
Abstract
Background:
Individuals with advanced chronic kidney disease benefit from an integrated palliative approach to care through timely advance care planning and discussions about their goals of care. Despite literature and guidelines emphasizing the need for advance care planning in chronic kidney disease management, treatment-focused approach remains the norm, partly due to provider reluctance and discomfort in engaging in advance care planning conversations. In British Columbia (BC), the Integrated Palliative Nephrology (IPN) project was launched to enhance kidney health care provider engagement in advance care planning and goals of care discussions, to train kidney health care providers in the province to initiate serious illness conversations, and to develop standardized resources for patients and providers across a provincial renal network.
Objective:
As part of the quality improvement, this study highlights the barriers/challenges and enablers to engage in advance care planning for health care providers of adult patients with chronic kidney disease.
Design:
A multi-methods approach was used.
Setting:
British Columbia, Canada
Participants:
Kidney health care providers who worked in nondialysis and dialysis care settings
Methods:
Data were collected through semistructured surveys, individual interviews, and focus groups with health care providers across the province who care for patients with chronic kidney disease.
Results:
The results of a kidney health care provider survey (n = 90) showed self-reported improvements in knowledge of the integrated palliative approach and competency and comfort engaging in advance care planning discussions. The results of one-on-one interviews (n = 15) and focus groups (n = 32) with kidney health care providers showed that taking a relational approach with patients, enhancing provider comfort and competency with advance care planning, clarifying roles and responsibilities around who should engage in advance care planning conversation was beneficial to patient care. Supporting cohesion among care teams around the goal of advancing an integrated palliative approach, and offering mentorship and targeted education and resources for the kidney care team, can enable effective advance care planning discussions.
Limitations:
The study was limited by purposive sampling, a small sample size, and potential bias due to participant interests and settings.
Conclusions:
For kidney health care providers, targeted education and resources, clarity around roles and responsibilities, and long-term relationships with patients may help advance the cultural shift from treatment focus to integrating palliative care across the continuum of the illness journey.
Trial registration:
Not registered.
Introduction
Much of clinical practice for advanced chronic kidney disease (CKD) has emphasized treatment and disease management, with a focus on dialysis and transplantation. However, individuals with advanced CKD need an integrated palliative approach to care which holistically addresses what matters most to them and helps to enhance their quality of life.1,2 This includes timely advance care planning (ACP), discussions about their goals of care, and a palliative approach throughout the continuum of their illness journey. Patients and their families have consistently expressed a preference to discuss ACP with health care providers,3-6 but these conversations rarely occur,7,8 despite guidelines emphasizing the need for ACP in dialysis and CKD management.9,10
Moving from a treatment-focused approach to an integrated palliative approach to CKD management requires a shift in practice and culture. Provider reluctance and discomfort have been identified as common barriers to integrating ACP,11-13 which has prompted the need for education and skills-building. Beyond understanding clinician motivation at the individual level, Holley and Davison note the importance of understanding health care structures and processes for implementing ACP programs, 14 and Paladino et al 11 have highlighted the role of organizational context and implementation strategies. Therefore, a shift in practice and culture to integrate ACP and palliative care in advanced CKD management and dialysis requires a multi-level understanding and effort.
The goals of the Integrated Palliative Nephrology (IPN) project in the province of British Columbia (B.C.), Canada were to enhance provider engagement in ACP and goals of care discussions, to train kidney health care providers to initiate serious illness conversations (SIC), and to develop standardized resources for patients and providers. The IPN project was part of a larger initiative that began in 2004 to shift toward integrating a palliative approach to advanced CKD care in B.C. 15 In 2018, BC Renal conducted an environmental scan that revealed significant gaps in palliative care within the provincial kidney care network. Findings from the environmental scan informed the development of the IPN project carried out from 2018 to 2022. The key components of this project were building capacity to enhance provider engagement in ACP and goals of care discussions with patients; training health care providers to initiate SIC; and developing a variety of standardized patient and provider resources. The project emphasized on capacity building, fostering cultural change, sharing knowledge, and developing resources to support the integration of palliative care within advanced CKD management.
