
Abstract
Background:
Knowledge, attitudes and practices (KAP) of kidney care providers regarding climate change, environmental impacts of kidney care and environmentally sustainable kidney care have been assessed in diverse regions worldwide, but little is known about the perspectives of people who receive dialysis therapies. We aimed to assess the KAP of people on dialysis about these subjects.
Methods:
An electronic KAP survey, based on a previous survey of Canadian kidney care providers, was administered to people receiving all available dialysis modalities in a single center in Canada, from December 2024 to May 2025.
Results:
A total of 69 people responded to the survey, of whom 67% identified as men, and 70% were undergoing in-center hemodialysis (ICHD), 14% home hemodialysis (HHD) and 16% peritoneal dialysis (PD). Most (87%) of the respondents felt informed about climate change to at least an average degree. Nearly half were either extremely or very concerned about climate change (44%) and the waste generated by dialysis treatments (43%), and the levels of concern differed across dialysis modalities. Overall, 51% of respondents never felt guilt or anxiety related to the carbon footprint of dialysis treatment. However, there were significant differences (χ2 test; P < .001) in the occurrence of these feelings depending on the dialysis modality (more frequent in people receiving home modalities, and more in PD than HHD). Most respondents were either very (45%) or slightly (45%) interested in obtaining more information about the themes explored in the survey.
Conclusions:
This survey showed that most respondents receiving a dialysis therapy felt informed and at least moderately concerned about climate change. Higher levels of concern about climate change and the amount of waste generated by dialysis treatment, as well as more frequent occurrence of guilt/anxiety about the carbon footprint of dialysis were observed in people on home therapies (PD and HHD) compared with ICHD.
Introduction
Climate change impacts kidney health and threatens the stability of kidney care delivery systems.1,2 People living with kidney failure, particularly those requiring dialysis, are uniquely vulnerable to the health effects of climate change. In the face of natural disasters (including climate change–related extreme weather events), reliable access to health care, including life-sustaining dialysis therapy, may be jeopardized and result in harm.
Conversely, health care is responsible for nearly 5% of global greenhouse gas emissions 3 and kidney care is a disproportionately large contributor owing to emissions associated with transportation of patients and staff; the manufacture, transport, consumption and disposal of single-use plastic medical devices; high energy requirements of dialysis facilities and equipment; and water use.4 -7 Some groups working to reduce the environmental impact of dialysis suggest that people undergoing dialysis treatment and health care workers themselves be actively involved in mitigation efforts. 8
Recently, many surveys in diverse settings have assessed the knowledge, attitudes and practices (KAP) of kidney care providers about climate change and environmentally sustainable kidney care (ESKC).9 -17 There is limited literature on the perspectives of patients about the impact of climate change on health and the environmental impact of health care: while the perspectives of people living with respiratory diseases on the health impacts of air pollution and the carbon footprint of inhalers (which are known to have substantial environmental impact) are gaining interest over the last decade,18 -26 very little is known about the perspectives of people on dialysis about climate change and the environmental impact of kidney care. 27 We hypothesize that people requiring dialysis therapy would be at least as likely to suffer from eco-anxiety (defined as chronic fear of environmental catastrophe) 28 and/or solastalgia (referring to a disruptive psychological response in people exposed to environmental degradation) 29 as the general population, particularly if access to their treatment has previously been affected by climate change-related events (eg, flood, forest fires). Moreover, some patients requiring these life-sustaining therapies report feelings of guilt or anxiety about their treatment related to their awareness of the amount of electricity and water used, as well as the waste generated by dialysis treatments. 30 Although engagement of health care workers and patients in mitigation strategies is crucial, informing patients of the environmental implications of their life-sustaining treatments may lead to a highly undesirable and fully unintended additional burden in this population who already faces substantial challenges.
In this single-center study, we aimed to assess (1) the KAP of people on dialysis about climate change, the environmental impact of kidney care and ESKC, and (2) the possible psychological impact of these concerns on this vulnerable population.
