
Abstract
Case summary
A 4-year-old castrated male Sphynx presented for evaluation of a heart murmur and was diagnosed with subclinical hypertrophic cardiomyopathy characterized by a primarily apical distribution of left ventricular (LV) wall thickening. Over the course of four sequential follow-ups, progressive LV apical hypertrophy and left atrial dilation developed. Despite medical therapy with clopidogrel and pimobendan, the cat developed congestive heart failure and was euthanized 32 months after echocardiographic diagnosis. No post-mortem examination was performed.
Relevance and novel information
Although feline hypertrophic cardiomyopathy (HCM) is common and the pattern of distribution of LV hypertrophy is heterogeneous, this is the first case report of apical HCM in cats. Data from the human literature are extrapolated to make the diagnosis and discuss potential negative prognostic indicators of this condition in cats.
Introduction
Hypertrophic cardiomyopathy (HCM) is the most common phenotype of myocardial disease in the cat. It has been reported to affect approximately 15% of all cats, and up to 29% of cats aged over 9 years in one rehoming center in the UK. 1 Symmetrical (affecting the interventricular septum [IVS] and the left ventricular free wall [LVFW] in similar proportions) and asymmetrical patterns of left ventricular hypertrophy (LVH) (confined to either the IVS or the LVFW) have been reported in cats with HCM.2–4 A diagnosis of HCM may carry significant implications with a predicted cardiac mortality rate (due to congestive heart failure [CHF], thromboembolism or sudden death) of approximately 7%, 23% and 29% at 1 year, 5 years and 10 years after diagnosis, respectively. 5 We identified a unique phenotypic presentation of primarily apical LVH in a cat.
Case description
A 4-year-old castrated male Sphynx cat weighing 3.9 kg was presented to The Ohio State University Veterinary Teaching Hospital for evaluation of a heart murmur (grade II/VI left parasternal holosystolic). The cat was diagnosed with an HCM phenotype 6 characterized by hypertrophy primarily affecting the left ventricular (LV) apex with normal thickness of the basilar aspects (upper third) of the IVS and LVFW. The left atrium (LA) was mildly enlarged. The cat’s heart murmur was primarily attributed to mild dynamic right ventricular outflow tract obstruction, and there was concurrent mild mitral regurgitation. The former is a frequent, benign finding in cats. 7 Mitral valve abnormalities are common in cats with HCM, 8 and no other defining features of mitral valve dysplasia were identified. No cardiac medications were initiated at this time.
On a subsequent recheck 14 months after the initial echocardiogram, the previously described distribution of relative wall thicknesses was again noted. There was also progressive dilation of the LA with mildly reduced left auricular flow velocity. Because of concerns over increased risk of systemic thromboembolic complications, clopidogrel (18.75 mg PO q24h) was prescribed.
