
Abstract
Background:
There is growing interest in the nephrology community for environmentally sustainable kidney care (ESKC) to alleviate the environmental impact of kidney care services.
Objective:
This study aimed to assess the knowledge of Canadian kidney care providers regarding their program’s ESKC strategies.
Design, Setting, Participants, Measurements, and Methods:
An electronic survey, created by the Canadian Society of Nephrology-Sustainable Nephrology Action Planning committee, was distributed to Canadian kidney care providers.
Results:
A total of 421 Canadian kidney care providers responded to the survey. Various degrees of implementation of ESKC practices across the country were reported, with higher proportions of respondents reporting the use of strategies related to medication stewardship, clinical care consumables, virtual care options, office consumables, office equipment, and general waste management. It also highlighted the lack of knowledge of kidney care providers about many areas related to ESKC practices, such as energy sourcing, reverse osmosis reject water savings, procurement and product sourcing, as well as policies within the kidney program and contact with environmentally sustainable officers. Knowledge of respondents about certain strategies was also dependent on their role within the unit (eg, nephrologist vs nurse vs management), with nephrologists being relatively more aware of strategies that directly involve them, such as medication stewardship. Finally, variation across provinces was noted in terms of the incorporation of climate change adaptation or preparedness and environmental planning strategies.
Limitations:
The overrepresentation of people working in academic centers, as well as those from Quebec and British Columbia, may affect the generalizability of results. As respondents may be affiliated with the same units, results reflect knowledge of the individuals regarding the strategies, rather than the presence or implementation of such strategies across units.
Conclusions:
The ESKC practices from various domains are incorporated at different levels across the country, and there are important gaps in providers’ awareness of such strategies, depending on their role within the unit.
Keywords
Introduction
The environmental impact of health care is increasingly recognized, 1 as is kidney care’s disproportionately large contribution to this impact. Dialysis therapies have high energy and water use and generate large amounts of greenhouse gas (GHG) emissions from the production, transport, and disposal of consumables such as solutions, dialyzers, and dialysis tubing.2-5 Dialysis therapies also produce significant plastic waste from large-scale use of these consumables. In addition, emissions from patient and staff travel amount to 14% and 28% of program emissions in the United Kingdom 6 and the United States, 7 respectively. Pharmaceuticals, which account for 25% of Canadian health system emissions, comprised the largest single category of renal program emissions at 35%. 6
A growing number of experts, committees, and scientific societies8-15 have called for environmental stewardship in kidney care. Surveys of kidney care professionals regarding environmentally sustainable kidney care (ESKC) practices have been performed in 6 kidney care jurisdictions worldwide,16-21 in each case establishing a helpful baseline while identifying areas for improvement. An international survey of health care professionals involved in kidney care also highlighted differences in knowledge, attitude, and practices in ESKC across income level,22,23 while challenges in implementing ESKC in low- and middle-income countries have also been identified. 24
The mission of the Canadian Society of Nephrology’s (CSN) Sustainable Nephrology Action Planning (SNAP) committee is to educate, innovate, and advocate for ESKC. 25 In order to effectively change practice, an understanding of the baseline state of ESKC awareness and actions across Canada was deemed a priority. We conducted a gap analysis to identify research and practice priorities related to climate change and ESKC practices in Canada by completing a large nationwide survey of kidney care providers. The knowledge gaps related to climate change among Canadian kidney care providers have previously been reported. 26 In this article, we present an overview of the reported current knowledge of kidney care providers about ESKC practices and strategies in place across Canada, as well as those surrounding emergency preparedness and planning.
Methods
Approach
The CSN-SNAP committee created a cross-sectional knowledge, attitudes, and practice (KAP) survey in English and French, destined for kidney care providers across Canada via the CSN and collaborating societies’ distribution lists. The survey incorporated similar domains regarding ESKC practices integrated in previous surveys.16-18 The complete methodology for this survey has been published, 26 but briefly, it was self-administered electronically from March 9, 2023, to April 18, 2023, while hosted on the secured REDCap server of the Centre de Recherche du Centre Hospitalier de l’Université de Montréal (CHUM). Ethics approval was obtained from the ethics board of the CHUM (2023-11317, 22.256).
