
Abstract
Case summary
A 10-year-old spayed female domestic medium hair cat presented after sustaining atraumatic insufficiency fractures of the right calcaneus and the left tibia approximately 6 weeks apart. Chronic alendronate therapy had been ongoing for 9 years for the management of previously diagnosed idiopathic hypercalcemia. The right calcaneal fracture was managed non-operatively due to minimal functional impairment. The left tibial fracture was managed via open reduction and internal fixation with orthogonal plating. Alendronate therapy was discontinued at the time of the fracture repair with prednisolone being used to manage the hypercalcemia. Despite rapid clinical improvement, the tibial fracture had a protracted healing course, with clinical union only being achieved 22 weeks postoperatively. At 17 months postoperatively, the idiopathic hypercalcemia remained well controlled. Gait assessment, orthopedic examination and orthogonal radiographs performed at this time revealed resolution of left pelvic limb lameness, a normal orthopedic examination of the left pelvic limb and no evidence of implant-associated complications. Monitoring is ongoing but at the time of publication, no further fractures have occurred.
Relevance and novel information
As reported in humans, this case report gathers evidence of associations between bisphosphonate treatment and the occurrence of insufficiency fractures in cats, and provides evidence that stress reactions may precede their development. If bisphosphonate therapy is utilized in the long term, serial radiographic monitoring for signs of impending fracture may be warranted. Fracture repair can be successful in cats that have received long-term bisphosphonate therapy, but delayed healing should be anticipated and implant choices made accordingly.
Keywords
Introduction
Bisphosphonate (BP) use in human medicine is widespread; it is highly researched for the treatment of osteoporosis, hypercalcemia of malignancy, bone metastasis and osteogenesis imperfecta.1–3 In veterinary medicine, BPs are gaining favor with treatment for a variety of conditions, including hyperparathyroidism, idiopathic hypercalcemia (IHC), secondary hypercalcemia, tooth resorption and neoplastic bone pain.3–10
BPs are potent osteoclast inhibitors that reduce osteoclast-induced bone resorption and remodeling.1,11 The most widely used BPs are nitrogen-containing, including alendronate, risedronate and zoledronate. These compounds bind to the bone, are endocytosed into osteoclasts and impede metabolic pathways through inhibition of multiple enzymes, predominantly farnesyl diphospate synthase. 12 This metabolic pathway constraint disrupts osteoclast activities involved in bone resorption. 12 Osteoclast apoptosis may also occur but is not required for inhibition of bone resorption.13,14
Of the reported adverse effects from BP use within the human literature, atypical stress fractures or insufficiency fractures have received the most attention.15–26 Insufficiency fractures occur in the absence of trauma when physiological stresses are placed on abnormal bones,27,28 while the term stress fracture is reserved for injuries sustained when repetitive forces act upon normal bone.29,30 Other potential complications from BP use in humans include jaw osteonecrosis,31–34 musculoskeletal pain, 35 atrial fibrillation36–38 and esophageal erosion/irritation. 2 In veterinary medicine, most BP use is transient so many of the side effects appreciated in humans have not been noted. However, the long-termuse of BP therapy has been associated with bilateral atypical patellar fractures in one cat 7 and jaw osteonecrosis.9,39
This case report describes atypical fractures sustained in the absence of trauma in a cat prescribed alendronate for the control of IHC. This is only the second reported case of BP-associated fracture in a cat and the first where surgical stabilization and long-term follow-up are reported.
Case description
A 10-year-old spayed female domestic mediumhair cat was referred for investigation of a 2-month history of right pelvic limb lameness with no inciting trauma. The cat had previously been diagnosed with IHC at the age of 1 year based on a history of sustained hypercalcemia and an absence of salient findings after an appropriate diagnostic work-up. Prednisolone and alendronate were prescribed for management, levels of which were titrated over time based on ionized calcium levels; the last documented period of hypercalcemia was 3 years after the diagnosis of IHC. Current medications consisted of alendronate (10 mg/week), prednisolone (2.5 mg q24h) and gabapentin (100 mg q8h).
On physical examination, the cat had a moderate weightbearing right pelvic limb lameness with moderate tarsal hyperflexion. The right hock had a normal range of motion with mild palpable crepitus. Orthogonal radiographs of both tibiae and tarsi were performed, revealing a complete transverse right calcaneal body fracture with mild displacement and moderate sclerosis of the fracture ends; there was minimal activity at the fracture site (Figure 1). Although surgical stabilization was recommended, due to perceived improvement over time, the owner elected to trial non-surgical management.

