
Abstract
Serious illnesses impact a large and growing number of older adults globally and in Singapore. Serious illness conversations (SICs) are a useful tool for clinicians to understand patients’ priorities and increase alignment between priorities and care. This study aimed to understand barriers and facilitators to SICs among older adults, noting that this population is understudied yet more impacted by serious illness. In-depth interviews were conducted with older adults living with serious illnesses (n = 11) and family caregivers (n = 6). Facilitators and barriers were identified at the individual, interpersonal, institutional, and socio-cultural levels of the socio-ecological framework. Facilitators included acceptance and awareness of their condition, patient readiness and willingness, hope and support on the journey, early and careful initiation, direct communication, accessible patient-centered and high-quality care, and religious support. Barriers included limited awareness and acceptance of their condition, poor emotional well-being, uncertainty about the future, lack of provider communication, information imbalances, low support on the journey, unclear and confusing language, inaccessible and low-quality care, religious beliefs, and cultural stigmas around prognosis and decision-making. Understanding these facilitators and barriers can inform changes in policy and clinical practice to improve SICs with older adults.
Keywords
Introduction
Serious Illness
The number of older adults living with serious illnesses is rising globally and in Singapore. The number of people over 65 is anticipated to double globally by 2054, and a quarter of the population of Singapore is estimated to be over 65 by 2030 (Lor, 2022; Thompson et al., 2014; van Teutem, 2024). Serious illnesses are health conditions that have a high risk of mortality and are associated with low quality of life, difficulty with activities of daily living, and a high caregiver burden (Aldridge & Bradley, 2017; Gozalo et al., 2011; Hanson et al., 1997; Hong et al., 2011; Kelley & Bollens-Lund, 2018; Tay et al., 1994; Teno et al., 2004). Serious illnesses also correspond with high healthcare utilization, particularly towards the end-of-life (Diernberger et al., 2024; Kaur et al., 2022). This care often occurs in high-acuity settings and differs from the goals of patients and caregivers, who often prioritize remaining at home and pain management (Ouchi et al., 2019; Steinhauser et al., 2000). Discordance in goals of care can result in unnecessary suffering at the end-of-life (Dev, 2015; Mack et al., 2012).
ACP and SIC
Advance care planning (ACP) and Serious illness conversations (SICs) are part of a continuum of serious illness communication that aims to improve goal-concordant end-of-life care (O’Shea & Wilkinson, 2025). Traditionally, ACP is a structured decision-making process that establishes a patient’s wishes for future care in the event of a medical emergency (Hamilton, 2017). Recent models have expanded ACP, describing it as a continuous, “building block” approach throughout an individual’s serious illness trajectory (Rosa et al., 2023). SICs are an integral yet relationally complex part of the ACP process that occurs once a person is diagnosed with a serious illness. SICs are iterative conversations that increase patients’ prognostic understanding of their illness and help clinicians to align patients’ priorities, concerns, and treatment goals with care (Baxter et al., 2024; Rosa et al., 2023). Evidence suggests that SICs are associated with positive outcomes, including lower healthcare utilization, increased goal-concordant care, and improved shared decision-making (R. E. Bernacki & Block, 2014; Geerse et al., 2019; Guo et al., 2025; Sanders et al., 2020). SICs have also been shown to increase quality of life, decrease hospital deaths, lead to less aggressive end-of-life care, and improve caregiver bereavement adjustment (Detering et al., 2010; Khandelwal et al., 2015, 2016; Lakin et al., 2016; Wright et al., 2008). Notably, evidence on ACP and SICs remains mixed (Morrison et al., 2021). One systematic review found limited associations between ACP and communication, goal-concordant care, and cost savings (Jimenez et al., 2018). Additional reviews and meta-analyses also demonstrated variable results, particularly on improvements in goal-concordant care, quality of life, decisional conflict, and patient and caregiver satisfaction (Crooks et al., 2025; McMahan et al., 2021; Zhang et al., 2025).
