
Abstract
Case summary
A 7-year-old castrated male domestic shorthair cat was presented for surgical intervention for obstructive pancreatolithiasis. The patient had a history of chronic weight loss, vomiting and lethargy. Elevation of feline pancreas-specific lipase and a marked decrease in cobalamin were documented on blood biochemistry. Abdominal ultrasound revealed an enlarged right pancreatic limb with a dilated central duct and multiple pancreatoliths visualized within, consistent with partial pancreatic duct obstruction. The patient was successfully treated with a minor duodenal papilla construction using a 2.5 Fr double pigtail ureteral stent.
Relevance and novel information
Pancreatolithiasis is an exceptionally rare condition in veterinary medicine, particularly in cats, with only a few reported cases. Given its low incidence, there is no established consensus regarding the best therapeutic options in clinical practice. This case report outlines the successful application of a locking loop catheter to re-establish the patency of a pancreatic duct. Notably, this is the first documented use of this technique for the surgical management of obstructive pancreatolithiasis.
Keywords
Introduction
Histopathologic evidence of pancreatitis can be seen in 67% of cats, including 45% of apparently healthy cats. 1 While the etiology of pancreatolithiasis in cats remains unknown, chronic pancreatitis in humans has been linked to the development of pancreatolithiasis in 50–100% of patients with this condition.2 –6 In veterinary medicine, pancreatolithiasis has been infrequently reported in bovine animals, experimentally demonstrated in dogs and only six cases have been documented in cats.7 –17 This case report describes an innovative approach to address obstructive pancreatolithiasis using a 2.5 Fr double pigtail ureteral stent (Vet Stent-Ureter; Infiniti Medical) to re-establish a non-patent minor duodenal papilla in a feline patient.
Case description
A 7-year-old castrated male domestic shorthair cat presented (day 0) to the referring veterinarian (rDVM) with approximately 7 days of lethargy and vomiting of undigested food, despite having a normal appetite. The patient weighed 6.82 kg (Figure 1) and the physical examination was largely unremarkable. Baseline bloodwork (complete blood count [CBC], serum biochemistry) showed a mild normocytic, normochromic anemia (red blood cell [RBC] range 5.3–5.9 ×106/µl, reference interval [RI] 5.92–9.93) and lymphopenia (range 924–1162/µl, RI 1200–8000) that was persistent on subsequent serial CBCs before surgery. Supportive care, including subcutaneous fluids, B-vitamin complex injection and maropitant, was initiated. The patient was discharged with a supplement (Pet-tinic; Zoetis) containing iron, copper, thiamine, riboflavin, niacin and B vitamins. Three weeks later (day 21), the cat weighed 6.68 kg (Figure 1) with occasional vomiting, albeit an improved activity level. Mild anemia and lymphopenia persisted. Four weeks later (day 49), the patient was presented for perceived weight loss, and was found to weigh 6.09 kg (Figure 1). Anemia and lymphopenia persisted, and a slight elevation of blood glucose (182 mg/dl, RI 64–170) was noted. A total thyroxine (T4) and urinalysis were run for completeness but were unremarkable.

Weight trend graph illustrates a progressive decline in weight before surgical intervention, followed by an increase in body weight postoperatively
The patient was referred to the internal medicine service (day 55) for further evaluation. An examination showed decreased body weight, at 5.79 kg (Figure 1), but was otherwise unremarkable. Thoracic and abdominal radiographs showed numerous calculi in the cranial abdomen, cranioventral to the stomach (Figures 2 and 3). An abdominal ultrasound further localized the calculi within the pancreatic duct (Figure 4). An enlarged right limb of the pancreas with a dilated central duct, measuring nearly 1 cm, was noted, consistent with partial obstruction of pancreatic fluid (Figure 5). Visualization of the left limb and body was obscured by gastric and colonic shadowing. Additional abnormalities included a mildly mottled, hyperechoic hepatic parenchyma, moderately decreased renal architecture and mildly thickened small intestines. A gastrointestinal (GI) panel revealed decreased cobalamin, normal folate and increased feline pancreas-specific lipase (Spec fPL) (Table 1). Maropitant and mirtazapine were prescribed, and a surgical consultation was recommended to address the obstruction.

