
Abstract
Objectives
Pancreatitis is a frequent disease in cats for which the ante-mortem diagnosis remains challenging. Feline pancreatic lipase immunoreactivity (fPLI) has been reported to have a high sensitivity for the diagnosis of pancreatitis. The aim of this study was to compare the rapid in-house test SNAP fPL with the standard test Spec fPL and to evaluate the use of SNAP fPL to diagnose pancreatitis in an emergency setting.
Methods
fPLI of 111 cats with a clinical suspicion of pancreatitis was measured with both SNAP fPL and Spec fPL. Furthermore, clinical signs, haematological and biochemical changes, and abdominal ultrasound findings were recorded.
Results
Seventy-eight of 111 cats (70.3%) were tested below the cut-off level for pancreatitis with SNAP, as well as Spec fPL, whereas 21/111 (18.9%) were tested with values above the cut-off level with both tests. In 12/111 (10.8%) cats the results were discordant. The comparison of both tests revealed an agreement of 78/80 (97.5%) when Spec fPL was ⩽3.5 μg/l (negative) and 18/20 (90%) when Spec fPL was ⩾5.4 μg/l (positive). The most common clinical signs in cats with suspected pancreatitis (n = 21) were lethargy (95.2%), reduced appetite and vomiting (90.5% each), dehydration (81.0%), diarrhoea (57.1%), abdominal pain and weight loss (47.6% each). Hyperglycaemia and hyperbilirubinaemia (85.7% each), increased aspartate transaminase (76.2%) and alanine transaminase (47.6%), leucocytosis (61.9%), lymphopenia (57.1%), decreased sodium and chloride (57.1% each), and increased urea (52.4%) were the most common abnormalities in blood work.
Conclusions and relevance
Clinical signs, as well as routine blood-work changes, were non-specific and thus proved to be insufficient to diagnose pancreatitis. The combination of SNAP fPL and subsequent Spec fPL, if indicated, provided the opportunity to rule out or to diagnose pancreatitis with a higher certainty than previously known test methods. This study proved SNAP fPL to be a valuable tool to exclude or include pancreatitis in an emergency setting.
Keywords
Introduction
Pancreatitis is the most common disorder of the exocrine pancreas in cats and is clinically important in this species.1,2 Despite that fact, the pathophysiology is poorly understood and its aetiology remains unknown in the majority of cases. 3 Furthermore, clinical signs are often non-specific hence its diagnosis remains challenging.2,4
Strictly speaking, pancreatitis refers to inflammation (ie, infiltration with inflammatory cells) of the exocrine pancreas. However, the term pancreatitis is commonly expanded to also include diseases of the exocrine pancreas characterised mainly by necrosis (necrotising pancreatitis) or irreversible structural changes such as fibrosis (chronic pancreatitis [CP]), sometimes with only minimal inflammatory component. 4 CP lesions in cats resemble CP in people, with fibrosis being more prominent than inflammatory changes. 1 Cystic degeneration gradually increases as other lesions of CP become more prominent. Histologically, acute pancreatitis (AP) consists of neutrophilic inflammation associated with interstitial oedema and necrosis of mesenteric fat. In the cat, there is often some overlap between the acute and chronic forms of feline pancreatitis.1,2 In 115 cats presented for necropsy, irrespective of the cause of death, 1 an overall prevalence of 67% of pancreatic changes was identified (45% in clinically normal animals). CP was found in 60% of the pancreases (50% CP only), with a significant correlation between age and occurrence of CP. AP was present in 16% (6% AP only).