Methods
Design
The KAP methodology, aiming to assess what is known (knowledge), believed (attitude) and done (practices) on a particular topic, was used through a structured questionnaire.31,32 The survey used in this cross-sectional study (Supplemental File 1) was modified from a version created by members of the Canadian Society of Nephrology’s (CSN) Sustainable Nephrology Action Planning committee (including members of our team) that was originally administered to kidney care providers. 17 Modifications were made by the core research team following discussions with patient-partners, mainly by adding new questions and removing questions not relevant to patients. Following the development of the questionnaire, the questions were uploaded and formatted on the Research Electronic Data Capture (REDCap) platform, in both French and English versions. Both online versions of the questionnaire were tested for usability and technical functionality by research team members and patient-partners, using both a cellphone and a computer. At least 2 subsequent rounds of feedback were completed before finalization of the questionnaire.
Following demographic questions, participants were asked about awareness, attitude and response to climate change in both their life and kidney care realms. The version used in the current study added questions about eco-anxiety, solastalgia and feelings of guilt/anxiety related to the carbon footprint of their dialysis treatment, as well as previous impacts of extreme weather events or natural disasters on participants’ life and dialysis therapy. Participants’ interest in obtaining more information about the themes explored in the survey, or in becoming involved in environmentally sustainable dialysis improvement initiatives, was assessed. Finally, to assess the psychological impact of the survey itself, participants were asked if the survey questions triggered any negative emotions about dialysis. Participants’ ideas to limit the environmental impact of kidney care and any additional comments were welcomed. The survey was reviewed by patient-partners (including co-author CC) in both languages; appropriate modifications were made following their feedback.
Sample and Survey Administration
Eligible adults (18 years or older) receiving a dialysis therapy (in-center hemodialysis [ICHD], peritoneal dialysis [PD] and home hemodialysis [HHD]) from a single university center (total of approximately 250 people receiving dialysis) in Montreal, Canada, were invited to participate in the survey. This center is 1 of 12 dialysis centers for adults in the city and one of the largest dialysis centers in the province of Quebec. The population served at this center is quite representative of the general dialysis population in Montreal, with the exception of a low representation of Indigenous Peoples compared with some of the other centers in the city. Eligibility criteria included a sufficient understanding of French or English to answer the survey questions and ability to provide informed consent. The survey, available in both French and English versions, was administered electronically from December 2024 to May 2025 and was hosted on the secured REDCap server of the Centre de Recherche du Centre Hospitalier de l’Université de Montréal (CHUM). Ethics approval was obtained from the research ethics board of the CHUM (project 2025-12319).
Posters inviting people to participate in the survey were placed in waiting areas and in treatment rooms of the ICHD unit, as well as in the PD clinic, and included a QR code and a web address to access the online survey (Supplemental File 3). The same poster was sent via e-mail from the clinical team of the HHD program to people receiving HHD. In addition, research assistants approached people during their ICHD treatment to invite participation, using a tablet made available for this purpose. If needed (eg, visual impairment or uncomfortable with using a tablet), participants could be assisted by someone to help them complete the online survey on site (by research personnel) or at home (by a family member/caregiver). Following the online study information, and once consent was provided, participants were asked if they required any assistance to complete the survey and were then linked to the survey.
Detailed methods are provided in Supplemental File 2, in accordance with the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) checklist. 33
Data Analysis
To assess KAP about climate change among participants, and to identify significant correlations between participants’ characteristics (age, self-reported gender, education level, dialysis modality) and KAP responses, descriptive analyses and χ2 tests were used. To illustrate differences across dialysis modalities, pie charts specific to each modality and overall were used; similarly, to illustrate the association between various levels of information and/or degrees of concern, eco-anxiety or solastalgia, bar charts were used. Analyses were performed using Stata/SE 15.1 for Mac (College Station, Texas). A P value <.05 was reported as statistically significant.
Results
Participants’ Characteristics
A total of 73 people read the information and consent form, and 70 consented to the study; one person answered only demographic questions, hence 69 participants were included in analysis (Table 1). About half (52%) of the respondents were assisted in survey completion. The majority (63%) of respondents were older than 60 years, and most of them identified as men (67%). Less than five percent identified as Indigenous and 19% as members of a racialized minority group. Nearly half of respondents (45%) reported having studied at a university level, regardless of degree completion. Seventy percent were receiving ICHD, 14% HHD, and 16% PD. Most respondents (59%) had been on dialysis for more than three years.
Participant Characteristics.

