
Abstract
Case summary
A 9-year-old neutered male domestic shorthair cat was presented for anorexia and lethargy with a 2-day history of ptyalism and dysorexia. The cat had undergone a cholecystoduodenostomy 8 years before presentation and had suffered from episodes of clinical cholangitis ever since. Abdominal ultrasound revealed duodenal obstruction. Two stones were surgically removed, subjected to spectrophotometric examination and identified as choleliths. Clinical improvement was noted postoperatively, and 12 months after surgery the cat was doing well and had no further digestive problems.
Relevance and novel information
This case report describes an original case of gallstone ileus, a complication which, to our knowledge, has never been described after cholecystoduodenostomy in cats. A parallel can be drawn with Bouveret’s syndrome in humans, which is characterised by duodenal or gastric gallstone ileus secondary to an acquired bilioenteric fistula.
Introduction
Cholelithiasis is rare in cats, and most of them are pigment stones composed of calcium carbonate, bilirubin or both.1 –3 They can be incidental or symptomatic, especially if they are obstructive. Of choleliths in cats, 80% are reported to be radio-opaque. 4 Biliary tract obstruction often requires surgical treatment by cholecystectomy or cholecystoenterostomy. 5 Potential complications associated with cholecystoenterostomy include duodenal or gastric ulceration, haemorrhage, incisional dehiscence, stoma stricture and ascending cholangitis. 4 In humans, gallstone ileus is a mechanical intestinal obstruction due to the impaction of one or more large gallstones within the gastrointestinal tract. It is an uncommon complication of cholelithiasis, and it is caused by the passing of a gallstone from the bile ducts into the intestinal lumen through a fistula, most frequently between the gallbladder and the duodenum. 6 This case report describes a new complication of cholecystoduodenostomy that has not been previously described.
Case description
A 9-year-old neutered male domestic shorthair cat was presented for vomiting, anorexia and lethargy with a 2-day history of ptyalism and dysorexia. The cat was feline immunodeficiency virus (FIV)-positive and had undergone a cholecystoduodenostomy 8 years earlier for extrahepatic biliary obstruction secondary to duodenal papilla thickening and stenosis in a context of bacterial cholangitis and cholecystitis. Ten days before presentation, he had been hospitalised for 48 h for vomiting, depression, anorexia and pyrexia. Abdominal ultrasound revealed signs of cholecystitis and pancreatitis, and choleliths in the gallbladder, biliary and intrahepatic ducts (Figures 1 and 2). On blood biochemistry, an increase in liver enzyme activity (alanine aminotransferase = 645.9 UI/l, reference interval [RI] 8–53; alkaline phosphatase = 363 UI/l, RI 60–100; and total bilirubin = 43.0 mg/l, RI 0.0–9.0) was documented at that time. The patient was discharged from the clinic with treatment, including choleretics (ursodeoxycholic acid, 15 mg/kg PO q24h for at least 3 months), corticoids (prednisolone, 0.5 mg/kg PO q24h for 7 days) and antibiotics (metronidazole 12.5 mg/kg PO q24h and amoxicillin/clavulanic acid 20 mg/kg PO q12h for 10 days). Treatment was only administered for 3 days because of vomiting. The cat had been experiencing these signs episodically since its former surgery, which improved with the above treatments. Neutrophilic cholangitis secondary to ascending bacterial infection was suspected to be at the origin of these crises, based on previous cytological examination of the bile, carried out during the first surgery.