In August 2022, a project evaluation was completed to assess effectiveness by gaining an understanding about the experiences of patients and care team members, and to gather suggestions for future actions and recommendations. This article reports on the barriers and enablers identified in the evaluation, as reported by kidney health care providers, to engaging in ACP with individuals with advanced CKD.
Methods
A multi-methods approach was used. Data were collected through semistructured surveys, individual interviews, and focus groups with kidney health care providers across the province who care for patients with chronic kidney disease to promote equity and participation.
A web-based semistructured survey was adapted from Weissman et al 16 (Supplemental material 1) It included questions regarding clinician comfort level with palliative care conversations, knowledge, and skills. kidney health care providers were asked to rank their knowledge, ability, and comfort level on various components of the palliative approach to kidney care using 5-point Likert scales. An invitation with survey link was emailed to kidney health care team members across the province. The survey was live from November 2021 to December 2021. A total of 90 fully completed survey responses were collected from five Health Authority Renal Programs in BC. The results were analyzed using descriptive statistics.
A semistructured interview guide was adapted from Heyland et al 17 and used for the interviews and focus groups (Supplemental material 2). The 30-minute interviews were conducted via videoconferencing or phone by YR and SW. A purposive sampling method was used to ensure each region and treatment modality was represented. Individual interviews were conducted with 15 clinicians, including social workers, nephrologists, pharmacists, nurses, and dietitians, with representation from the five regional health authorities across diverse geographical settings.
