
Abstract
Introduction
Serious Illness Conversations (SICs) involve building prognostic awareness and exploring patients’ goals in the context of advancing serious illness. 1 SICs were initially developed for use in the outpatient setting2,3 and are ideally conducted 1-2 years prior to death. 1 Despite the known benefits of SICs and advance care planning (ACP) with seriously ill individuals, including satisfaction with communication, improved psychological outcomes, and earlier hospice referrals,1,4,5 more than a quarter of Medicare beneficiaries have not engaged in these conversations, with rates not increasing with older age or number of chronic medical conditions, and with lower rates noted in minorities and those with lower levels of educational attainment. 6
Many hospitalized patients, regardless of comorbidity burden or prognosis, have not had a SIC or ACP.7,8 Patients seen by medicine generalists and specialists are among the most medically complex with the highest mortality risk. 9 Approximately 20% of patients ≥70 years old with an unplanned hospitalization die within one year following this event. 10 It is vital to consider SICs during hospitalization because of this increased mortality risk and to optimize meaningful patient and caregiver participation in the decision-making process,11,12 which are required to honor patient autonomy 13 and provide patient-centered care.
Conversations about patients’ goals and values in the acute care setting can also lead to candid conversations about code status, hospice referrals, and other medical decisions when such decisions are pressing.14,15 Documenting code status within 48 hours of admission is associated with less resuscitation attempts and intensive care unit (ICU) admissions. 16 Though hospice enrollment has increased in the last several decades,17,18 it remains underutilized, including among patients with terminal medical conditions, such as advanced cirrhosis 19 and end-stage heart failure 20 and among patients with hospitalizations prior to death. 21
Clinicians, including hospitalists and primary care professionals at our institution, have previously received training in conducting SICs22,23 and in documenting these conversations using the institutionally approved electronic health record (EHR) module studied in this manuscript,24,25 as it facilitates rapid identification of and building upon prior conversations. This EHR module is reflective of the key components of SICs 26 and includes checkboxes and open-ended questions to describe who the conversations were held with, the patient’s illness understanding, hopes, worries, prognostic information shared, what is important to the patient and family, and recommendations. Providers can fill out the module partially or in its entirety depending on parts of the SIC guide discussed with the patient.
This study aims to determine if use of this EHR module to document SICs (Figure 1)24,25 during a hospital encounter is associated with palliative care consultation, documented change in code status from Full Code to Do Not Resuscitate (DNR)/Do Not Intubate (DNI) or Comfort Measures Only (CMO), hospice enrollment during hospitalization, and 90-day readmissions among patients with high comorbidity burden and healthcare utilization. We hypothesized that standardized documentation of SICs using this EHR module will be low in our cohort and will be associated with these outcomes. Structured Serious Illness Conversation Module Within the Electronic Medical Record.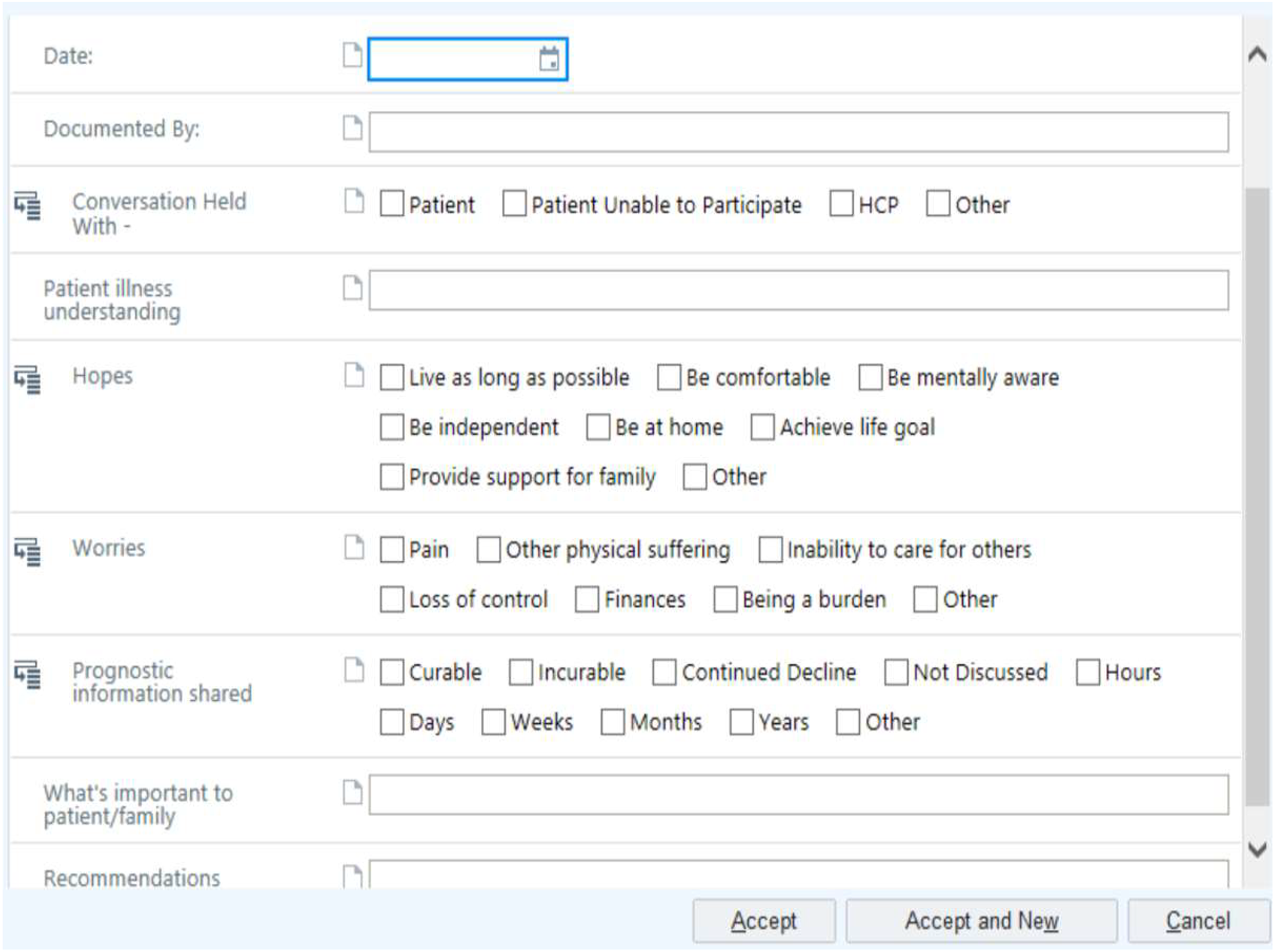
Methods
Study Participants, Setting, Data Sources