Mediolateral and dorsoplantar radiographs of both tarsi
Six weeks later, the cat re-presented for an acute onset non-weightbearing lameness of the left pelvic limb, again with no inciting trauma. Gait analysis confirmed non-weightbearing lameness on the left and mild weightbearing lameness of the right pelvic limb with persistent tarsal hyperflexion. Orthopedic examination revealed swelling and instability at the level of the proximal left tibia. Orthogonal radiographs of both tibiae revealed a complete transverse fracture of the left proximal tibial metaphysis and fibula (Figure 2a). The fracture of the right calcaneus remained static with a persistent fracture line, sclerosis and minimal activity (Figure 2b). Surgical stabilization of the tibial fracture was elected. Complete bloodwork showed no significant findings with the exception of a mild total hypocalcemia (8.2 mg/dl, reference interval [RI] 9.1–10.7), ionized calcium (5.5 mg/dl, RI 5.1–6.0) and phosphorous (5.3 mg/dl, RI 2.7–5.7) were within normal limits.

Mediolateral and craniocaudal radiographs of both tibiae
Open reduction and internal fixation via a medial approach 40 was undertaken. A 1.5 mm six-hole locking compression plate (LCP) (DePuy Synthes) was placed cranially and was used to reduce the fracture. A 1.5/2.0 mm split-T seven-hole LCP (DePuy Synthes) was then placed medially. Postoperative radiographs showed anatomic alignment, near-anatomic reduction and appropriate implant placement (Figure 3a and ai). While bone biopsy was considered, as this was not considered likely to impact on therapeutic recommendations, it was not performed due to the brittle nature of the bone and the paucity of bone stock available for repair. Postoperatively, analgesia was managed with methadone (0.2 mg/kg IV q6h) while hospitalized. The cat was discharged the next day with instructions for cage rest, amantadine for additional analgesia (2.9 mg/kg PO q24h) and continuation of current medications (prednisolone 2.5 mg q24h, gabapentin 100 mg q8h), with the exception of alendronate, which was discontinued.

Mediolateral and craniocaudal radiographs of the left tibia taken (a and ai) immediately postoperatively, (b and bi) 4 weeks postoperatively, (c and ci) 8 weeks postoperatively, (d and di) 14 weeks postoperatively, (e and ei) 22 weeks postoperatively and (f and fi) 17 months postoperatively. (a,ai) Immediately postoperatively, anatomic alignment and near-anatomic reduction have been achieved. Implant placement is appropriate with a 1.5 mm six-hole LCP placed cranially and a 1.5/2.0 mm split-T seven-hole LCP placed medially. (b,bi) At 4 weeks postoperatively, there is minimal evidence of healing at the tibial or fibula fracture sites. Anatomic alignment and near-anatomic reduction have been maintained and there is no evidence of implant-associated complications. (c,ci) At 8 weeks postoperatively, the tibial fracture line is slightly narrower cranially than at the 4-week re-check, and there is evidence of early callus formation caudally and medially. There is also evidence of early remodeling of the fibula fracture. Alignment and apposition have been maintained and implants remain static. (d,di) At 14 weeks postoperatively, there is progressive narrowing of both the tibial and fibula fracture lines when compared with the radiographs taken at 8 weeks postoperatively and evidence of moderate callus formation. Alignment and apposition have been maintained and implants remain static. (e,ei) At 22 weeks postoperatively, clinical union of the tibial fracture has been achieved with no signs of implant-associated complications. There is an oligotrophic nonunion of the fibula. (f,fi) At 17 months postoperatively, radiographs remain static when compared with those taken at 22 weeks postoperatively
Findings at follow-up visits from 4 weeks to 17 months postoperatively are detailed in Table 1. At final follow-up, screening radiographs were performed of the pelvis, both stifles, the right tibia and both tarsi, which revealed no evidence of impending fracture.