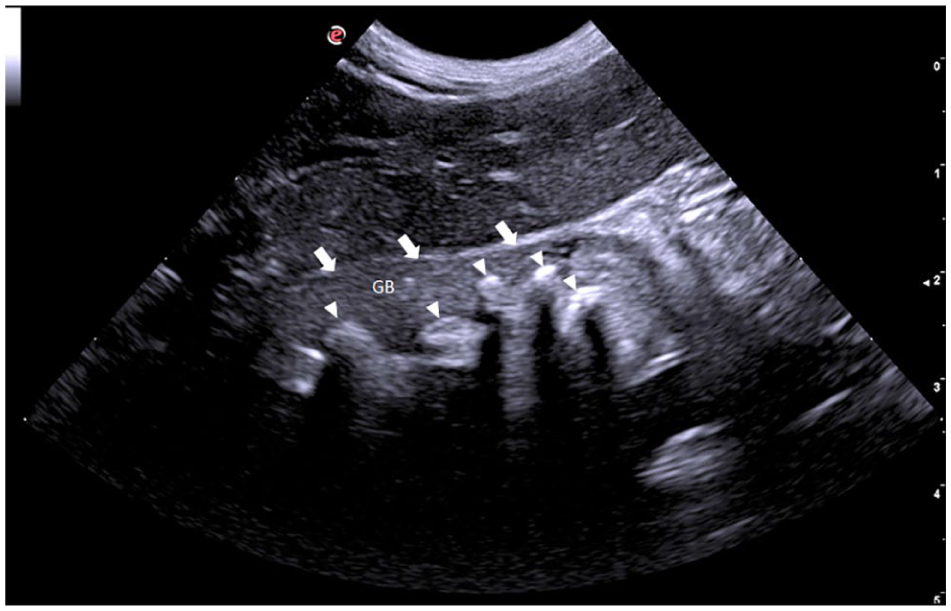
Abdominal ultrasound: gallbladder (GB) (the arrows highlight its border) and multiple choleliths (arrowheads)
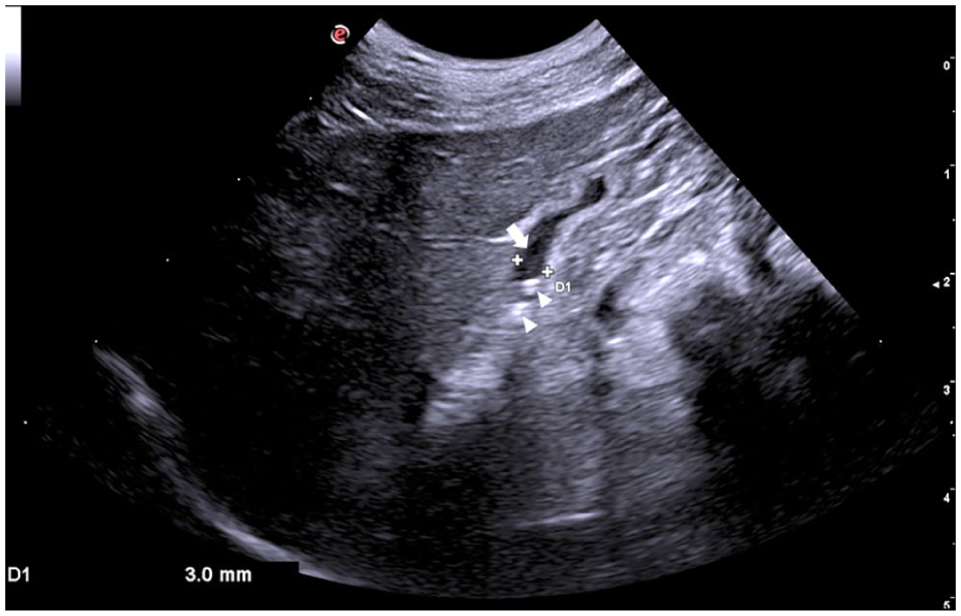
Abdominal ultrasound: dilation of an intrahepatic duct (arrow) secondary to choleliths (arrowheads)
On admission, clinical examination revealed a cat in lateral decubitus, depression, hypothermia at 35.5°C, 10% dehydration, pale pink tacky mucous membranes, capillary refill time of 2 s, bradycardia at 100 bpm and pain on abdominal palpation. These findings were consistent with hypovolaemic shock and abdominal pain.
Blood tests are summarised in Table 1. Abdominal radiographs were unremarkable (Figure 3). On abdominal ultrasound, an empty bladder, renal pelvic lithiasis without associated dilatation and a mechanical ileus due to an obstructive duodenal foreign body were noted. Observations also included a thickened gallbladder wall with predominantly hyperechoic, heterogeneous content with posterior acoustic shadows, hyperechoic elements with acoustic shadows in the intra- and extra-hepatic bile ducts, and diffuse steatitis.