The 30-minute focus groups were conducted via videoconferencing with provincial committees or community of practice groups consisting of providers who work broadly in kidney care or the home dialysis modality setting, with GH or SS facilitating the discussion. Convenience sampling was used for interviews and focus groups utilizing the established groups in the provincial network. The interviews and focus groups were conducted from December 2021 to March 2022.
The data from interviews and focus groups were categorized using NVivo qualitative data analysis software (QSR International, Burlington, Massachusetts). Thematic analyses methods were applied by YR.18,19 We utilized the Consolidated Framework for Implementation Research (CFIR)20-22 to inform the structure of this analysis at the level of the health system and culture, organization, and individuals with CKD and health care providers (see Figure 1).
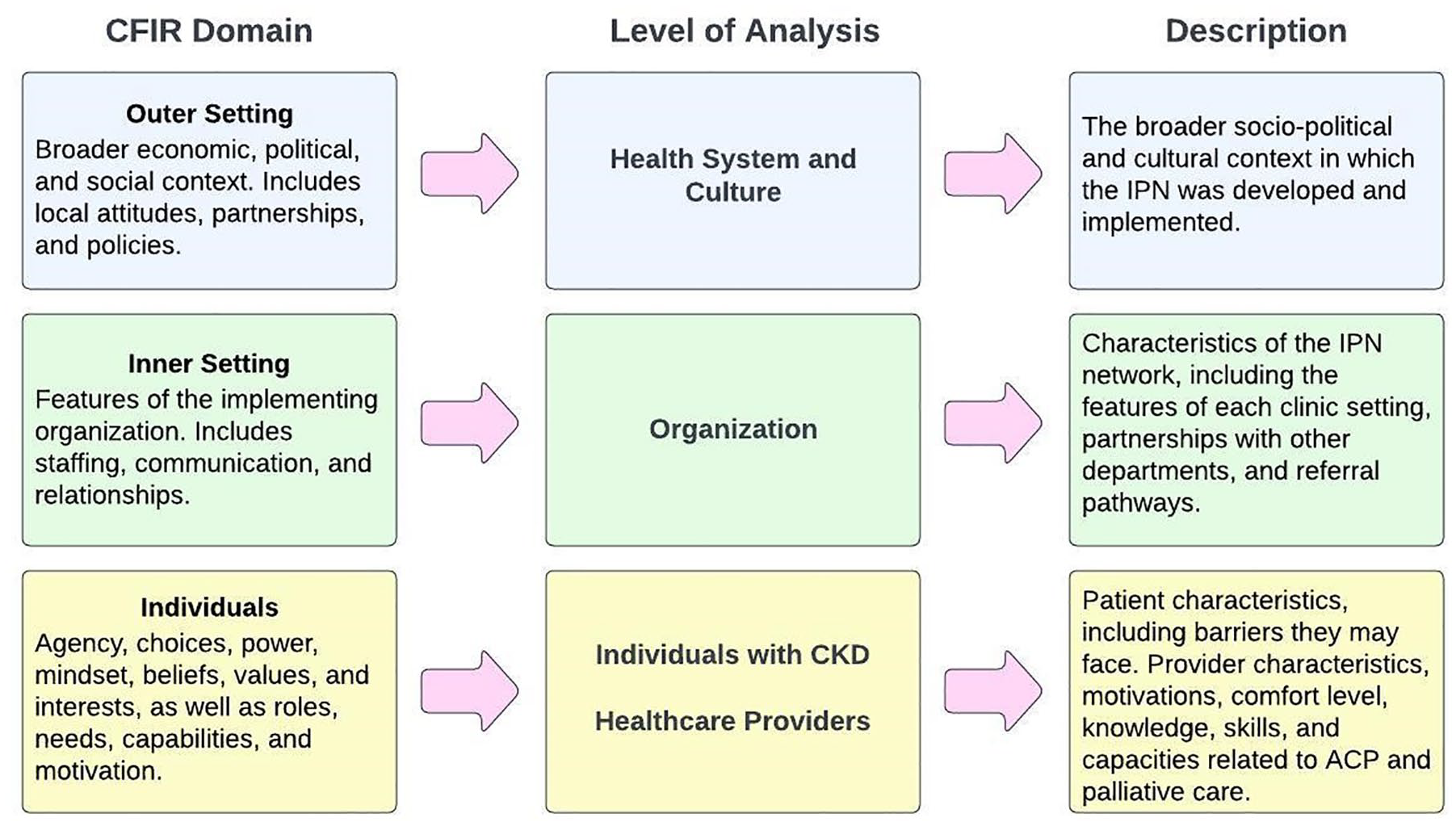
Consolidated framework for Implementation research (CFIR) domains adapted to levels of analysis.
Results
Ninety survey responses were collected. Individual interviews were conducted with 15 clinicians, including social workers, nephrologists, pharmacists, nurses, and dietitians, with representation from the 5 regional health authorities across diverse geographical settings (eg, rural and remote, urban). Three focus groups were conducted with a total of 32 providers from the provincial Peritoneal Dialysis Nurses Group, the Home Hemodialysis Educators, and the Palliative Care Committee coordinated by BC Renal. See Table 1 for demographic details of all participants.
Demographic Details of Interview, Focus Group, and Survey Participants.

Includes nonclinical personnel, such as renal managers, data coordinators/statisticians, care aids, and clerical technicians.
Information not collected.
Includes nonclinical settings, such as administration and data coordination.
Health Care Provider Survey
Approximately 60% of providers “agreed” or “strongly agreed” that their knowledge about the palliative approach to care had increased over the duration of the IPN project. Almost half (48%) “agreed” or “strongly agreed” that their ability to have ACP discussions with their patients and family members had improved.