Challenges With ACP and SIC Implementation
Mixed evidence on ACP and SICs may be partly attributed to the heterogeneity of interventions and the presence of substantial implementation barriers. In Singapore, infrastructure to support ACP and SICs remains limited, and ACP processes have traditionally been avoided by Singaporeans, largely due to stigma around mortality (Arivalagan & Gee, 2019; Yeo et al., 2023). One study found that approximately half of Singaporeans were aware of palliative care and would be willing to use it (Yeo et al., 2023). Despite the introduction of a national ACP planning program in 2011 under the Respecting Choices model, many challenges remain in implementing ACP processes as a standard of care (Ng et al., 2023). In particular, SICs have not been the focus of many research studies in the Asian and local setting among older populations. Studies in other settings have identified additional barriers to SICs, including insufficient provider training, lack of appropriate patient identification, and late initiation (R. Bernacki et al., 2015; Brighton & Bristowe, 2016; Geerse et al., 2019; Mack et al., 2012). However, barriers specific to older patient populations remain understudied (Im et al., 2019).
Several facilitators of SICs have been described in the literature, including patient readiness for SIC, structured conversation guides, institutional support, provider communication style, and family support. Nevertheless, it remains unclear if these can be extrapolated to the older adult population (R. Bernacki et al., 2015; Hanley et al., 2025; Paladino et al., 2019). Understanding the facilitators and barriers to SIC experienced by older adults is critical, as this population has a higher proportion of healthcare utilization at the end-of-life (Xu et al., 2022), and decision-making in the local context for older adults is often familial rather than autonomous (Krishna, 2011). Given the dearth of evidence on SICs among older adults, this study aimed to understand the facilitators and barriers to SICs in our multicultural Asian setting.
Methods
Setting and Participants
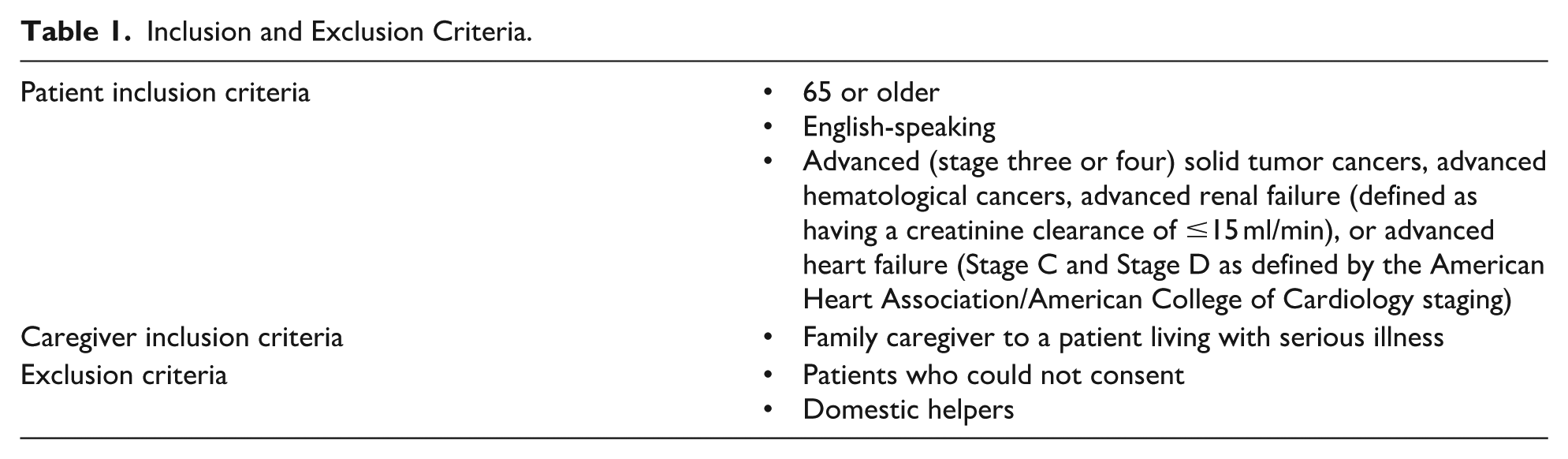
This qualitative exploratory study was conducted across three outpatient settings in a large tertiary hospital in Singapore. IRB approval was received (#2022-2736). Sampling was purposive to increase diversity in the sample population, considering disease type, age, gender, and marital status. Oncologists, renal physicians, and cardiologists referred potentially eligible patients and caregivers in outpatient clinics. Research coordinators screened participants, and those who met the inclusion criteria were invited to join the study (Table 1). Recruitment stopped once thematic saturation was met. Older adults (n = 11) and family caregivers (n = 6) were included. Of 28 eligible participants, 17 chose not to participate, with time being the most common reason for refusal.
