
Abstract
Case summary
A 5-year-old female spayed domestic shorthair cat was presented with a 4.5 × 3 cm ulcerated cutaneous mass on the nasal bridge with extension into the nasal cavity. Tissue biopsy was obtained and a diagnosis of large-cell lymphoma was confirmed on histopathology. The cat was started on prednisolone and injectable chemotherapy; however, only a partial response was observed. A CT scan revealed a highly infiltrative mass with extensive subcutaneous involvement, extending into the nasal cavity, resulting in lysis of numerous nasal and facial bones. The cat received hypofractionated, palliative intent radiation therapy (four fractions of 8 Gray) and a complete clinical response was achieved. Nine months after radiation therapy, minimal residual intranasal disease was observed on advanced imaging. Sixty-nine months after the completion of radiotherapy, a mass was observed dorsal to the right eye within the previous radiation field. CT scan revealed a mass associated with the right frontal sinus with extension throughout the nasal cavity and facial bones. Histopathology was consistent with a moderately differentiated sarcoma. Seventy-one months post-radiation therapy, the cat developed neurologic clinical signs and was humanely euthanized. Radiation-induced sarcoma was suspected based on human criteria, which included history of irradiation and tumor development within the irradiated field, a latent period after irradiation prior to the development of the second tumor and histopathologic confirmation of a different malignant neoplasm at the irradiated site.
Relevance and novel information
To our knowledge, this is the first report of a malignant radiation-induced sarcoma in a cat. Based on this case, radiation-induced sarcomas should be considered as a late-term side effect associated with radiation therapy in cats.
Case description
A 5-year-old, 3.78 kg (8.33lb) spayed female domestic shorthair cat was presented to the primary veterinarian for evaluation of a rapidly growing mass dorsal to the nasal planum. On physical examination, a cutaneous mass on the dorsal nasal bridge was observed and intranasal involvement was suspected. An incisional biopsy was collected from the external, cutaneous aspect of the mass and histopathologic evaluation was diagnostic for large-cell lymphoma. Based on the diagnosis of large-cell lymphoma, the cat was started on single-agent glucocorticoid therapy (prednisolone 1 mg/kg PO q24h). Two weeks after incisional biopsy, regrowth of the mass was reported.
Three months after biopsy, while on glucocorticoid therapy, the cat was presented for consultation at The Ohio State University Veterinary Medical Center. The owner reported that the cat was exhibiting clinical signs consistent with progressive intranasal disease, including increased frequency of sneezing and facial discomfort. At the time of evaluation, the cat had a 4.5 × 3 cm ulcerated mass associated with the nasal bridge. The mass appeared to extend laterally resulting in mechanical compression of the left eye (Figure 1). Upon examination, both conjunctival membranes were swollen, and erythematous and lateral strabismus were present bilaterally.

Appearance of nasal large-cell lymphoma prior to initiation of chemotherapy or radiation therapy
Injectable chemotherapy was initiated with L-asparaginase (10,000 IU/m2 SC Elspar [compounded by SBH Medical]) and doxorubicin (1 mg/kg IV doxorubicin hydrochloride [Novaplus]) under the supervision of a board-certified medical oncologist. One week after chemotherapy, the cat experienced a partial clinical response with a reduction in gross tumor volume; however, a significant gross tumor was still present. A CT scan (GE Medical Systems LightSpeed Ultra, eight-slice detector) was performed 8 days after the first chemotherapy treatment. Pre- and post-contrast images were obtained (Iohexol 2 ml/kg IV [Omnipaque; GE Healthcare]) and helical slice images with a slice thickness of 1.25 mm and pitch of 0.625 were acquired. The tube rotation was 0.8 s with a peak kilovoltage of 120 and 10 mA. The field view was 250 mm with a matrix of 512 × 512. CT scan revealed a 5.2 × 3.6 × 2.4 cm mass associated with the nasal bridge with subcutaneous extension and lysis of the adjacent nasal, maxillary and frontal bones (Figure 2).

(a) Sagittal pre-contrast CT image of the skull using conventional bone window demonstrating nasal mass with subcutaneous extension into the nasal cavity and frontal sinus bone lysis (arrow). (b) Sagittal post-contrast image: note the invasion into the nasal cavity (arrow) and subcutaneous extension. Images were obtained prior to the start of radiation therapy
A hypofractioned, palliative intent radiation protocol was initiated. The protocol received was once weekly treatment to a total of four fractions of 8 Gray (Gy) to a total dose of 32 Gy (Siemens Mevatron linear accelerator; Seimens Medical Laboratories). Radiation treatments were performed under general anesthesia and overseen by a board-certified radiation oncologist. The cat was treated in sternal recumbency with a mouth gag. The radiation delivery was a manual plan of a single dorsal field of 6 megavolt (MV) photons with 0 degree gantry angle. The field size was 5 × 5.5 cm treated to 98.7 source to surface distance with a 1 cm bolus. Two blocks were used to minimize dose to both eyes. One month after completion of radiation, the cat experienced complete resolution of upper respiratory clinical signs and gross tumor was no longer visible on physical examination. No acute side effects, as per the Veterinary Radiation Therapy Oncology Group toxicity criteria, were noted. 1 Following radiation therapy, the cat remained on glucocorticoid therapy (prednisolone 0.66 mg/kg PO q48h [PrednisTab; Nextsource]).
