
Abstract
Case summary
A 9-year-old intact female domestic shorthair cat was evaluated for lethargy, vaginal discharge and intermittent perineal swelling that resolved after urination. Ultrasonography revealed severe uterine enlargement consistent with pyometra. During ovariohysterectomy, the urinary bladder was found retroflexed into the pelvic canal and manually repositioned. Despite initial improvement, perineal swelling recurred. CT confirmed persistent urinary bladder retroflexion in the absence of perineal hernia, pelvic trauma or pelvic canal mass. Exploratory celiotomy demonstrated complete absence of the ventral and left lateral vesical ligaments, providing a structural explanation for the recurrent displacement. The bladder was surgically stabilised with an incisional cystopexy, resulting in an uneventful recovery and no recurrence over 7 years.
Relevance and novel information
Urinary bladder retroflexion is exceptionally rare in cats and has been described only in association with pelvic disruption or perineal hernia. This case is the first to describe bladder retroflexion in a cat independent of pelvic diaphragm failure and instead driven by severe uterine distension from pyometra. The case introduces a previously unrecognised pathophysiological mechanism in which chronic uterine enlargement exerts caudal traction on the bladder, potentially compromising vesical ligament integrity and permitting retroflexion. These findings expand current understanding of the factors influencing bladder positioning in cats and demonstrate that reproductive tract pathology alone can lead to bladder malposition. Long-term resolution after incisional cystopexy underscores the effectiveness of surgical stabilisation when bladder support structures are deficient. This case broadens the differential diagnosis for perineal swelling in female cats and highlights pyometra-induced uterine distension as an under-recognised cause of urinary bladder displacement.
Introduction
Urinary bladder retroflexion (UBR) is a pathological condition in which the bladder is displaced from its normal abdominal position and folds backwards into the pelvic canal or even perineal region.1,2 Without timely diagnosis and correction, UBR can lead to serious complications, including lower urinary tract obstruction, hydronephrosis and azotaemia.1,3
In dogs, UBR is most commonly associated with perineal hernia (PH), a condition predominantly affecting older, intact males. Perineal hernia results from weakening of the pelvic diaphragm, often exacerbated by increased intra-abdominal pressure during straining. This leads to distention of the pubovesical pouch – the caudal-most recess of the abdominal cavity – thereby facilitating herniation of abdominal viscera, including the urinary bladder (UB) into the perineal space. Studies indicate that UBR occurs in 14–29% of canine PH cases.4 –6 Less frequently, UBR results from abdominal trauma7 –9 or from conditions causing chronically increased intra-abdominal pressure. 10
PH is rare in cats, accounting for only 0.1–0.4% of reported cases in small animal veterinary medicine, with the vast majority occurring in dogs. 11 Furthermore, its pathophysiology differs markedly from that in dogs, as prostatic disease and hormonal influences appear to play little or no role. Instead, PH in cats is typically associated with congenital malformation of the pelvic diaphragm or, more commonly, with acquired weakening secondary to pelvic trauma, perineal urethrostomy, megacolon, chronic colitis or perineal neoplasia.12,13 Given the overall rarity of PH in cats, UBR is even less frequently encountered. To the authors’ knowledge, only three feline cases of UBR have been reported, all involving marked pelvic disruption: one secondary to a traumatic sacral hernia, 14 one associated with a pelvic fracture and bilateral PH, 15 and one as a recurrence after unsuccessful perineal herniorrhaphy. 16
This case report describes UBR in a female cat in the absence of pelvic trauma, PH or prior perineal surgery. The findings support a previously unrecognised pathophysiological mechanism, in which severe uterine distension due to pyometra appeared to push the pubovesical pouch caudally, resulting in secondary bladder retroflexion. This broadens the differential diagnosis for perineal swelling in female cats and identifies a previously unreported complication associated with pyometra.
Case description
A 9-year-old, 3.9 kg, female intact domestic shorthair cat was presented to the referring veterinarian for evaluation of vaginal discharge, lethargy and an intermittent, fluctuating swelling lateral to the anus. According to the owner, the perineal swelling typically became apparent before urination and resolved immediately after voiding. Fine-needle aspiration of the swelling yielded urine, raising suspicion of UBR. No dysuria, stranguria or defecatory abnormalities were reported. Rectal temperature was elevated at 39.8°C.