Knowledge
When asked whether they thought climate change is happening, 93% of respondents answered “yes.” The vast majority (81%) felt they were informed about climate change at an average level (46%) or better (25% above average; 16% very well informed; Figure 1A). In addition, 46% of the respondents reported being somewhat informed about the impact of health care services on climate change, whereas 41% felt they were not at all informed (Figure 1B). No participant characteristics were associated with being informed.
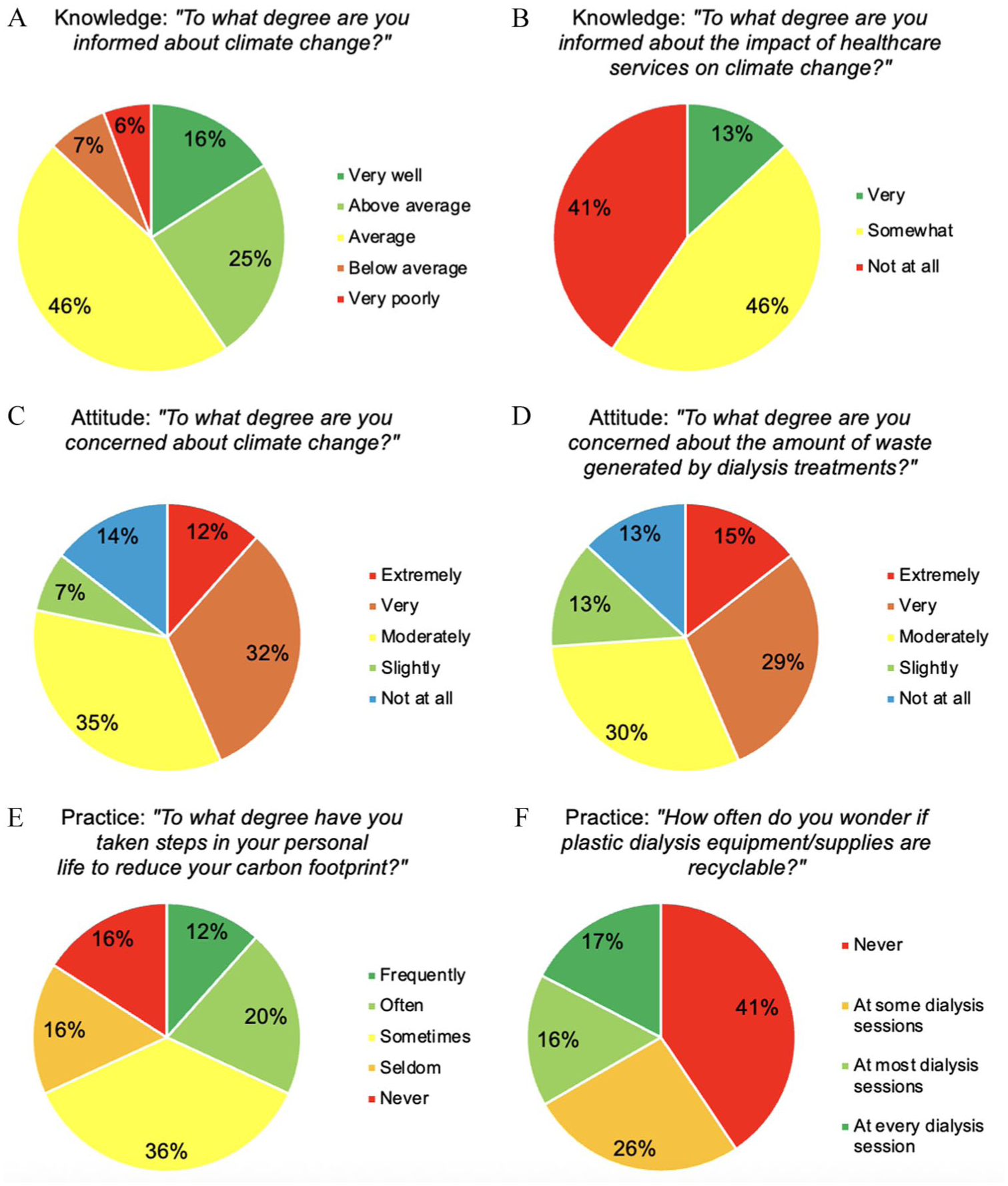
Knowledge (A-B), attitude (C-D) and practices (E-F) of people on dialysis about climate change and about the impact of kidney care on the environment.
