
Abstract
Objectives
The aim of this study was to determine if there were any characteristic features of urethral ruptures (URs) on plain radiographs of cats.
Methods
A retrospective, multicentre, case-control study was conducted. Radiographs including the perineum of 22 cats with UR and 70 cats without UR were blindly assessed by two reviewers, scrutinising for features including a perineal bulge, heterogeneous perineal tissue and visibility of the urinary bladder.
Results
A significant association was identified between URs and a perineal bulge (P ⩽0.003), resulting in a sensitivity of 95.5% and a specificity in the range of 38.6–47.1%, and between the presence of URs and a larger perineal bulge size (P <0.001). URs secondary to traumatic accidents were associated with a larger perineal bulge than those secondary to iatrogenic rupture. Cats with URs were more likely to have heterogeneous perineal tissue (P <0.001). There was a significant association between pelvic fractures and a perineal bulge (P ⩽0.001), but not between pelvic fractures and URs (P = 0.783). Binary logistic regression revealed associations between the reviewers’ suspicion for a UR and the reviewers’ recommendation for a lower urinary tract contrast study (LUTS) and a confirmed UR (P <0.001). There was no significant association between an invisible urinary bladder and the presence of a UR (P ⩾0.243).
Conclusions and relevance
Identification of a perineal bulge or heterogeneous perineal tissue in a cat may raise suspicion for a UR, especially in the absence of musculoskeletal injury, which is crucial in reducing time to diagnosis and, therefore, treatment. However, because of the low specificity, correlation with the clinical findings and confirmation or exclusion via a LUTS remains necessary. Visibility of a urinary bladder does not exclude UR.
Introduction
Urethral ruptures (URs) in cats may result from various traumatic causes, such as vehicular trauma, blunt trauma, high rise syndrome, gunshot trauma, 1 lower urinary tract (LUT) disease such as lithiasis or neoplasia, or iatrogenic injury such as urinary catheterisation, urethral deobstruction (eg, retrohydropulsion) or surgery.1 –6 In the largest feline UR study, trauma is the most common cause of URs in cats, accounting for 55.6% of the 63 cases; 1 however, previous studies have shown iatrogenic UR to be the most common.3,7,8
As urine is an irritant to tissues, leakage into the periurethral tissues can result in marked inflammation, pain, tissue death, delayed wound healing and scar tissue formation.2,3,7,9,10 Affected animals may be unable to excrete urine, resulting in a build-up of toxins and electrolytes, such as creatinine, urea and potassium, and subsequent acid-base disturbances that rapidly become life-threatening.2,5,11 In a previous study on URs in 63 cats, 24 (57.1%) suffered short-term complications, but 47 (74.6%) survived to discharge. 1 Potential complications include urethral stricture formation, urinary tract infections, urinary incontinence and fistula formation.3,7,9
Abnormalities that raise concern for UR include LUT signs (dysuria, stranguria, anuria, haematuria), biochemical changes (azotaemia, hyperkalaemia), bradycardia, absent urinary bladder on palpation or imaging, or free abdominal fluid.1,2,4 –7,11 –13 However, URs can easily be missed during initial triage and management, either because of more apparent injuries or life-threatening conditions, or the vague nature of the clinical signs.4,7,13 These signs can take time to develop or be detected, and may require a period of monitoring micturition. For these reasons, there can be significant delays between the initial presentation and UR diagnosis.
Positive contrast retrograde urethrography or vaginourethrography, using radiography or fluoroscopy, is the gold standard diagnostic test if a UR is suspected,1,2,5,11,13,14 collectively referred to as lower urinary tract studies (LUTS). UR is confirmed by extraluminal leakage of contrast into the periurethral soft tissues. 14 It is standard practice to perform plain radiographs before contrast studies to ensure appropriate exposures and screen for an obvious diagnosis (eg, radiopaque calculi). Our radiology team noted an irregularly marginated, heterogeneous, soft tissue opacity bulge in the perineal region of multiple cats on plain radiographs, with subsequently confirmed URs, presumably due to the volume of urine within the periurethral tissues and the secondary inflammatory response. In some cases, these radiographic findings were identified before any clinical suspicion for a UR, facilitating a more rapid diagnosis and prompting the authors to perform this study. In small animals, a perineal bulge is reported as a physical examination finding secondary to extravasation of urine into the surrounding soft tissues; 2 however, to the authors’ knowledge, radiographic changes affecting the perineal region have not previously been described or investigated within the veterinary literature.