Approximately 9 months post-radiation therapy, the cat was re-presented for increased stertor and snoring. On physical examination, no gross tumor was observed and the cat showed no overt signs of nasal discharge, decreased airflow or ocular abnormalities. A CT scan with contrast (Iohexol 2 ml/kg IV) of the skull was repeated under general anesthesia. The previously identified intranasal mass involving the frontal and sphenoid sinuses was no longer present. A persistent soft tissue structure was noted within the rostral nasopharynx; however, the remainder of the CT scan was unremarkable (Figure 3).

Sagittal CT image of the skull obtained post-contrast using a conventional bone window demonstrating complete resolution of subcutaneous and intranasal disease. Persistent soft-tissue mass noted in the rostral nasopharynx (arrow). Images obtained 9 months following completion of radiation therapy
Doxorubicin was re-initiated at 1 mg/kg intravenously every 3 weeks for a total of three treatments. Clinical improvement with respect to the degree of stertor was noted with doxorubicin treatment. After three treatments, doxorubicin chemotherapy was discontinued owing to the development of treatment-related hyporexia. The cat received one dose of lomustine (48.1 mg/m2 PO [Gleostine; Nextsource]) and was subsequently lost to follow-up.
Sixty-nine months (~5.75 years) after the completion of radiation therapy, the cat was presented for evaluation of a rapidly growing soft tissue swelling above the right eye. On physical examination, a 1.5 × 2.2 cm cutaneous mass was observed dorsal to the right eye within the previous radiation treatment field. Right-sided serous nasal discharge and an area of leukotrichia, a late-term side effect of radiation therapy, was present within the previous radiation field (Figure 4). 1

Images obtained 69 months post-radiation therapy demonstrating (a) the area of leukotrichia and mild anisocoria and (b) new mass (arrow) associated with the right frontal sinus region within the previous radiation field
A complete blood count and chemistry panel revealed no values outside of the laboratory reference intervals. Cytology of the mass was evaluated by a board-certified clinical pathologist and demonstrated marked neutrophilic inflammation and suspected fibroplasia.
To obtain a definitive diagnosis, a CT scan and incisional biopsy of the cutaneous aspect of the mass was performed. CT images (GE Light Speed, 8-detector) with contrast (Iohexol 2 ml/kg IV) were obtained in sternal recumbency under general anesthesia. Helical images with a slice thickness of 0.625 mm and pitch of 0.52 were acquired. The tube rotation was done for 0.8 s and a set peak voltage of 120 kVp. The field of view was 320 mm with a matrix of 512 × 512. A CT scan revealed a 3.0 × 2.8 × 2.6 cm amorphous, heterogeneous, soft-tissue mass centered over the rostral aspect of the right frontal sinus. The mass extended into the caudodorsal aspect of the nasal cavity bilaterally and was primary lateralized to the right side. The mass also extended dorsally into the frontal sinuses, involving the maxillary and frontal bones and into the right retrobulbar space causing lysis of the cribriform plate. Additionally, a round, 7 mm, contrast-enhancing nodule was observed within the right cerebrum (Figure 5).

(a) Transverse and (b) sagittal CT images of the skull demonstrating a soft tissue mass overlying the right frontal sinus region and associated bone and cribiform plate lysis (red arrow) and focal contrast-enhancing lesion (suspect metastasis) in the cerebrum (green arrow). Images obtained 69 months following completion of radiation therapy
Based on the CT images, primary differentials included recurrent large-cell lymphoma, a new primary neoplasia (adenocarcinoma, squamous cell carcinoma, radiation-induced sarcoma) or, less likely, abscess/granuloma. The main differential for the lesion in the right cerebrum was lymphoma; however, an abscess or extra-axial neoplasia (ie, meningioma, metastatic disease) could not be ruled out.