The cat continued to undergo routine rechecks that revealed progressive LV apical concentric hypertrophy, generalized LV eccentric hypertrophy and LA dilation (Figures 1–3 and Videos 1–5 in the supplementary material). Mitral regurgitation, although mild, was progressive and attributed to mitral valve annular stretch associated with diastolic dysfunction and LV volume overload. Maximal apical-to-free wall thickness surpassed cutoffs of apical HCM established in humans, 9 as did the apical cavity obliteration ratio. The latter was assessed as the ratio of the end-systolic length of apical obliteration to end-systolic height of the LV cavity, as previously described. 10 Left atrial shortening fraction and left auricular flow velocity continued to decline, and spontaneous echocardiographic contrast became appreciable within the lumen of these structures. One ventricular premature complex was noted on a single-lead electrocardiogram (ECG) during echocardiography 21 months after initial presentation and again at 25 months after the initial diagnosis. Pimobendan (1.25 mg PO q12h) was prescribed because of progressive reduction in LA function with the goal of improving left atrial transport function.11,12 Table 1 summarizes LV echocardiographic indices over the course of five studies.6,9,10 Table 2 summarizes additional echocardiographic indices of LA size and LV/LA function.13–17
Right parasternal long-axis four-chamber view. Severe left atrial (LA) enlargement is demonstrated. Location of the end-diastolic wall thickness measurements are labelled (*). The left ventricular (LV) apical wall is disproportionately hypertrophied (10.09 mm) while the upper third of the LV has normal wall thickness (interventricular septum 2.67 mm, LV free wall 4.46 mm)

Right parasternal short-axis view. End-diastolic left ventricular (LV) wall thickness measurements (*) are within the reference interval of <5 mm (interventricular septum 4.90 mm, LV free wall 4.40 mm)

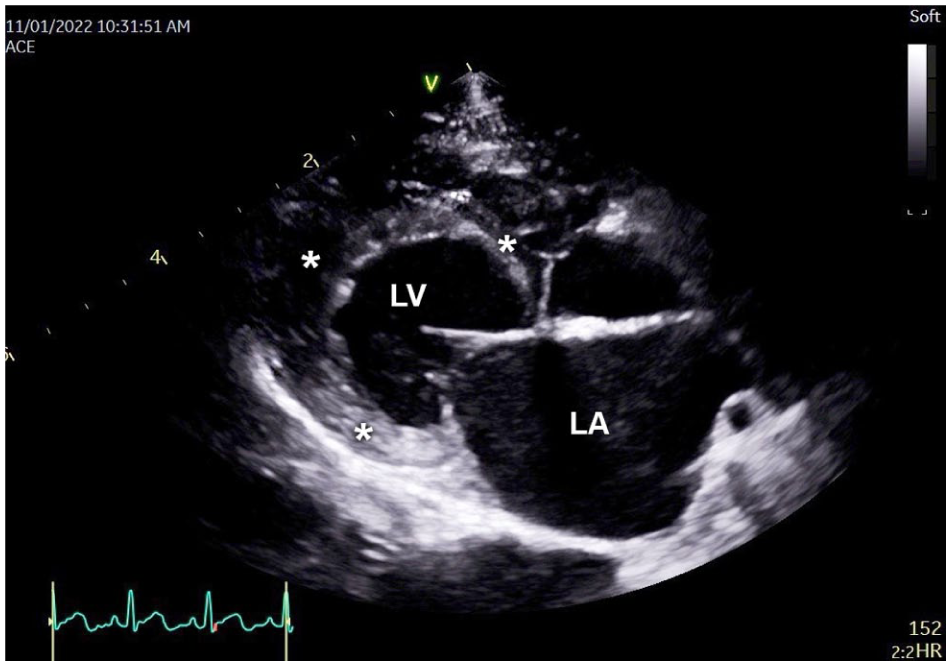
Left apical long-axis four-chamber view. Severe left atrial (LA) enlargement is demonstrated. Location of the end-diastolic wall thickness measurements are labelled (*). The left ventricular (LV) apical myocardium is disproportionately hypertrophied (10.53 mm) compared with the other LV wall segments (interventricular septum 3.90 mm, LV free wall 3.50 mm)
Indices of left ventricular (LV) wall thickness from five subsequent echocardiographic studies over a period of 29 months
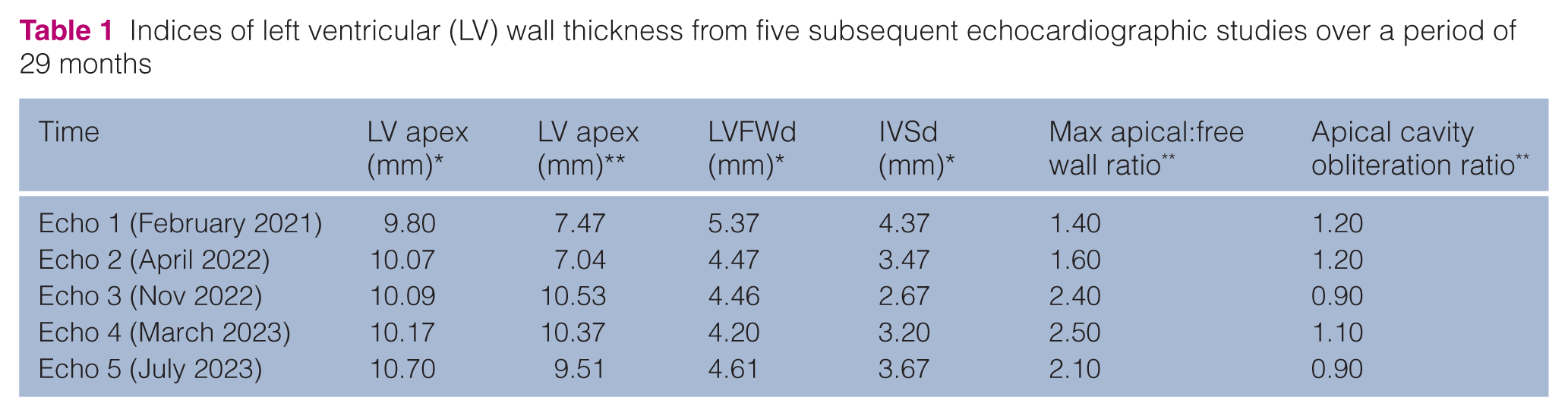
LV wall thickness was measured at end-diastole (d) using the first frame after mitral valve closure at the level of the tips of the open mitral valve leaflets. A cutoff of ⩾6 mm wall thickness of any segment at end-diastole was used to unequivocally define LV concentric hypertrophy per the American College of Veterinary Internal Medicine consensus statement on feline cardiomyopathy. 6 Maximum apical LV wall thickness was measured from the blood–tissue interface at the LV apex to the leading edge of the apical compacted myocardium–pericardial interface using right parasternal long-axis four-chamber (*) and left apical long-axis four-chamber images (**). Measurements of the interventricular septum (IVS) were made using the leading-edge-to-trailing-edge technique, while measurements of the left ventricular free wall (LVFW) were made using the leading-edge-to-leading-edge technique. The ratio of maximal apical to LVFW thickness was obtained as previously described by Eriksson et al. 9 The apical cavity obliteration ratio was obtained from measurements using left apical four-chamber (**) images at end-systole as previously described by Kim et al 10