Diagnosing feline pancreatitis ante-mortem remains a challenge for the clinician.2,4 This difficulty has multiple origins, which include the undefined aetiology, often mild and non-specific clinical signs,1,5 poor sensitivity and specificity of most of the imaging or clinicopathological findings,6,7 frequent concomitant disorders and difficulty in obtaining or interpreting biopsy samples. 2 In addition, sensitive and specific tests for the diagnosis of feline pancreatitis were, until recently, not available. Serum amylase and serum lipase activities have been evaluated in both experimental and spontaneous feline pancreatitis showing non-specific increases associated with liver,8,9 renal or other gastrointestinal diseases. Results of clinical studies suggest that these two traditional tests, which are not specific for pancreas, are of no clinical value in cats and should not be used for the diagnosis of feline pancreatitis.3,6 However, moderate-to-good sensitivity and specificity of lipase has been reported for the diagnosis of feline pancreatitis using the 1,2-o-dilauryl-rac-glycero-3-glutaric acid-(6’-methylresorufin) ester (or DGGR-lipase) assay. 10
Feline pancreatic lipase immunoreactivity (fPLI) is a species-specific immunoassay that became available some years ago. 11 In contrast to the traditional catalytic assays for serum lipase activity, which indiscriminately measure the activity of lipases of any origin (eg, pancreatic, gastric, duodenal), fPLI specifically measures pancreatic lipase and thus it is specific for pancreatic disease. Studies in cats with spontaneous and experimental pancreatitis have shown that fPLI is very sensitive for moderate to severe pancreatitis,12,13 being superior to the sensitivities of feline trypsin-like immunoreactivity (fTLI) and abdominal ultrasound. IDEXX provides two different tests to measure fPLI. Spec fPL is a quantitative test performed in reference laboratories. Based on the same concept, SNAP fPL is a semi-quantitative rapid in-house test available for practitioners and reveals a ‘normal’ (⩽3.5 μg/l) or ‘abnormal’ (>3.5 µg/l) test result.
The aim of this study was to compare the rapid in-house test SNAP fPL with the standard test Spec fPL and to evaluate the use of the SNAP fPL to diagnose pancreatitis in an emergency setting.
Materials and methods
Animals
All cats with a clinical suspicion of pancreatitis admitted to the Veterinary Teaching Hospital of the University of Leipzig between June 2011 and March 2012 entered the study. The prospective study protocol included signalment (sex, breed and age) as well as body weight at time of presentation, history and physical examination, blood work, abdominal ultrasound, SNAP fPL and Spec fPL, and follow-up.
History and physical examination
Investigated clinical signs included diarrhoea, vomiting, reduced appetite, lethargy, abdominal pain, dehydration, jaundice, fever or hypothermia and weight loss. Furthermore, historic or present co-occurring diseases were evaluated.
Blood work
Blood samples were taken for all patients mostly at presentation, but always within 24 h. We would like to note that data presentation and discussion is limited to cats with diagnosed pancreatitis. A complete blood count (CBC) with differential was performed. The analysis included haematocrit, number of leukocytes, neutrophilic granulocytes (with potential left shift), eosinophilic granulocytes, monocytes, lymphocytes and thrombocytes. The measurements were performed on the following machines: ProCyte (IDEXX Vet Med Labor), pocH-100 iv Diff (Sysmex) or Vet abc (Scil), and were manually checked in most cases.
The chemistry profile included the following parameters: total protein and albumin, glucose, urea, creatinine, alkaline phosphatase, alanine transaminase (ALT), aspartate transaminase (AST), total bilirubin and electrolytes (Na, K, Ca, P). These measurements were performed on a Fuji Dri Chem 3500i (Scil).
SNAP fPL and Spec fPL
The serum concentration of fPLI of all cats was measured with SNAP fPL in-house and with Spec fPL at IDEXX. Both values were measured within 24 h of presentation and within the same blood sample. The semi-quantitative SNAP fPL can only distinguish between normal and abnormal results, whereas Spec fPL differentiates between negative (⩽3.5 μg/l), increased (3.6–5.3 μg/l) and positive (⩾5.4 μg/l) values.
Abdominal ultrasound
Abdominal ultrasound was performed within 24 h on a Logiq E9 (GE Healthcare) if possible. In some cases (emergency situation, no specialist in house, etc) ultrasound was performed at a later stage; however, these results (>24 h after presentation) were not considered owing to the possible influence of symptomatic therapy. The following parameters were considered indicative for pancreatitis: enlargement of the pancreas, peripancreatic fluid accumulation, heterogenicity with increased (fibrosis) or decreased (necrosis) echogenicity and increased echogenicity in the surrounding mesentery (adiponecrosis).
