
Abstract
Case summary
A 6-month-old domestic shorthair cat was evaluated for proprioceptive ataxia of the pelvic limbs. Over 2 months, the cat became poorly ambulatory, paraparetic with proprioceptive ataxia and developed a firm, distended bladder with intermittent overflow urinary incontinence. Block vertebrae (T1–3, T4–5 and T10–11) and lordosis were identified on radiographs of the vertebral column. MRI revealed T3/4 intervertebral disc protrusion with severe extradural compression, secondary syringohydromyelia caudal to the protrusion and generalised intervertebral disc disease throughout the cervical and thoracic vertebrae. Dorsal laminectomy at T3/4 resulted in resolution of paraparesis and marked improvement in coordination and strength. Block vertebrae are usually considered an incidental finding. In this patient, angular deformation (lordosis) and adjacent segment disease probably contributed to clinically significant intervertebral disc degeneration and protrusion.
Relevance and novel information
There are few case reports in the literature of multiple congenital vertebral malformations causing neurological deficits in cats. This is the first reported case of successful surgical management of intervertebral disc protrusion, possibly secondary to block vertebrae and lordosis in a cat.
Keywords
Case description
A 6-month-old male entire domestic shorthair cat was surrendered to our institution with no known owner or history. The patient’s body weight was 1.8 kg and its body condition score was 2/9.
Pertinent physical examination findings included pale pink mucous membranes, tachycardia (200 beats per minute) and a heavy infestation of fleas (Ctenocephalides felis). Neurological examination revealed an ambulatory, mild, uncoordinated, swaying gait, restricted to the pelvic limbs. No pain was elicited on palpation of the whole vertebral column. The remainder of the neurological examination was considered normal. The gait abnormality was classified as mild pelvic limb proprioceptive ataxia, most consistent with T3–L3 spinal cord segment neuroanatomical localisation.
Haematology identified a non-regenerative anaemia and mild lymphocytosis. Serum biochemistry revealed a mild increase in alanine aminotransferase activity. An ELISA (Snap Combo; IDEXX) for feline leukaemia virus antigen and feline immunodeficiency virus antibody was negative. Mycoplasma haemofelis PCR testing was also negative.
Radiographs of the vertebral column showed seven cervical, 12 thoracic and seven lumbar vertebrae. T1–T3 vertebral bodies were fused, forming a block vertebra (Figure 1). Additional block vertebrae due to partial fusion were also present at T4–T5 and T10–T11. The inter-vertebral disc spaces at T3/T4 and T9/10 were narrowed. There was also ventral deviation of the cranial thoracic vertebral column at T2 resulting in focal lordosis.

Lateral radiograph of the cervical and thoracic vertebrae from a 6-month-old domestic shorthair cat with paraparesis. The image shows block vertebral malformation and lordosis at T1–3. Partial fusion of T4–5 and T10–11 is also seen
Two months later, proprioceptive ataxia was more pronounced and the cat became poorly ambulatory and paraparetic. Pelvic limb postural reactions, including paw replacement, hopping and extensor postural thrust, were inconsistently delayed. The patellar reflex was exaggerated and muscle tone increased in the pelvic limbs. Withdrawal reflexes were normal in all four limbs. The cutaneous trunci reflex was not assessed. The cat’s bladder was firm and distended with intermittent overflow urinary incontinence. Urinalysis was not performed. The clinical signs were consistent with T3–L3 myelopathy. The cat was treated empirically with prednisolone (1 mg/kg PO q24h [Pred-X 5; APEX]) for 4 weeks with minimal improvement in clinical signs.
For further investigation, the cat was anaesthetised for MRI of the vertebral column. MRI examination was performed on a high-field (1.5 T) system (GE Signa Excite), with the patient positioned in dorsal recumbency on a spinal coil. Sequences to evaluate the vertebral column included T2-weighted (T2W) fast relaxation, fast spin echo (FRFSE) sagittal (cervicothoracic, thoracolumbar), T1-weighted (T1W) fast spin echo (FSE) sagittal (cervicothoracic, thoracolumbar), T2W FRFSE transverse (C7–T5) and T1W FSE transverse (C7–T5). Gadolinium-based contrast media was not administered.
MRI confirmed the block vertebrae at T1–T3 with lordosis, as well as block formation with partial fusion at T4–T5. At the level of T3/T4 there was T2W hypointense extradural material in the ventral vertebral canal. This material was confluent with the dorsal aspect of the intervertebral disc annulus, and most consistent with intervertebral disc protrusion (IVDP). 1 Additionally, there was dorsal angulation of the intervertebral disc due to lordosis between T3 and T4. The angulation and slight bulging of the intervertebral disc caused severe compression of the spinal cord (59% cross-sectional area compared with adjacent normal spinal cord), with attenuation of the subarachnoid space and localised increased T2W signal of the spinal cord parenchyma. Caudal to the site of compression, there was increased intraparenchymal spinal cord fluid signal in the T2W image, most compatible with syringohydromyelia, but other possibilities include oedema or gliosis (Figures 2 and 3). The remaining nucleus pulposi of the intervertebral discs had reduced (non-homogenous grey to black) T2W signal and loss of distinction between the nucleus pulposus and annulus fibrosus, compatible with generalised intervertebral disc degeneration. There were similar changes in the cervical and thoracic vertebral column. Surgical decompression was recommended due to the progressive neurological signs.
