rinsed with diluted chlorhexidine gluconate. Treatment with dobutamine (2.5 μg/kg/min) constant rate infusion (CRI) was started to improve cardiac output and therefore BP. 2 Constant ECG monitoring was used to check for worsening arrhythmia. After initial stabilisation, comparative BP of all four limbs was performed to rule out feline arterial thromboembolism (ATE) of the hindlimb as a cause for the ataxia, which showed comparable results in all four limbs (forelimbs: left/right 140/135 mmHg, hindlimbs: left/right 150/140 mmHg).
Blood gas analysis revealed mild metabolic acidosis; electrolyte concentrations were within reference intervals (RIs). Subsequent laboratory results showed increased creatine kinase at 5288 U/l (RI <205) and mild, clinically non-relevant derangements (Table S2 in the supplementary material). Serum amyloid A was mildly elevated at 9 µg/ml (RI <3.9).
After BP increased (140 mmHg), dobutamine CRI was discontinued. Based on the findings on echocardiographic point-of-care ultrasound, anticoagulant therapy was started with enoxaparin (1 mg/kg SC), which was changed approximately 8 h later to a CRI (3 mg/kg/day). 3
Complete echocardiography (Philips IE33; Philips Healthcare) was carried out 11 h after presentation. Hypertrophic cardiomyopathy (HCM) phenotype was diagnosed with severe dilatation of the LA (LAmax 24 mm, RI 12.66–18.78, 4 LA:Ao 2.73, RI 1.01–1.39 5 ) (Figure 2) and left auricle, with spontaneous echo contrast and suspected thrombus formation. The left free wall (LVFWd) was severely thickened, measured in diastole (11 mm, RI 3.56–5.79 4 ) (Figure 3). The fractional shortening was within normal limits (49%, RI 42–64 5 ). LA and Ao diameters were assessed in end-diastole using a two-dimensional echocardiographic approach from the right parasternal short-axis view and LA:Ao ratio subsequently calculated. The LAmax was obtained in end-systole from the interatrial septum to the lateral wall of the LA in the right parasternal four-chamber view. LVFWd was measured using the two-dimensional-guided M-mode, and the left ventricular shortening fraction was calculated using the standard M-mode method from a right parasternal short-axis view at the level of the papillary muscles. All measurements were performed by a board-certified veterinary cardiologist. 6 ECG at this time point showed sinus rhythm with occasional isolated premature beats with narrow or broad morphology.
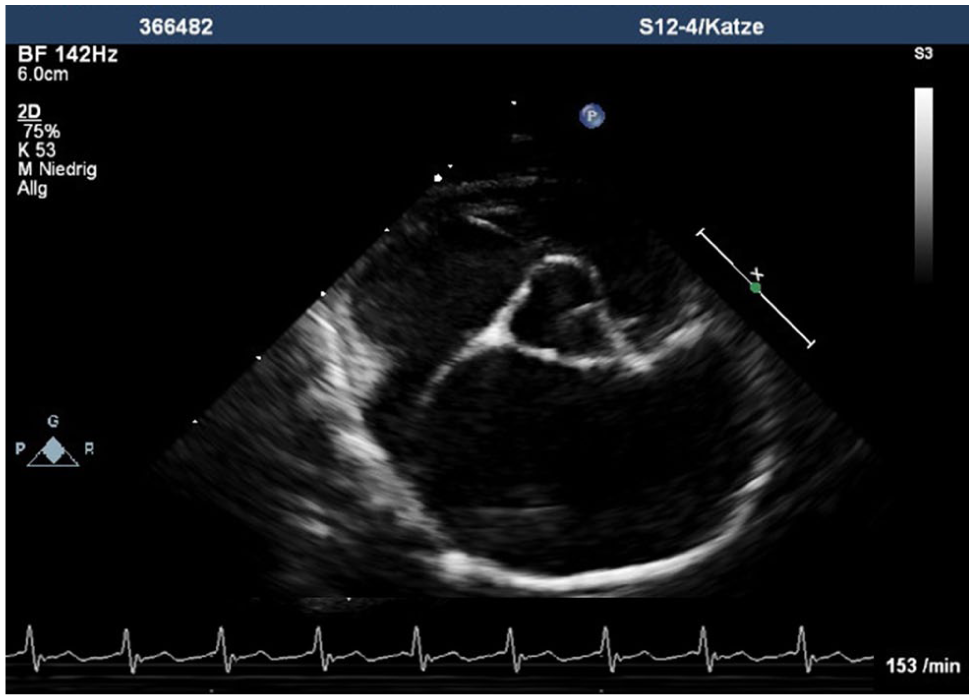
Echocardiographic right parasternal short-axis view of the heart base shows severely enlarged left atrium and left auricle

Echocardiographic four-chamber view from the right parasternal long axis revealed an enlarged left atrium and marked thickening of the left free wall
MRI of the head, using a 3 T MRI scanner (Magnetom Verio 3 Tesla; Siemens Healthcare), was performed, including T2-weighted, T2-weighted fluid-attenuated inversion recovery (T2-FLAIR), diffusion-weighted imaging and susceptibility weighted imaging (SWI), as well as T1-weighted three-dimensional before and after IV administration of gadolinium-chelated contrast agent images. MRI revealed a diffuse, hyperintense signal of the tongue in T2-weighted and T2-FLAIR sequences. An abrupt fading of contrast uptake of the rostral two-thirds of the tongue was noted (Figure 4). The lack of contrast enhancement of the tongue indicates a lack of perfusion to the tongue, likely due to thromboembolism in the vascular bed of the tongue. MRI was performed under general anaesthesia, with monitoring of end-tidal CO2, SpO2, BP and heart rate. The increased risk of anaesthesia was discussed with the owner, who decided to proceed to further investigate the acute neurological signs and provide prognostic information.

T1-weighted MRI sequence and sagittal view of the head, showing contrast uptake of the base of the tongue (*) and no uptake of the rostral part (white arrow)
At the level of the left choroid plexus in the fourth ventricle, SWI showed two roundish susceptibility artefacts. These findings suggest a small haemorrhage in the choroid plexus in the fourth ventricle on the left side. No other pathological findings of the brain or suspicion for thrombus within the brain could be detected.