Details of follow-up from 4 weeks to 17 months postoperatively, including findings from gait assessment, orthopedic examination, radiography and bloodwork

RI = reference interval

Mediolateral and dorsoplantar radiographs of the right tarsus taken 14 weeks after tibial fracture repair and 28 weeks after calcaneal fracture. There is minimal callus formation, and this is only evident laterally. The fracture ends have become smooth in outline but remain hazy in appearance. This is considered consistent with a viable, oligotrophic non-union
Discussion
Forces are constantly applied to bone with normal activity, which creates microcracks. Bone is constantly remodeling, and therefore these microcracks are repaired in normal tissues. 1 When the balance of bone turnover is compromised, as with BP therapy, this diminishes microfracture healing, which leads to skeletal fragility and fracture formation.2,21 Humans on chronic BP therapy have increased risks of atypical fractures;20,23 these fractures tend to occur at specific locations, most commonly in the subtrochanteric region of the femur, and have distinct characteristics including cortical hypertrophy and a largely transverse configuration. These characteristics are not similar to those seen with other types of pathological fractures, such as those associated with osteoporosis.16,17,19,21,34,41 Based on a previous report 7 and the cat detailed therein, the imbalance of remodeling secondary to chronic BP use may also cause a subset of atypical fractures in cats.
In humans on long-term BP therapy, impending fractures, or stress reactions, can be diagnosed on radiographs, which then progress to a complete fracture. These stress reactions are typically areas of sclerosis or focal increased opacities within the cortex but may also be as subtle as a cortical bulge.18,22 Similar changes have been reported in a cat with a suspected stress fracture of the calcaneus. 42 The cat detailed in this report had radiographs performed of the left tibia as part of a routine work-up for the right calcaneal fracture, 6 weeks before sustaining the left tibial fracture. At that time, no abnormalities were noted associated with the left pelvic limb. Retrospectively, a stress reaction was noted in the proximal cranial cortex of the left tibia, which corresponds with the subsequent site of tibial fracture (Figure 5). As identification of such radiographic features may help predict impending fracture, serial radiographic monitoring of cats on chronic BP therapy may be indicated. The timeline for such monitoring remains uncertain as the accumulation of microdamage leading to fracture takes several years, with microcrack density being linearly related to BP treatment duration. 