The complete survey is provided as a supplement. This study focuses on questions pertaining to respondents’ awareness of specific strategies aimed at mitigating the environmental impact of kidney care services and vulnerability of kidney care to climate change (Supplemental File 1—section C, p.6-18), providers’ perception of patient interest in ESKC (section C, p.4), and open-ended “additional comments” provided by participants at the end of the survey (section E).
Data Analysis
Descriptive analyses were used to assess ESKC practices across Canada, as reported by kidney care providers. Significant associations between participants’ characteristics (eg, job title, province of practice, etc) and responses to the survey were also evaluated, using the chi-square test. Analyses were performed using Stata/SE 15.1 for Mac (College Station, Texas), and a P-value <.05 was reported as statistically significant. Thematic analysis using an inductive approach to generate themes from text (generated by I.E. and confirmed by S.S.) was used to assess open-ended responses.
Results
Participant Characteristics
A total of 516 people participated in the survey, with the section on environmentally sustainable practices started by 421 individuals but completed by 386 respondents. We analyzed all responses, and for each section of the survey presented, the number of respondents is reported. There were no statistically significant differences in characteristics between those who completed the survey and those who provided incomplete responses (Table 1). Most respondents (80%) identified as women, and 27%, 31%, and 25% were aged 30 to 39, 40 to 49, and 50 to 59 years, respectively. Most respondents were either kidney nurses (42%) or consultant nephrologists (26%). The majority of respondents were from Quebec (37%), British Columbia (BC) (34%), and Alberta (14%). The main dialysis workplace was an in-center dialysis facility for about half (52%) of respondents, and a majority (64%) of participants worked in academic centers.
Participants’ Characteristics.

Note. There were no statistically significant differences between participants completing the survey vs participants providing incomplete survey responses.
Environmentally Sustainable Strategies
Power consumption
Questions related to lighting (n = 421), heating and cooling (n = 419), and energy savings (n = 416) are presented in Figure 1. Most respondents did not know if low-energy light bulbs were used (70%), if renewable energy is sourced (63%) or generated on site (58%), and if heating/cooling is turned off when the unit is not in use (58%). Among respondents who could provide an answer, less than a third selected the option always/very often for the following: use of low-energy light bulbs (32%), staff encouraged to turn off lighting when not in use (22%), motion sensors installed to regulate lights in low traffic areas (15%), heating/cooling turned off when unit is not in use (16%), renewable energy sourced (24%), and renewable energy generated on site (4%). Most participants (67%) reported that thermostats were always/very often set at appropriate temperatures (22-24°C as per the Canadian Standards Association [CSA] recommendation), and almost half (46%) reported that patients were always/very often permitted or encouraged to bring their own blankets.

Incorporation of lighting, heating and cooling, energy savings, office equipment, office consumables, water savings, and waste management strategies into participants’ kidney care services.
Office equipment and consumables
For strategies related to office equipment (n = 415) and office consumables (n = 411), most respondents were aware of their implementation (“don’t know”: ≤22%), except for the sustainable sourcing of paper (“don’t know”: 80%). The most frequently reported strategies were computers and photocopiers auto-configured to sleep/standby/hibernation mode when not in use (always/often: 77% and sometimes: 20%), recycling of used paper (62% and 30%), staff encouraged to log off computers when not in use (52% and 25%), and electronic documentation available as an alternative to paper (ie, e-mail use; 48% and 46%). Notably, the monitoring of printing/photocopying was never implemented according to 78% of respondents. Additional strategies were variably used: staff encouraged to switch off computers when not in use, printing/photocopying discouraged, printers/photocopiers set to double-sided, and paper sustainably sourced (Figure 1).
Water savings
In regard to water saving strategies (n = 408), most ([A] 72%; [B] 78%) respondents did not know if reverse osmosis (RO) reject water is collected and either (A) used as “gray water” for other building operations (ie, watering plants, use for toilets) or (B) resent through RO system again to minimize water consumption. The RO reject water was never collected and used as “gray water” or resent through RO system again according to 93% and 80% of those who could provide an answer. Water saving taps (sensor on/auto off function) were in place “always/very often” according to 40% and “sometimes” according to 42% of those who could provide an answer (Figure 1).