Retrospective classification
Depending on their history, physical examination, clinical signs, blood work, abdominal ultrasound and follow-up, the cats were retrospectively assigned to four different groups with regard to the probability of having pancreatitis, as described previously. 14 Group I included cats with negative SNAP and Spec fPL results and no evidence for pancreatitis otherwise (eg, in abdominal ultrasound). Group II included cats with clinical signs similar to pancreatitis, but suspicion was not confirmed by SNAP and/or Spec fPL, abdominal ultrasound and/or follow-up. Group III included cats with clinical signs fitting to pancreatitis and confirmed by SNAP fPL and/or Spec fPL, abdominal ultrasound and/or follow-up (minimum three points indicating pancreatitis). Group IV included cats with conflicting results, where diagnosis was unclear (eg, pancreatitis possible owing to clinical signs and/or ultrasound, but SNAP and Spec fPL negative).
Statistical analysis
Agreement of SNAP fPL and Spec fPL was calculated with Cohen’s kappa (κ).
Results
Animals
A total of 111 cats with an initial suspicion of pancreatitis were entered in the study. Most cats were domestic shorthairs (n = 92; 82.9%). Furthermore, six Persians, four crossbreeds, three Maine Coons, two Birmans and one each of Chartreux, British Shorthair, Thai and Siberian Forest Cat completed the study population. Male cats were over-represented [72 (64.9%; 54 castrated, 18 intact)], whereas only 39 females (35.1% [26 castrated, 13 intact]) were included. Age ranged from 4 months to 17.6 years (median 7.25 years).
SNAP fPL and Spec fPL
Seventy-eight of 111 cats (70.3%) were tested as normal with SNAP fPL, as well as Spec fPL, whereas 21/111 (18.9%) were tested as elevated with both tests. In 12/111 (10.8%) of the cats, results of the two tests were discordant (Figure 1). The comparison of both tests revealed an agreement of 78/80 (97.5%) when Spec fPL was ⩽3.5 μg/l (negative) and 18/20 (90%) when Spec fPL was ⩾5.4 μg/l (positive) (Table 1). In the cases where the Spec fPL level was 3.6–5.3 μg/l, only 3/11 (27.3%) had an abnormal SNAP fPL result, whereas 8/11 (72.7%) were tested normal. Evaluating both abnormal Spec fPL intervals together (⩾3.6 μg/l), only 21/31 (67.7%) showed an abnormal SNAP fPL. The calculation of Cohen’s κ revealed a high accordance of the two tests with a value of 0.6524.