Attitudes
A majority of respondents were either moderately (35%) or very concerned (32%) about climate change (Figure 1C), and moderately (30%) or very (29%) concerned about the amount of waste generated by dialysis (Figure 1D). No statistically significant associations were found between level of concern and age, gender or education. However, differences emerged across dialysis modalities: respondents on PD and HHD reported higher degrees of concern about climate change (P = .022; Figure 2A) and about the amount of waste generated by dialysis (P = .044; Figure 2B).

Level of concern of respondents about climate change (A) and about the amount of waste generated by dialysis treatments (B), according to dialysis modality: in-center hemodialysis (ICHD), home hemodialysis (HHD) and peritoneal dialysis (PD); P = .022 (A) and P = .044 (B).
Most respondents believed that it was important to reduce carbon footprint in their personal life (fairly 25%, important 25%, very 33%) and in kidney care services (fairly 22%, important 32%, very 28%). None of the participants’ characteristics were associated with the importance given to the reduction of carbon footprint.
Impact of Climate Change, Eco-anxiety and Solastalgia
When asked to what degree they had ever been personally impacted by an extreme weather event or natural disaster, 29% of respondents reported having been moderately impacted, whereas 22% reported having been slightly impacted and another 22% not at all impacted, and the remaining 9% and 17% reported having been extremely and very impacted, respectively. When asked to what extent their dialysis treatment had been impacted by such events, most respondents reported being not at all impacted (61%) or only slightly (17%) or moderately (10%) impacted.
To evaluate eco-anxiety, respondents were asked how often they had been unable to stop thinking about climate change or other environmental challenges in the past two weeks. Among them, 42% answered “never”, whereas 19% and 25% responded “rarely” and “sometimes.” Most respondents reported being worried about the transformation or changes experienced in the environment around them, with 43% indicating being moderately worried and 26% very worried, reflecting solastalgia.
Guilt or Anxiety About Personal or Dialysis-Related Carbon Footprint
Overall, 36% of respondents reported never having experienced feelings of guilt or anxiety related to their personal carbon footprint, whereas 38% stated they had rarely experienced such feelings (Figure 3A). A large majority also reported never (51%) or rarely (26%) having experienced these feelings related to their dialysis treatment (Figure 3B). An association was found between feelings of guilt or anxiety related to dialysis and dialysis modality (χ2 test; P < .001): 55% of respondents on PD answered having experienced such feelings “very often,” and 50% of the respondents on HHD reported having experienced them “often,” whereas these degrees of guilt/anxiety were rare in ICHD (4% “very often,” 6% “often”) (Figure 3C).