Inclusion and Exclusion Criteria.
Data Collection
Data collection for this study commenced in February 2023 and was completed in September 2024. Due to the qualitative exploratory design, the study protocol was not registered. Written informed consent and demographic information were obtained from participants before conducting semi-structured interviews. Interviews took place either via video conferencing or in a quiet clinic room. The duration of the interviews ranged from 45 min to an hour, and the interviewer had extensive experience in SICs and qualitative interviewing techniques. Interviews followed a guide with predetermined questions, and additional questions were asked as needed. Interviews were tape-recorded and subsequently transcribed and de-identified.
Data Analysis
An adapted version of Colaizzi’s method of phenomenological analysis was used to understand the lived experiences of older adults and family caregivers (Beck, 2021; Morrow et al., 2015). Firstly, transcripts from all participants were thoroughly read and re-read for data familiarization by EH and JT. EH and JT coded the transcripts using an inductive line-by-line approach with NVivo (Lumivero, (n.d.), version 15). The authors met to discuss areas of misalignment and disagreement. Themes were deductively mapped using the Socio-Ecological Framework (SEF) following inductive coding (Kilanowski, 2017). The SEF is commonly used by public health professionals to examine dynamics between individuals and wider cultural and systemic drivers of health (Kilanowski, 2017). In the context of this study, there were reciprocal relationships between the lived experiences of older adults and caregivers with interpersonal, institutional, and societal factors. Combining Colaizzi’s method with the SEF highlighted the interplay between individual experiences and structural determinants. In place of participant verification, patient data were triangulated with caregiver data, as we did not re-interview participants for ethical reasons.
Results
Participant Characteristics
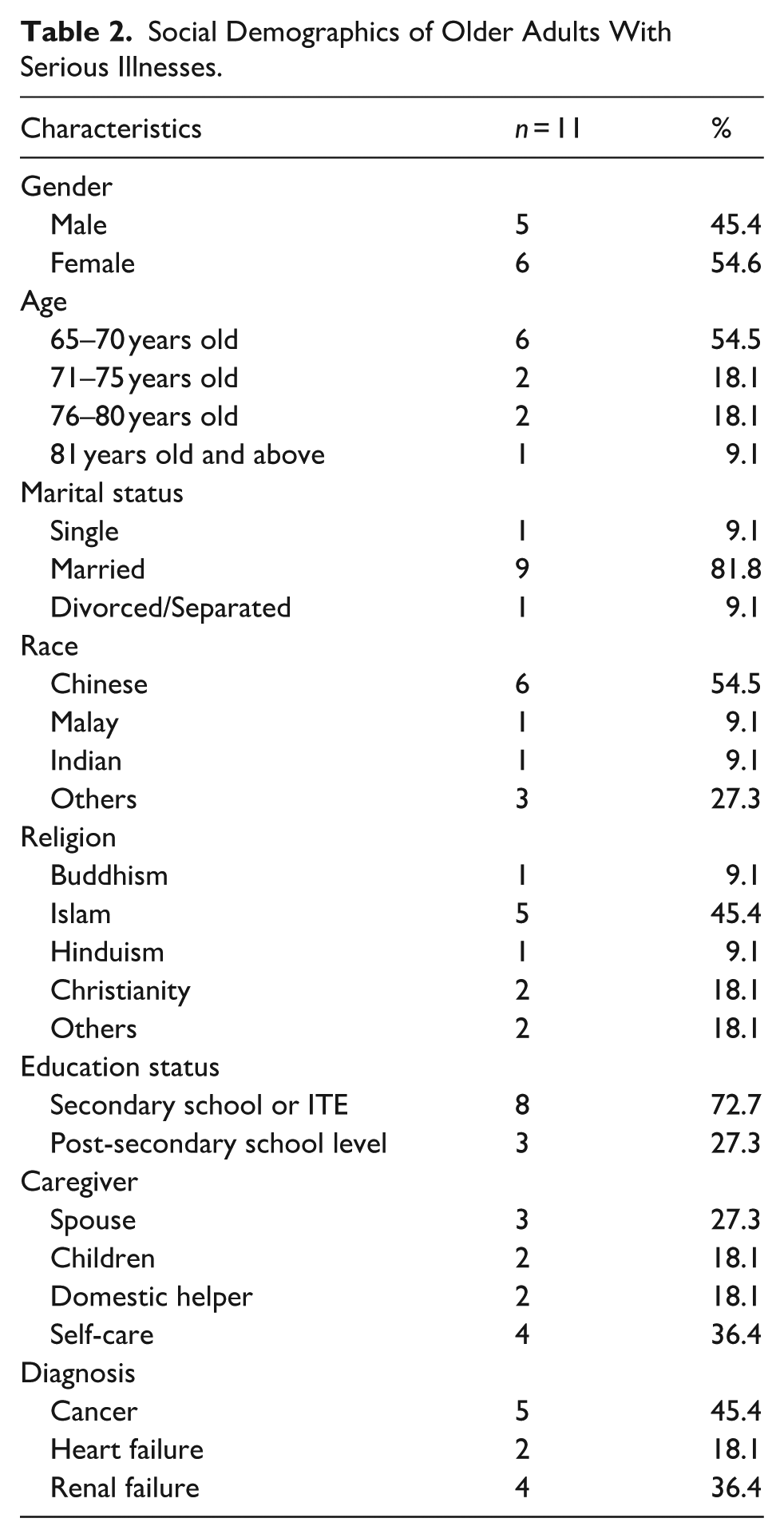
The demographic characteristics of the participants (N = 17) are shown in Tables 2 and 3.
Social Demographics of Older Adults With Serious Illnesses.
Social Demographics of Family Caregivers of Older Adults With Serious Illnesses.

Thematic Framework
Themes were mapped onto four levels of the SEF: individual, interpersonal, institutional, and cultural and societal. There were facilitators and barriers of SICs at each SEF level (Figure 1).

SEF of facilitators and barriers to SICs.
Individual Level
Most of the identified facilitators and barriers were related to the patient. Facilitators included acceptance, patient-driven SICs, and awareness of the illness through information-seeking (Table 4). Lack of acceptance, poor emotional well-being, and uncertainty about the future were reported as barriers (Table 4).