Waste management
Most respondents (n = 400) were aware of waste management strategies (“don’t know”: ≤34%), except for recyclable polyvinyl chloride (PVC) plastics being collected in a separate recycling stream, waste audits being regularly undertaken (ie, appropriate waste sorting into the bins provided) and product suppliers being requested to retrieve pallets and cardboard boxes at delivery (56%, 58%, and 78%: “don’t know,” respectively). According to most respondents who provided an answer, varying waste stream bins are available and appropriately sited (always/very often: 55% & sometimes: 38%); any batteries in unit operations are collected for recycling (56% and 35%); posters that correctly identify appropriate waste bins are available for referencing (34% and 49%); and staff is educated at time of workplace intake about appropriate management of clinical waste (38% and 34%). Interestingly, 34% of respondents did not know if staff receives education at time of workplace intake or ongoing/refresher as to appropriate management of clinical waste. This was driven mostly by nephrologists’ unawareness of such strategies (“don’t know”: 65%-68%). Ongoing staff education regarding waste management, regular audits, and retrieval of pallets/cardboard boxes by suppliers were infrequently reported by respondents who could provide an answer (never in 53%, 77%, and 54%, respectively). Although less than half of respondents knew if recyclable PVC plastics were collected in a separate recycling stream, more than half of those providing an answer were positive (always/very often: 28% and sometimes: 32%).
Clinical care consumables
Listed strategies pertaining to stewardship of clinical care consumables (n = 397) and medications (n = 396) were at least sometimes present according to 93% to 97% of respondents (Figure 2). Such strategies included preferential selection of materials nearing their expiry date to avoid wasteful non-use (always/very often: 54% and sometimes: 43%); movement of materials nearing expiry dates to front of storage area (63% and 33%); formalized product stewardship practices (eg, opening supplies only when needed; 56% & 38%); scheduled/routine medication reconciliation (eg, regular review of drug therapy; 73% and 23%); and preferential use of oral versus intravenous medications, when appropriate (62% and 33%).
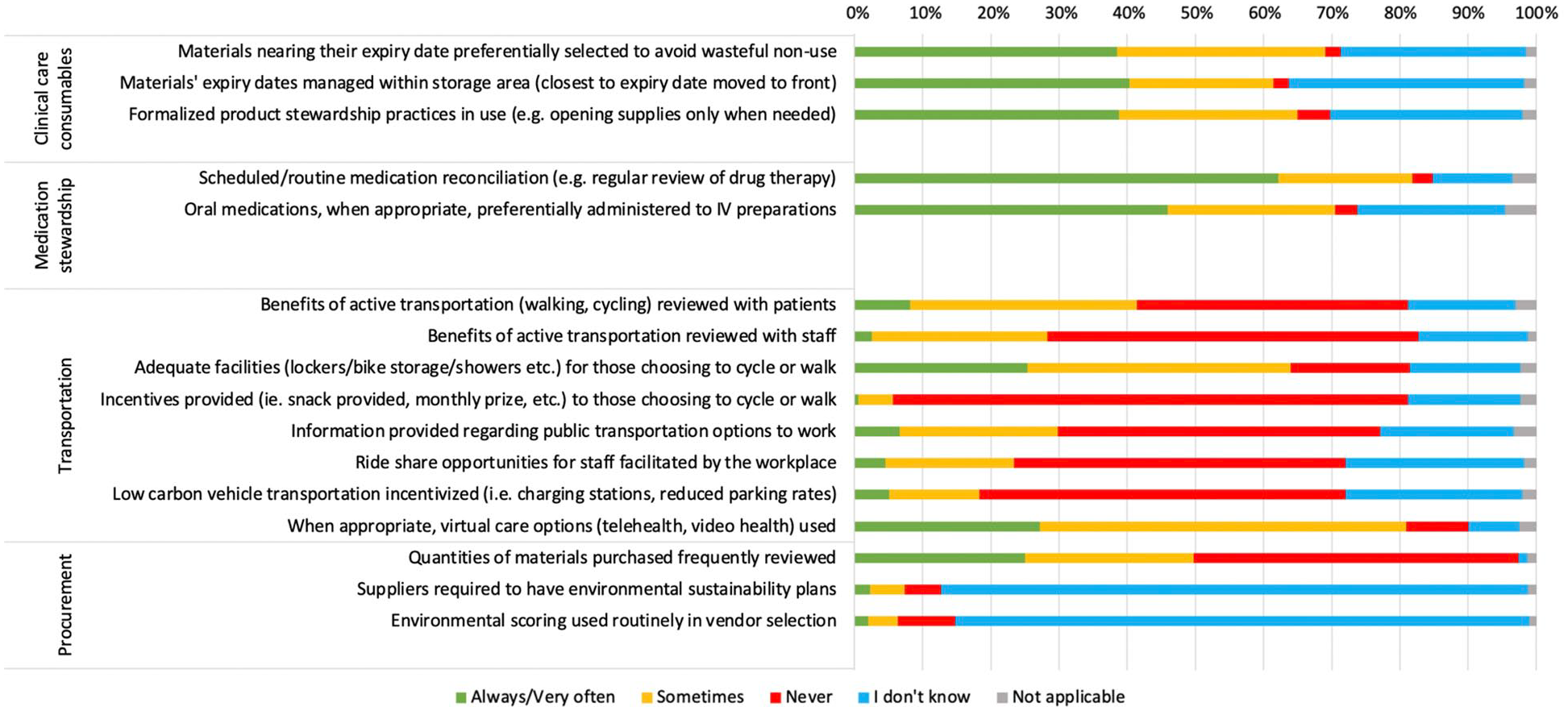
Incorporation of clinical care consumables, medication stewardship, procurement, and transportation strategies into participants’ kidney care services.
