
Abstract
Background:
End-stage kidney disease is associated with a 10- to 100-fold increase in cardiovascular mortality compared with age-, sex-, and race-matched population. Cardiopulmonary resuscitation (CPR) in this cohort has poor outcomes and leads to increased functional morbidity.
Objective:
The aim of this study is to assess patients’ preferences toward CPR and advance care planning (ACP).
Design:
cross-sectional study design.
Setting:
Two outpatient dialysis units.
Patients:
Adults undergoing dialysis for more than 3 months were included. Exclusion criteria were severe cognitive impairment or non-English-speaking patients.
Measurements:
A structured interview with the use of Willingness to Accept Life-Sustaining Treatment (WALT) tool.
Methods:
Demographic data were collected, and baseline Montreal Cognitive Assessment, Patient Health Questionnaire–9, Duke Activity Status Index, Charlson comorbidity index, and WALT instruments were used. Descriptive analysis, chi-square, and t test were performed along with probability plot for testing hypotheses.
Results:
Seventy participants were included in this analysis representing a 62.5% response rate. There was a clear association between treatment burden, anticipated clinical outcome, and the likelihood of that outcome with patient preferences. Low-burden treatment with expected return to baseline was associated with 98.5% willingness to accept treatment, whereas high-burden treatment with expected return to baseline was associated with 94.2% willingness. When the outcome was severe functional or cognitive impairment, then 45.7% and 28.5% would accept low-burden treatment, respectively. The response changed based on the likelihood of the outcome. In terms of resuscitation, more than 75% of the participants would be in favor of receiving CPR and mechanical ventilation at their current health state. Over 94% of patients stated they had never discussed ACP, whereas 59.4% expressed their wish to discuss this with their primary nephrologist.
Limitations:
Limited generalizability due to lack of diversity. Unclear decision stability due to changes in health status and patients’ priorities.
Conclusions:
ACP should be incorporated in managing chronic kidney disease (CKD) to improve communication and encourage patient involvement.
Introduction
End-stage kidney disease (ESKD) is associated with a significant increase in cardiovascular mortality and morbidity compared with age-, sex-, and race-matched general population controls. 1 Cardiopulmonary resuscitation (CPR) has a poor outcome among ESKD patients, with a reported 8% to 21.9% of patients receiving CPR surviving until hospital discharge2,3 and a median survival of 5 months post-discharge. 3 A substantial proportion of patients receiving CPR will have severely diminished functional outcomes post-CPR.4,5 Sudden unwitnessed death is also a frequent cause of death among ESKD patients, suggesting that arrhythmias leading to cardiac arrest occur quite frequently. 6
The ESKD patients sometimes have either uncertain or overly optimistic expectations about their prognosis 7 and this could potentially contribute to inappropriately intensive patterns of end-of-life care. Limited engagement in advance care planning (ACP) could lead by default to more patients receiving CPR8-10 and the continuation of dialysis for longer in the setting of advanced morbidity and in end-of-life situations than may be appropriate. 8
This highlights the importance of having early and transparent communication about ACP and establishing goals of care to respect patient autonomy. Also, there is a growing need to assess ACP benefits on patient care with reported favorable outcomes in levels of anxiety, depression, and posttraumatic distress among patients’ surrogates when ACP is in place.11-17
Not infrequently, nephrologists are very involved in the end-of-life care decision-making for their patients when they develop serious illness and capacity is in question. Misunderstanding patients’ preferences might lead to delivery of unwanted medical intervention or, alternatively, to inappropriately withholding treatment.18,19 There is a high discrepancy between patients’ attitudes and physicians’ views about CPR reported in the literature.20-23 Frequent end-of-life care discussions can provide more insight and provide valuable assistance to patients in the process of decision-making. 24 In this study, we aim to explore dialysis-dependent patients’ preferences toward ACP and resuscitation. Secondarily, we will assess how mild cognitive impairment, depression, and functional capacity may influence discussions regarding ACP and CPR preferences.