Preoperative ventrodorsal thoracic radiograph. Multiple, various sized, mineral opacities are seen in the cranial abdomen
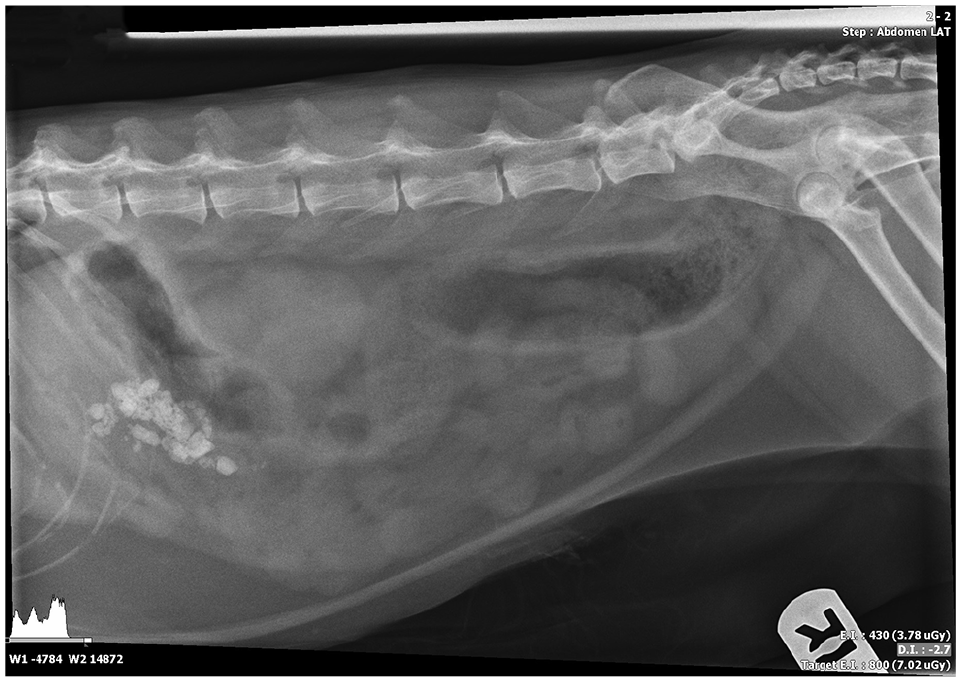
Preoperative right lateral abdominal radiograph. Multiple, various sized, mineral opacities are visible ventral to the stomach
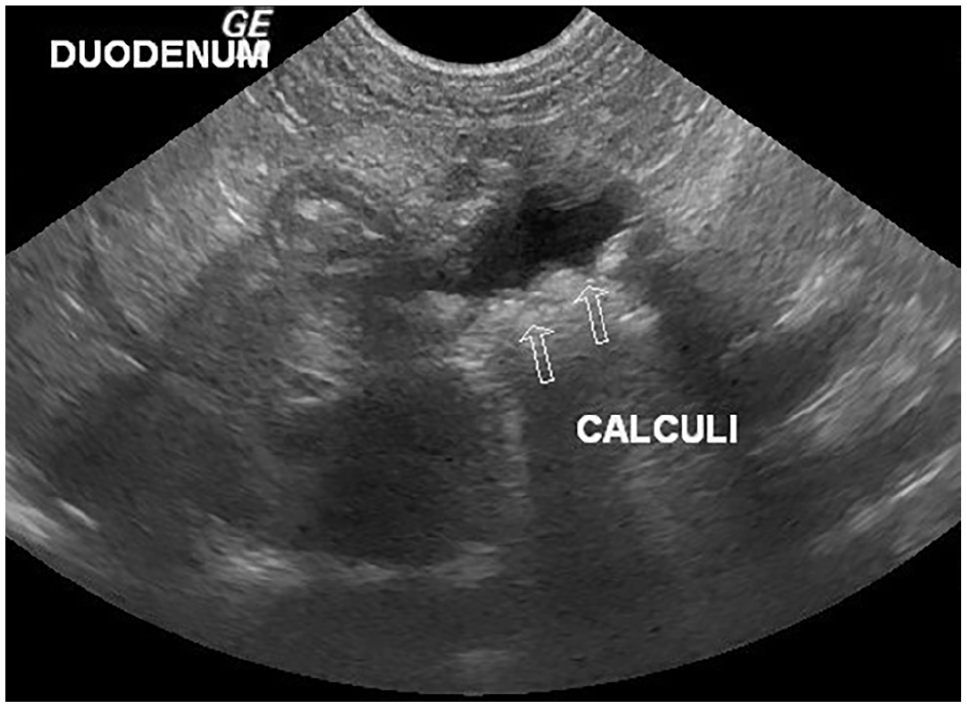
Abdominal ultrasound image of the right limb of the pancreas containing calculi characterized by multiple hyperechoic, shadowing structures (pancreatic calculi)

Abdominal ultrasound image depicts the markedly dilated pancreatic duct filled with anechoic fluid with rounded hyperechoic, shadowing structures (pancreatic calculi)
Gastrointestinal panel values (IDEXX)

B12 = vitamin B12; Spec fPL = feline pancreas-specific lipase
Abnormal value
As a result of limited information regarding the management of obstructive pancreatolithiasis, the owners were presented with two surgical options: (1) extracorporeal shockwave lithotripsy (ESWL) with endoscopic evaluation; or (2) abdominal exploration with comprehensive GI biopsy series (stomach, duodenum, jejunum, ileum, mesenteric lymph node and pancreas), duodenal papillae assessment, pancreatic duct evaluation, stone removal, if feasible, and potential stent placement. The owners elected the second option. Preoperative CBC and biochemistry (day 63) showed persistent mild anemia and the patient’s weight at surgery was 5.70 kg (Figure 1). A heart murmur was deemed innocent on echocardiogram, likely due to stress.