Procurement
Almost all respondents (99% of n = 393) were aware of the frequent review of quantities of materials purchased, and about half reported this being performed in their unit (always/very often: 26% and sometimes: 25%). However, about 85% of respondents did not know if suppliers are required to have environmental sustainability plans or if environmental scoring is used routinely in vendor selection. According to 42% and 57% of those providing answers, these strategies were never in place, respectively (Figure 2).
Transportation
Most respondents (n = 393) were aware of transportation strategies (“don’t know”: ≤26%; Figure 2). The use of virtual care options (telehealth, video health), when appropriate, was the strategy most frequently reported as available (always/very often: 30% and sometimes: 60%), followed by adequate facilities (lockers, bike storage, showers, etc) for those choosing to cycle or walk (31% and 47%) and review with patients of the benefits of active transportation (10% and 41%). Incentives for those choosing to cycle or walk (eg, snack provided, monthly prize, etc) were never in place according to 93% of respondents. Other transportation strategies were variably reported by the respondents providing an answer (25%-39%): review of the benefits of active transportation with staff, information provided regarding public transportation options to work, ride share opportunities for staff facilitated by the workplace, and low carbon vehicle transportation incentivized (ie, charging stations, reduced parking rates, etc).
Preparedness and Planning
Climate change adaptation or preparedness
Over 74% of 389 respondents were aware of climate change adaptation or preparedness strategies (“don’t know”: ≤26%; Figure 3). Staff and patients were at least sometimes informed about the health impacts of climate disasters (ie, heat waves, floods, fires) according to 40% of respondents providing an answer, while staff (39%) and patients (26%) were informed about the kidney care delivery impacts of climate disasters. Most reported that patients were provided a disaster plan (always/very often: 40% and sometimes: 22%), and about 75% reported that staff were aware of the workplace disaster plan and where/how to access these materials (43% and 32%).

Incorporation of climate change adaptation or preparedness and environmental planning strategies into participants’ kidney care services.