Materials and Methods
Study Design, Setting, and Participants
This was a 2-center cross-sectional study design to assess dialysis patients’ preferences on resuscitation, using a questionnaire delivered during a structured interview. It involved 2 dialysis units in the SAOLTA University Health Care Group under the governance of the Galway University Hospitals and Mayo General Hospital, respectively, providing hemodialysis, peritoneal dialysis, and home hemodialysis therapies. All adult (age more than 18 years) ESKD patients established on dialysis treatment for more than 3 months were approached to be recruited in the study. Patients who had communication barriers in the form of severe cognitive impairment or patients who were not able to understand English were excluded from the study (as the tool was in English). This was performed during a routine clinic visit or a hemodialysis session with recruitment of eligible patients from June 2020 through December 2020.
Questionnaire
The questionnaire was delivered during a structured one-to-one interview by a trained health care professional after obtaining fully informed consent. Baseline demographic data collected included the date of birth, sex, living arrangement, type of dialysis, date of commencing dialysis, and belief in God. A Montreal Cognitive Assessment (MoCA) 25 was performed to screen for cognitive impairment, Patient Health Questionnaire–9 (PHQ-9) 26 was performed to objectify depression symptoms, Duke Activity Status Index (DASI) 27 was performed to assess functional capacity, and Charlson comorbidity index (CCI) 28 was performed to reflect comorbid burden of disease. The patients’ attitudes toward ACP and CPR were tested using Willingness to Accept Life-Sustaining Treatment (WALT) instrument,29,30 the presence of surrogate decision-makers, preference of place of death, and delivering two validated questions about mechanical ventilation and CPR.
Montreal Cognitive Assessment
Cognitive impairment is relatively prevalent in the dialysis populations31,32 and this has significant implications for care. The MoCA instrument is a brief instrument used to screen for cognitive impairment presented as a 1-page, 30-point test administered in 10 minutes. 25 It has been used and validated with good sensitivity and specificity in the dialysis population. 33
Patient Health Questionnaire–9
Depression is known to complicate many comorbidities, including renal disease. It is considered the most common psychiatric illness in ESKD 34 although many of the uremic symptoms can overlap with symptoms of depression. 35 The PHQ-9 is a responsive and reliable measure to screen for depression and symptom severity through 9 questions.26,36 We opted to use the PHQ-9 for its simplicity and reliability in the general population.
Duke Activity Status Index
Functional capacity has been linked closely to quality of life and DASI is a reliable tool for its assessment. 27 It is a brief self-administered questionnaire that asks 12 questions about the patient’s independence in daily activities and is expressed in points and metabolic equivalents. It has been reliably used in chronic kidney disease (CKD). 37
Charlson comorbidity index
The CCI aims to quantify individual comorbid conditions burden of disease predicting 10-year survival for use in longitudinal studies. 28 It is a strong predictor of mortality in dialysis patients.38-40
WALT instrument
Patients’ preferences toward receiving life-sustaining treatment were assessed using the WALT instrument. It offers a quantitative assessment of patients’ willingness to accept treatment based on 4 domains: (a) treatment burden, (b) treatment outcome, (c) likelihood of the outcome, and (d) length of life following treatment. 29 This is done through 6 scenarios that encompass the 4 domains with variable likelihood of return to current status. This instrument was formed based on previous research of open-ended interviews and focus groups. 30 It was developed and validated among patients older than 60 years with a limited life expectancy secondary to congestive heart failure, chronic obstructive pulmonary disease, or cancer 30 and was later used in patients with CKD. 41
Mechanical ventilation and CPR
Patients’ preferences toward receiving mechanical ventilation and CPR were assessed based on 2 validated questions.42,43 The questions explain in simple terms the process of performing both in the patient’s current state of health.
Bias
Cross-sectional studies are known to be prone to selection bias depending on the study sample participation. Thus, for this study, we aimed to recruit all patients attending dialysis in the 2 dialysis units who met the inclusion and exclusion criteria. Another source of bias that we were conscious of was social desirability bias as participants might feel their wishes are not in line with what might be considered socially or medically appropriate or supported by high-quality evidence. We minimized this by having a health care professional not directly involved in participant’s care perform interviews and confidentiality was assured at all times.
Statistical Methods
Data were analyzed using Minitab Version 19 for Windows (Minitab LLC, State College, Pennsylvania, USA). Categorical variables are described as simple frequencies and percentages. Continuous variables are described as means (standard deviation) for normally distributed data and median (interquartile range [IQR]) for skewed data. Descriptive analysis, chi-square, and t test were performed along with probability plot for testing hypotheses to identify factors associated with patients’ preferences. A P value <.05 was considered significant.