SNAP fPL followed by Spec fPL results of all 111 cats tested. SNAP fPL levels are abnormal if the colour intensity of the sample spot is equal to or darker than the colour intensity of the reference spot, and normal if the sample spot is lighter than the reference spot. Spec fPL differentiates between negative (⩽3.5 μg/l), increased (3.6–5.3 μg/l) and positive (⩾5.4 μg/l) values
Results of SNAP fPL vs Spec fPL of all 111 cats tested
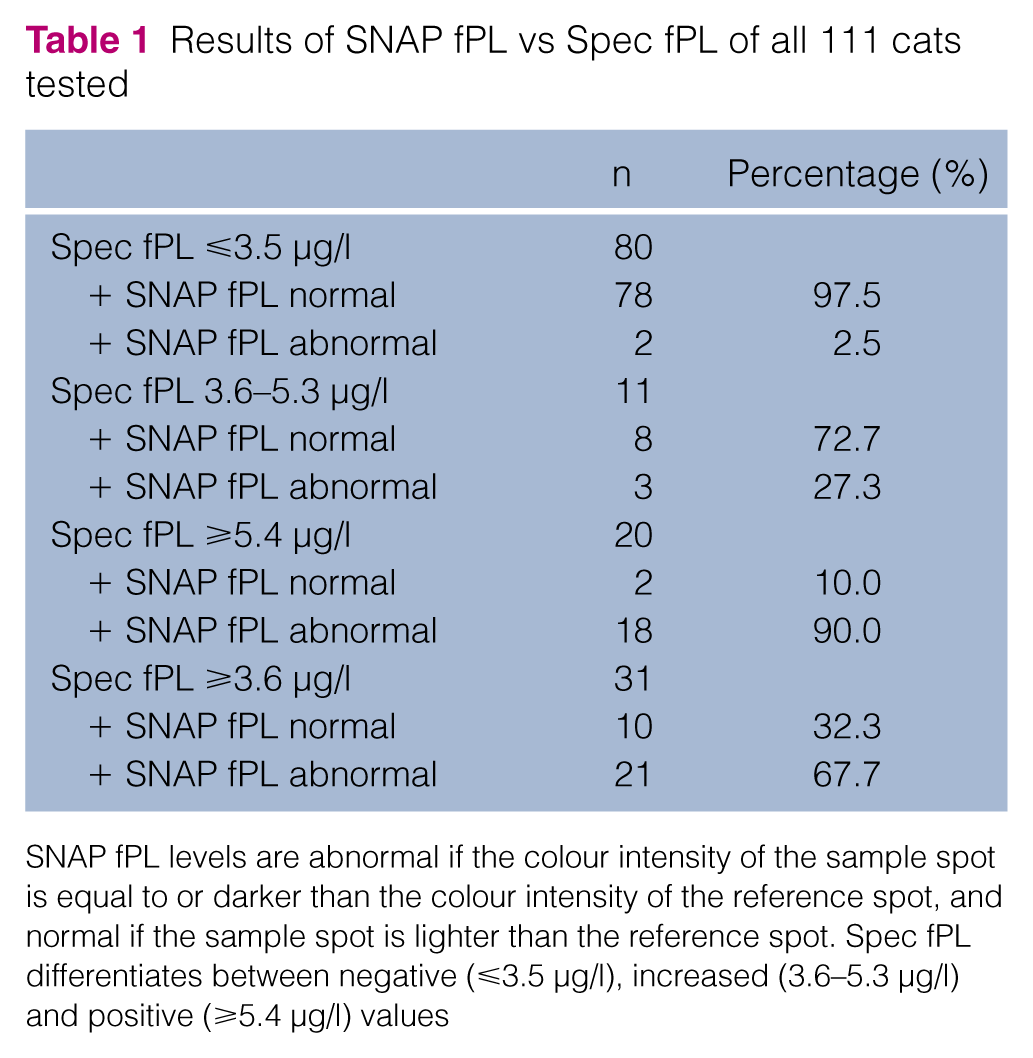
SNAP fPL levels are abnormal if the colour intensity of the sample spot is equal to or darker than the colour intensity of the reference spot, and normal if the sample spot is lighter than the reference spot. Spec fPL differentiates between negative (⩽3.5 μg/l), increased (3.6–5.3 μg/l) and positive (⩾5.4 μg/l) values
Retrospective classification: group I
Twelve cats (10.8%) were negative with SNAP as well as Spec fPL, and displayed generally no evidence for pancreatitis (group I). In two of these cases abdominal ultrasound was performed. Owing to their low probability of pancreatitis, cats in this group were not investigated further.
Retrospective classification: group II
Seventy-four cats (66.7%) were assigned to group II, with clinical signs similar to pancreatitis, but suspicion was not confirmed by SNAP and Spec fPL, abdominal ultrasound (12 cats) or follow-up (Figure 2). Most cats in this group were domestic shorthairs (n = 62 [83.8%]). Furthermore, four Persians, three crossbreeds and one each of Maine Coon, Birman, Chartreux, British Shorthair and Thai completed this group. Forty-five (60.8%) were male (36 castrated, nine intact) and 29 were female (39.2%; 19 spayed and 10 intact). The median age in this group was 7.7 years (range 4 months to 15 years) with a median body weight of 5.0 kg (range 1.9–11.2 kg). For 62/74 (83.8%) cats, SNAP fPL and Spec fPL yielded normal results (Figure 2). The remaining 12/74 (16.2%) cats had discordant results with normal SNAP fPL but elevated Spec fPL between 3.6 and 5.3 µg/l, making up for most of these discordant results (n = 8/12).