Environmental planning
About one third of respondents (n = 386) were not aware of most environmental planning strategies in their unit, while up to 57% and 52% of respondents did not know if environmentally sustainable policies are in place in their kidney program and if environmentally sustainable officers at the hospital, health authority, or provincial level liaise with or assist their kidney program, respectively (Figure 3). Of the respondents providing an answer, more than two thirds reported a complete absence of the following strategies related to environmental sustainability: policies in place in their kidney program (68%); environmentally sustainable improvement as a standing agenda item for unit meetings (86%); staff and patients encouraged to propose improvement ideas (71%); education provided at workplace education events (80%); environmental sustainability champions (81%) and teams (91%) identified in the kidney program; culture of developing, implementing, and improving existing work (67%); and environmental sustainability officers at hospital, health authority, and provincial-level liaise with their kidney program (87%). Overall, between 76% and 92% of respondents selected that environmental planning strategies were either never incorporated or that they did not know if they were.
Responses Pertaining to Patient’s Concerns About Recycling
Of the 380 respondents who reported working directly with patients on a dialysis unit, 43% responded that patients never asked if plastic dialysis (peritoneal or hemodialysis) equipment/supplies are recyclable, whereas 24%, 16%, 11%, and 5% of patients seldomly, sometimes, often, or almost always asked, respectively.
Association Between Participants’ Characteristics and Responses
No relevant association was identified between gender or age group and the responses provided. However, there were significant patterns identified between provinces and responses regarding climate change adaptation or preparedness strategies (Figure 4) and environmental planning strategies (Figure 5). The strategies were more likely to be reported as incorporated by respondents from BC, Alberta, and Saskatchewan, compared to Quebec. In addition, nephrologists were consistently less aware (responding “I don’t know”) than other categories of respondents for most strategies, except for strategies directly related to their work (ie, medication stewardship strategies, use of virtual care options). For example, compared to nurses, higher proportions of nephrologists were unaware of waste management strategies (“I don’t know”: 14%-90% for nephrologists vs 6%-78% for nurses but consistently higher for nephrologists for each waste category), clinical care consumables strategies (52%-63% for nephrologists vs 8%-18% for nurses), and the frequent review of quantities of materials purchased (64% for nephrologists vs 40% for nurses). In terms of climate change adaptation or preparedness and environmental planning strategies, nephrologists showed similar knowledge compared to nurses, while other categories of kidney care providers were less aware of these strategies.

Incorporation of climate change adaptation or preparedness strategies into participants’ kidney care services by province.

Incorporation of environmental planning strategies into participants’ kidney care services by province.
Additional Comments and Suggestions
Open-ended comments collated at the end of the survey fell into 6 thematic categories: (1) Feelings of eco-anxiety and awareness of environmental impact of kidney care services and impact of climate-related events on kidney care delivery; (2) using the survey as a learning/action planning opportunity and need for more education; (3) feeling of lack of impact from individual/local action and need for governmental/institutional engagement, collective action, guidelines, and action plans; (4) additional comments on environmentally sustainable strategies; (5) potential barriers to implementation of strategies (ie, unavailability of necessary facilities/resources; perceived competing priorities); (6) others (eg, thanks and show of interest for the subject [n = 20]; justification on unawareness of strategies due to job title/position [n = 3], etc). Relevant quotes from participants illustrating these themes identified are presented in Table 2, and more detailed comments are shown in Supplemental Table 1.
Relevant Quotes From Participant Responses From Invited Open-Ended Comments, by Identified Themes.

Note. BC = British Columbia; CSN = Canadian Society of Nephrology.
Discussion
This survey study of 421 Canadian kidney care providers showed varying degrees of implementation of a wide range of ESKC climate change mitigation and adaptation practices across the country. Although provincial variabilities were noted, at least 60% of respondents reported one or more environmentally sustainable strategies in their workplace. This highlights a growing recognition of ESKC in the Canadian kidney community as well as helps identify opportunities for improvements, as several strategies explored require simple implementation approaches or protocols, such as those related to medication stewardship; clinical care consumables management; virtual care options; and availability of waste bins and posters specifying proper waste sorting.