Individual Level Facilitators and Barriers to SICs.

Facilitators
Patients and caregivers mentioned the importance of acceptance of the condition and prognosis. Many noted that it would be easier to engage in SICs and identify goals of care if the person already accepted their condition. Patient-driven SICs were also referenced as a facilitator and was described as patient readiness and willingness, including patient initiation and preparation for discussions. This facilitator was closely related to providers taking a careful approach to SIC initiation, as some patients reported being more willing and ready to engage. Patient awareness of their illness through information-seeking was also discussed. Patients noted that online searches and other information-seeking avenues allowed them to ask more questions and prepare for SICs.
Barriers
Participants emphasized that accepting the reality of having a serious illness is very difficult. Patients and caregivers struggled to engage in SICs because they had not come to terms with their own or their loved one’s illness. Lack of acceptance was described as contributing to poor emotional well-being, another barrier to SICs. Depression and shame related to illness were reported by many patients and caregivers. Similarly, some caregivers described not wanting to have SICs to avoid demoralizing the patient. Participants also mentioned that discussing the future was very difficult due to uncertainty around their illness and prognosis. These participants noted that it could be distressing to think about goals of care or hopes for the end-of-life, especially if they viewed themselves as having limited time.
Interpersonal Level
Factors at the interpersonal level occurred in dyads: patient-caregiver, patient-provider, and caregiver-provider. Facilitators of SICs at this level included education, giving hope, early initiation of SIC, careful clinician approaches, someone to journey with, and direct communication (Table 5). Barriers were limited provider communication, unclear language, information imbalances, negative family attitudes towards SICs, and no one to journey with (Table 5).
Interpersonal Level Facilitators and Barriers to SICs.

Facilitators
Education was mentioned by patients and caregivers as a facilitator of SICs. This education often occurred between the provider and the patient and/or caregiver, although caregivers and patients also educated one another. Caregivers preferred for clinicians to serve as educators to ensure accuracy, increase clarity, and facilitate the conversation. Patients noted that clinicians providing information about their illness during consults allowed them to better understand and engage in SICs.