The aim of the present study was to describe the plain radiographic features associated with URs in cats and determine their frequency in cats with and without URs. The objective was to determine whether detecting perineal changes in plain radiographs of cats should raise suspicion for URs. The authors hypothesised that an irregular soft tissue opacity perineal bulge would have high sensitivity and low-to-moderate specificity for URs in cats.
Materials and methods
Selection and description of cases
This was a retrospective, multicentre, case-control study. Study design was approved by the Royal College of Veterinary Surgeons Ethics Review Panel. Cases were acquired from the veterinary referral hospitals between January 2013 and January 2023.
The databases of two hospitals (Davies Veterinary Specialists and The Queens Veterinary School Hospital) were searched for feline patients with abdominal or pelvic radiographs including the perineum. The final database (DWR Veterinary Specialists) was searched for feline patients with confirmed URs. For inclusion in the study, at least one lateral radiograph including the entire region of the urethra and the perineal soft tissues was required pre-contrast. Cases were excluded if the radiographs were not of diagnostic quality (eg, if the collimation did not include the perineal region or the tail, if other materials [eg, forceps, positioning aids] were superimposed with the perineal region or if rotation precluded perineal assessment), no plain radiographs were available, the medical records were incomplete, or confirmation or exclusion of a UR was impossible. A diagnostic quality positive contrast LUTS proving UR (Figure 1) and/or identification of UR at surgery was required to confirm a UR. LUTS were performed radiographically or fluoroscopically, depending on the institution and clinician in charge. All studies were performed using diluted non-ionic iodinated contrast instilled into the distal urethra during image acquisition. The studies were deemed diagnostic when the urethral contrast column and extravasated periurethral contrast could be identified on diagnostic-quality images.

Lateral pelvic radiographs of (a) a normal cat and (b) a cat subsequently diagnosed with a urethral rupture showing a large, heterogeneous, soft tissue opacity bulge identified in the perineal region causing dorsal displacement of the tail base. (c) Lateral and (d) frog-legged ventrodorsal positive contrast retrograde urethrogram radiographs of the cat in panel (b) demonstrating contrast extravasation and confirming a urethral rupture
URs were excluded if any of the following criteria were met: (1) no evidence of UR on a diagnostic quality positive contrast LUTS (55/70); (2) no evidence of UR during exploratory laparotomy performed at one of the included institutions (2/70); or (3) the patient had a confirmed diagnosis that was not a UR, no indication of UR in the clinical records, a good response to treatment for the confirmed diagnosis and was successfully discharged (13/70). These cases formed the control group. Approval for the use of anonymised patient data was obtained from each owner.
Patients meeting the criteria were divided into two groups: cats with UR and cats without, which formed the control group. The control group included patients with abdominal or pelvic radiographs acquired for any reason. The rationale behind this was to replicate a normal clinical caseload in order to reduce potential bias. This also allowed investigation into the effect of local trauma on the perineal tissues.
Recorded patient information included age, breed, sex, neuter status, history pertinent to the inciting event, abdominal radiographs, radiology report, surgical report and pertinent follow-up information where available.
A total of 80 cases were initially collected from two hospitals only. This data set was anonymised and randomised by one author (JM) using Excel, and blindly reviewed by reviewer 1 (AH, hereafter R1). Subsequently, 12 anonymised cases from the third hospital were added, and the data set was re-randomised for assessment by two reviewers.
Radiographic assessment
Two European College of Veterinary Diagnostic Imaging board-certified radiologists independently reviewed the plain radiographs of each patient. A minimum of one lateral radiograph was required for each patient; however, ventrodorsal and additional lateral radiographs were provided where available. The complete data set was independently reviewed by R1 and reviewer 2 (RB, hereafter R2), allowing for assessment of inter- and intra-observer agreement. All cases were evaluated using DICOM viewing software (Osirix v14 Bernex) on dedicated medical image viewing monitors. Window width, window level and magnification were adjusted at the reviewer’s discretion.