An incisional biopsy of the external component of the mass was obtained for histopathology. Histologically, the neoplasm comprised interlacing bundles of haphazardly arranged spindle cells on a thin fibrous stroma (Figure 6). Neoplastic cells were characterized by moderate amounts of pale eosinophilic cytoplasm with indistinct cell borders. There was moderate anisokaryosis with nine mitoses per ten × 400 fields. There were foci of edema and necrosis, representing <50% of the neoplasm. The histopathologic findings were consistent with a moderately differentiated sarcoma. Immunohistochemistry (IHC) was performed and neoplastic cells demonstrated strong intracytoplasmic vimentin staining. Individual cells with moderate intracytoplasmic staining for Iba1 were variably scattered throughout the neoplasm and areas of extracellular matrix demonstrated mild-to-moderate Alcian blue staining, which were interpreted as mucin. IHC for cytokeratin, S-100, CD31, smooth muscle actin and desmin were all negative. Taken together, the clinical history and histopathologic findings were most compatible with a malignant radiation-induced sarcoma (RIS).
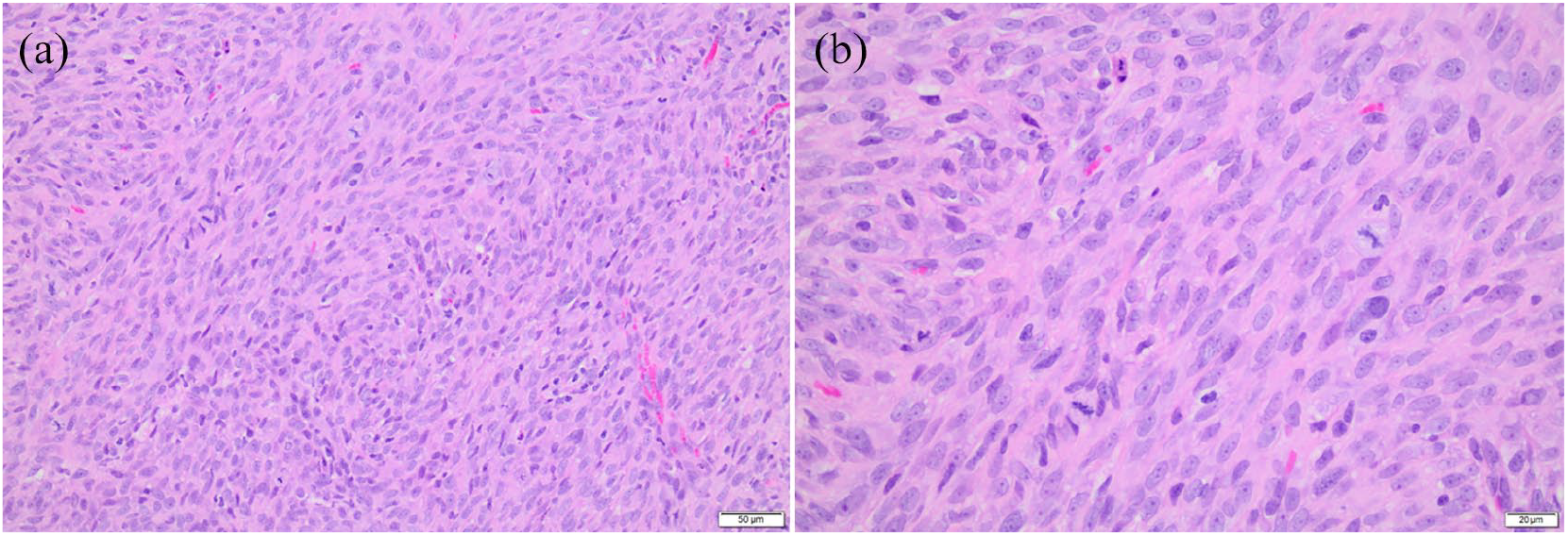
Photomicrographs of hematoxylin and eosin-stained biopsy specimens. At low magnification (a; × 200), the neoplasm is characterized by spindle cells haphazardly arranged in interlacing bundles with moderate eosinophilic cytoplasm and indistinct cell borders. On higher magnification (b; × 400), variably sized, oval nuclei with 1–2 distinct nucleoli and frequent mitotic figures can be appreciated
At this time, the owner declined further therapy. The cat was restarted on prednisolone at 0.94 mg PO q24h. At home, the cat began head pressing and developed seizures. Approximately 71 months (~5.9 years) after the completion of radiation therapy the cat was humanely euthanized.
Discussion
RISs are a well-recognized late-term complication of ionizing radiotherapy in humans,2–5 and, to a lesser extent, in dogs. Similarly, RISs have been described in dogs receiving external beam or intraoperative radiation therapy for spontaneous tumors (acanthomatous epuli, 6 soft tissue sarcomas and mast cell tumors, 7 primary bony neoplasia 8 ) and in healthy adult laboratory beagle dogs given experimental intraoperative radiation therapy. 8 While previously considered a rare clinical entity, the incidence of RIS in humans has increased significantly.9,10 Improvements in radiation delivery and technology have led to improved clinical outcomes. With continued improvements in veterinary radiation therapy, a similar increase in the incidence of RISs can be expected.