Most patients and caregivers also mentioned giving hope as being crucial. Caregivers and providers were often in the position of giving hope to patients. Hope was noted as taking many forms, including encouragement and positivity. Hope between providers, patients, and caregivers built a stronger foundation for SICs; patients stated that positivity from providers fostered trust. Strong patient-provider relationships were also frequently mentioned as facilitating open dialogue, particularly when discussing sensitive topics.
Clinicians’ approach to SICs was also a facilitator. For instance, early initiation of SICs was described as positive because patients and caregivers had more time to process information. Participants emphasized that early initiation with a careful approach also allowed providers to understand patients’ goals of care. Many participants described this approach as gradual, gentle, and person-centered, including being tactful and seeking permission. Effective providers were also described as being encouraging and positive throughout the encounter, especially while sharing serious information. Direct communication was another facilitator related to how clinicians conduct SICs. Both patients and caregivers stated that concise, specific, and simple language was helpful to their understanding of the illness and care planning. Language was described as more effective when it was individualized, culturally appropriate, and streamlined.
Having someone to journey with was cited as an important facilitator of SICs by all participants. This support was noted to come from a variety of sources, including family, peers, community members, and health professionals. While family support was the most referenced, the importance of having someone to accompany the patient during their illness was not restricted to one role.
Barriers
Limited provider communication was frequently cited as a barrier to SICs by patients and caregivers. Participants mentioned that providers occasionally made assumptions about patients’ goals or understanding of their condition. This led to SICs that patients were not adequately prepared for, causing shock and/or confusion. Some patients and caregivers reported that providers were not receptive to their questions about the seriousness of their illness, despite patient initiation of SICs and willingness to discuss these topics. Some participants mentioned that they felt uncomfortable broaching these topics because of their providers’ discomfort with discussing them. Limited provider communication was connected to information imbalance, which was reported by patients and caregivers as existing between them and providers. For some participants, this imbalance was due to a lack of information, while others experienced overwhelming information, which made it more difficult to engage in SICs.
Two other barriers at this level were related to social support. While experiences of family support were largely positive, other families were avoidant of SICs. Patients reported that they did not wish to over-burden their children with information. Similarly, caregivers noted that they did not want to demoralize their loved one with negative information. Some participants also mentioned that they had complicated family dynamics or living situations, which made attaining positive family support difficult. Likewise, not having someone to journey with was mentioned by patients, who were worried about not being able to manage as they became increasingly sick. This isolation was referenced as a barrier to SICs due to the lack of support and strength that is found in connection.
Finally, there was a challenge with unclear language, as clinician communication with patients and caregivers was described as overly complex and confusing, particularly for an older adult population. This barrier was emphasized by participants with less English proficiency, who reported needing simpler and clearer provider communication.
Institutional Level
The institutional level addresses factors within the larger health system. Facilitators included: institutional values of patient-centered care, accessible providers, comfortable environment, and effective care coordination and continuity (Table 6). Barriers were also identified: lack of patient-centered care, inaccessible providers, and limited care coordination and continuity (Table 6).
Institutional Level Facilitators and Barriers to SICs.

Facilitators
Institutional prioritization of patient-centered care was reported by caregivers and patients as a facilitator to SICs. This was described as healthcare settings where clinicians were encouraged to listen to patients and be mindful of communication preferences and goals of care. Person-centered care contributed to reported improvements in provider-patient relationships and trust in the SIC process.
Like patient-centered care, accessible providers facilitated SICs by strengthening provider-patient relationships. Accessible providers were described as having sufficient time and routes of communication, including outside of regular office hours and during emergencies. These providers were also described as having sufficient non-English language skills.
A comfortable health care setting was also mentioned. Some patients and caregivers reported preferring in-person visits, while others noted feeling more comfortable virtually. Effective care coordination and continuity were also reported as being important to SICs. Patients and caregivers reported that information sharing between providers on their current health status, treatment plan, and medical history was helpful. Additionally, participants noted that continuity of care from providers allowed them to build rapport and trust with their care team.
Barriers
A lack of patient-centered care was reported by both patients and caregivers as a barrier to SICs. Patients and caregivers reported feeling dismissed and rushed, hindering the patient-provider relationship and SICs. While participants mentioned provider accessibility, they also mentioned provider inaccessibility. Specifically, patients and caregivers reported that a lack of provider time limited their ability to ask questions and understand their condition. Many also expressed skepticism that providers would have sufficient time to conduct SICs and noted that language barriers decreased access.