Indices of left atrial (LA) size, left ventricular (LV) and LA systolic function, and LV diastolic function from five subsequent echocardiographic studies over a period of 29 months

Measurements are compared with established normals13–15 and breed-specific reference intervals (RIs) where available. 16 Maximal LA (LAD max) and LA fractional shortening (FS) were obtained from two-dimensional right parasternal long-axis four-chamber images. The LAD max was measured at end-systole in the last frame before mitral valve opening (diagnostic cutoff of >16 mm used to define LA enlargement),13,14 while LA FS was calculated using the LAD max and minimal LA diameter obtained at end-diastole in the last frame before mitral valve closure as an estimate of LA function (RI 29.4 ± 5.5 in apparently healthy control cats). 15 The maximal LV internal diameter in diastole (LVIDd) and the LV LV FS were obtained from M-mode of the LV in a right parasternal short-axis plane at the level of the papillary muscles. The LVIDd was measured from the trailing edge of the interventricular septum to the leading edge of the left ventricular free wall (RI 12.0–18.4 mm). 16 The LV FS was derived from the calculated difference between the maximal LV internal dimension in diastole and the minimal LV internal dimension in systole as an estimate of LV systolic function (RI 39–67%). 16 The left atrial:aortic ratio (LA:Ao) was obtained from a two-dimensional right parasternal short-axis view at the level of the heart base using the ‘Swedish’ method 17 as an index of LA enlargement (RI 0.63–1.18). 16 Peak left auricular flow velocity (LAu) was obtained from an oblique left apical parasternal long-axis view of the left auricle using pulsed-wave Doppler and used as an estimate of left auricular function (diagnostic cutoff <0.2 m/s used to define increased risk of LA thrombus). 13 The maximal early transmitral flow velocity (Emax or summated Emax and A [EAfusmax], RI 0.6–1.3 m/s) 16 and LV isovolumic relaxation time (IVRT) (RI 37–60 ms) 14 were obtained from left apical long-axis views using pulsed-wave Doppler as estimates of LV diastolic function
At the time of the fourth echocardiogram, the cat was documented to be normotensive (unsedated systolic Doppler blood pressure of 100–110 mmHg). 18 At the time of the fifth echocardiogram, the cat was not azotemic (plasma blood urea nitrogen concentration 32 mg/dl, RI 18–39; plasma creatinine concentration 1.4 mg/dl, RI 0.7–2.0). 19 Thyroid function testing was not performed owing to young age and lack of clin-ically compatible signs. 20
At 32 months after diagnosis, the cat experienced an acute onset of labored breathing. It was evaluated by an emergency veterinarian not affiliated with the institution who performed thoracic radiography and diagnosed congestive heart failure. Because of clinical deterioration, the cat was humanely euthanized. No post-mortem examination was permitted.