SNAP fPL followed by Spec fPL results for cats in group II (clinical signs similar to pancreatitis but suspicion not confirmed) and group III (suspicion of pancreatitis). SNAP fPL levels are abnormal if the colour intensity of the sample spot is equal to or darker than the colour intensity of the reference spot, and normal if the sample spot is lighter than the reference spot. Spec fPL differentiates between negative (⩽3.5 μg/l), increased (3.6–5.3 μg/l) and positive (⩾5.4 μg/l) values
Retrospective classification: group III
According to their history, physical examination, clinical signs, blood work, abdominal ultrasound (13 cats) and follow-up, 21 cats (18.9%) were retrospectively assigned to group III with a very high probability of having pancreatitis (Figure 2). Besides two Maine Coons and one Persian, all cats in this group were domestic shorthairs (n = 18 [85.7%]). Seventeen (81.0%) were male (13 castrated, four intact) and four were female (19.0%; three spayed and one intact). The median age in this group was 9.4 years (range 2 months to 17.6 years) with a median body weight of 4.9 kg (range 2.5–8.4 kg). For 20/21 (95.2%) cats, SNAP fPL and Spec fPL yielded abnormal results ⩾3.6 μg/l (Figure 2). Only one cat yielded a normal SNAP fPL but an elevated Spec fPL ⩾5.4 μg/l.
Clinical signs in group III
Typical clinical signs in the cats with a high suspicion of having pancreatitis (group III; out of history and physical examination) were lethargy (95.2%), reduced appetite and vomiting (90.5% each) and dehydration (81.0%). The results are summarised in Table 2.
Clinical signs of 21 cats with a suspicion of pancreatitis (group III)

Blood work in group III