RISs are thought to develop secondary to radiation-induced double-stranded DNA breaks and the resultant genomic instability that leads to carcinogenesis. 10 Newer research evaluating the transcriptome of spontaneously occurring sarcomas and RIS has demonstrated that mitochondrial dysfunction is discordantly present in RIS and thus may be a contributing factor. 11 While both sarcomas and carcinomas have been reported, sarcomas are far more common in the veterinary literature while squamous cell carcinoma is the most commonly reported radiation-induced malignancy in humans who have undergone previous head or neck radiation therapy. 4
Given the morphologic and histochemical characteristics of the neoplasm, fibrosarcoma and myxosarcoma were considered as primary differential diagnoses. Additionally, the lack of S-100, CD31, Iba1, smooth muscle actin and desmin staining of the neoplastic cell population supports the exclusion of tumors of neural crest origin, hemangiosarcoma, histiocytic sarcoma, leiomyosarcoma and rhabdomyosarcoma, respectively. The primary differential diagnosis of fibrosarcoma is in line with the reported incidence of nearly 20% in humans with RIS. 12
In the human literature, criteria have been established defining RIS, requiring patients to have a history of irradiation and tumor development within the irradiated field, there being a latent period present after irradiation prior to the development of the second tumor and histopathologic confirmation of a different malignant neoplasm at the irradiated site. 13 Although it is unclear whether companion animals fit this definition, these criteria have been used for the limited cases reported in the canine literature. Based on the history of the cat in this report, a >5-year latency period between radiation and secondary tumor development, and histopathologic diagnosis of a different neoplastic entity (moderately differentiated sarcoma) within the previous irradiated site, this cat met the criteria for diagnosis of an RIS.
At this time, a standard of care for nasal lymphoma in cats is unclear. Radiation therapy has shown significant benefit in ameliorating localized upper respiratory clinical signs, with response rates reported as high as 93%. 14 Up to 18% of cats with nasal lymphoma are reported to have systemic progression of their lymphoma, thus advocating for the use for adjuvant systemic therapy for this population is often reasonable. 15 Radiotherapy and cytotoxic chemotherapeutics both appear to have efficacy in the treatment of nasal lymphoma, although no significant differences in overall survival time have been reported in cats treated with chemotherapy and radiation therapy vs cats treated with systemic chemotherapy alone. 14
It is unclear whether a hypofractionated protocol may put cats at greater risk for the development of late-term side effects vs a conventionally fractionated radiation protocol. A hypofractionated protocol increases the risk of late-term side effects vs conventionally fractionated protocols, as in a hypofractionated protocol a larger dose per fraction is administered to both tumor and normal tissues.16,17 In a study evaluating the outcomes of 65 cats with various nasal tumors treated with hypofractionated radiotherapy, one cat reportedly developed an osteochondroma of the maxilla 1267 days (3.47 years) after hypofractionated radiation therapy of nasal lymphoma. 18 In another study evaluating 19 cats with stage 1 nasal lymphoma being treated with megavoltage radiation ranging from 22 to 48 Gy (median dose 42 Gy) and multi-agent chemotherapy, no cases of RIS were identified in any of the 19 cats treated with radiation therapy. 15 Based on this case report, owners of cats expected to have prolonged survival because of age or diagnosis after hypofractionated radiation therapy should be warned that RIS is a potential late-term side effect.
Conclusions
This case describes a cat that developed an RIS 69 months after hypofractionated radiation therapy. To our knowledge, this is the first report of a malignant RIS in a cat. Based on this case, development of RISs in cats receiving radiation therapy should be considered as a potential late-term outcome. With improvements in radiation therapy planning and delivery, the incidence of RISs in companion animals may increase with concurrent improvements in survival. More information is needed to understand the genesis, treatment options and prognosis for cats that develop RIS.
Footnotes
Acknowledgements
We would like to acknowledge the help and support provided by all the faculty and staff at The Ohio State Veterinary Medical Center with the care and treatment of the cat discussed in this report.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Financial support for this work was provided by the Office of The Director and National Institutes of Health (K01OD019923, JMF). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding sources.
Ethical approval
This work involved the use of non-experimental animal(s) only (owned or unowned), and followed established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care. Ethical approval from a committee was not necessarily required.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work for the procedure(s) undertaken. For any animals or humans individually identifiable within this publication, informed consent for their use in the publication (verbal or written) was obtained from the people involved.