Discussion
To the best of the authors’ knowledge, this is the first report of an apical HCM phenotype in a cat. The echocardiographic and electrocardiographic features of apical HCM were first reported in humans in 1976. 21 The constellation of an ‘Ace of Spades’ LV cavity appearance in end-diastole visualized during left ventriculography along with giant negative T waves on ECG was de-scribed in 1979. 22 This phenotype differs significantly from the classical appearance of HCM, which is phenotypically heterogeneous but characterized by predom-inantly septal hypertrophy in humans.23–25 In humans, apical HCM has been defined on echocardiography by an apical wall thickness ⩾15 mm and a ratio of maximal apical-to-left ventricular free wall thickness of 1.5:1.0 or above. 9 Additional features have been reported and include systolic apical cavity obliteration, 10 apical aneur-ysms 26 due to ischemia, 27 variable degrees of mid-LV obstruction 28 and progressive LV diastolic dysfunction leading to LA enlargement.
The 2020 American Heart Association/American College of Cardiology guidelines for the identification of HCM in adult humans describe that a diagnosis of HCM can be made using two-dimensional echocardiography based on a maximal end-diastolic wall thickness of 15 mm or above affecting any LV segment in the absence of another cause for hypertrophy. 29 By applying this rationale to our cat and utilizing the cutoff of an end-diastolic LV wall thickness of 6 mm or greater to define LV hypertrophy in cats, 6 we found unequivocal evidence of apical hypertrophy while wall thickness of the basilar LV walls was within the RI. The ratio of maximal apical thickness to basilar LV free wall thickness in the range of 1.6–2.5 at each of the later four echocardiographic examinations exceeded cutoffs extrapolated from the human literature 9 and further demonstrates that the pathologic changes are confined to the apical region. Based on the methods of assessing apical cavity obliteration described by Kim et al, 10 the cat in this study demonstrated a systolic LV obliteration length:total LV height ratio of 0.9–1.2. In humans with apical HCM, a ratio greater than 0.5 has been associated with significantly worsened outcomes. 10
Several features that have been identified in humans with apical HCM were not identified in our cat: giant nega-tive T waves on the ECG and apical aneurysms. The presence of giant negative T waves on ECG has been identified in the precordial leads (predominantly V4 and V5) in humans diagnosed with apical HCM. In our cat, a 12-lead, diagnostic ECG was not recorded. It should be noted that abnormalities of the T wave are not pathognomonic for apical HCM. The finding of giant inverted T waves is most prevalent in Japanese patients with apical HCM. 30 In a study performed at the Mayo Clinic using a population of North American patients with apical HCM, abnormal T waves were only identified in 11% of cases. 31 The giant negative T waves can disappear from the ECG over time, indicating a dynamic relationship with disease progression. 30 The absence of an apical aneurysm in our cat is not unexpected, as the human literature indicates that this abnormality develops as a result of apical ischemia over prolonged periods of time and may take up to 10 years to manifest. 26 LV apical aneurysms have been previously observed in cats with other HCM morphologies.32–34 Strain imaging has been used more recently in the diagnosis of apical HCM in people, with the ‘Blueberry-on-Top’ phenomenon described in time-to-peak longitudinal strain parametric mapping of the LV in one patient. 35 Generation of these images requires evaluation of two-, four- and five-chamber apical views of the LV, which were not consistently obtained in this case.