The most important changes found in the CBCs of the cats in group III were leucocytosis (13/21 [61.9%]) and lymphopenia (12/21 [57.1%]).
With regard to the chemistry profile, the most prominent abnormalities in the cats of group III were hyperglycaemia and hyperbilirubinaemia (18/21 [85.7% each]), increased AST (16/21 [76.2%]) and ALT (10/21 [47.6%]), hyponatraemia and hypochloraemia (12/21 [57.1% each]), as well as increased urea (11/21 [52.4%]). The results are summarised in Table 3.
Changes in blood work and blood chemistry of 21 cats with a suspicion of pancreatitis (group III)
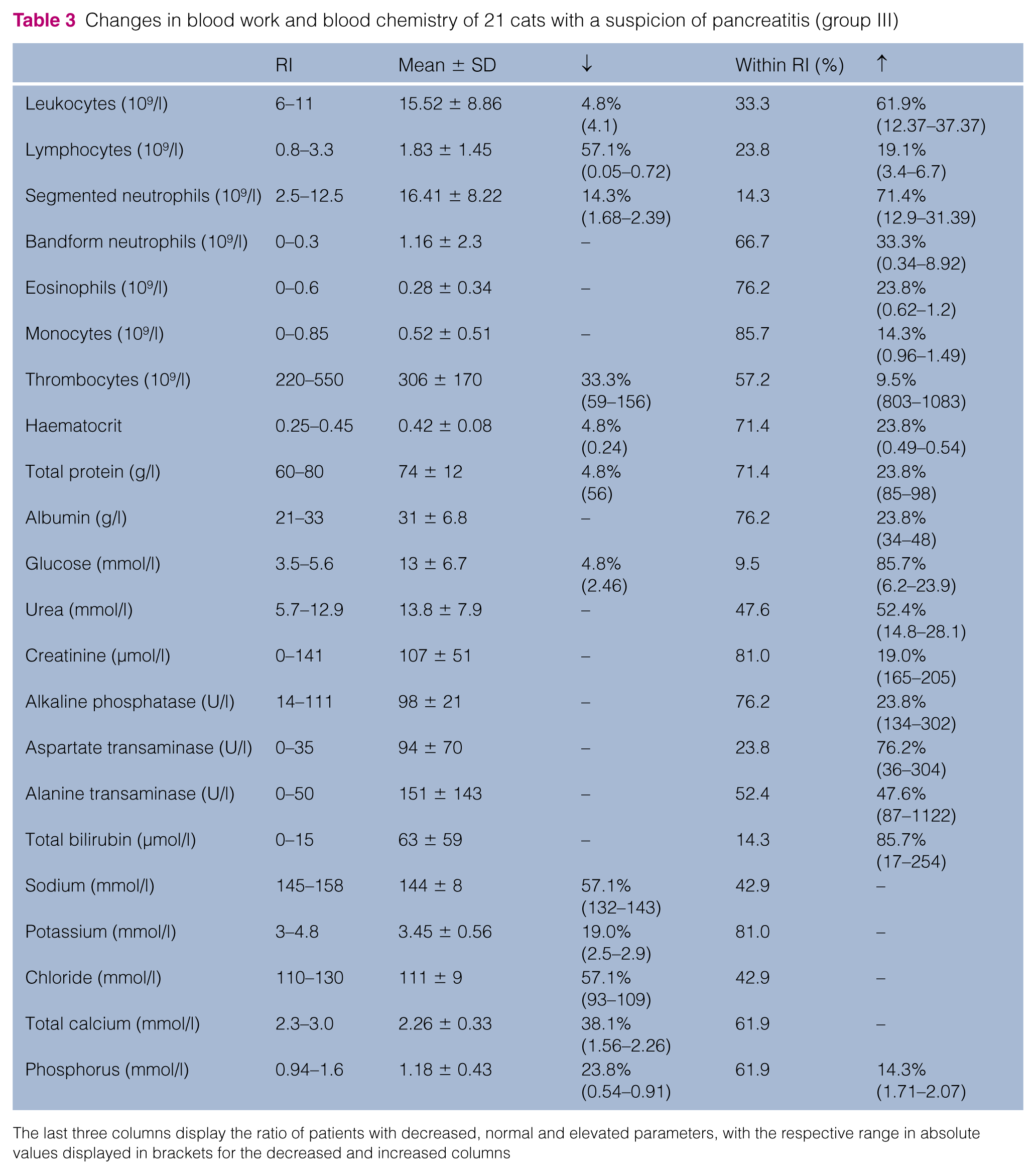
The last three columns display the ratio of patients with decreased, normal and elevated parameters, with the respective range in absolute values displayed in brackets for the decreased and increased columns
Abdominal ultrasound in group III
In 13 patients an abdominal ultrasound was performed leading to an ultrasonographic diagnosis of pancreatitis in seven cats (53.8%). Decreased echogenicity of the pancreatic tissue, enlargement of the pancreas and increased echogenicity of the surrounding mesentery (adiponecrosis) were the most prominent findings. In five cats, there was nothing abnormal detected in ultrasonography and one pancreas could not be evaluated sufficiently. Furthermore, additional cholecystitis was found in two and cholestasis of the cystic duct and choledochus in one cat. Two cats had ascites.
Retrospective classification: group IV
In four cats (3.6%), pancreatitis could not be excluded due to clinical signs and ultrasound (four cases), but SNAP and Spec fPL were negative. Therefore, they were assigned to group IV with an unclear diagnosis. Owing to this, they were excluded from the study.