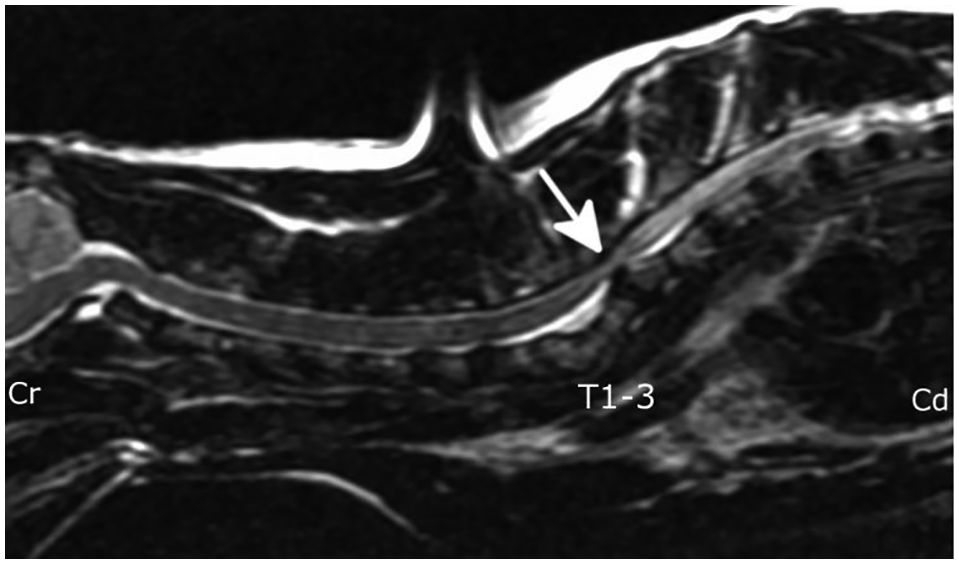
T2-weighted sagittal MRI of the cervical and cranial thoracic spine from a 6-month-old domestic shorthair cat with paraparesis. The angulation of the vertebral column and the slight bulging of the intervertebral disc at T3/4 can be seen (arrow). These abnormalities combine to cause the severe compression of the spinal cord. Cranial (Cr) and caudal (Cd) are labelled on the image for reference

T2-weighted transverse MRI from a 6-month-old domestic shorthair cat with paraparesis. The arrows show the degree of spinal cord compression at the level of T3/4, when compared to a non-compressed site (T2)
The cat was anaesthetised and placed in sternal recumbency. A standard approach to the caudal cervical and cranial thoracic vertebrae was performed. 2 The median raphe was incised and sharp and blunt dissection exposed the dorsal spinous processes of T1–T4. The dorsal spinous processes of T2 and T3 were removed with bone rongeurs to the level of the lamina and spinal decompression was executed by a dorsal laminectomy of T3 and T4 utilising Kerrison rongeurs and a high-speed spinal burr (B Braun Hilan XS). At the level of T3/T4, a focal devascularised region of the dura mater was noted during surgery, which resolved following decompression. Prior to routine closure of the surgical site, a gelatin sponge (Gelfoam; Pfizer) was placed over the laminectomy site. Antimicrobial prophylaxis with cephazolin (22 mg/kg IV [Cefazolin; AFT]) was initiated perioperatively and postoperatively at 2, 4 and 12 h. This was followed by amoxicillin-clavulanic acid (22 mg/kg PO q12h [Amoxclav; APEX]) for 7 days. The prolonged use of postoperative antibiotics was not in accordance with current perioperative antibiotic therapy guidelines. 3 Postoperative analgesia included a constant rate infusion of morphine (0.1 mg/kg/h [DBL Morphine Sulfate Injection BP; Hospira]), with lidocaine (1 mg/kg/h [Lignocaine 20; Ilium]) and ketamine (0.3 mg/kg/h [Ketamine; Ceva]). This was followed by buprenorphine (0.02 mg/kg IV q8h [Temvet; Troy]). Prednisolone was tapered from 1 mg/kg q24h to 0.5 mg/kg q24h for 7 days, then 0.5 mg/kg q48h for 7 days and then discontinued.
The day after surgery, the cat remained ambulatory but paraparetic with marked proprioceptive ataxia. Six weeks after surgery, the cat was able to ambulate with mild-to-moderate proprioceptive ataxia and the paraparesis had resolved. Four years later, with ongoing phys-iotherapy, there was proprioceptive ataxia, similar to initial presentation. The cat showed marked improvement in coordination and strength, postural reactions and spinal reflexes remained normal and no urinary incontinence was reported.