Surgical findings documented diffusely atrophied right and left pancreatic limbs with nodular changes. A single, severely dilated pancreatic duct, measuring approximately 1 cm, was observed coursing through both limbs containing numerous, palpable, mobile, intraluminal stones. Further investigation through an anti-mesenteric duodenotomy confirmed the patency of the major duodenal papilla, which allowed grossly normal bile to flow freely. However, attempts to cannulate the minor duodenal papilla, both normograde and retrograde, were unsuccessful. A vertical incision made along the dilated accessory pancreatic duct allowed for the extraction of smooth, pale, white stones, though not all could be removed. An intraductal swab sample was obtained for culture. Cannulation of the minor duodenal papilla remained unfeasible; therefore, a 20 G over-the-needle catheter was inserted normograde through the incision made into the dilated duct and into the duodenal lumen. A wire was passed through the catheter, followed by positioning of a 2.5 Fr double pigtail ureteral stent through the newly established minor duodenal papilla and into the pancreatic duct of the right limb, partially extending into the left limb (Figure 6). The stent was sutured within the pancreatic duct with a single 5-0 polypropylene encircling suture and within the duodenal lumen with three separate 5-0 polypropylene-encircling sutures. The duodenotomy was closed with 3-0 polydioxanone in a simple interrupted pattern and the pancreatic ductal incision was closed with 5-0 polypropylene in a simple continuous pattern. Full-thickness GI series and liver biopsies were performed. Postoperative radiographs confirmed appropriate stent placement and remaining calculi in the pancreatic ducts (Figures 7 and 8).