Results
Description of the Sample
One-hundred-and-twelve candidates were approached, 23 declined to participate, 10 died before completing the structured interview, 7 were hospitalized at the time of their planned interview, and 2 withdrew from the study. Seventy participants were included in the analysis, reflecting a 62.5% response rate. Most of the participants were receiving in-center hemodialysis (77.1%). The mean age was 59 ± 15 years, and 62.5% were males. Most of the participants lived with their spouse, partner, or parents (77.2%), whereas the rest lived alone. The mean time on dialysis (vintage) was 41 (±36) months. Of the participants, the mean score for MoCA was 26 (±3), PHQ-9: 5 (IQR = 1.7-7), DASI, METs: 6.8 (±2.1), and CCI: 5 (±2.5). The majority of the patients (81.4%) believed in God. Detailed baseline characteristics are shown in Table 1.
Baseline Participants Characteristics.

Note. Data reported as mean (SD), No. (%), or IQR. MoCA = Montreal Cognitive Assessment; PHQ-9 = Patient Health Questionnaire–9; IQR = interquartile range; DASI = Duke Activity Status Index; METs = metabolic equivalents; CCI = Charlson comorbidity index.
WALT Instrument
The participants’ responses are described in detail in Tables 2 and 3. The first and third scenarios reflect a low and high burden of treatments, respectively, with the full range of possible outcomes, where no treatment means death. Responses to the first scenario were almost unanimous (98.5%) in their wishes to receive the low-burden treatment to return to their current status with the full range of possible outcomes, but this declined with decreasing probability of recovery. The result was very similar in the third scenario but less participants (94.2%) were inclined to receive high-burden treatment and that inclination continued to decline with the decreasing probability of recovery. The second and fourth scenarios reflect a low and high burden of treatment, respectively, with the possibility of extending life. Positive responses to the second scenario were high (80%) for treatment if it hypothetically resulted in a prolongation of life by 1 week. On the contrary, responses to the fourth scenario showed a lower tendency to accept the higher treatment burden (70%) if it only hypothetically extended life for 1 week but increased with prolonged life expectancy to 1 year (92.7%). The fifth scenario described a low-burden treatment, resulting in severe functional impairment, and less than half of the participants (45.7%) indicated that they would accept the intervention from the start but more appeared willing to accept treatment when the chances were more favorable. The last scenario described a low-burden treatment, resulting in severe cognitive impairment, with 28.5% of the participants accepting the intervention and most willing to accept treatment with improved likelihood of returning to baseline. There was a significant association between declining the high treatment burden associated with limited life expectancy in older participants with a t-value = 3.54 (3.75,17.59) and P value <.05 but no other associations were observed for dialysis vintage, MoCA, DASI, or CCI scores.
Percentage of Participants Who Prefer to Receive Treatment at Different Likelihoods of Death or Functional and/or Cognitive Impairment as an Outcome of Treatment (N = 70).

Percentage of Participants Who Prefer to Receive Treatment With Outcome of Different Degrees of Life-Extension (N = 70).

Note. Outcome without treatment was certain death. WALT = Willingness to Accept Life-Sustaining Treatment instrument.
CPR and Mechanical Ventilation Preferences
The responses to CPR and MV preferences were analyzed as a “Yes” or “No” response and the “uncertain” responses were excluded to simplify the analysis. Most of the participants chose “Yes” to receiving MV (77.4%) and CPR (82.8%; Figure 1). There was an association toward declining inclination for MV with older participants, with a t-value = 2.25 (confidence interval [CI] [1.17-19.88]), P value <.05, but not for CPR. There was no association noted with either DASI or CCI scores. The number of “uncertain” responses for receiving MV and CPR were 8 (11%) and 6 (8%), respectively.