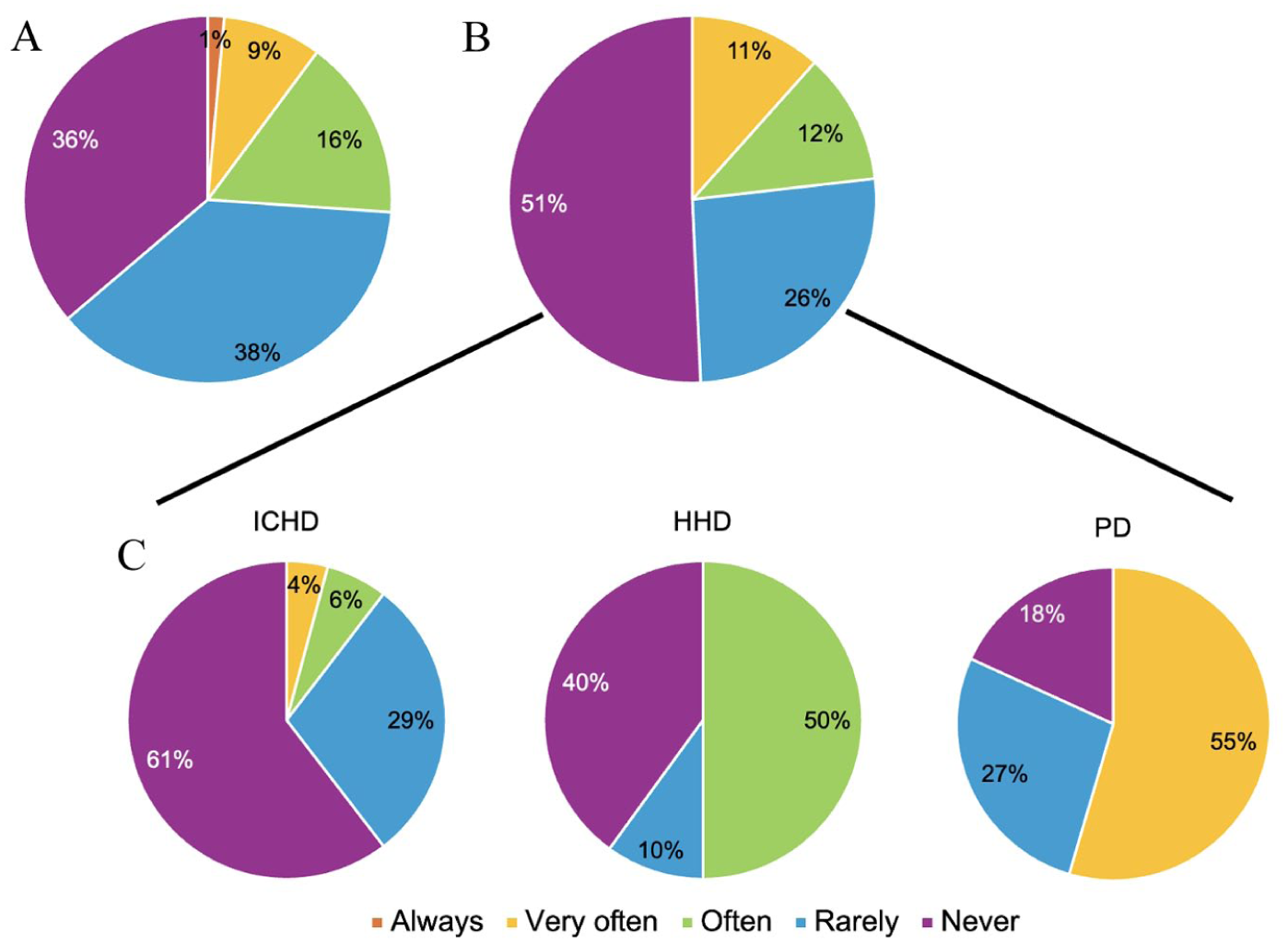
Respondents’ frequency of feelings of guilt or anxiety toward their personal carbon footprint (A—overall) and dialysis-related carbon footprint (B—overall; C—according to dialysis modality).
Practices
Most respondents answered having taken steps to some degree in their personal lives to reduce their carbon footprint: sometimes 36%; often 20% (Figure 1E). The most frequent steps reported were increased use of locally produced food (54%), increased use of public transit (54%), reduced meat consumption (46%), reduced vehicle travel (45%) and cycling or walking (45%).
When asked how often they wonder if plastic dialysis equipment/supplies are recyclable, 41% of respondents answered “never,” 25% “at some dialysis sessions,” 16% “at most dialysis sessions” and 17% “at every dialysis session” (Figure 1F). No association was found with dialysis modality.
Interrelations Between KAP
Statistically significant associations were observed between the degree of concern about the amount of waste generated by dialysis and feeling more informed about climate change (P = .011), as well as about the impact of health care services on climate change (P = .026) (Figure 4B). No such association was found between these self-reported levels of knowledge and the degree of concern about climate change (Figure 4A). In Figure 4, the level of knowledge is illustrated by each column (from very well informed on the left to very poorly informed on the right), while the degree of concern is shown by the various colors used (from extremely concerned in red to not at all concerned in blue).

Degree of concern about climate change (A) and about the waste generated by kidney care services (B) according to how informed respondents reported being about climate change and the impact of health care services on climate change.
No association was found between respondents who reported feeling more informed/having greater concern about climate change or the environmental impact of health care and the extent of steps taken to reduce their personal carbon footprint.
Respondents who reported feelings of guilt or anxiety about their personal and dialysis-related carbon footprint (shown as the columns on the left) reported being more unable to stop thinking about climate change or other environmental challenges (eco-anxiety, illustrated as warmer colors; P = .003 and P < .001, respectively; Figure 5A). Similarly, those who were more concerned about climate change and about the amount of waste generated by dialysis (shown as the columns on the left) reported more worry about the transformation or changes experienced in the environment around them (solastalgia, illustrated as warmer colors; P < .001 and P = .005, respectively; Figure 5B).