Schematic representation of the surgical technique used to place the double pigtail ureteral stent. (a) A 20 G over-the-needle catheter was inserted normograde through the incision at the dilated accessory pancreatic duct. (b) A wire was passed through the catheter. (c) A 2.5 Fr double pigtail ureteral stent was passed over the wire and guided through the newly established minor duodenal papilla and into the pancreatic duct. (d) The stent was sutured in place within the pancreatic duct and within the duodenal lumen; the duodenal and pancreatic ductal insertions were then sutured closed. A = major duodenal papilla; B = minor duodenal papilla and site of obstruction; C = duodenotomy; D = incision into the accessory pancreatic duct; E = over-the-needle catheter

Postoperative right lateral abdominal radiograph. Multiple, various sized, mineral opacities (pancreatoliths) are visible ventral and caudal to the stomach. The double pigtail ureteral stent is visible in the cranial to mid-abdomen

Postoperative ventrodorsal abdominal radiograph. The double pigtail ureteral stent is visible in the cranial, mid-abdomen, extending to the right lateral abdomen. Numerous mineral opacities (pancreatoliths) of varying sizes can be observed in the cranial abdomen
Postoperatively, a tapering fentanyl continuous rate infusion (4 µg/kg/h IV) for analgesia, maropitant (1 mg/kg IV q24h) and dolasetron (0.5 mg/kg IV q12h) for nausea, ampicillin-sulbactam (22 mg/kg IV q8h, Unasyn, Pfizer) and a crystalloid solution (45 ml/kg/day IV, Plasma-Lyte; Baxter International) were given. The patient was discharged within 48 h given clinical improvement with a healthy appetite and sent home with buprenorphine (0.015 mg/kg PO q8–12h), amoxicillin-clavulanate (13 mg/kg PO q12h), mirtazapine (0.6 mg/kg PO q72h), maropitant (1.4 mg/kg PO q24h) and cobalamin (250 µg/cat PO q24h). A broad-spectrum antibiotic was prescribed postoperatively and continued upon discharge to minimize surgical risks and prevent ascending pancreatic infections, particularly those related to the stones acting as a nidus.
Histopathology of the pancreatic biopsy revealed severe atrophy and moderate lymphoplasmacytic, neutrophilic and eosinophilic interstitial pancreatitis with fibrosis, consistent with the history of pancreatic ductular lithiasis. Mild triaditis, characterized by mild portal hepatitis and chronic enteritis, was also observed from the GI and liver biopsy samples. Pancreatic duct culture identified Pasteurella species and two strains of Actinomyces species, susceptible to all antibiotics with no anaerobic organisms isolated. Pancreatolith analysis reported 100% calcium carbonate.
Two weeks postoperatively (day 78), the patient demonstrated notable weight gain to 6.14 kg, an increase of nearly 8% (Figure 1). At the 4-week follow-up (day 92), the patient was thriving, with no reported concerns. A recheck abdominal ultrasound revealed remaining pancreatoliths, persistent pancreatic duct dilation and an in-place stent. A recheck GI panel revealed an adequate cobalamin level, normal folate and persistently elevated Spec fPL (Table 1). At the 12-week recheck (day 149), an increased weight at 6.68 kg (an increase of over 17%) (Figure 1) and unremarkable CBC and biochemistry were noted. The patient was euthanized 3 months before the 24-month mark owing to an unspecified illness; however, the owner reported an overall excellent outcome and quality of life.
Discussion
Feline pancreatolithiasis has been documented in only six cases. Although the etiology remains poorly understood, five of these cases involved chronic pancreatitis.7 –12 This is a presumed similarity to the current case as Spec fPL was not checked until day 55. In humans, pancreatolithiasis is a direct sequela of chronic pancreatitis,2,5 suggesting a potential association in cats.
Abdominal exploratory surgery with pancreatolith removal to resolve obstruction was performed in 3/6 feline cases, but only one survived to a 2-year follow-up. The patients were euthanized in the three cases where surgical intervention was not elected.7 –12 Treatment modalities for obstructive pancreatolithiasis in humans encompass endoscopic retrograde cholangiopancreatography (ERCP) with stone extraction, ESWL, surgical drainage and resection, and stone dissolution. ERCP is preferred for stones measuring ⩽5 mm, while ESWL with endoscopy is recommended for stones ⩾5 mm in size. 6 In small animals, advancements such as laser lithotripsy for various calculi suggest its potential applicability to pancreatolith treatment. 18 Pancreaticoduodenostomy has been successfully performed in a cat to remove pancreatic abscesses, resulting in long-term survival. 19 Thus, pancreaticoenteric anastomosis could also be a viable option for managing obstructive pancreatolithiasis in cats.