Blood tests revealed severe hyperkalaemia and ionised hypocalcaemia, as well as increased levels of blood urea nitrogen (BUN), creatinine, blood glucose, total proteins, liver enzyme activities and elevated total bilirubin; there were also signs of haemoconcentration and moderate neutrophilic leukocytosis
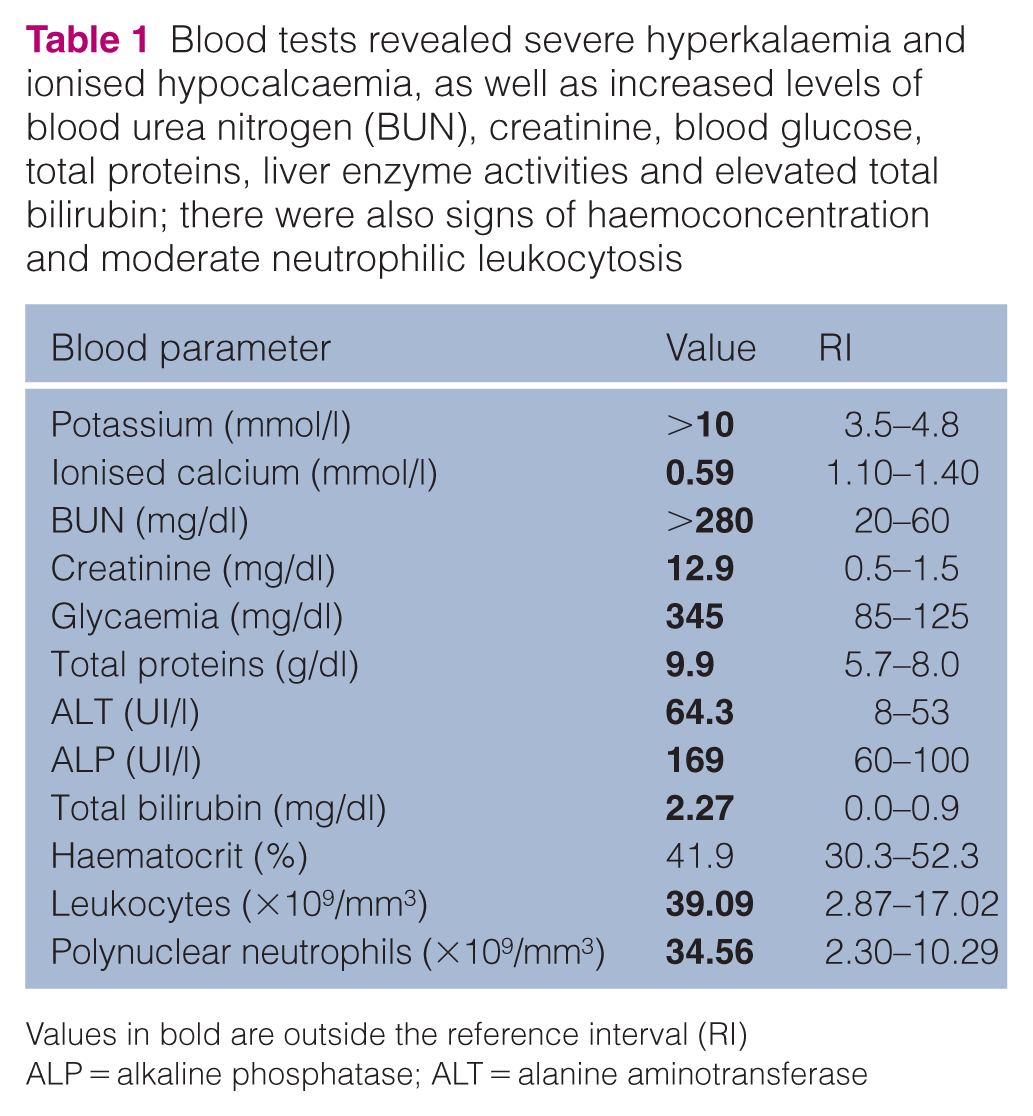
Values in bold are outside the reference interval (RI)
ALP = alkaline phosphatase; ALT = alanine aminotransferase

Right lateral and ventrodorsal abdominal radiographs were unremarkable
Initial management consisted of correction of electrolyte imbalances, treatment of hypovolaemic shock and an insulin-glucose protocol with administration of calcium gluconate for hyperkalaemia. Supportive medical treatment (maropitant 1 mg/kg IV q24h; methadone 0.2 mg/kg IV q4h then buprenorphine 20 µg/kg IV q8h; pantoprazole 1 mg/kg IV q12h; ursodeoxycholic acid 15 mg/kg PO q24h) and antibiotic therapy (ampicillin/sulbactam 20 mg/kg IV q8h) were initiated pending surgical management. After normalisation of the hyperkalaemia (K+ = 3.73 mmol/l, RI 3.5–4.8) and improvement in azotaemia (blood urea nitrogen [BUN] = 136 mg/dl, RI 20–60; creatinine = 2.61 mg/dl, RI 0.5–1.5), two distal duodenal calculi were removed by enterotomy approximately 48 h after admission (Figure 4). Closure of the duodenum was standard, with a simple continuous monofilament absorbable suture (Monosyn 4-0; B Braun). Spectrophotometric analysis of these calculi revealed the presence of calcium bilirubin and calcium palmitate with traces of aragonite (calcium carbonate). This composition suggests that these stones were of biliary origin, 5 and moved into the intestine at the site of cholecystoduodenostomy.

The two occlusive distal duodenal calculi that were removed by enterotomy. The largest one measured 1.5 cm
In the postoperative period, the initial treatment was continued; an improvement in general condition and renal parameters was noted, leading to discharge from the clinic 48 h postoperatively. Two weeks later, the cat’s general condition was good, which led to the continu-ation of the treatment with choleretics and corticoids (prednisolone 0.5 mg/kg PO q48h; ursodeoxycholic acid 15 mg/kg PO q24h) and the discontinuation of antibiotic therapy. At 12 months postoperatively, the cat was doing well, had regained weight, had no digestive disorders and was still on the same treatment.