Abdominal ultrasound revealed markedly distended uterine horns containing echogenic fluid, consistent with pyometra. The UB could not be identified within the abdominal cavity, likely due to interference from the enlarged uterus. Partial visualisation was achieved using a transperineal approach. However, the small acoustic window and overlying tissues limited reliable assessment of bladder position and morphology. On rectal palpation, no PH was detected.
Exploratory laparotomy confirmed pyometra, and ovariohysterectomy (OHE) was performed. Intraoperatively, the UB was found retroflexed within the pelvic canal but was easily reducible into the abdomen using a combination of digital perineal pressure and gentle traction on the bladder body. No evidence of pelvic trauma was observed. Although the immediate postoperative period was uneventful, the owner reported recurrence of perineal swelling associated with urination in the days after surgery. Persistence of these clinical signs raised concern for ongoing bladder displacement, prompting referral for further diagnostic evaluation.
At the referral centre, rectal examination was again unremarkable with normal anal sphincter tone, and no evidence of PH or palpable masses. Pre-anaesthetic blood work was within reference intervals, except for mild stress-induced hyperglycaemia (Table 1). No urinalysis or urine culture was performed. Abdominal CT revealed a moderately filled UB located entirely within the pelvic canal (Figure 1). Both kidneys were normal in size and shape, with symmetric contrast enhancement and normal excretion. The right ureter appeared unremarkable, while mild dilation of the distal left ureter was observed, suggestive of partial obstruction of the ureterovesicular junction (Figure 2). No pelvic fractures, masses or signs of PH were identified.
Pre-anaesthetic serum biochemistry results
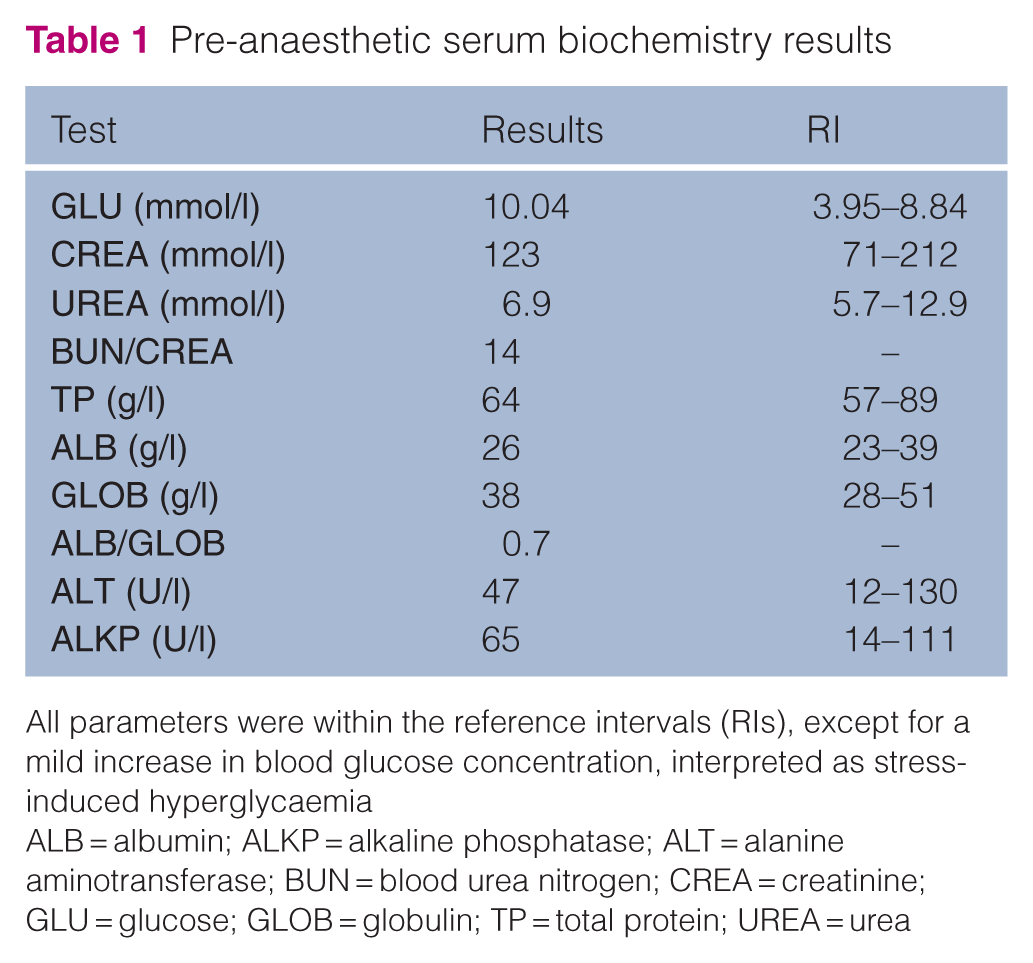
All parameters were within the reference intervals (RIs), except for a mild increase in blood glucose concentration, interpreted as stress-induced hyperglycaemia
ALB = albumin; ALKP = alkaline phosphatase; ALT = alanine aminotransferase; BUN = blood urea nitrogen; CREA = creatinine; GLU = glucose; GLOB = globulin; TP = total protein; UREA = urea

Sagittal CT image of the caudal abdomen and pelvis. The urinary bladder is moderately distended, with the majority of its volume located within the pelvic canal, consistent with urinary bladder retroflexion

Coronal post-contrast CT image of the abdomen and pelvis. The urinary bladder (UB) is moderately filled and abnormally positioned within the pelvic canal. Both kidneys (left [LK] and right [RK]) enhance normally after contrast administration, with no structural abnormalities. The left ureter is mildly dilated caudally near its insertion into the bladder. No contrast medium is visible within the urethra