First, for each case, the reviewers were asked to assess for a perineal bulge (absent/present) and, if present, categorise it as mild, moderate or marked in size. The grading of perineal bulge size was arbitrarily assigned by the primary author. The perineum was considered normal (ie, no bulge) when the caudal perineal margin was concave. The perineal bulge was considered mild when the caudal perineal margin was flattened or mildly biconvex (with a focal indentation at the level of the anus), moderate when there was a clear biconvex shape of the caudal perineal margin, and marked when there was a pronounced biconvex shape and severe swelling of the perineal soft tissues that extended to involve the ventral portion of the tail and/or proximal hindlimbs (Figure 2). The reviewers were shown this example of a normal perineum and of each grading before reviewing the cases; the examples were tightly cropped to show only the perineal region and remove any other potential identifying features from the images. The reviewers did not have access to the example figure during the case review.

Cropped lateral perineal radiographs from four cats determined to have (a) a normal perineum and (b) a mild, (c) moderate and (d) marked perineal bulge by the primary author (JM)
Second, the reviewers were required to record whether the perineal soft tissues were heterogeneous or homogeneous in opacity. Heterogeneous perineal tissue was defined as ill-defined and streaky material within the perineal soft tissues, with a mixture of soft tissue and fat opacities. Third, reviewers were also required to record whether the urinary bladder was included in the radiograph collimation (no/yes) and, if included, whether the urinary bladder small, moderate or large in size. If the collimation was deemed to include the urinary bladder but it could not be assessed (eg, unidentifiable urinary bladder margins due to loss of serosal detail/border effacement, or empty urinary bladder), it was classified as ‘not visible’. All cases had lateral radiographs, and the reviewers were provided the orthogonal radiographs where they were available. The same criteria were used for male and female cats.
For the final assessment, the reviewers were asked to consider all the radiographic features together (eg, presence of perineal changes in combination with the presence or absence of injuries, presence or absence of abdominal serosal detail) and to record if they suspected a UR (no/maybe/yes) and if they would recommend a LUTS based solely on the plain radiographic findings (no/yes). No additional clinical information was provided to the reviewers for this portion of the study. The reviewers were not required to comment on changes unrelated to the urinary tract or surrounding soft tissues.
Statistical analysis
Intra-observer agreement for assessments from 80 patients by R1 and inter-observer agreement for assessments from 92 patients by both reviewers were evaluated using Cohen’s kappa with interpretation as per Landis and Koch. 15 All 80 patients used for the intra-observer agreement were used for the inter-observer agreement, supplemented by the additional 12 patients.
A Mann–Whitney U-test adjusted for ties was used to compare the ages of cats with and without URs. Comparisons of binary variables were made using Fisher’s exact test, separately for each reviewer. Binary logistic regression was used to compare the presence/absence of URs with ordinal variables of perineal bulge size, again separately for each reviewer. Similarly, the presence/absence of URs was compared with the reviewer’s ordinal assessment (no, maybe, yes) of a rupture. Significance was set at P <0.05. The analysis was carried out using Minitab21 and R4.3.3.
Results
A total of 92 cases met the inclusion criteria: 75 male cats (66 castrated, nine entire) and 17 female cats (12 spayed, five entire). The median age was 48 months (range 3–187), which did not differ significantly between cats with and without URs; the medians were 33 months (range 6–116) and 48 months (3–187), respectively (P = 0.183). Breeds comprised domestic shorthair (n = 73), British Shorthair (n = 6), Bengal (n = 4), Siamese (n = 3), domestic longhair (n = 2) and one each of Birman, Norwegian Forest Cat, Persian and Ragdoll. At least one lateral radiograph was available for review in all 92 cases, and ventrodorsal or dorsoventral radiographs were available in 38/92 (41%) cases.
A UR was confirmed in 22/92 (24%) cats; in 21 cases, this was confirmed with a LUTS and in one cat this was confirmed surgically. This resulted in a control group of 70 cats. Of the 22 cats with a UR, 21 were male (19 castrated, two entire) and one was a spayed female.