Discussion
Feline pancreatitis is a common disorder with a rather non-specific clinical, haematological and biochemical manifestation. Abdominal ultrasound is the preferred imaging method to diagnose pancreatitis,3,11 although its sensitivity has been reported to be low in the range of 11–67%.7,11–13
Neither the traditional serum amylase/serum lipase activity2,6,14–16 nor fTLI13,17,18 are sufficient for the diagnosis of feline pancreatitis. SNAP fPL is supposed to enable general practitioners to diagnose pancreatitis more rapidly. In this study, 78/111 cats (70.3%) revealed normal test results in both tests, whereas 21/111 (18.9%) were tested abnormal in SNAP fPL as well as Spec fPL. SNAP fPL and Spec fPL yielded discordant results in only 12/111 (10.8%) cases. Thus, the overall correlation of both tests was 99/111 (89.2%). SNAP fPL correlated best with Spec fPL when results were ⩽3.5 μg/l (97.5%) or ⩾5.4 μg/l (90.0%). These findings correspond approximately to statements of the IDEXX Vet Med Labor (92% and 96%, respectively). 19 For a Spec fPL between 3.6 and 5.3 μg/l, 8/11 (72.7%) cats revealed normal results in SNAP fPL. Where Spec fPL was increased (3.6–5.3 μg/l) and consequently pancreatitis was possible (but not proven), only 3/11 (27.3%) SNAP fPL results were abnormal. Feasible reasons are that SNAP fPL shows a deficiency when measuring a slight increase or that the colour change is subjectively misjudged. However, not every cat with an increased Spec fPL concentration (3.6–5.3 μg/l) had a strong suspicion of pancreatitis. With regard to the cases with a strong suspicion of pancreatitis (group III), only one cat (4.8%) had a false-negative SNAP fPL result (Spec fPL was 6.0 μg/l). An abnormal SNAP fPL result was recorded for 20/21 cats (95.2%) with pancreatitis. Therefore, although the Spec fPL results in the range of 3.6–5.3 μg/l cannot be used as a reliable indicator for pancreatitis, SNAP fPL meets the demand for a reliable and easily performable in-house test. SNAP fPLI revealed an abnormal test result in 100% of the cases with a Spec fPL ⩾7.9 μg/l. Furthermore, in this study a single SNAP fPL Test was considered normal with a Spec fP above the cut-off of 5.4 µg/l (7.4 µg/l). This highlights the advantage of SNAP fPL in severe cases with high Spec fPL.
For the four cases with positive abdominal ultrasound but double-negative SNAP fPL and Spec fPL results (group IV), we were unable to determine whether both fPLI tests were false negative or the ultrasound false positive without histological analysis. Reasons for the mismatch of the commercial tests and ultrasonographic statements can be an indisposition of the pancreas not involving an increase of fPLI (eg, neoplasia, hyperplastic nodules, oedema).3,13 Furthermore, a trauma such as high-rise syndrome can cause ultrasonographic alterations, which persist longer than an increase of the fPLI level. 20 Additionally, other gastrointestinal diseases can develop ultrasonographic evidence consistent with pancreatitis.3,13 Moreover, ultrasonographic aberrances can be a consequence of CP (eg, atrophy, fibrosis) without acute inflammation and release of fPLI at the time of taking blood samples. These deviations support the argument that the sensitivity of fPLI is lower for CP. 3 But even if these cats are considered false negative in SNAP fPL, this study still shows 80.0% (20/25) sensitivity, which is higher than any other single test published to date.
According to the manufacturer, the SNAP fPL is designed to rule out pancreatitis. In our study, 83/86 cats (96.5%) allocated to groups I and II (no pancreatitis) were correctly tested as negative. For 9/74 cats (12.2%) in group II, Spec fPL results between 3.6 and 5.3 μg/l were recorded. According to the manufacturer, a slightly increased Spec fPL simply indicates that pancreatitis is possible. 21 Another potential explanation is that other diseases cause clinical signs and a co-occurring mild pancreatitis leading to a misclassification into group II. Additionally, cats might have a naturally occurring inter-individual variability of their normal fPLI concentration above the reference interval. However, there is still the possibility of false-negative SNAP fPL results. For the 86 cats within groups I and II (no pancreatitis), SNAP fPL was only false positive in three cats (3.5%). Two of these results were negative in Spec fPL (⩽3.5 μg/l), whereas pancreatitis in one of these cats could not be excluded by Spec fPL.