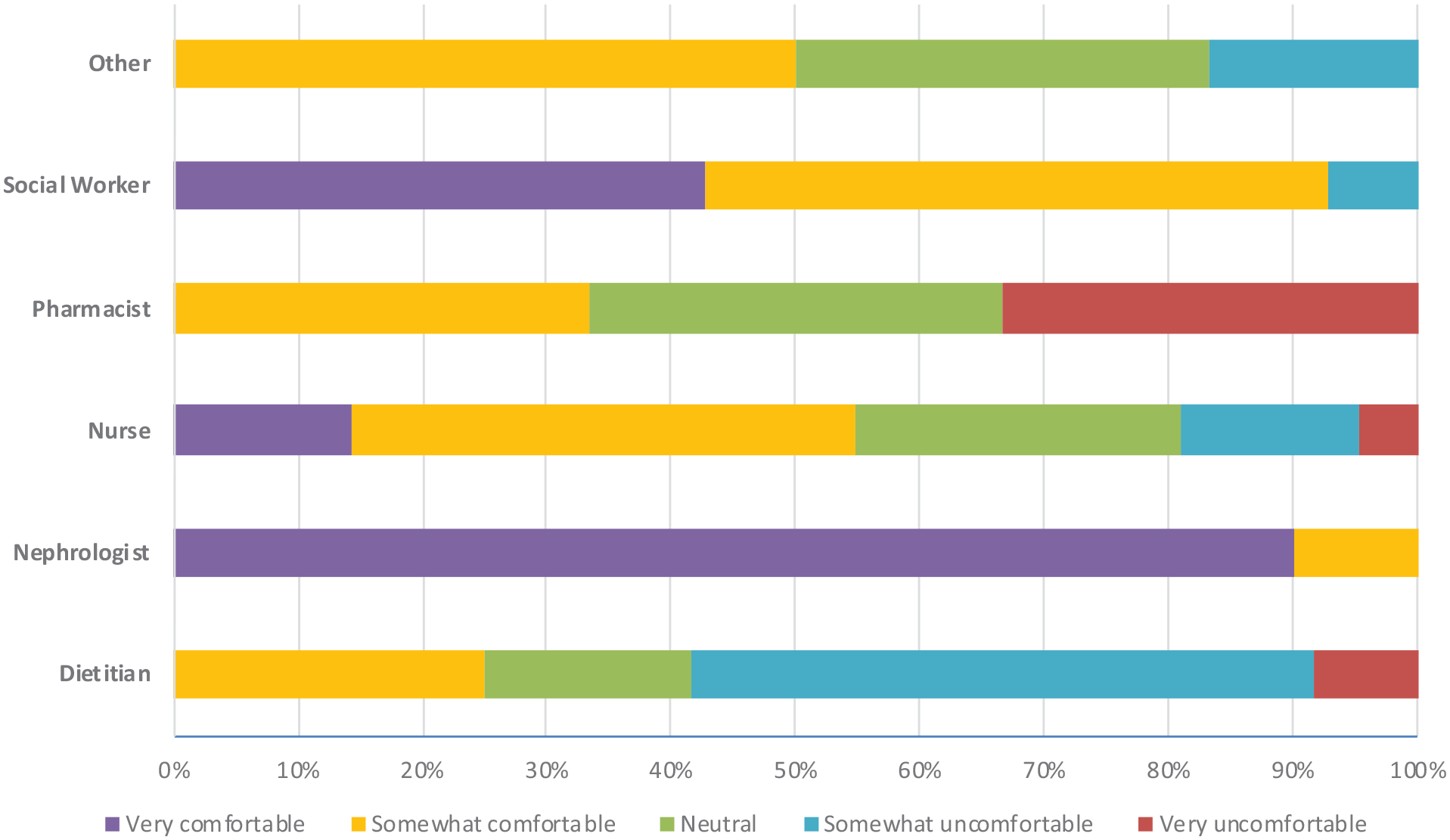
Most providers reported feeling “very comfortable” or “somewhat comfortable” discussing bad news (53.3%) and a shift in treatment approach from intensive care to conservative care (60.0%). When the level of comfort was analyzed by clinician type (see Figures 2 and 3), pharmacists and dietitians reported greater discomfort giving bad news, while nephrologists, social workers, and nurses reported greater comfort.