The most common cause of UR was trauma (15/22, 68%), followed by iatrogenic rupture (4/22, 18%), unidentified cause (2/22, 9%) and urethral obstruction (1/22, 5%). Of the 15 cats that sustained trauma, eight had a road traffic accident (RTA) and seven had unwitnessed trauma. Vertebral, pelvic and hindlimb fractures were present in 5/92 (5%), 23/92 (25%) and 2/92 (2%) cats, respectively.
Intra- and inter-observer agreements are summarised in Table 1. Cohen’s kappa indicates moderate to substantial agreement for all categories assessed. 15
Intra-observer agreement on 80 cases assessed by reviewer 1 on two separate occasions and inter-observer agreement on 92 cases (the initial 80 plus 12 additional) assessed by both reviewers, with interpretation as per Landis and Koch 15

LUTS = lower urinary tract study
A perineal bulge was identified in 21/22 (95%) cats with a UR by both R1 and R2. In comparison, they identified a perineal bulge in the control group in 43/70 (61%) cats (P = 0.003) and 37/70 (53%) cats (P <0.001), respectively. This resulted in a sensitivity of 95.5% (95% confidence interval [CI] 77.2–99.9) for both reviewers and a specificity of 38.6% (95% CI 27.2–51.0) and 47.1% (95% CI 35.1–59.4) for R1 and R2, respectively. The positive predictive value (PPV) for UR when a perineal bulge was observed was 32.8% (95% CI 21.6–45.7) and 36.2% (95% CI 24.0–49.9), and the negative predictive value (NPV) was 96.4% (95% CI 81.7–99.9) and 97.1% (95% CI: 84.7–99.9) for R1 and R2, respectively.
In 18/92 cats, the perineal bulge demonstrated homogeneous fat opacity rather than soft tissue opacity, which was attributed to increased body habitus; however, a UR was confirmed in one of these cats. Excluding these 18 cases from the data set, a perineal bulge was then identified in 20/21 (95%) cats by both R1 and R2, reducing the sensitivity to 95.2% (95% CI 76.2–99.9) for both reviewers, but increasing the specificity to 45.3% (95% CI 31.6–59.6) and 52.8% (95% CI 38.6–66.7), and PPV to 40.8% (95% CI 27.0–55.8) and 44.4% (95% CI 29.6–60.0) for R1 and R2, respectively.