Discussion
Cholelithiasis is rare in veterinary medicine compared with human medicine, where it is a common reason for hospitalisation, affecting almost 20% of the population; it is considered asymptomatic and of incidental discovery in 75% of cases. 7 According to a recent study, a prevalence of 0.99% was suggested in cats, being an incidental finding in 41% of cases, with affected animals not having any clinical signs of extrahepatic biliary obstruction. 5 In this clinical case, the presence of choleliths is important because they caused a mechanical duodenal obstruction, and may have contributed to the development of a chronic bacterial cholangitis, acting as a nidus of infection.
In humans, various genetic, environmental, metabolic and clinical factors are known to predispose to cholelith formation. 7 However, because the compos-ition of gallstones in cats is different, it is difficult to draw parallels with humans. Confirmed or suspected causes in cats include altered bile composition, bile supersaturation, precipitation of a nucleus, mucin hypersecretion, aberrant biliary pH, biliary stasis or aberrant gallbladder motility, biliary bacterial infections, cholecystitis, cholangitis and dietary factors.8 –14 In this cat, episodes of bacterial cholangitis/cholecystitis and cholecystoduodenostomy may have favoured the formation of choleliths. The surgical procedure likely altered bile flow and allowed duodenal bacteria to reach the gallbladder, potentially causing chronic infection and changes in bile composition, while the large ostomy site may have induced enterobiliary reflux, leading to chronic gallbladder inflammation, ascending infection of the hepatic ducts and chronic cholangitis. As they were asymptomatic, renal pelvic calculi detected on abdominal ultrasound were not investigated. However, as most of these stones in cats are composed of calcium oxalates,15,16 it would have been interesting to check this cat’s blood calcium levels outside of this crisis period (Table 1), since chronic hypercalcaemia could be a risk factor for both the renal pelvis stones and choleliths.17,18 Indeed, the low calcium level measured here was probably mainly due to vomiting and dehydration.