Given the abnormal caudal position of the UB and the associated dilation of the left ureter, a presumptive diagnosis of caudal bladder displacement with suspected (dynamic) retroflexion was made. Exploratory celiotomy was performed. The cat was premedicated with medetomidine (10 µg/kg IM) and buprenorphine (0.02 mg/kg IM). Anaesthesia was induced with propofol (4 mg/kg IV) and maintained with isoflurane in oxygen. Perioperative analgesia included meloxicam (0.5 mg/kg) administered at induction. Intraoperatively, the UB was confirmed to be retroflexed within the pelvic canal but could be readily repositioned. Both the ventral and left lateral bladder ligaments were absent. After bladder repositioning, the previously observed dilation of the distal left ureter resolved spontaneously. Both ureters appeared grossly normal, and no further abnormalities were identified. An incisional cystopexy was performed 1 cm paramedian right using two interrupted 3-0 polydioxanone sutures. 17 Routine closure was performed.
Postoperative recovery was uneventful, and the cat was discharged the following day with oral meloxicam (0.05 mg/kg q24h) and oxybutynin (1.25 mg q8h). Normal urination and defecation resumed without recurrence of perineal swelling. Follow-up ultrasonography at 2, 6 and 90 weeks confirmed a normal position of the UB and resolution of the previously observed dilation of the distal left ureter.
Discussion
This report describes the first documented case of UBR in a female cat, occurring secondary to a space-occupying abdominal mass (pyometra) in the absence of PH, pelvic trauma or prior perineal surgery. In this case, marked uterine enlargement due to pyometra induced UBR, which persisted after OHE but was successfully resolved by cystopexy.
The proposed pathophysiological mechanism in this case involves a significant mass effect exerted by the distended uterus. Chronic pressure from the enlarged uterus likely displaced the UB caudally into the pelvic canal, while the bladder neck remained anatomically aligned. This retroflexed configuration explains the intermittent perineal swelling and partial obstruction at the ureterovesical junction, as observed on CT imaging. 1
During exploratory laparotomy, the ventral and left lateral vesical ligaments were noted to be absent. These ligaments, derived from embryonic remnants of the urachus and umbilical arteries, are critical for stabilising the bladder within the caudal abdomen and limiting caudal displacement. 18 Their absence provides a direct structural explanation for the recurrent retroflexion of the bladder apex after OHE.