Where present, perineal bulges were graded as mild (R1 = 35, R2 = 23), moderate (R1 = 24, R2 = 20) and marked (R1 = 5, R2 = 15); an example of each grade is shown in Figure 3. For both reviewers, a larger perineal bulge was significantly associated with the presence of a UR, as demonstrated in Figure 4 (R1: odds ratio [OR] 3.93, 95% CI 1.95–7.95; P <0.001 and R2: OR 2.46, 95% CI 1.49–4.05; P <0.001).
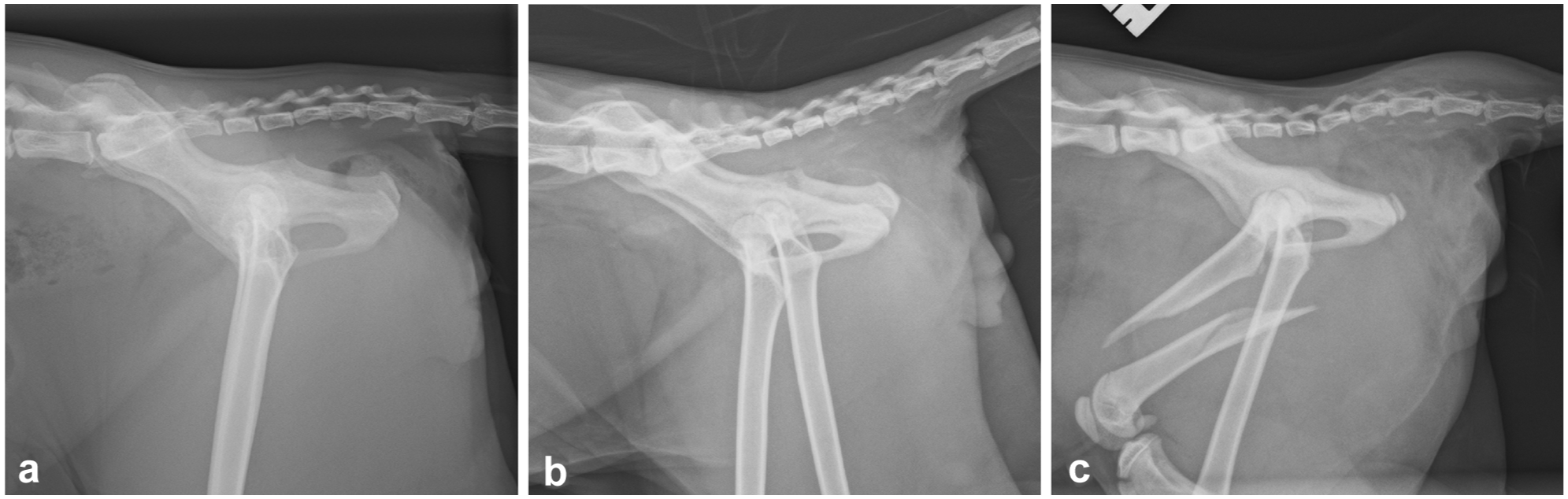
Lateral pelvic radiographs from three cats that were determined to have a (a) mild, (b) moderate and (c) marked perineal bulge by both reviewers

The percentage of cases placed into each perineal bulge size category by reviewer 1 (blue bars) and reviewer 2 (red bars) that had a urethral rupture
For the UR group, Figure 5 shows the relationship between the grading of perineal bulge size for each reviewer and the cause of the UR. URs secondary to trauma were associated with larger perineal bulges; a moderate or marked bulge was identified in 10/15 (67%) and 11/15 (73%) 15 cats that sustained trauma by R1 and R2, respectively. By comparison, URs secondary to iatrogenic perforation most commonly had a mild perineal bulge (3/4, 75% for both reviewers), and no marked perineal bulges were identified by either reviewer.
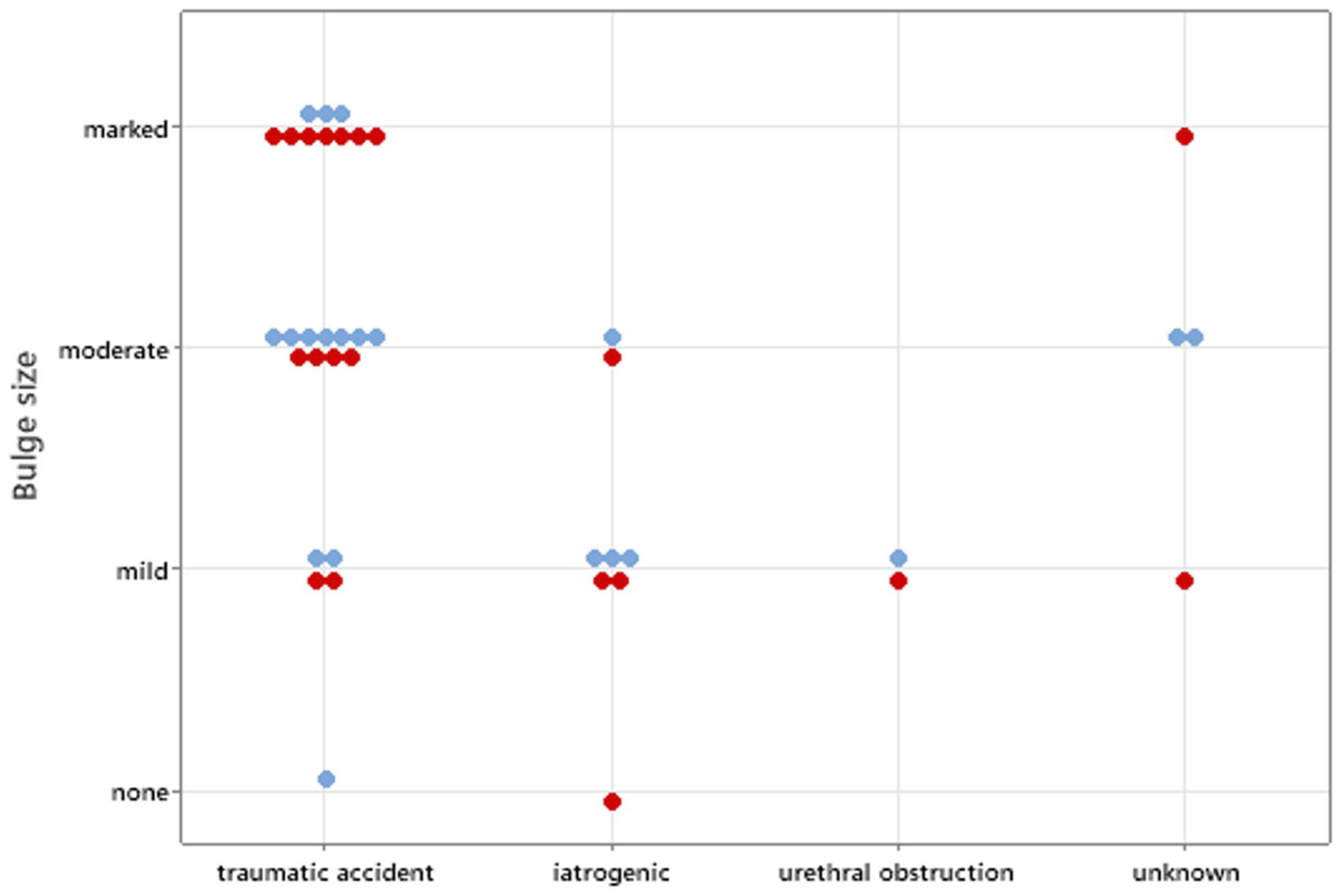
Perineal bulge size gradings by reviewer 1 (blue dots) and reviewer 2 (red dots) plotted against the cause of urethral rupture
Heterogeneity of the perineal soft tissues was identified significantly more often for cats with UR compared with the control group: 91% vs 40% (P <0.001) for R1 and 91% vs 43% (P <0.001) for R2. This resulted in sensitivities of 90.9% (95% CI 70.8–98.9) for both reviewers and specificities of 60.0% (95% CI 47.6–71.5) and 57.1% (95% CI 44.7–68.9) for R1 and R2, respectively. Of the 21/92 cats that presented for an RTA, both reviewers concluded that 20/21 (95%) had a perineal bulge and 20/21 (95%) had heterogeneous perineal tissue. One cat from the RTA group did not have a perineal bulge or heterogeneous perineal tissue identified by either reviewer.