Discussion
Congenital malformations of the vertebral column are often identified radiographically in both the canine and feline population. These findings may or may not be clinically significant. 4 There has been little information published on the incidence and types of congenital vertebral anomalies specific to the cat. 4 A genetic predisposition has been identified in some cases. 5 Other possible causes of congenital anomalies include metabolic disease, such as folate deficiency; storage diseases, such as mucolipidosis II; teratogenous drugs; and toxin exposure. 5
In a study from a general hospital population of 200 cats, the incidence of congenital axial skeletal abnormalities was determined using radiography of the entire vertebral column. Transitional vertebrae were most common at the sacrocaudal and thoracolumbar junctions and were not associated with clinical signs. 4 Block vertebrae were identified in three cats (just over 1% of the population) and, despite marked associated scoliosis, there were no clinical signs or palpable deformities. 4
Block vertebrae are due to defects in segmentation during foetal development, resulting in partial or complete fusion of two or more vertebrae. 5 When the fusion occurs in one plane, a bony bar develops that restricts growth causing angular deformity in that plane. Block vertebrae are usually considered an incidental finding, but neurological deficits may occur in patients with angular deformation, stenosis of the vertebral canal or if there is abnormal loading of adjacent vertebra leading to intervertebral disc degeneration or protrusion, instability or ligament hypertrophy. 5 In this case, the cat had multiple anomalies, including only 12 thoracic vertebrae, block vertebrae and angular deformation (lordosis). It is suspected that abnormal loading of adjacent vertebrae during growth likely contributed to intervertebral disc degeneration and protrusion; however, given the cat’s unknown history, trauma cannot be ruled out.
The incidence of intervertebral disc disease (IVDD) in cats with neurological deficits or pain localised to the vertebral column has been estimated to be between 0.02 and 0.24%.6,7 British Shorthairs and Persians were over-represented with thoracolumbar IVDD in a recent study, but it is unknown if this represents a true breed predisposition. 7 It is unclear why this cat had multiple degenerate intervertebral discs in areas without congenital vertebral malformation.
There has been little research into the disease characteristics associated with intervertebral disc extrusions (IVDE) and IVDP in cats. This contrasts with dogs where degenerative IVDD is considered the best characterised spinal condition. 8 In a limited number of studies in cats,7,9 IVDE was slightly more prevalent than IVDP and was associated with shorter duration and more severe clinical signs. The mean age of cats with clinically significant IVDP was 8 years and the most commonly affected discs were L4/5, L7/sacral and T13/L1. There was increased prevalence of IVDD at T2/3 and T3/4 in cats vs dogs. IVDD is uncommon in these locations in dogs because the intercapital ligament covers intervertebral discs between T1 and T11, which extends from the head of one rib to the head of the opposite rib over the intervertebral disc and across the floor of the vertebral canal. 10 This is thought to provide additional support for the discs and protection from protrusion.10,11 Cats, however, have an extremely flexible vertebral column from T4 to T10, despite the presence of the intercapital ligament. 10 It is therefore possible that a more flexible area (T4–11) adjacent to a more stable area (T2–3) may lead to the development of IVDD at those locations. 9
Adjacent segment disease is defined as degeneration or another pathological process that occurs cranial or caudal to a region of vertebral column fusion. 12 It has been described in dogs following vertebral fusion of the cervical vertebral column for the management of caudal cervical spondylomyelopathy and more recently in dogs with vertebral fusion secondary to spondylosis deformans or diffuse idiopathic skeletal hyperostosis. 12 The exact mechanism is unclear, but biomechanical stress appears to result in degeneration of the neighbouring unfused intervertebral disc spaces and protection of the fused intervertebral discs from degeneration. 12 It is likely a combination of factors, including adjacent segment disease, resulted in IVDD and IVDP in this cat.
Syringomyelia is the development of a fluid-filled cavity in the spinal cord. 13 This may be congenital or occur as a result of obstruction of the subarachnoid space and accumulation of fluid within the spinal cord. 13 Causes include tethered spinal cord, trauma, arachnoiditis, neoplasia and abnormalities of the caudal fossa (Chiari malformations). 13 Additionally, any cause of chronic spinal compression, including IVDP or angular deformation of the vertebral bodies, as in this case, may lead to syringomyelia. 13
The prognosis for cats undergoing surgical decompression of the spinal cord owing to IVDD is reported to be good.6,9,14 There are few case reports on surgical management of spinal cord compression in congenital vertebral malformations in either dogs or cats, but the prognosis for surgical intervention is reported to be fair to good.15,16
Conclusions
This is the first reported case of successful surgical management of IVDP possibly secondary to block vertebrae and lordosis in a cat. Although definitive conclusions cannot be drawn from limited case reports, the outcome of this case, as well as previous reports, suggests surgical decompression of the spinal cord is a promising treatment option for these patients.
Footnotes
Acknowledgements
Thanks go to Dr Joanna White BVSc (Hons), MVSc (Epi), DipACVIM (Internal Medicine), PhD for editorial assistance.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of a client-owned animal only, and followed established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care. Ethical approval from a committee was not therefore needed.
Informed consent
Informed consent (verbal) was obtained from the owner of the animal described in this work for the procedures undertaken.