Historically, apical HCM in humans has been considered to follow a relatively benign course in most patients. A retrospective study of 105 cases demonstrated the absence of sudden cardiac death and a 95% survival rate 15 years after diagnosis. 9 These findings were confirmed in a subsequent study. 36 However, in a 2011 study of 454 patients with apical HCM, clinically relevant cardiovascular events including heart failure, stroke and cardiac death occurred in 25% of the study population in a median period of just over 3.5 years after diagnosis. 37 Another study revealed that patients with apical HCM, when compared with an age-matched control population, had worse odds of 20-year survival. 31 Specifically, LA enlargement, impaired LV systolic function and increased LV filling pressures have been associated with worse outcomes,37,38 as have end-systolic cavity obliteration 10 and the presence of an apical aneurysm. 39
Our cat demonstrated marked and progressive LA enlargement, as noted by increasing maximal LA dimension over the course of repeated echocardiographic studies. An LA diameter of 20 mm has been shown to correlate significantly with the risk of CHF in cats. 40 As already described, marked apical cavity obliteration was also identified in our cat, although the time course of disease may have been too short for the development of an apical aneurysm. As the last echocardiogram was performed 3 months before euthanasia, the possible development of an aneurysm before clinical decompensation is not excluded.
There are very few phenotypic differentials for apical HCM described in humans. Up to 23% of patients with Fabry’s disease may have evidence of an apical HCM phenotype on cardiac MRI. 41 This condition has not been reported in cats. Other lysosomal storage disorders are rare in cats, and when reported, are often fatal at a young age. 42 People with Fabry’s disease commonly develop comorbid conditions, including proteinuric chronic kidney disease leading to renal failure, which was not identified in our cat. 43 Elite athletes, particularly men, may also demonstrate equivocal apical hypertrophy on echocardiography 44 mimicking apical HCM. Finally, complete fusion of papillary muscles can lead to the impression of apical HCM in humans. 45 However, fusion commonly results in a parachute mitral valve, and if extreme, in mitral stenosis, both not observed in our cat.
In cats, other conditions reported to cause an HCM phenotype include dehydration with pseudohyper-trophy, 46 systemic hypertension,47,48 hyperthyroidism,49,50 acute myocarditis 51 and myocardial lymphoma. 52 In the present case, the cat was never documented to be clin-ically dehydrated or had a condition leading to disproportionate loss of fluid. The cat was documented to be normotensive, and hyperthyroidism was not considered a likely differential based on the young age and absence of supportive clinical findings. In the numerous cases of thyrotoxic cardiomyopathy available in the literature, a primarily apical distribution of hypertrophy in this condition has never been described in cats or humans. 53 Case chronicity similarly renders myocarditis or a neoplastic process unsubstantiated. The lack of histopathology is a limitation of this case report.
Conclusions
We report a novel form of cardiomyopathy in cats characterized by hypertrophy confined to the apex of the LV. Apical HCM is well documented in humans, but to the authors’ knowledge, has not been described in cats. Contemporary opinion suggests that apical LV hyper-trophy confers more substantial morbidity and mortality than originally believed. In the present case, an un-favorable clinical outcome occurred in a young cat with an apical hypertrophy phenotype.
Footnotes
Acknowledgements
The authors would like to thank Dr Alba Stavri and Tim Vojt for their contributions to this case.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
Supplementary material
The following files are available as supplementary material:
Video 1: Cine loop of the left heart from a right parasternal long-axis four-chamber view.
Video 2: Cine loop of the left heart from a right parasternal long-axis four-chamber view.
Video 3: Cine loop of the left heart from a right parasternal short-axis view in the upper third of the left ventricle at the level of the papillary muscles and chordae tendineae.
Video 4: Cine loop of the heart from a left apical long-axis four-chamber view.
Video 5: Cine loop of the heart from a left apical long-axis four-chamber view.