The urinary bladder was deemed to be included within the radiographic study in 89/92 (97%) cases by both reviewers. The urinary bladder was considered to be within the study but was not visible in five (5%) and 10 (11%) cats by R1 and R2, respectively. There was no significant association between the lack of a visible urinary bladder and the presence of UR (P = 1.000 for R1 and P = 0.243 for R2).
There was no significant association between the presence of UR and pelvic fractures (P = 0.783), vertebral fractures (P = 0.333) or hindlimb fractures (P = 1.000). A significant association between pelvic fractures and a perineal bulge was identified for both reviewers (R1: 96% of fractures had a perineal bulge vs 61% for non-fractures; P = 0.001 and R2: 96% vs 52%; P <0.001); however, there was no significant association between hindlimb fractures and a perineal bulge (R1: P = 0.525; R2: P = 0.529), or between vertebral fractures and a perineal bulge (R1: P = 0.318; R2: P = 0.648).
Binary logistic regression revealed an association between the reviewers’ suspicion for UR and the confirmed diagnosis of UR (Figure 6). R1 had an OR of 175 (95% CI 16–1896; P <0.001), while R2 had an OR of 205 (95% CI 19–2172; P <0.001).

The percentages of cases with confirmed urethral ruptures that were classified by reviewer 1 (blue bars) and reviewer 2 (red bars) as not having, maybe having and having a urethral rupture based on assessment of plain radiographs
There was a significant association between the reviewers’ recommendation to perform a LUTS and the presence of UR. A LUTS was recommended for 91% and 95% of UR cases and 41% and 49% of non-rupture cases by R1 and R2, respectively (both P <0.001). However, in 20/64 cases for which either reviewer recommended a LUTS, at least one reviewer commented it was because of their concern for urethral obstruction as opposed to a UR.