This cat (Spec fPL: 4.7 μg/l; SNAP: abnormal) suffered from hypertrophic cardiomyopathy and hypertension, which was treated successfully. Subsequently, SNAP fPL and Spec fPL tests were repeated, later yielding normal results. The cat with an abnormal Spec fpL (7.4 μg/l; SNAP fPL normal) was euthanased at the owner’s request. It was considered a false positive because necropsy revealed a normal pancreas but a perforated gut.
If practitioners receive an unexpected SNAP fPL result, it is recommended that this measurement is confirmed with Spec fPL and preferably backed up with abdominal ultrasound evaluation. This approach is supported by the data from group II, where three abnormal SNAP fPL test results were corrected by Spec fPL, as well as in group III, where the only SNAP-normal cat was proven to have a pancreatitis with a Spec fPL value ⩾5.4 µg/l. In emergency situations it is recommended that cats are treated symptomatically with infusion, antiemetics and analgesics, etc, until the diagnosis is clear and the treatment can be specifically adapted.
The major shortcoming of our study is that the diagnosis of pancreatitis was almost exclusively based on non-invasive methods and expert opinion. 15 Histological biopsies – the gold standard to diagnose pancreatitis – are needed to evaluate these tests with a higher certainty, but would require extensive clinical studies and owners willing to take biopsies in an already diseased animal. This is, at least in our environment, very difficult to get.
As known from other studies, it is impossible to diagnose feline pancreatitis on the basis of clinical signs, CBC and blood chemistry without any further investigations,6,7,10 as they are very unspecific. The percentages of unspecific lethargy (95.2%) and reduced appetite and vomiting (90.5% each) are even higher than results from another study. 11 Furthermore, dehydration was seen regularly (81.0%) compared with other studies (eg, 92% and 39% 11 ).6,11 Diarrhoea (57.1%) was less common than other clinical signs, which has been shown in previous studies.6,10,11 Abdominal pain was detected in 47.6% of the cats – a value that is higher than in older studies but similar to newer ones.6,10,11 Nevertheless, cats either conceal their pain or pancreatitis is less painful for cats than for dogs and humans. Additionally, the detection of abdominal pain is not only subjective, but also variable owing to different veterinarians on emergency duty seeing the cats.
Similar to other surveys, predispositions concerning breed and body weight were not perceived.1,6 Additionally, the average age of group III (9.4 years) was slightly higher than in group II (7.7 years), which is compatible with older animals that suffer more often from pancreatitis. 20
A higher ratio of males was noticed in the group of cats with pancreatitis (81%); however, the proportion of males was higher in the whole study population (64.7%).
The most common haematological changes associated with pancreatitis were leucocytosis (61.9%) and lymphopenia (57.1%). An increased incidence of hyperglycaemia and hyperbilirubinaemia (85.7% each) and an increase in hepatic enzymes (AST, ALT, alkaline phosphatase) were conspicuous, as in previous studies.6,11 Only 19% of the cats had an increased creatinine; therefore, it is unlikely that kidney disease had an influence on serum lipase level. Electrolyte imbalances (hyponatraemia and hypochloraemia, 57.1% each) were most likely induced by vomiting and anorexia. However, various instruments with various reference intervals were applied owing to cases coming in as emergencies or during day shifts. However, these parameters proved to be rather unspecific to diagnose pancreatitis.
Conclusions
As there is no ante-mortem gold standard to diagnose feline pancreatitis, a combination of history, clinical signs, measurement of pancreatic lipase immunoreactivity and ultrasonography is the most reliable non-invasive procedure to diagnose feline pancreatitis. Clinical signs, as well as routine blood-work changes, were non-specific and thus proved to be insufficient to diagnose pancreatitis. SNAP fPL and Spec fPL have a good agreement, especially when Spec fPL is ⩽3.5 or ⩾5.4 μg/l. The combination of SNAP fPL and subsequent Spec fPL, if indicated, provided the opportunity to rule out or to diagnose pancreatitis with a higher certainty than previously known test methods. This study proved SNAP fPL to be a reliable tool to exclude or include pancreatitis in an emergency setting in-house.
Footnotes
Acknowledgements
We would like to thank Dr Jörg Schnauß for proofreading this manuscript and helpful discussions.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.