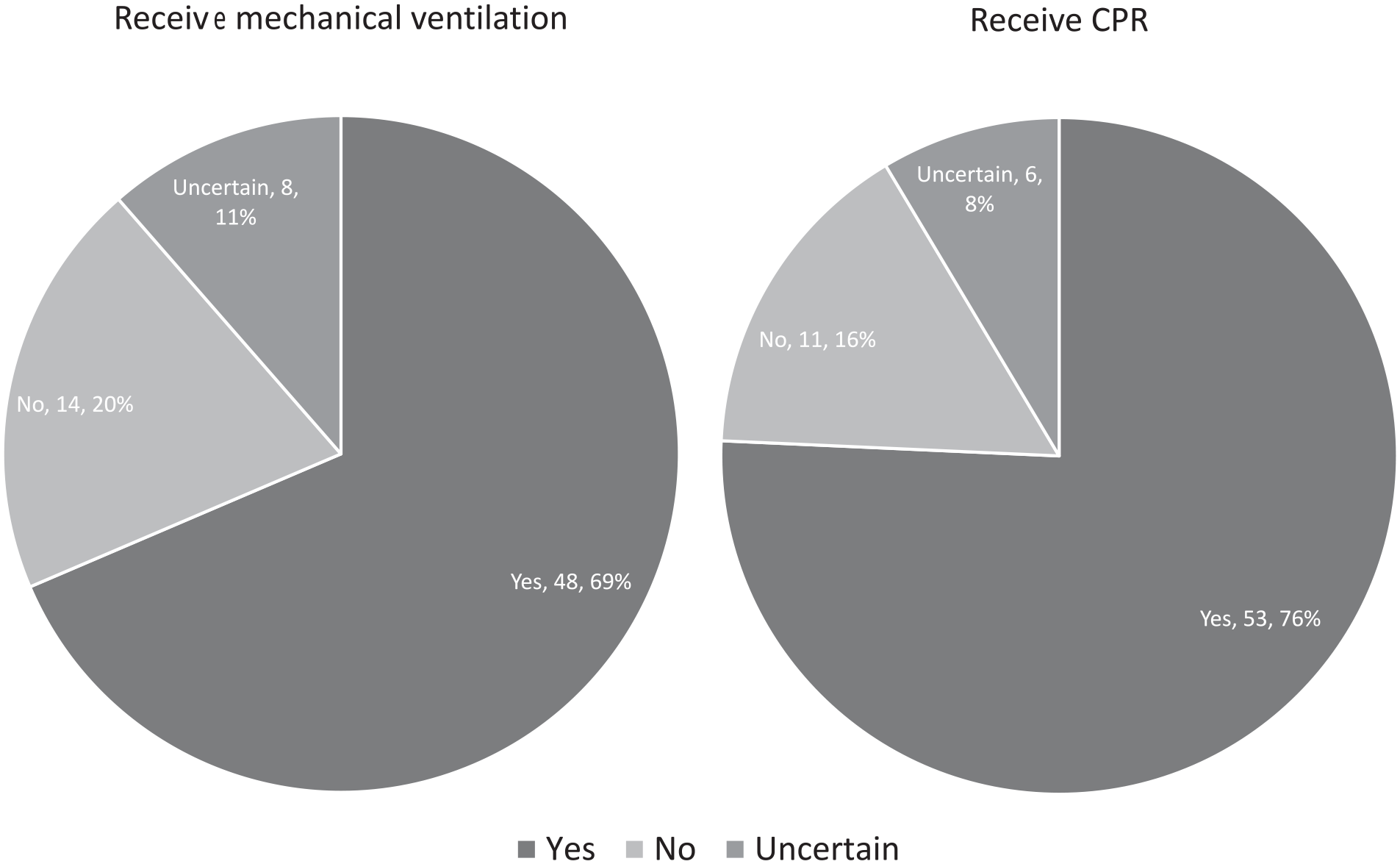
Preferences toward accepting mechanical ventilation and CPR.
ACP Preferences
Most of the participants had thought about assigning a surrogate decision-maker or know who that will be (44.1%) but never asked them nor signed any official documents. Less than a quarter (23.5%) had assigned a surrogate decision-maker but had not signed official documents to finalize this and a quarter (25%) had never thought about this (Figure 2). In terms of end-of-life care, most of the participants (51.4%) stated that they had never considered or talked about the types of treatments they may or may not want (Figure 2), although most expressed that it was their wish to die in their own home (n = 55, 82%) as opposed to a hospital (n = 11, 16%) or a friend/relative’s home (n = 1, 1.5%), with 3 participants who preferred not to answer. The majority said that they had never discussed ACP with their primary nephrologist (94.2%), and more than half of the participants (59.4%) expressed their wish to discuss this with their primary nephrologist, and the presence of a family member or a friend was not favored (67.6%; Figure 3). As for the in-center hemodialysis participants, the preferred location to carry out these discussions was the dialysis unit (n = 33, 67.3%) as opposed to a separate clinic visit (n = 16, 32.7%).