Limited care coordination and continuity were also referenced as barriers by patients and caregivers. Participants mentioned frustration with poor information sharing between providers, leading to confusion about their treatment plan. It was noted that examinations sometimes had to be repeated, and a large burden was placed on patients and caregivers to manage their health information.
Socio-Cultural Level
Socio-cultural factors are facilitators and barriers that are tied to larger belief systems and societal structures. Religious beliefs were identified as a facilitator and barrier at this level. Other barriers included: cultural stigma around prognosis, cultural beliefs around decision-making, and a pragmatic focus on solutioning (Table 7).
Socio-Cultural Level Facilitators and Barriers to SICs.

Facilitators
Religious support was mentioned as an important part of SICs by both caregivers and patients. Many respondents described their religion as a source of strength during their illness and SICs. They reported that their religion helped them to accept and cope with their condition. One patient noted that without their religion, they may have had increased difficulty with SICs.
Barriers
While religious beliefs facilitated SICs for some patients and caregivers, other respondents reported that SICs contradicted their religious beliefs and were potentially harmful to their spiritual well-being.
Cultural stigma around prognosis and time limits was reported as a barrier to SICs. Patients and caregivers mentioned that prognostic estimates were unhelpful and could cause unnecessary distress. Respondents shared that it was not the provider’s role to estimate time limits, as there was too much uncertainty. This was emphasized as being a societal and cultural perspective rather than an individual one.
Cultural stigma around decision-making was also mentioned. Some patients and caregivers noted that they preferred to avoid SICs, or that others may prefer to avoid them. It was also reported that who is involved in the decision-making process is important yet variable, with some patients preferring to be alone. Similarly, some caregivers preferred to discuss with the patient, while others stated that they did not want to involve the patient or did not want to be involved themselves. Caregivers also mentioned a preference for delaying SICs to avoid frightening the patient.
Cultural beliefs around prognosis and decision-making were reported to influence cultural pragmatism when it comes to SICs. Cultural pragmatism was described as a strict focus on adhering to the treatment plan and taking practical steps to address illness. Respondents reported that they preferred to only follow medical plans and not engage in SICs.
Discussion
Key Findings
This study aimed to identify facilitators and barriers to SICs experienced by older adults and caregivers in a multi-cultural Asian setting. Using the SEF, we identified four layers of facilitators and barriers that had reciprocal relationships with one another. These factors operated at the individual, interpersonal (patient-caregiver, patient-clinician, and clinician-caregiver), institutional, and societal levels.
At the individual level, factors that facilitated SICs included patient readiness, which was driven by acceptance and awareness of the illness, often through information seeking. Readiness and acceptance have been found to be facilitators and barriers in other studies, including within the Asian context (Cheung et al., 2020; Hanley et al., 2025). However, the role of self-information seeking to increase illness awareness and readiness for SIC has not been explored previously. In addition to a lack of acceptance, poor emotional well-being and uncertainty about the future hindered SICs. Previous research, including a study involving seriously ill Chinese patients, has highlighted that SICs can evoke emotional discomfort for patients and clinicians (Cheung et al., 2020; Paladino et al., 2023). While emotional well-being has been discussed, individual uncertainties about the future had not been discussed before this study.
The interpersonal level focused on two types of relationships: provider relationships with patients and caregivers and relationships between patients and their support system, which was often family caregivers. One systematic review of facilitators and barriers to ACP discussions emphasized the importance of family in end-of-life discussions and a careful approach to SICs (Suen et al., 2024). In our study, clinicians and families supported SICs by fostering patient hope, which has been shown to be a valuable strategy (Velić et al., 2023). Leveling the information balance, communicating directly, and providing education around illness and SICs were, however, unique factors found within our study. Under the Singapore Medical Council’s Ethical Code and Guidelines, patients are entitled to information on their condition; however, information imbalances persist, likely due to cultural norms and preferences (Singapore Medical Council, 2025). Specific informational material around SICs could pave the way for clinicians to initiate SICs, as well as facilitate patient and caregiver understanding of the illness trajectory. Moreover, in both the SIC guide and the teaching of clinicians, empathetic and clear communication styles should be emphasized to foster hope and facilitate SICs.