Colour flow Doppler assessment via ultrasound (Canon Aplio a450; Canon Medical Systems) showed blood flow in the base of the tongue, but no flow detectable in the rostral parts.
Tongue swelling progressed within 12 h of presentation, and the cat developed an inability to swallow (Figure 5). Although ataxia resolved during hospitalisation, blindness persisted throughout.

Presentation of the cat’s tongue approximately 12 h after presentation. The tongue is notably hanging from the oral cavity and bluish discoloration of its most proximal part can be clearly recognised
As a result of the progression and the cautious prognosis of tongue preservation and functionality, and the advanced heart disease, the owners elected euthanasia approximately 17 h after presentation.
Discussion
The cat in our report presented with an acute onset of unspecific neurological signs and pain. Upon clinical examination, the most striking finding was the swollen tongue with a bluish discoloration, which was progressive. The cat showed slight improvement of his general condition after stabilisation of the cardiovascular and blood pressure status. Further investigations showed an absent blood circulation to the cranial tongue and severe dilatation of the LA, leading to the most likely diagnosis of lingual infarction with a thromboembolic event secondary to HCM.
Feline ATE is a serious and painful condition in cats, in most cases characterised by the sudden onset of ischemic necrosis in one or more limbs, causing severe pain, paralysis, absent pulse and coldness in the affected limbs.7,8 This condition is most commonly triggered by thrombus formation in a severely enlarged LA or left auricle and its dislodgment to circulation.7–10 The thrombus travels through the bloodstream and lodges in a peripheral artery, obstructing blood flow and leading to tissue ischemia. 9 ATE is a frequent and often fatal complication of cardiomyopathies in cats, with a high rate of euthanasia at presentation 11 and reported survival rates in the range of 29–45%.11–15 Although HCM is the most common cause of ATE in cats, other conditions such as hyperthyroidism, pulmonary neoplasia and systemic inflammatory reactions can also contribute to thrombus formation.9,14
Feline ATE most commonly lodges at the aortic trifurcation.7,14 Other locations of thromboembolism, including the brachial, mesenteric, coronary, renal, subclavian or cerebral arteries, have been reported.14,16–18 Clinical signs observed in these cases included severe pain, vocalisation, myocardial infarction, intestinal ischemia or infarction, abdominal pain, vomiting and neurological signs, such as circling, head tilt, hemiparesis, seizures, sudden blindness or other focal neurological deficits.7,9,11,14
To the authors’ knowledge, no case of lingual infarction secondary to ATE has been described in the veterinary literature to date. Even among human patients, ATE affecting the tongue is rare, with the medical literature including only a few cases of thrombus in the oral cavity. 19 Cardiac causes, such as atrial fibrillation, have been described in human medicine. 20
Both CT and MRI are valuable modalities for detecting ATE.21–24 In this case, MRI was selected because of the presence of neurological signs, as it is superior for identifying ischemic and structural changes within the brain compared to CT. Several studies have shown that MRI is an effective tool for detecting thromboembolism, providing good accuracy and detail through its ability to generate detailed images of arteries.21,22