(Left) designating a surrogate decision-maker and (Right) decisions of end-of-life care and related treatments.
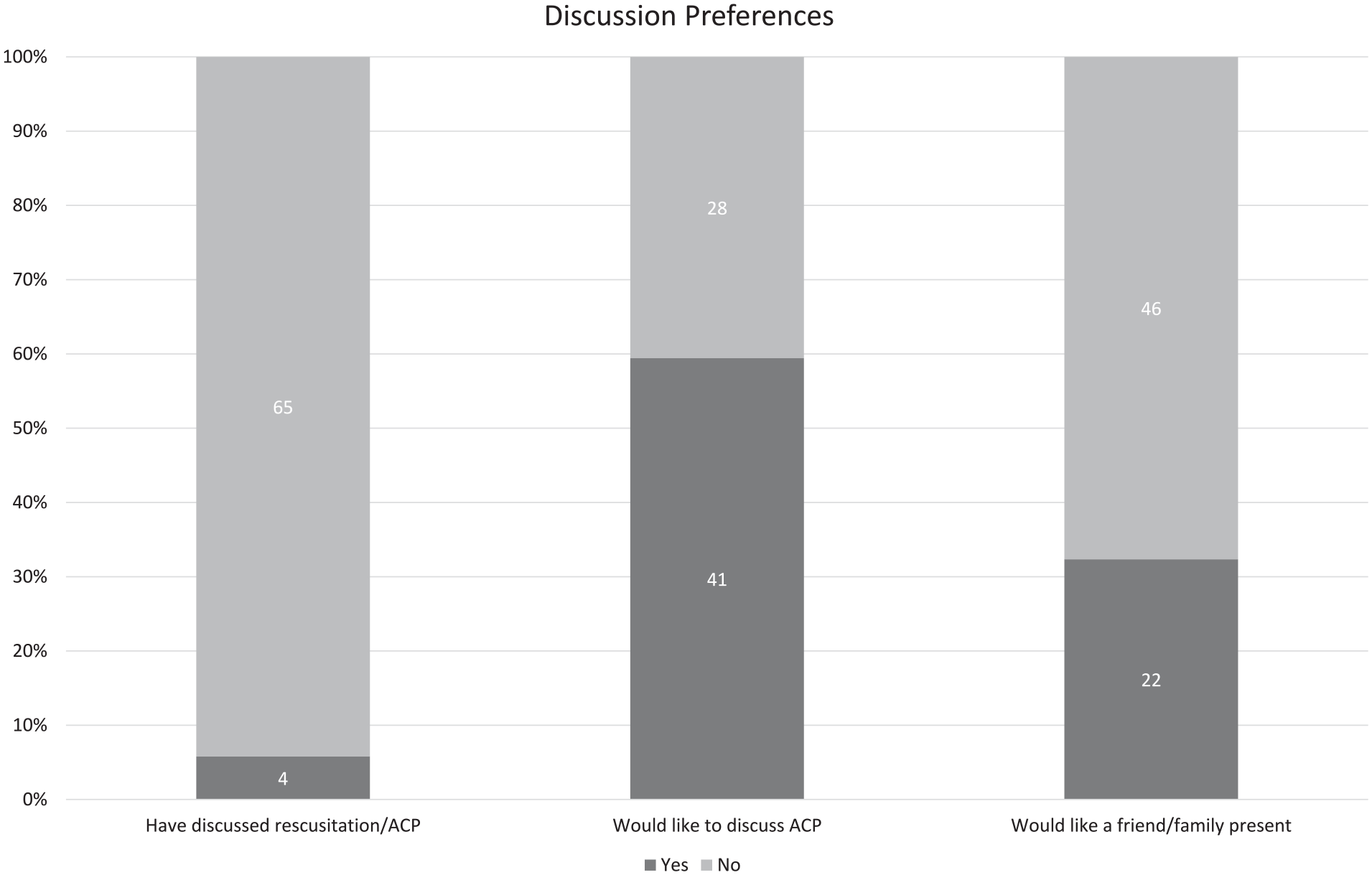
Prior ACP discussions with primary physician and discussion preferences on ACP and the presence of a family member or friend.