Kidney health care provider survey results: comfort level giving bad news to an individual or family member (percentage of providers by role).
Kidney health care provider survey results: comfort level discussing a shift in treatment approach from intensive care (including renal replacement therapy) to conservative care (percentage of providers by role).
Health Care Provider Interviews and Focus Groups
Tables 2 and 3 summarize the themes, along with transcript excerpts, regarding the barriers and challenges to, and enablers of, engaging in the palliative approach and discussions about ACP that emerged from the individual interviews and focus groups.
Themes and Interview Excerpts: Barriers and Challenges.

Note. HD = hemodialysis; PD = peritoneal dialysis; All = kidney care settings, including HD, home HD, PD, and kidney care (nondialysis).
Themes and Interview Excerpts: Enablers.

Note. HD = hemodialysis; PD = peritoneal dialysis.
Barriers and challenges
Health system and culture
Tension between care driven by disease-specific therapies and palliative care: Providers pointed to challenges within the health system where there were separate approaches to care—palliative and CKD—although 1 social worker said that “there’s been a shift in the culture of talking about palliative approach to care that I think is more open now.”
Virtual care limitation: During the COVID-19 pandemic, the dependence on virtual care via phone and video visits challenged providers further in engaging in these discussions.
Organization
Delayed ACP discussions: Despite the project goal to support the integration of ACP and palliative care across the continuum of an individual’s illness journey, providers shared that ACP discussions occurred after the optimal time.
Lack of clarity around roles and ownership of ACP discussions in care teams: In general, the responsibility for discussing ACP fell on the nephrologist or the social worker as it appears that certain kinds of information, conversations, or decision-making authority were best suited for specific disciplines. However, this perception was not consistent among the providers, some of whom felt it was the responsibility of everyone in the care team.
Health care provider
Provider discomfort: Most providers stated feeling some level of discomfort in discussing ACP and palliative care with patients and their families. Sometimes, providers may not feel certain about the accuracy of the information they offer to patients, which may contribute to their feeling of discomfort.
Disagreement with values and expectations from patients: There were descriptions of providers experiencing tension when there was a misalignment with a patient’s choice and the provider’s recommendation.
Lack of established relationship with the individual: For providers who did not have a long-term relationship with a patient, the lack of rapport could make it difficult to initiate a difficult conversation.
Provider burnout: The discussions could be draining, which was particularly challenging amid competing priorities when the strain on providers was particularly high. In addition, providers also needed to respond to nonclinical needs which require time and capacity that could otherwise be devoted to ACP discussions.
Individual with CKD
Lack of readiness to discuss ACP: The providers stated that, for the most part, individuals with CKD were positive and receptive to discussing ACP. When they were not receptive, the providers felt this was related to not being ready or feeling overwhelmed by the information offered to them. Specifically, providers perceived that some patients seem to misunderstand the purpose of ACP discussions. Lack of information about ACP also created confusion around patients’ perceptions of illness and care options, including continued dialysis.
Family and cultural dynamics: Even if an individual with advanced CKD was ready to discuss ACP and had sufficient knowledge about palliative care, family members could have opinions and preferences regarding care that were different from the those of the patient. Cultural differences contributed to the role of family members as well as attitudes and perception of life and death which could pose a challenge among some providers in approaching ACP conversations with patients.
Socioeconomic challenges: Providers stated that education levels and financial stability of a patient could affect their understanding of the health care system and their ability to advocate confidently for their own well-being.
Enablers
Health system and culture
Cultural shift toward integrating palliative approach in advanced CKD: In general, providers stated that the culture shift toward integrating a palliative approach in advanced CKD management was taking place. A key factor was creating a culture of openness to discuss with patients and other providers broadly, using a provincial focus on data collection, program quality data reviews, standardized treatment options education, and tracking of the ACP conversations.