Association between respondents’ feelings of guilt/anxiety about personal and dialysis-related carbon footprint and eco-anxiety (A), and association between respondents’ level of concern about climate change and the amount of waste generated by dialysis and solastalgia (B).
Emotional Impact of the Survey Itself
Of all respondents, 87% reported not having been triggered by the survey questions, whereas 9% reported feeling uncomfortable and 4% feeling anxious or stressed.
Interest in Obtaining More Information or Getting Involved
A large majority of respondents were either very (45%) or slightly (45%) interested in obtaining more information about the impact of climate change on kidney health, the impact of kidney care services on the environment and ESKC, while 35% of respondents answered being interested in getting involved in initiatives or projects toward environmentally sustainable practices in dialysis. None of the respondents’ characteristics were associated with their interest in obtaining more information on the subject. Respondents’ interest in getting more involved was not associated with feelings of eco-anxiety or solastalgia.
Respondents’ Ideas for Improvement to Limit the Environmental Impact of Kidney Care and Additional Comments
Overall, 13 people (19%) reported having ideas to limit the environmental impact of kidney care. Ideas from more than half of them (7) pertained to recycling or recovery of waste, packaging or consumables. Other ideas included machines with lower energy and/or water use, “avoiding squandering of consumables” and use of personal items instead of single-use (eg, water or coffee cups) and/or unit-managed items (eg, blankets, pillows). In addition, at the end of the survey, respondents were invited to provide additional comments. Some expressed that they had interest and/or concern about environmental issues but that their health issues refrained them from being more involved; some reported that the survey was a good initiative and/or that it incited reflection; and one expressed that some actions deemed to reduce their carbon footprint were in fact adopted as a consequence of their chronic disease (eg, lower meat consumption, using public transportation, reduced plane travels). Finally, one respondent expressed that he had experienced dialysis in different countries and informed that low-resource settings had more environmentally sustainable practices, and that some consumables varied across countries (eg, smaller dressings). Relevant quotes from respondents are reported in Table 2.
Relevant Quotes From Respondents About Ideas for Improvement to Limit the Environmental Impact of Kidney Care and Additional Comments.

Note. HHD = home hemodialysis; ICHD = in-center hemodialysis; PD = peritoneal dialysis.
Discussion
In this study, we report on the KAP of people receiving a dialysis therapy in a single center in Canada about climate change and the environmental impact of kidney care. We showed that most respondents (87%) felt informed about climate change at least at an average degree; and that roughly equal numbers of participants were either somewhat informed (46%) or conversely not at all informed (41%) about the environmental impact of health care services. About three-quarters of respondents were at least moderately concerned about climate change and about the amount of waste generated by dialysis treatments, and the levels of concern varied by dialysis modality. About a third of participants reported taking steps in their personal life to reduce their personal carbon footprint often or frequently, while a similar proportion wonder at every or most dialysis sessions if plastic dialysis equipment/supplies are recyclable. Most respondents (74%) reported rarely or never experiencing anxiety or guilt toward their personal or dialysis-related carbon footprint. However, these feelings were much more frequently reported in people receiving home-based dialysis (“often” for 50% of HHD respondents; “very often” for 55% of PD respondents).