For a definitive diagnosis, a post-mortem examination would have been necessary, which was declined by the owners. However, the MRI findings in combination with the diagnosed heart disease, and the absence of evidence of other causes, support the probable diagnosis of ATE affecting the arteries of the tongue due to underlying HCM. Nutritional deficiencies were unlikely, as a commercial diet was fed, and no other clinical findings were suggestive of thiamine deficiency. Other diseases that might cause hypercoagulable states and thromboembolism, such as hyperthyroidism,25,26 cannot be definitively excluded, as total thyroxine was not measured. This was because measurement required an external laboratory, and the cat was euthanased before sample submission and insufficient serum remained after euthanasia. This represents a limitation of this case. Nevertheless, pathophysiology behind thrombus formation in hyperthyroidism is also multifactorial and the diagnosed cardiac disease would still be likely to play a major role in the formation of the ATE in this cat. 14 No evidence of pulmonary neoplasia or significant systemic inflammation was present. The increase in creatine kinase was considered secondary to the ischemic injury of the tongue; however, a transient ATE affecting the limbs cannot be excluded. Based on the neurological examination, there was no suspicion of a generalised myopathy.
Not all mentioned clinical signs, including ataxia, bilateral blindness with mydriasis, bilateral absent menace response and absent pupillary light reflex, can be explained by the findings of the lingual thromboembolism. The change in vision and mydriasis might be partly explained with the given opioids, which were administered before the complete neurological examination and are known to cause mydriasis in cats, possibly impairing their vision. 1 The mild ataxia noted on initial examination may have been secondary to systemic hypotension and generalised weakness at presentation rather than indicating a primary neurological disorder. As the tongue was the primary concern of this cat, no further investigation into the cause of the neurological signs was conducted.
Conclusions
This case presents a lingual artery thromboembolism in a cat, representing an unusual and previously undescribed localisation of ATE caused by HCM. Although the clinical and diagnostic imaging findings support this aetiology, alternative causes, such as hyperthyroidism, cannot be definitively ruled out, although this is less likely.
In summary, this case highlights the need for vigilance in identifying atypical thromboembolic sites in cats with cardiac disease and demonstrates the significance of advanced imaging and cardiovascular evaluation in such complex presentations.
Supplemental Material
sj-docx-1-jor-10.1177_20551169261433274 – Supplemental material for Tongue infarction in suspected lingual artery thromboembolism in a cat with hypertrophic cardiomyopathy
Supplemental material, sj-docx-1-jor-10.1177_20551169261433274 for Tongue infarction in suspected lingual artery thromboembolism in a cat with hypertrophic cardiomyopathy by Fabienne Blunschi, Jackie Riwers, Tereza Jaresova, Julia Ortlieb, Sebastian Schaub, Claudia Vollmar, Esther Hassdenteufel and Matthias Schneider in Journal of Feline Medicine and Surgery Open Reports
Supplemental Material
sj-docx-2-jor-10.1177_20551169261433274 – Supplemental material for Tongue infarction in suspected lingual artery thromboembolism in a cat with hypertrophic cardiomyopathy
Supplemental material, sj-docx-2-jor-10.1177_20551169261433274 for Tongue infarction in suspected lingual artery thromboembolism in a cat with hypertrophic cardiomyopathy by Fabienne Blunschi, Jackie Riwers, Tereza Jaresova, Julia Ortlieb, Sebastian Schaub, Claudia Vollmar, Esther Hassdenteufel and Matthias Schneider in Journal of Feline Medicine and Surgery Open Reports
Footnotes
Author note
This case report was presented at the 21st European College of Veterinary Emergency and Critical Care Congress, Gothenburg, Sweden, 30 May – 1 June 2024.
Supplementary material
The following files are available as supplementary material:
Table S1: Results of the neurological examination performed.
Table S2: Original laboratory report including serum biochemistry profile and haematology [in German].
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). For any animals or humans individually identifiable within this publication, informed consent (either verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.