Linkages between kidney health care providers and palliative care: Receiving mentorship from providers already trained in the palliative approach outside of kidney care was supportive.
Organization
Professional training, resources and support: Structured training and resources were helpful, particularly for professions for whom ACP was not traditionally seen as within their scope of practice. More interactive and less formal support for providers, with close collaboration with palliative care or regular debriefing with colleagues, were also thought to be supportive. Several providers highlighted the importance of learning from their peers by informally observing them or by teaching/learning from each other.
Care team cohesion and clarity of roles: This included regular meetings and conversations with other members of the care team, engaging in shared training, and recognizing and working with the strengths and experience of other team members toward a shared goal of supporting patients and their families. This rapport among providers could extend beyond the clinic to other non–kidney health care providers, particularly the primary care physician. It was deemed productive when several providers within a care team perceived this as a shared responsibility. Furthermore, having clear roles based on professional scope and strengths of each discipline seemed to contribute to better team cohesion. In particular, the role of the nephrologist was emphasized as anchoring and leading the care team in integrating ACP into each patient’s care plan.
Health care provider
Experiential knowledge: Through time and experience, providers gained skillsets and a personal approach for navigating potentially uncomfortable conversations.
Relational approach for better patient engagement: Providers learned the importance of a relational approach to effectively engage individuals with CKD in challenging conversations. Providers used the terms “trust,” “rapport,” and “respect” and emphasized the importance of giving people time and space to absorb the information and make decisions, being nonjudgmental about their choices, recognizing one’s own biases, and placing the patient at the center.
A sense of commitment: This sensibility and personal commitment could help providers move through the discomfort of having these conversations.
Discussion
The results show that a relational approach to longitudinal care is vital for advancing the cultural shift from treatment focus to integrating palliative care across the continuum of the CKD journey. The findings are consistent with other studies involving individuals with advanced CKD, which show that it takes time for patients to gain a full understanding of the care options and supports available to them. 23 Therefore, it is important to engage in ACP discussions early and regularly and offer education and support as needed.11,24 As individuals with CKD have been reported to value trust and rapport in their care, 7 providers in this study also described building trusting relationships with patients over the course of their care and prioritizing empowerment of individuals with CKD as factors that enabled their engagement in ACP discussions. Kidney care teams are uniquely positioned to establish long-term relationships with individuals with CKD and facilitate earlier and more frequent ACP conversations. ACP conversations can be complex and elicit difficult emotions; therefore, considerations should be applied to optimize use of virtual and in-person care to support this aspect. 25 Virtual care can present additional challenges in maintaining this relational approach which can be addressed with a considered approach.
Similar to findings in other studies, the providers in this study expressed discomfort and uncertainty around having conversations with patients and families about ACP and palliative care.11,26 Providers pointed out that greater clarity of roles and responsibilities around ACP conversations, cohesion among team members, and training and mentorship both within CKD clinics and with palliative care could help curtail the discomfort and uncertainty. Strong cohesion amongst the care team members, a shared vision of integrated palliative care, regular meetings to discuss cases and strategies, and a supportive environment of learning from one another have also been identified as instrumental enablers in similar studies on providers engaging in serious illness conversations.11,24 Other studies have noted the importance of fostering a culture of openness and interdisciplinary conversations, embedding the philosophy of integrated palliative approach into data collection and program evaluations, and creating formal linkages and collaborations with palliative care.26,27 These steps require institutional leadership and commitment, which have been identified as an important aspect of successful integration of ACP and palliative approach to CKD care. 12
The providers in this study desired targeted education and resources to provide guidance around ACP conversations and treatment options. Many also noted challenges related to providing care for individuals and families from diverse backgrounds. Consistent with other observations in the literature on advanced CKD care, cultural differences with respect to end-of-life care and the role of the family,28,29 and tensions and challenges that emerge in family dynamics in general,23,26,28,29 are common in ACP. Further, these results echo other findings that socioeconomic disadvantages experienced by individuals with CKD could be associated with decreased capacity for self-advocacy (eg, due to less formal education or less financial stability) which can be a barrier to patient empowerment. 7 Training for providers in cultural competency and safety when supporting individuals and families of diverse cultural and socioeconomic backgrounds will be supportive. Professional language interpretation service (including technology-assisted options) would also be beneficial when language barriers may exist, rather than relying on family members, to ensure accuracy. Additional supports for providers may include opportunities and resources around self-care and self-reflection, as well as support for debriefing.