To our knowledge, this is the first comprehensive evaluation of the perspectives of people on dialysis about climate change and the environmental impact of kidney care. An abstract previously reported the results of a survey of 125 patients and providers in India (25 people undergoing continuous ambulatory PD [CAPD] and 100 health care providers) as part of a pilot program using plastic pebbles repurposed from plastic waste, to determine their awareness of plastic neutrality and willingness to adopt sustainable dialysis practices. 27 Similar to our finding that knowledge about the environmental impact of kidney care was limited, 65% of Indian survey respondents did not know what sustainable kidney care is. Furthermore, all Indian patients disposed of plastic waste in regular trash bins, and 99% of participants in the survey (patients and providers) were willing to participate in awareness programs for environmental protection and safe plastic waste disposal. Our findings include greater concern among the third of study participants who were receiving home-based therapies for both climate change and dialysis waste, with people receiving PD reporting the highest degrees of concern, followed in turn by HHD, then ICHD. In fact, there was more concern about the amount of waste generated by dialysis treatment than for climate change. We suggest that these results are likely due to the ongoing requirement of people on home dialysis to manage the predominantly plastic waste burden of their therapies. This was recently emphatically described in an editorial by Ms Verdin, a person with a lengthy personal experience of PD and HHD in Canada, who stated that she was “painfully conscious that dialysis uses a lot of power, water, and supplies” while adding “Ask us where the waste is generated—we will tell you!”. 30 In addition, these differences in degree of concern between people on ICHD versus home-based therapies may also be driven by differing priorities and/or poorer health in those on in-center treatment. Lesser degrees of concern about climate change from people undergoing ICHD due to their health status were illustrated by additional comments provided by participants (eg, “Dialysis tires the body so less energy left for ecology” [translated from French]; Table 2). Finally, other unmeasured differences between participants on home therapies, compared with ICHD, may have influenced these perceptions (eg, socioeconomic status, autonomy level).
Irrespective of dialysis modality, 11% of overall participants reported “very often” experiencing guilt or anxiety feelings in relation with the dialysis carbon footprint, representing 4% of respondents receiving ICHD and 55% PD. Similarly, 12% of overall respondents reported “often” experiencing such feelings, representing six percent of respondents receiving ICHD and 50% HHD. While it should be noted that small numbers of participants were on home-based therapies (PD: 11 people; HHD: 10 people), the striking differences across modalities warrants reflection. Verdin et al 30 also described “guilt” and “embarrassment” related to disposal of her home dialysis waste. Interestingly, and sadly, people who experience the most guilt or anxiety related to the environmental impacts of their treatment are those who receive a lower impact modality, according to a recent comparative life cycle assessment of dialysis therapies. 34 In the Australian setting, CAPD, HHD and automated PD were shown to have 59%, 41% and 29% lower carbon impacts than ICHD. 34 Enacting calls of Verdin et al 30 for open discussions about the health impacts of climate change, resource stewardship and climate resilience, the psychological burden associated with waste generated by dialysis therapies might be mitigated through better stewardship of dialysis waste, improved dialysis products’ design to optimize recyclability, and by reassuring patients who select a home dialysis therapy through informed shared decision-making that—despite the waste evident to them—their treatment has lower environmental impact than ICHD.
To minimize any patient discomfort associated with asking about environmental implications of dialysis therapy, we collaborated with patient-partners (including co-author CC) to co-create and revise the questionnaire. Fortunately, the survey was generally well received, with 87% of participants denying any negative feelings triggered by the questionnaire. While these data are reassuring for patient engagement on the topic of ESKC, they highlight the sensitivity needed for safe participation for a significant number of people (13%).
Our study showed that a vast majority of respondents were either very (45%) or somewhat (45%) interested in obtaining more information about the bidirectional relation between climate change and kidney health/care, and an impressive 35% of participants were interested in becoming involved in ESKC initiatives. As many national and international societies are publishing best practice guidelines and recommendations for ESKC, we therefore suggest that patients be provided with opportunities to co-create sustainability strategies. 35 Furthermore, some bioethicists argue that environmental values should be considered in relation to patient autonomy 36 and that “green informed consent” 37 should be a component of shared decision-making between patients, caregivers and health care providers. At a minimum, health care systems and clinicians should be equipped to inform patients about environmental impacts of kidney therapies, and how such effects can be mitigated, and teams should seek active patient involvement in sustainable practices.
Our study has some limitations, including its small sample size, the potential limited generalizability of findings due to the single-center design in an urban center with low representation of Indigenous peoples, and a setting in which very few respondents had previously been impacted by extreme weather events. In addition, there are risks of subjective, selection (ie, participants may have been more environmentally minded people interested in the subject; and people without written or spoken fluency in English or French were not eligible), cognitive and social acceptability biases. Regarding the latter, it should be noted that analyses were conducted to compare results from participants requiring assistance for survey completion to determine whether their answers may have been influenced by social acceptability, which did not appear to be the case as people who required assistance generally reported being less concerned about climate change and experiencing feelings of guilt/anxiety less frequently. Finally, due to the small number of participants in each category, we opted for a descriptive approach to analyze the results and did not specifically address directionality to compare results across categories. These limitations should be balanced against some strengths. This is the first study of its kind, reporting on the perspectives of people on dialysis on this subject. Moreover, people with lived experiences were involved in the creation of the survey and the psychological impact of the survey on respondents was also evaluated. Furthermore, the availability of research personnel to assist participants in responding to the electronic survey ensured better representativity of a typical dialysis population, by permitting participation of people of diverse age and digital literacy. Finally, the environmental impact of the study itself was minimized by avoiding the use of paper.