In feline cases, pancreatoliths were composed of 100% calcium carbonate, except for one case with a 50:50 mixture of calcium oxalate monohydrate and calcium phosphate.1 –6 This mirrors human cases where downregulation of pancreatic stone protein leads to increased calcium carbonate in pancreatic fluid, precipitating onto an amorphous nidus.2,6 Moreover, one theory posits that partial obstruction of pancreatic ducts and fluid stagnation during chronic pancreatitis contribute to stone formation. Experimental evidence shows that pancreatic calculi were found in 46.7% of dogs with partial duct obstructions, whereas none were observed in dogs with complete obstruction. 13 Our patient had a partial obstruction and a non-patent minor duodenal papilla, corroborating this hypothesis.
Most cats (80%) have a single pancreatic duct that merges with the common bile duct before entering the duodenum at the major duodenal papilla. However, our patient had a patent major pancreatic duct and an obstructed minor duodenal papilla. The clinical impact is not entirely understood. It is possible the anatomical variation in the accessory pancreatic duct in this patient resembles that of a dog, where it transports the majority of pancreatic secretions to the duodenum. 20
Histopathology showed an expected mild triaditis, given pancreatitis in cats is often associated with concurrent endocrine, GI, renal and immune-mediated diseases. 21 Furthermore, the pancreatic atrophy, fibrosis, and lymphocytic and plasmacytic infiltration of the small intestinal lamina propria may indicate exocrine pancreatic insufficiency, potentially explaining our patient’s chronic weight loss and/or failure to gain weight.7,9,10,12 Intraoperatively, the pancreas appeared diffusely atrophied, corroborating the histopathological findings. The right pancreatic limb appeared enlarged on ultrasonographic examination, which remains unexplained and may be subjective because of difficulties delineating the pancreas from the surrounding mesentery.
Hematological and biochemical findings are often non-specific, and tests such as serum amylase, lipase and Spec fPL have debatable sensitivity for diagnosing pancreatitis, particularly with hepatic or intestinal comorbidities. Our patient’s bloodwork exhibited elevated Spec fPL, indicative of pancreatitis, and low cobalamin, suggesting ileal malabsorptive disease. 22 Persistent mild anemia, likely anemia of chronic disease and/or inflammation, along with lymphopenia and mild hyperglycemia, was also noted, likely due to stress. In addition, our patient’s chronic vomiting was consistent with chronic enteropathy and pancreatitis.
This case marks the first documented use of a locking loop catheter to re-establish a pancreatic duct in obstructive pancreatolithiasis. The double pigtail ureteral stent was chosen for its durability and suitability for permanent placement, made from polyurethane to ensure biocompatibility. 23 Originally intended for ureteral use, this has since expanded to include successful applications in endoscopic gallbladder stenting in humans and the drainage of non-resolving pancreatic pseudocysts in children.24,25
Pancreatolithiasis should be considered a potential differential diagnosis in feline patients with recurrent pancreatitis and a history of progressive weight loss. Surgical treatment is currently recommended in feline patients, although ESWL remains a viable option despite limited available data. Prognosis and survival rates are guarded and highly dependent on the patient’s stability at presentation, disease chronicity and comorbidities.
Conclusions
To the authors’ knowledge, this case represents a novel approach to treating obstructive pancreatolithiasis in cats by employing a double pigtail ureteral stent. Furthermore, this case contributes to the notion that pancreatolithiasis can manifest in cats with chronic pancreatitis and adds to the theory of the formation of these stones.
Footnotes
Acknowledgements
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.