Noting that nearly 70% of survey respondents were either physicians or nurses, it is not surprising that a lack of knowledge was demonstrated regarding facility-level ESKC practices, such as energy sourcing, water stewardship, procurement practices, as well as policies within the kidney program and contact with regional environmental sustainability professionals. In fact, respondents in management or administration positions (7% of participants) showed greater awareness of the strategies incorporated in their program. Accordingly, respondents’ knowledge of specific strategies depended on their role within the unit (eg, nephrologist vs nurse vs management), with nephrologists being most aware of practices in which they are directly engaged, most notably medication stewardship. Overall, this highlights the need for targeted strategies to appropriately engage those who are most likely to champion and adopt them and allocating time and resources appropriately given the overstretched role of kidney care providers across the country. For example, while dialysis nurses and technicians can champion ESKC practices surrounding water management, office managers and administrators might be the delegated champions for implementation of ESKC practices surrounding office equipment and consumables. This was also highlighted in a recent opinion piece on patient, kidney donor, and care provider perspectives on ESKC, presenting insightful reflections on various strategies to engage with all involved stakeholders. 27
An important finding of this survey was the low awareness of kidney care professionals about the potential impacts of climate disasters on the health and stability of kidney care delivery, with less than 25% in the highest reporting jurisdiction (BC) reporting “always or very often” incorporation into kidney care services, and in the remaining jurisdictions between 40% and 95% of respondents either lacked knowledge or had no such information provided. This survey has helped our team identify approaches to improve climate resilience as a priority and to pursue research and practice initiatives surrounding disaster management.28,29
The questionnaire used was informed by previous surveys conducted in dialysis units that systematically explored ESKC practices16-18 across multiple domains of actions, from health care or hemodialysis specific (eg, medication stewardship, RO water collection and reuse, etc) to more general measures (eg, lighting, heating and cooling, office equipment and consumables, etc). In recent years, various working groups from other nephrology societies have published ESKC practice guidelines and recommendations with correspondingly general and dialysis-specific measures;30-33 some recommendations are more thematic, such as engaging in medication stewardship, 33 or raising awareness in eco-gestures, 31 whereas others are clear and specific actions, such as installing motion detectors with light timers or using LED lightbulbs.30-32 Our survey was designed to incorporate precise strategies that can be incorporated in kidney care programs. As such, responding to the survey itself was intended as a learning opportunity, not only for environmentally sustainable strategies but also to raise awareness on the impact of kidney care services on the environment. 16 The influence of completing a survey about climate change on the awareness of the issue has been previously demonstrated. 34
While previous survey studies on ESKC practices in dialysis units focused on practices in each unit, the present results were based on kidney care providers’ knowledge of such measures. The first survey of this kind, conducted in the United Kingdom from 2009 to 2010, was based on answers from a contact in each unit prepared to complete the survey, which were “predominantly Green Nephrology Local Representatives (individual staff members with widely differing roles within their local units, who were actively identified as part of the Green Nephrology Programme [. . .]).” 16 Surveys done in Australia and New Zealand,17,18 Italy, 20 and Portugal 19 targeted individual facilities by contacting dialysis units through either chiefs of nephrology departments, medical directors/heads of units, or nurse unit managers, with some offering the option to delegate the completion of the survey to an appropriate person within the facility.17,18 The Japanese survey 21 was circulated through the Japanese Association of Dialysis Physicians, and duplicate responses from the same facility were deleted. Response rates were highly variable in each of these surveys (Italy 19%, Japan 29%, Australia and New Zealand 33%, Portugal 59%, the United Kingdom 74%, and Australia [Victoria] 86%), and participation of dialysis units with greater knowledge, interest, or enthusiasm in ESKC practices was highlighted as potential bias in all studies.16-21 The present study highlighted many providers’ (in particular nephrologists) lack of awareness of ESKC strategies and emergency preparedness in their own unit. In addition, knowledge across domains of strategies also varied according to job title. Therefore, to better assess the implementation of ESKC practices in a dialysis unit, a multidisciplinary team would provide a more comprehensive report than any 1 individual. Of note, the implementation of some strategies directly involving providers (eg, staff educated at time of workplace intake and ongoing education/refresher about appropriate management of clinical waste) was unknown to a large proportion of respondents, which can be interpreted as either not being incorporated or, at the very least, not being memorable enough for providers to be aware of such practices.