Although the exact timing and cause of ligamentous disruption remain unclear, several potential mechanisms warrant consideration. First, the absence of the ventral and left lateral vesical ligaments may represent a congenital anomaly. Second, progressive uterine enlargement associated with pyometra could have exerted sustained tension on the ligamentous attachments of the bladder, leading to gradual elongation, attenuation or rupture of these ligaments. Finally, although intraoperative manipulation during OHE might theoretically result in the compromise of the bladder ligaments, the presence of perineal swelling that fluctuated with urination before surgery suggests that iatrogenic causes are unlikely.
Although no prior feline reports directly link pyometra to UBR, a similar pathophysiological mechanism has been postulated in dogs. Sontas et al 19 described a case of UBR in a pregnant Rottweiler, attributing bladder displacement to mechanical compression from the gravid uterus, compounded by increased intra-abdominal pressure during excessive barking. Similarly, Niles and Williams 10 reported UBR in a multigravid Cocker Spaniel shortly after parturition, while Özenç et al 9 documented UBR with concurrent vaginal prolapse in a Pointer during late gestation after abdominal trauma. Additional case reports further support the association between reproductive tract conditions and UBR.20,21 Collectively, these canine cases support the hypothesis that gestational or space-occupying reproductive tract pathology – even in the absence of pelvic diaphragm failure – can exert sufficient mechanical, inflammatory or hormonal influence to compromise the integrity of bladder support structures, leading to retroflexion. The present case parallels these findings and represents the first description of this mechanism in a cat with pyometra.
Pelvic bladder syndrome, a condition primarily documented in dogs, was considered an alternative cause for caudal bladder displacement in this case. This condition is characterised by congenital or developmental caudal positioning of the bladder within the pelvic canal, typically without retroflexion. It is most frequently reported in young, intact, large-breed female dogs and is often associated with urinary incontinence, likely due to altered urethral length. 22 Radiographically, the pelvic bladder presents with a blunted caudal pole with 6–26% of the bladder body extending into the pelvic canal. Crucially, the bladder retains its sagittal alignment without retroflexion. In healthy cats, however, the UB remains intra-abdominal regardless of volume, making pelvic positioning highly atypical. 23 In the present case, the dynamic nature of the perineal swelling resolving after micturition, the absence of incontinence and the intraoperative finding of a mobile, easily repositioned bladder all support a diagnosis of UBR and effectively exclude pelvic bladder syndrome.
CT, although not essential for definitive diagnosis, provided valuable information by demonstrating that the UB remained persistently displaced caudally after removal of the enlarged uterus. Mild dilatation of the distal left ureter indicated functional consequences of the malposition and supported the hypothesis of suspected, potentially dynamic, retroflexion. In addition, CT excluded concurrent differential diagnoses, including PH, pelvic fracture or additional space-occupying lesions. These findings highlight the broader clinical significance of UBR, as failure to recognise this condition may result not only in lower urinary tract dysfunction but also predispose to upper urinary tract obstruction and potential renal compromise.
Definitive treatment was achieved through incisional cystopexy, which successfully restored normal bladder position and resulted in durable long-term resolution. Although cystopexy is a well-established technique in dogs with UBR secondary to PH,6,7 its application in cats – particularly in the absence of herniation – remains sparsely documented. To date, cystopexy has been reported in only one other feline case of UBR, where it was performed in conjunction with perineal herniorrhaphy to address concurrent PH. 15 In contrast, the present case involved UBR unrelated to herniation, and cystopexy was performed as a standalone procedure. The absence of recurrence during a 7-year follow-up period supports the efficacy of this technique in cats with compromised ligamentous bladder support.
Conclusions
This case demonstrates that severe uterine enlargement secondary to pyometra can compromise the ligamentous support of the UB, leading to persistent retroflexion in the absence of PH or pelvic trauma even after OHE. Resolution after incisional cystopexy illustrates that surgical stabilisation is effective in restoring bladder position when the vesical ligaments are compromised. These findings identify chronic uterine distension as a potentially under-recognised risk factor for bladder malposition in cats, broaden the differential diagnosis for perineal swelling and emphasise the importance of considering intra-abdominal space-occupying lesions as a cause of bladder displacement. Further studies are warranted to determine the prevalence of UBR associated with reproductive tract pathology and to clarify the mechanisms by which uterine distension may affect bladder support.
Footnotes
Acknowledgements
The authors thank Ilse Tiemessen for her interpretation and assessment of the CT images in this case.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.