In conclusion, this single-center survey showed that most people receiving a dialysis therapy who responded felt informed and at least moderately concerned about climate change. Higher level of concern about climate change and the amount of waste generated by dialysis treatment, as well as more frequent occurrence of guilt/anxiety about the carbon footprint of dialysis, were observed in people on home therapies (PD and HHD) compared with ICHD. It is hoped that these findings will serve as a foundational step to informing our approach to positive, psychologically safe and meaningful engagement, dialogue and quality improvement as we seek to embed ESKC. Future work by our group will aim to broaden the KAP assessment of this population in different settings and obtain qualitative data for a deeper understanding of the perspectives of people receiving dialysis therapies toward climate change and ESKC.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581261434815 – Supplemental material for Perspectives of People Receiving Dialysis About Climate Change and Environmentally Sustainable Kidney Care: A Knowledge, Attitudes and Practices Survey in Canada
Supplemental material, sj-docx-1-cjk-10.1177_20543581261434815 for Perspectives of People Receiving Dialysis About Climate Change and Environmentally Sustainable Kidney Care: A Knowledge, Attitudes and Practices Survey in Canada by Camilia Minville, Carven Cambry, Daphne Esquivel Sada, Éliane Boucher, Alexia Mihalache, Ximena Fabiola Iraheta Palacios, Shaifali Sandal, Caroline Stigant and Isabelle Ethier in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-pdf-2-cjk-10.1177_20543581261434815 – Supplemental material for Perspectives of People Receiving Dialysis About Climate Change and Environmentally Sustainable Kidney Care: A Knowledge, Attitudes and Practices Survey in Canada
Supplemental material, sj-pdf-2-cjk-10.1177_20543581261434815 for Perspectives of People Receiving Dialysis About Climate Change and Environmentally Sustainable Kidney Care: A Knowledge, Attitudes and Practices Survey in Canada by Camilia Minville, Carven Cambry, Daphne Esquivel Sada, Éliane Boucher, Alexia Mihalache, Ximena Fabiola Iraheta Palacios, Shaifali Sandal, Caroline Stigant and Isabelle Ethier in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-pdf-3-cjk-10.1177_20543581261434815 – Supplemental material for Perspectives of People Receiving Dialysis About Climate Change and Environmentally Sustainable Kidney Care: A Knowledge, Attitudes and Practices Survey in Canada
Supplemental material, sj-pdf-3-cjk-10.1177_20543581261434815 for Perspectives of People Receiving Dialysis About Climate Change and Environmentally Sustainable Kidney Care: A Knowledge, Attitudes and Practices Survey in Canada by Camilia Minville, Carven Cambry, Daphne Esquivel Sada, Éliane Boucher, Alexia Mihalache, Ximena Fabiola Iraheta Palacios, Shaifali Sandal, Caroline Stigant and Isabelle Ethier in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors would like to thank all survey participants for their time responding to the survey and the local in-center hemodialysis personnel for their assistance with our project. The authors would also like to acknowledge the members of the Canadian Society of Nephrology’s Sustainable Nephrology Action Planning committee for their contribution to the creation of the initial survey. Drs Ethier and Sandal are supported by the Chercheur boursier clinicien—Junior 1 award from the Fonds de recherche du Québec—Santé. Dr Stigant is supported by the Marcia Bell Distinguished Scholar Award.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Sandal has received an education grant from Amgen Canada to increase living donor kidney transplantation and improve outcomes of patients with graft failure. The rest of the authors have no relevant conflict of interest to disclose. The funding organizations had no role in the study design and conduct, data collection and management, interpretation of the results and manuscript preparation.
Data Availability Statements
The data supporting the results of this study will be made available on reasonable request to the corresponding author (IE) and following ethics approval and a contract agreement between institutions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.