Discussion
Key Findings and Discussion of the Results
This study design was to explore dialysis patients’ preferences toward ACP and end-of-life care, using validated instruments. The ESKD is an extremely relevant disease entity in which to study these questions because of its very high mortality rate, notably higher than several solid organ malignancies. 44 Indeed, it was notable that 10 participants, constituting 8.9% of the original sample actually died over the course of this 6 months study. The sample CCI average score reflected a 21% estimated 10-year survival; there was no adjustment of the score for the presence of kidney disease. The MoCA results revealed the presence of mild cognitive impairment in approximately half of the participants. With regard to the screening for depression (PHQ-9), this was difficult to determine as the score pointed toward the presence of mild depressive symptoms, and these may have significant overlap with uremic and volume overload symptoms, such as tiredness, fatigue, and loss of energy. Moreover, the PHQ-9 results did not shows obvious differences between patient preferences.
Seventy participants were included in this analysis, representing a 62.5% response rate. Participants’ attitudes toward receiving life-sustaining treatment were related to treatment burden and perceived likelihood of adverse outcome. There was a clear propensity toward accepting low-burden treatment regardless of the likelihood of death, but this changed with high-burden treatment where participants were less agreeable to receiving treatment with lower possibility of recovery (Table 2). This was similar when limited life extension was in question with high-burden treatment (Table 3).
When faced with severe functional or cognitive impairment, participants were even less agreeable to receive treatments when compared with death. This response could reflect that patients are not well informed about the long-term effects of dialysis on functional and cognitive outcomes as cognitive impairment is already prevalent in almost half of the participants, likely related to receiving a life-sustaining treatment, namely, dialysis. It could also mean that patients are more likely to accept the inevitable slow development of these feared long-term outcomes, as opposed to the stark version the WALT instrument proposes (see supplemental material).
These results are very similar to the initial article that described the WALT instrument as a patient-centered tool of assessing treatment preferences.29,30 These hypothetical scenarios may well be influenced by transient changes in health or social status and these pose significant challenges in ACP. Our study demonstrates how complex ACP is and highlights the level of difficulty inherent in decision-making at end of life in this very challenging population.
Less than 20% of the participants expressed a preference to not receive CPR or MV and older participants seemed numerically more likely to decline MV, although the significance of this result is questionable due to small numbers and therefore diminished power. Wachterman et al 45 have reported different results of only 44% (n = 18) of patients focusing on life extension when estimating their chance of survival beyond 1 year to be more than 90%. In addition, Scherer et al 46 reported similar results in a larger cross-sectional study evaluating the association of self-reported importance of religious or spiritual beliefs and end-of-life care preferences among people receiving dialysis. The percentage of patients declining CPR and MV was no less than 30.2% and 57.4%, respectively, with participants more likely to receive the intervention the stronger their religious or spiritual beliefs. These two studies were done in the United States and could reflect the cultural differences unique to our population. The participants in this trial are from the west of Ireland and they could be considered from rural populations with strong family ties and historic religious traditions that might deter engagement in ACP discussions. They have reported a stronger belief in God (81.4%), which is likely to have some effect on their preferences as demonstrated by Scherer et al. 46
More than half of the participants reported not having considered ACP and only 7% reported having completed the process of choosing a surrogate decision-maker. More than half of the participants wished to discuss ACP with their primary nephrologist irrespective of their choices regarding CPR and MV, with most of the hemodialysis patients choosing the dialysis unit as a preferred venue for this. Albeit, the reported number of participants wanting to discuss ACP in this study is less than what has been reported in the literature. Many of the participants could have perceived that these discussions could translate into efforts to make a decision not to resuscitate or intubate, whereas deferring the discussions would be accepting these interventions when the need arises. This further highlights the importance of ACP as a process and not as a decision. 47