This study was limited by purposive sampling. There is a potential for missing perspectives due to limited availability of providers to participate in the study. The participant settings can influence the data collected as a limitation of this study. Sample size was limited albeit reflecting a cross section of kidney care professions and different types of care settings. The findings are subject to possible reporting bias as some interview and focus group participants have a vested interest in a palliative approach to care. Validation of participant responses, which could strengthen the validity of the findings, was not undertaken. Additional studies that include a larger sample of frontline providers not involved in the provincial committees and the inclusion of perspectives of individuals with CKD may provide more comprehensive insights.
The study was strengthened by the use of multi-methods. The study scope—a provincial renal network—allowed us to examine a system as a whole. The findings are interpreted in the context of a publicly funded provincial renal network.
Conclusion
This study highlights the importance of role definition within a multidisciplinary kidney care team, targeted resources to support team efforts in ACP and the need for team organization care provider to work collaboratively to support the ACP conversations with patients. Long-term relationships with patients, common to CKD care, may enhance an integrated palliative approach across the continuum of the illness journey. The shift to this approach can be facilitated by enhancing provider comfort and competency, clarifying roles and responsibilities, supporting cohesion among care teams, and offering mentorship and targeted education and resources for all members of the kidney care team. Future research on the longitudinal impacts of the integrated palliative approach, enabled by timely ACP, on provider satisfaction, quality of care, and patient outcomes and experience will contribute to this growing field of literature in nephrology and potentially all areas of health care that support individuals with chronic life-limiting illness.
Supplemental Material
sj-pdf-1-cjk-10.1177_20543581251350891 – Supplemental material for Enablers and Barriers to Integrating Advance Care Planning in Chronic Kidney Disease Care in a Canadian Provincial Network
Supplemental material, sj-pdf-1-cjk-10.1177_20543581251350891 for Enablers and Barriers to Integrating Advance Care Planning in Chronic Kidney Disease Care in a Canadian Provincial Network by Helen H.L. Chiu, John Duncan, Sherri Lynn Kensall, Yanchini Rajmohan, Sushila Saunders, Sarah Thomas, Salma Wadhwania and Gaylene Hargrove in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-pdf-2-cjk-10.1177_20543581251350891 – Supplemental material for Enablers and Barriers to Integrating Advance Care Planning in Chronic Kidney Disease Care in a Canadian Provincial Network
Supplemental material, sj-pdf-2-cjk-10.1177_20543581251350891 for Enablers and Barriers to Integrating Advance Care Planning in Chronic Kidney Disease Care in a Canadian Provincial Network by Helen H.L. Chiu, John Duncan, Sherri Lynn Kensall, Yanchini Rajmohan, Sushila Saunders, Sarah Thomas, Salma Wadhwania and Gaylene Hargrove in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors are grateful for the feedback from all survey, interview, and focus group participants. We also acknowledge Helen Kang for her assistance in preparing the manuscript for publication.
Ethical Considerations
The IPN project evaluation was proceeded as a limited risk study exempt from full review of institutional research ethics board. HC, YR, SS, ST, and SW are staff members at BC Renal. GH, JD, and SLK receive a stipend from BC Renal for their roles as chair and vice chairs of the provincial Palliative Care Committee. All authors report no other conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The evaluation of the IPN project was funded via BC Renal internal funding for quality improvement.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.