At the institutional level, patient-centered care, accessible providers, comfortable environments, and care coordination were reported as impacting SIC experiences. Many of these facilitators are also facilitators of good quality of care, demonstrating that building an institutional setting where care quality is valued can positively impact SICs. While other studies have noted that systems-level failures in care coordination can hinder SICs, our study was rather unique in reporting that giving good quality care encourages patients and caregivers to engage in SICs (Lakin et al., 2016). Thus, it is important to ensure that healthcare settings promote patient-centered and accessible care alongside effective care coordination and communication. Information truncation and lack of care coordination with patients can lead to confusion, as patients might not understand why the clinician is choosing that time to engage in SIC. Other impacts of poor care coordination include worsened patient-provider relationships and trust in their care, which can lead to inappropriate healthcare utilization. From the provider perspective, Paladino found that poor care coordination can lead to later initiation of SICs due to a lack of established team roles (Paladino et al., 2023). Without a proper institutional environment for SICs, it is challenging for patients and caregivers to engage in a timely and appropriate manner and to see SICs as valuable in the continuum of decision-making.
Finally, societal norms around end-of-life decision-making, stigma around prognosis, a pragmatic focus on solutioning, and religion were important factors reported by patients and caregivers. Unique to the local setting, we have a melting pot of different spiritual and religious considerations (Miner, 2023). Each religion has distinct considerations around serious illness and the end-of-life. There is also a cultural preference for pragmatic solutioning rather than an overemphasis on prognosis and end-of-life decision-making, which can be stigmatized (Lall et al., 2021). Previous research has found that there is a death taboo in many Asian contexts, which resonated with our study results, particularly the observed stigma around prognosis and time limits (Ali et al., 2021; Suen et al., 2024; Yeo et al., 2023). Thus, locally and in related settings, it is important that clinicians are aware and consider the impact of religion and cultural norms on SIC implementation.
Strengths and Limitations
This study is the first to examine facilitators and barriers to SICs reported by older patients and caregivers in the Singaporean and Asian context, filling an important gap. Furthermore, patients were recruited with cancer, heart failure, and renal failure, making our findings more easily generalizable to the wider serious illness population. Nonetheless, there were limitations. Only patients and caregivers who spoke English were included, excluding those who primarily speak other languages such as Mandarin, Malay, Tamil, and various dialects, though locally, English remains the most commonly spoken language (Department of Statistics, Ministry of Trade & Industry, Republic of Singapore, 2021). Additionally, only patients and caregivers were included. Future studies should include the perspectives of healthcare staff to understand facilitators and barriers from their point of view, especially with regard to how institutional factors can be overcome. In this study, patients and caregivers still provided insights on healthcare providers and institutional factors that can guide future exploration. Additionally, qualitative themes were not verified by participants, potentially introducing coding bias. Data was triangulated between patient and caregiver interviews to reduce this likelihood.
There is also a potential for self-selection bias, as those who participated may have been less culturally stigmatized against SICs (Florczak, 2022). Additionally, while participants were recruited in patient-caregiver dyads, more patients participated than caregivers due to time and logistical challenges. Although self-selection bias is a challenge in most qualitative research studies, we have tried to address this through purposive sampling across different religious groups and disease conditions to maximize participant diversity (Florczak, 2022). It is important to consider these findings in context to avoid over-generalizations about SICs in older adult populations. Future work should address how these facilitators and barriers interrelate to the language in SIC guides, as well as inform clinician training and structural reform (Ariadne Labs, 2023).
Footnotes
Acknowledgements
The authors thank participants for their important contribution.
Ethical Considerations
This study was approved by the Institutional Review Board (2022–2736).
Consent to Participate
Informed consent for participation in the study and publication was obtained.
Author Contributions
Dr. Shirlyn Hui-Shan Neo is the principal investigator. Eleanor Hummel and Jasmine Yun-Ting Tan conducted the analysis reported in this article with guidance from Dr. Shirlyn Hui-Shan Neo. Eleanor Hummel wrote the first draft and all authors contributed to the revisions and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Lien Centre for Palliative Care Education Incubator Award. Project title: Cultural adaptation of the serious illness conversation guide for seriously ill patients in Singapore. Principal Investigator: Dr Shirlyn Hui-Shan Neo. Project id number: LCPC-EX22-0001. Funding amount: 31,000.00.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data is shared in the attached tables.