43 As both cats with BP-related fractures only developed them after 8 years of medication and humans tend to develop them after 3–9 years,17,21,26 monitoring may not need to be started immediately. Obtaining baseline radiographs at the time of commencing therapy and considering annual screening radiographs after 5 years may be a reasonable proposed timeline, with monitoring starting earlier if clinical signs of pain or lameness arise. The half-life of BPs within bone is not currently known in cats, but due to the prolonged half-life in humans (10 years) 44 and dogs (3 years), 45 continued monitoring for several years after stopping therapy may also be indicated. In the cat detailed in this report, radiographic monitoring performed 17 months postoperatively revealed no evidence of stress reaction.
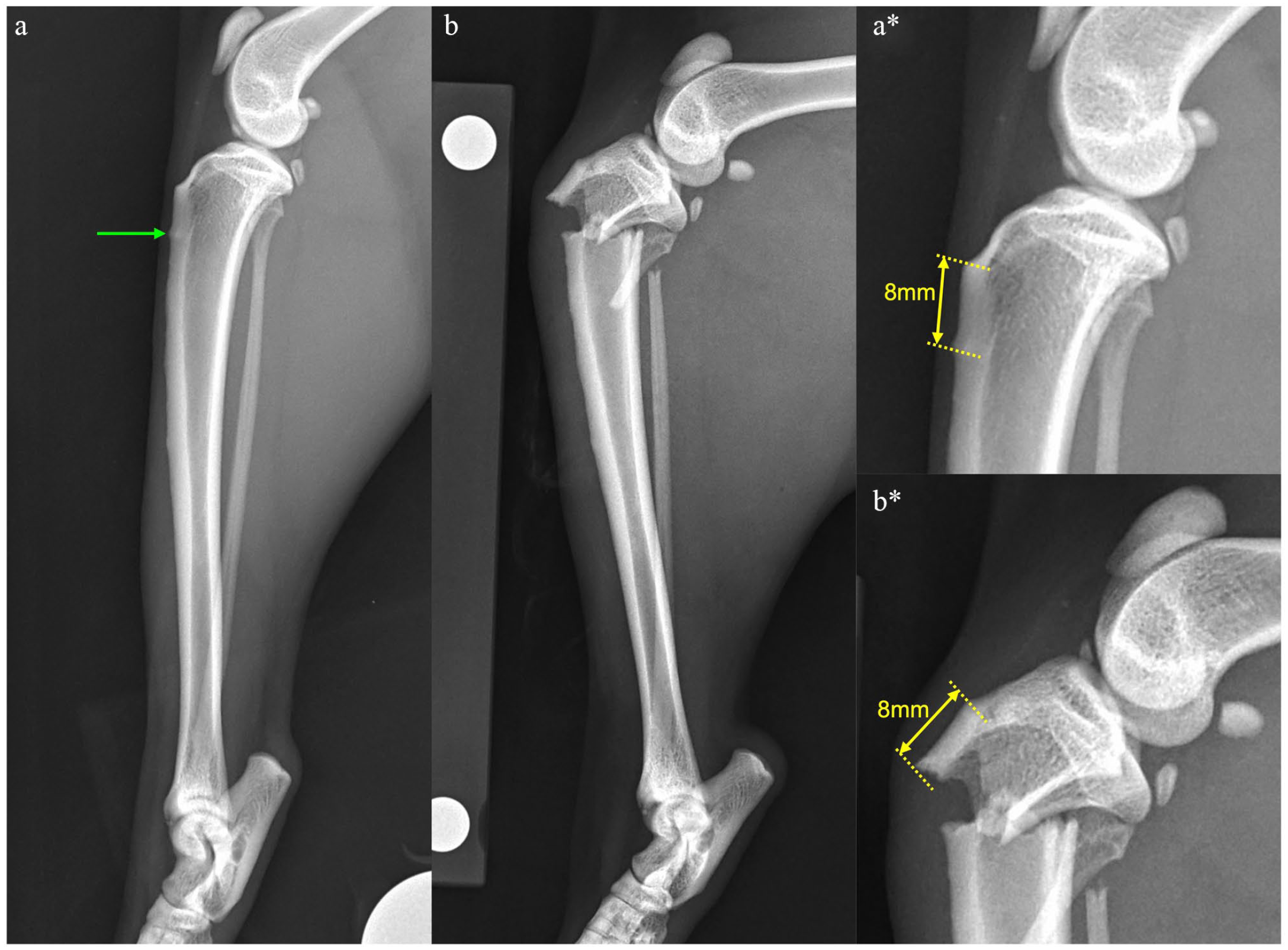
Mediolateral views of the left tibia taken (a) 6 weeks before tibial fracture and (b) at the time of tibial fracture diagnosis, with magnified images from the same time periods (a* and b*). Note the stress reaction in the cranial cortex of the tibia, evidenced as a focal area of increased opacity seen 8 mm distal to the tibial tuberosity (green arrow). This corresponds to the site of fracture noted 6 weeks later, which was, again, 8 mm distal to the tibial tuberosity
The use of BP in animals is not well studied when compared with its use in humans, but there are case reports and retrospective studies describing their use and associated complications.3–6,10,46–50 Due to the way that BPs are generally used within veterinary medicine, reports of complications associated with long-term use are scarce. In dogs, where BPs tend to be prescribed for short treatment periods, such as for toxicities causing hypercalcemia and palliative treatments for bone neoplasia, there are currently no reports of BP-associated fracture.3,4,48,49 Dogs have been used in studies aiming to evaluate the side effects of BP in humans, but these studies have relatively short therapeutic periods.51–53 This makes atypical fractures less likely, as they tend to be reported after years of therapy in other species.17,21,26 The most common indication for prolonged BP use in veterinary medicine is feline IHC.4–6,10 While the long-term follow-up of chronically treated cases of feline IHC is sparse, rendering the prevalence of adverse effects unknown. This report, in addition to a previous one, 7 indicates that owners should be warned of the risk of atypical fracture formation.
Chronic glucocorticoid treatment reduces bone turnover and has been identified as a risk factor for atypical fracture formation. 20 The long-term administration of steroids inhibits fracture healing in rabbits 54 and is known to decrease osteoblastic activity and therefore matrix synthesis.55–58 It should be considered that the chronic prednisolone therapy may have exaggerated the effect of alendronate in this cat, both in terms of the predisposition to fracture and the delayed healing noted.