While the distribution of the results may be biased due to numerous respondents potentially affiliated to the same programs, strategies related to climate change adaptation or preparedness varied across provinces. This variability may be due to variable levels of regional risk and past exposure to disasters. For example, strategies related to disaster plans were more frequently reported by respondents from BC, a province prone to forest fires, which are known to affect population health due to air quality changes.35,36 It should be noted that the survey was completed a few months prior to the forest fires, which strongly affected the province of Quebec in 2023.
Overall, the least incorporated domain of strategies in Canadian kidney care programs was environmental planning (ie, environmentally sustainable team/champion, policies, educational events, etc). Similar to our results, the Japanese survey 21 reported that 19% of facilities had policies or action plans for environmental sustainability and only 18% reported the formation of “green teams,” compared to 33% and 39% in Australia. 17 While recommendations by “green” working groups support both the establishment of environmental policies and of working groups/teams within units,30-33 in practice, these strategies rely heavily on the enthusiasm and commitment of motivated individuals. The leadership of “green” working groups and committees established within nephrology societies should be levered to encourage and support pertinent efforts of all members of kidney care teams. This multidisciplinary approach may thereby foster a sense of ownership and accountability from all. As such, one of the key themes identified in respondent’s open-ended comments was a need for higher-level engagement, including institution and administrative-level support, to aid collective action. The BC Renal’s Planetary Health Working Group has embedded environmental sustainability across its operations as a foundational principle and may serve as a useful example to jurisdictions similarly seeking to embed both climate change mitigation and resiliency aspects of ESKC practice to advance quality in kidney care. 37
The interpretations of our survey results must be considered in light of the following limitations. Although this study relied on responses from over 400 kidney care providers from across Canada, the overrepresentation of people working in academic centers and people from Quebec and BC may affect the generalizability of results. In addition, the targeted respondents for this survey were individuals (health care providers) who may be affiliated with the same units. Consequently, the results presented mostly reflect the knowledge of the individuals regarding the strategies, rather than the implementation of such strategies across units. In addition, our survey is at risk of non-respondent bias, as those with an interest in this subject are more likely to agree to participate in this study, as well as social acceptability bias. Although we did mitigate this risk as the survey was self-administered, participants may have selected more favorable responses.
Conclusions
Our survey provides insightful information on Canadian kidney care providers’ awareness of ESKC practices within their unit and highlights the importance of developing an approach to advancing ESKC in Canada. This baseline assessment is part of our ongoing initiatives to strengthen climate adaptation and mitigation approaches on a large-scale system level, involving the range of kidney care stakeholders. Our survey highlights several simple and pragmatic approaches that kidney care facilities across the country may consider implementing to decrease the environmental burden attributed to kidney care.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251365337 – Supplemental material for A Gap Analysis to Assess the Implementation of Environmentally Sustainable Kidney Care Strategies in Canada
Supplemental material, sj-docx-1-cjk-10.1177_20543581251365337 for A Gap Analysis to Assess the Implementation of Environmentally Sustainable Kidney Care Strategies in Canada by Isabelle Ethier, Shaifali Sandal, Ahmad Raed Tarakji, Bhavneet Kahlon, Ratna Samanta and Caroline Stigant in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors would like to thank all survey participants for their time responding to the survey, as well as the Canadian Society of Nephrology, the Société Québécoise de Néphrologie, the Canadian Association of Pediatric Nephrologist and the Canadian Association of Nephrology Nurses, and Technologists for disseminating the link to the survey to their members. Drs I.E. and S.S. are supported by the Chercheur boursier clinicien—Junior 1 award from the Fonds de recherche du Québec—Santé.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr S.S. has received speaking honorarium from AstraZeneca and an education grant from Amgen Canada to increase living donor kidney transplantation and improve outcomes of patients with graft failure. The rest of the authors have no relevant conflict of interest to disclose. The funding organizations had no role in the study design and conduct, data collection and management, interpretation of the results, and manuscript preparation.
Data Availability
The data supporting the results of this study will be made available on reasonable request to the corresponding author (I.E.) and following ethics approval and a contract agreement between institutions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.