At the time of the first surgery, a cholecystoduodenostomy was performed because of the inability to insert a biliary stent, which is not always feasible in cases of stenosis or thickening of the duodenal papilla secondary to bacterial cholangitis and cholecystitis. This was necessary despite the cat being only 1 year old. A biliary stent may be preferable, when possible, as it preserves the physiology of bile flow. For several years, the cat had been treated with a combination of corticosteroids and antibiotics (metronidazole and amoxicillin/clavulanic acid) by his veterinarian whenever he experienced phases of anorexia, vomiting and lethargy. Ideally, a cytological analysis and bacterial culture would have been performed on bile taken by cholecystocentesis before these treatments to confirm the initial hypothesis of bacterial cholecystitis. However, the episodic nature of these relapses, financial considerations and the owners’ fatigue may explain why further tests were not performed, especially when treatments led to clinical improvement in the cat.
The originality of this clinical case lies in the duodenal obstruction secondary to choleliths, which, to our knowledge, is a complication of cholecystoduodenostomy that has never been described in the literature in cats. This condition is known as Bouveret’s syndrome in humans, which is defined as proximal pyloric or duodenal obstruction secondary to the presence of a cholelith that has passed through an acquired bilioenteric fistula.19,20 A number of factors have been reported to contribute to the obstructive nature of choleliths; 21 for example, they can lead to ileus if they are large (>2.5 cm) or if an anatomical or clinical context favours obstruction. In cats, pyloric obstruction does not appear to be possible in this context, given the position of the stoma in the proximal duodenum. These choleliths could also be occlusive at the level of the jejunum, ileum or ileocolic orifice, depending on their size. The size of the stoma could play a role in stone formation: if it is too small, biliary obstruction could occur again; if it is too large, this could encourage ascending bacterial contamination. In this cat, the choleliths were relatively large (approximately 1.5 cm), resulting in duodenal obstruction after passing through the opening created during the first surgery. The clinical presentation of Bouveret’s syndrome in humans is not specific: acute abdomen (70%), haematemesis (15%), dehydration and vomiting (85%) and melena (6%). 20 Some similar signs were observed in this cat (vomiting, dehydration and pain on abdominal palpation) but did not help to guide the diagnostic hypotheses. The Mordor triad – a history of gallstones, clinical signs of cholecystitis and sudden duodenal obstruction – has been described in human medicine to guide diagnosis. 22 Evidence of this triad should raise suspicion of Bouveret’s syndrome in the affected patient. These criteria were met in this cat, which could have led to suspicion of this syndrome.
There is no consensus on the management of Bouveret’s syndrome in humans. A duodenotomy was performed to remove the duodenal obstruction. Despite multiple medical treatments with ursodeoxycholic acid, bile stones formed and could not be cleared. It is likely that this cat’s FIV-positive status contributed to the chronic bacterial infection and poor clearance of the bile stones.
The lack of histological or bacteriological analysis for financial reasons is one of the limitations of this case, as it would have been of interest to study the factors predisposing to cholelithiasis in this cat. Another limitation is the lack of urine output monitoring. Indeed, monitoring urine output might have been of interest, as it is likely that the cat had an acute kidney injury given the high blood values of BUN, creatinine and hyperkalaemia. The cat’s response to treatment and the normalisation of potassium levels within 48 h are consistent with acute kidney injury, with renal perfusion, diuresis and potassium elimination resuming after fluid therapy.
Conclusions
This original case presents a duodenal obstruction caused by choleliths that should be considered a newly described complication of cholecystoduodenostomy. A parallel can be drawn with Bouveret’s syndrome in humans. The Mordor triad (a history of gallstones, clinical signs of cholecystitis and acute duodenal obstruction) should be considered when identifying symptomatic choleliths in cats as it provides a strong diagnostic guide.
Footnotes
Acknowledgements
The authors would like to thank Mélanie Garcia, DVM, and Charlotte Bibaut, DVM, for their participation in the medical and surgical management of this case report.
Author note
This case report was presented at the annual scientific meeting of the Association Française des Vétérinaires pour Animaux de Compagnie in November 2024 in Lyon, France.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.