Involving patients and their surrogate decision-makers is not only about deciding what type of treatment they may or may not want because medical emergencies cannot be predicted in detail and this needs to be acknowledged beforehand. Poorly written and badly designed advance care directives can clearly sometimes fail to meet their purpose 48-50 but it is rather the emotional journey that patients and their family take toward end of life11,51 that is important. It is about offering our vulnerable patients guidance and helping them live their days in full while we assume the role of caregiver. The literature has described how both families and physicians fail to predict patients’ preferences with limited practiced autonomy,19,20,22,52 reflecting an increasing need for good communication and meaningful clinical encounters. 24 Furthermore, there is growing evidence that patients tend to change their wishes and this makes ACP a relevant issue that needs frequent discussion.41,53
Limitations of the Study
There are a number of limitations to this study. The race status was not captured here but the lack of racial diversity in these centers limits its generalizability outside of the Irish and European societies. Non-English speakers were excluded from the study although their numbers are small in the context of the sample size. As mentioned previously, although WALT is a validated instrument, these are hypothetical scenarios that might not reflect the choices these patients might opt for when it becomes reality. This study was also conducted during the height of the coronavirus pandemic and before the supply of the vaccine. It had a good response rate but we could not out rule bias in the participants’ responses. However, the psychometric properties of WALT make it a good tool for an overall assessment of patients’ preferences for end-of-life care. 29 Acknowledging a cross-sectional study design describes a point of time and the pattern, and stability of patients’ preferences could not be assessed here. The evidence of mild cognitive impairment in this sample is in line with previous literature describing patients with kidney failure 54 and could lead to questions around the ability of these patients to answer questions regarding these scenarios, while acknowledging that mild cognitive impairment should not prevent patients who have the capacity from expressing their wishes.
Clinical Implications of Results
Even with the limitations of this study, there is a clear need to incorporate high-level ACP in managing patients with ESKD. This cohort of patients has a poor prognosis and ACP is an integral part of improving their quality of care. Involving surrogate decision-makers in the conversation is vital and provides much needed emotional support to patients. Identifying the patient’s values is a fundamental aspect of ACP, which helps in guiding patients during frequent ACP discussions. Adopting a systematic approach to navigate ACP in patients with CKD has been proposed by Davison 24 through the following steps: (a) identifying patients who would most likely benefit from ACP, (b) determining patient and family readiness for participation in ACP, (c) introducing ACP, (d) facilitating ACP, (e) documenting and developing a follow-up plan, and (f) continuing quality improvement. As patients have expressed their wishes to have meaningful conversations with their primary nephrologist to start ACP, health care providers should feel more comfortable initiating these dialogues.
Recommendations for Future Research
Further research is needed to explore the agreement between patients’ choices and real-life outcomes. Identifying the central constant values and temporarily changing circumstances in patients’ life will help make more informed decisions and a better understanding from health care providers. It should be done within the wider community, with a properly representative population to draw valid conclusions. It is also essential to assess the impact of ACP on surrogate decision-makers as a primary outcome in these studies. Integrating ACP in nephrology medical training should happen at an earlier stage to prepare physicians to guide their patients at the end of life.
Conclusion
Advance care planning should be part of the standard of care when managing ESKD. Improving communication and empowering patients to establish goals of care that prevent invasive and unnecessary procedures that lead to more suffering rather than improved care should be sought. Understanding patients’ values toward the burden of treatment, nature of the outcome, the likelihood of the outcome, and life expectancy all play a role in making informed decisions toward end of life.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581221113383 – Supplemental material for Dialysis Patients’ Preferences on Resuscitation: A Cross-Sectional Study Design
Supplemental material, sj-docx-1-cjk-10.1177_20543581221113383 for Dialysis Patients’ Preferences on Resuscitation: A Cross-Sectional Study Design by Husam Alzayer, Annette M. Geraghty, Kuruvilla K. Sebastian, Hardarsh Panesar and Donal N. Reddan in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors are grateful to the patients who generously gave theirtime and participated in the study. The authors also thank the dialysis nursing staff who supported and facilitated this study.
Ethics Approval and Consent to Participate
The study approved by the local ethics committee at Galway University Hospital and Mayo University Hospital. All participants provided written informed consent prior to participating in this study.
Consent for Publication
All authors provided consent for publication.
Availability of Data and Materials
The data underlying this article will be shared on reasonable request to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.