Discussion
Three plain radiographic features with significant association to URs in cats were identified in this study: the presence of a perineal bulge; a larger perineal bulge; and heterogeneous perineal tissue. A perineal bulge alone resulted in a high sensitivity (95.5%) and NPV (96.4–97.1%), but a low specificity (38.6–47.1%) and PPV (32.8–36.2%) for UR, partially supporting our hypothesis. However, it is important to note that the prevalence of URs in this data set is expected to exceed the true prevalence, and the PPV and NPV may not reflect those of the general population.
Specificity (45.3–52.8%) and PPV (40.8–44.4%) were further increased once the fat opacity perineal bulges that were presumed to be associated with increased body habitus were excluded. Sensitivity was slightly lower for heterogeneous perineal tissue (90.9%), but specificity was greater (57.1–60.0%). The lower specificities and PPVs for these features can be explained by the other possible differentials for perineal swelling and heterogeneity, including haemorrhage, cellulitis, oedema, perineal hernias, abscessation, granulomas, urinomas 16 or neoplasia. Many of these changes may occur concurrently with trauma, complicating assessment of the perineal region.
Pelvic fractures were associated with a perineal bulge for both reviewers, supported by the high sensitivity and NPV, which correlates with the expected soft tissue trauma, oedema and haemorrhage associated with most pelvic fractures. This is supported by the higher prevalence of concurrent musculoskeletal injuries in cats with traumatic URs. 1 However, in this study, pelvic fractures were not significantly associated with the presence of URs. Pelvic fractures have previously been commonly associated with LUT rupture in small animals;3,11,13,17,18 however, another study showed only 37% of URs in cats were associated with pelvic fractures compared to 85.7% in dogs. 2 One study in cats and dogs concluded that animals with pelvic fractures were 6.4 times more likely to incur urinary tract trauma; however, cats were not separated from dogs in this part of the analysis, and therefore, this is considered less representative of the feline population. 13 Neither vertebral fractures at or near the lumbosacral junction nor hindlimb fractures were associated with a perineal bulge, although limited cases met these criteria; therefore, these findings should be interpreted with caution.
The perineal bulges observed with iatrogenic URs were smaller compared with those identified in trauma cases; however, this result should be interpreted with caution, as only 4/22 UR cases were classified as iatrogenic. A previous study determined that URs secondary to trauma were more likely to be associated with complete rupture of the urethra in comparison to iatrogenic injuries. 1 A greater volume of urine extravasation and secondary cellulitis would be expected for these cases, which may explain a larger perineal bulge. Cats with URs secondary to trauma are also more likely to have concurrent musculoskeletal injuries, 1 resulting in concurrent bruising and haematoma formation, inflammation, tissue oedema and cutaneous/subcutaneous wounds, which may also contribute to soft tissue swelling in the perineal and pelvic regions.
When the reviewers considered all plain radiographic changes together, there was a strong association between both their suspicion for UR and recommendation to perform a LUTS, with the presence of UR. For multiple cases, both reviewers commented that their suspicion for a UR notably increased when the perineal swelling could not be explained by the presence or degree of local trauma. In approximately one-third of cases where a LUTS was recommended, the reviewers also noted that their recommendation was due to concern for a urethral obstruction (eg, urolithiasis, marked urinary bladder distension) as opposed to a UR. In this study, the reviewers were blinded to any case information; however, in a clinical setting, the clinical and biochemical findings would also be taken into consideration, helping to further narrow down cases for which a LUTS would be indicated.
Intra- and inter-observer agreement was moderate to substantial across all radiographic findings. Substantial intra- and inter-observer agreement was found for the presence of a perineal bulge (range 0.61–0.65) or heterogeneous tissue (range 0.70–0.74), both of which were significantly associated with URs. This substantial inter-observer agreement highlights that independent reviewers can repeatedly identify these radiographic findings, despite them being subjective, and demonstrates their potential clinical utility in raising a suspicion of urethral or peri-urethral disease. Intra- and inter-observer agreement was moderate for the size of the perineal bulge (0.43–0.51); however, this assessment is more subjective, so greater variability is unsurprising. As a cutoff for perineal bulge size and likelihood of UR are not being suggested, the lower intra- and inter-observer agreement for this feature compared to the presence of a perineal bulge is less likely to have a significant clinical implication; however, perineal bulge size remained significantly associated with UR for both reviewers.