In the only other published case report detailing BP-associated fractures in a cat, bilateral, staged, atraumatic patellar fractures were sustained in a Maine Coon receiving chronic alendronate therapy to prevent progression of tooth resorption. 7 In that cat, the cortices of the long bones were shown to be significantly thicker than in the control cats. 7 The relative tibial medullary cavity diameters from each set of radiographs were calculated for the cat detailed in the present report, based on the measurements described previously; 7 there was no evidence of a narrower medullary cavity or thicker cortices in this case.
The atraumatic fractures sustained in this case, and those reported previously in a cat on chronic BP therapy, 7 were located in areas and had characteristics that are uncommon. Interestingly, the fractures that these cats sustained have all been reported in cats with patellar fracture and dental anomaly syndrome (PADS). This syndrome is described in cats that have a combination of dental anomalies and which sustain atraumatic insufficiency fractures to the patellae and multiple other bones.58–62 Excluding patellar fractures, other fracture sites encountered in this syndrome include the acetabulum, tibia, ischium, humeral condyle, calcaneus, ilium and pubis. 61 These fractures tend to have similar characteristics, including a simple fracture with a sclerotic fracture line. 61 In the previous BP-associated fracture case, 7 the patellar fractures were radiographically similar to those sustained in cats with PADS. Tibial fractures described in PADS are predominantly proximal diaphyseal or metaphyseal transverse fractures, while calcaneal fractures are typically short oblique fractures located at the base. 61 These fracture patterns are consistent with what was observed in the case reported here.
Currently, the etiology of PADS remains unknown; however, speculations have arisen, including osteopetrosis, a primary bone disorder or a connective tissue disease process.58–62 The similarities in location and radiographic appearance between fractures encountered in PADS and those detailed secondarily to chronic BP therapy may indicate a common pathogenesis. Indeed, if fractures in cats on long-term BP therapy occur secondarily to osteoclast inhibition, it would hold that a primary dysfunction of osteoclasts (and potentially odontoclasts) could also be involved in PADS. Clearly, this hypothesis requires further research, but due to the similarities, if radiographic monitoring of cases receiving long-term BP therapy is considered, it may be prudent to focus on areas where fractures have been reported in PADS.
While it is not possible to state definitively that the cat reported herein did not suffer from PADS, there are several aspects of presentation that would not be typical for this condition. There was no history, or evidence, of dental or oral abnormalities and there were no patellar fractures. In addition, the signalment of the patient is not typical for PADS as these cats generally present with their first fracture earlier in life, at a mean age of 28 months. 59 Given these inconsistencies and the history of chronic alendronate administration, a BP-related insufficiency fracture was considered more likely.
Delayed healing of insufficiency fractures in patients receiving BPs is well recognized in humans17,20,21 and was observed in this case. In this cat, alendronate therapy was discontinued after tibial fracture repair to reduce the risk of additional fractures and potentially facilitate healing of the current ones. However, based on a previous study in humans, likely due to the long half-life of BPs, there was no difference in fracture healing between patients that discontinued BP therapy and those that continued with it. 20 Based on the very small numbers of cats with BP-related fractures, it is not possible to make a definitive recommendation regarding whether BPs should be discontinued in order to reduce future fracture risk; however, given their long half-life as reported in dogs and humans,44,45 discontinuation of therapy is unlikely to make a significant difference to healing of fractures that have already occurred. As protracted healing is anticipated, stabilization should be planned accordingly. Given the risks of plate bending after tibial fracture stabilization in cats 63 and the lower risk associated with orthogonal plating 64 or use of angle-stable interlocking nails, 65 consideration should be given to the latter two methods in cases with BP-associated tibial fracture. Orthogonal plating in this case resulted in a very satisfactory outcome with no implant-associated complications 17 months after stabilization.
Conclusions
This is the first report describing surgical stabilization and long-term follow-up in a cat with atypical fractures receiving long-term BP therapy as well as steroid treatment. As anticipated, clinical union was delayed and stabilization methods for BP-associated fractures should be chosen specifically to withstand cyclic loading throughout a protracted healing period. Retrospectively, a stress reaction was evident in the tibial cortex, which progressed to complete fracture; serial radiographic monitoring may be indicated in cats on long-term BP therapy as this may allow the early detection of stress reactions that may predispose to complete fracture.
Footnotes
Acknowledgements
The authors would like to acknowledge both Dr Danielle Marturello and Dr Courtney Bartels for their involvement with this case.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.