The lateral radiographs were primarily used by both reviewers to assess for perineal changes. Subjectively, larger perineal bulges could be identified on both lateral and ventrodorsal/dorsoventral projections, but smaller perineal bulges were identified on the lateral radiographs only. Both reviewers, therefore, utilised the lateral projection as the primary radiograph for classification. The presence and/or size of the perineal bulge between orthogonal radiographs were not formally assessed in this study.
The UR population in this study was heavily dominated by male cats (21/22, 95%), which is in accordance with the recent literature, in which 88.9% of the 63 cats with UR in a large retrospective study were male. 1 Several studies suggest that male cats are more frequently affected than female cats. This is attributed to factors such as their narrower urethra, which predisposes them to obstruction; the attachment of their urethra to the ischium via the ischiocavernosus and ischiourethralis muscles, which limits their ability to tolerate traction or shear forces; and their increased roaming behaviours, leading to a higher risk of vehicular trauma. However, many of the existing references for this concept actually relate to an increased risk of urinary bladder or LUT rupture in general for males, rather than UR specifically. One study suggested that the increased likelihood of LUT rupture in males may not hold true in cases caused by severe blunt trauma; however, this portion of their study only included eight patients, five of which were male, and it was therefore considered that this may represent a type II error. 13
No association was found between the inability to identify the urinary bladder on radiographs and URs. This is in accordance with previous literature5,19 as with URs, the extravasated urine often leaks through a small defect distal to the urethralis muscle and therefore may not affect the ability of the urinary bladder to store urine.5,13,20 In addition, distal URs may result in extravasation into the peri-urethral soft tissues but not the peritoneal space, meaning free abdominal fluid may not be present.1,5,13 Hence, a visible urinary bladder should not be used to exclude UR.
The authors postulated that the UR location may influence the presence and size of a perineal bulge, with more caudal ruptures potentially resulting in more pronounced perineal changes. However, previous studies have indicated that intra-pelvic UR is most prevalent in trauma cases, whereas post-pelvic rupture is more frequently observed in iatrogenic cases,1,21 contradicting this proposed theory. The increased likelihood of post-pelvic ruptures in iatrogenic cases may be attributed to the presence of the sigmoid flexure and the relatively narrow diameter of the penile urethra caudally.1,22 Accurate confirmation of UR location and size was not available for this study, precluding further statistical analysis.
Body condition was not included because of its inconsistent documentation. However, a perineal bulge caused by increased body habitus should result in a homogeneous increase in fat opacity, not soft tissue opacity, which a competent reviewer should be able to differentiate. This is demonstrated by the increased specificity and PPV when the fat opacity perineal bulges were excluded from the perineal bulge category.
This study has several limitations, including the small number of confirmed UR cases despite the multicentre approach and its retrospective nature, resulting in small numbers within some subgroups, limiting statistical analysis. The number of radiographs, projections, collimation, quality and positioning varied between patients. In some patients, a urinary catheter had been placed before the acquisition of radiographs, and the presence or location of the urinary catheter may therefore have introduced bias. In multiple cases, wet fur artefact also complicated assessment of the perineal tissues. However, these all reflect the variability seen in clinical practice. In addition, not all control cases were confirmed by a LUTS or surgical assessment, and the urinary studies were performed by a variety of personnel and techniques; therefore, some cases could potentially have been misclassified.
Conclusions
Delays in suspicion for, or identification of, feline UR can occur because of the time taken to develop recognisable clinical signs or biochemical changes. This study revealed significant associations between the presence of a perineal bulge, a larger perineal bulge and heterogeneous perineal soft tissues with the presence of URs in cats. Identification of these radiographic features can prompt performing a LUTS in cases where this otherwise may not have been considered, which in turn may lead to earlier diagnosis and treatment of URs. Therefore, careful scrutiny of the perineal tissues on plain radiographs is recommended. However, as a result of the low specificity and PPV of these plain radiographic features, the decision to perform a LUTS in the clinical setting should factor in the history, physical examination findings, biochemistry and any other imaging findings.
Footnotes
Author note
Preliminary findings from this study were presented at the 2023 European Association of Veterinary Diagnostic Imaging-British and Irish Division Spring Meeting.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Linnaeus Veterinary Limited supported the costs of the open access publication charges.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.