We conducted retrospective analyses of adult (≥18 years old) general medicine inpatient encounters at Brigham and Women’s Faulkner Hospital, a community teaching hospital affiliated with Mass General Brigham, a large integrated health care system in Massachusetts, from October 2018 to August 2019. All data were obtained from the enterprise data warehouse, including data from our EHR (Epic Systems, Inc., Verona, WI) and other administrative sources. The MGB institutional review board approved this study.
Propensity Score Matching Protocol
We identified encounters with standardized documentation of a SIC in a structured EHR module (Figure 1) during index hospitalization and matched these encounters by propensity score to encounters without a SIC in a ratio of 1:3 to control for confounding by indication (i.e., clinicians who choose to conduct and document SICs in sicker patients). We used a greedy matching algorithm with caliper size .25 x standard deviation [SD] for each matching variable, without replacement, i.e., the closest match is found for each case and cannot be used in another match. We included sociodemographic, comorbidity burden, and health care utilization factors thought to be potential confounders in the propensity score (i.e., in a multivariable logistic regression model to predict receipt of a SIC): age, sex, diagnosis related group (DRG) weight, electronic Cardiac Arrest Risk Triage (eCART) score (a validated predictor of death, cardiac arrest, or ICU transfer), 27 Epic’s Risk of Unplanned Readmission (Readmission Risk Score [RRS]) 28 and Elixhauser/Van Walraven 29 comorbidity scores on admission, and a history of one or more hospitalizations in the year prior to the index hospitalization. We calculated standardized mean differences (SMDs) for covariates after matching, with < ±.1 considered indicative of balance. We used descriptive statistics to report baseline characteristics, including variables not included in the propensity score, prior to and after propensity score matching.
Propensity Score Matched Analyses
We used multivariable, paired logistic regression to assess the odds of a palliative care consultation, code status change, and discharge with hospice services among patients with and without standardized documentation of a SIC. Models used SIC documentation as the predictor and were additionally adjusted for race, ethnicity, language, median income by zip code, insurance, and any variable used in propensity score matching with an SMD > ±.1.
In secondary analyses, we used multivariable, Cox proportional-hazards modeling, adjusted for the variables listed above, to assess the association between standardized documentation of a SIC and 90-day hospital readmission, where death censors the patient. Kaplan-Meier curves for 90-day readmission were computed.
We also reported percent encounters with and without standardized documentation of a SIC and six-month, post discharge mortality. Among decedent encounters with and without a SIC, percent with a code status of DNR/DNI or CMO at the time of discharge, palliative care consultation, and discharge with hospice services were reported. Fisher’s exact test was used for all statistical comparisons.
Statistical analyses were conducted using V.9.4 of SAS statistical software (SAS Institute, Cary, NC). Tests were considered statistically significant at a two-sided α < .05.
Results
Of 6853 encounters (5143 patients) during the study period, 59 (.86%) encounters (59 patients) had a documented SIC in the EHR module. Using propensity score matching, 58 encounters (.85%) with standardized documentation of a SIC (cases) were matched to 167 (2.43%) encounters (167 patients) without standardized documentation of a SIC in the EHR module (controls). One case did not have any comparable controls, and 5 cases were matched to 1 or 2 controls instead of 3 due to high propensity scores and inability to find additional close matches.
Demographic characteristics of encounters with and without standardized documentation of a Serious Illness Conversation (SIC) prior to and after matching.
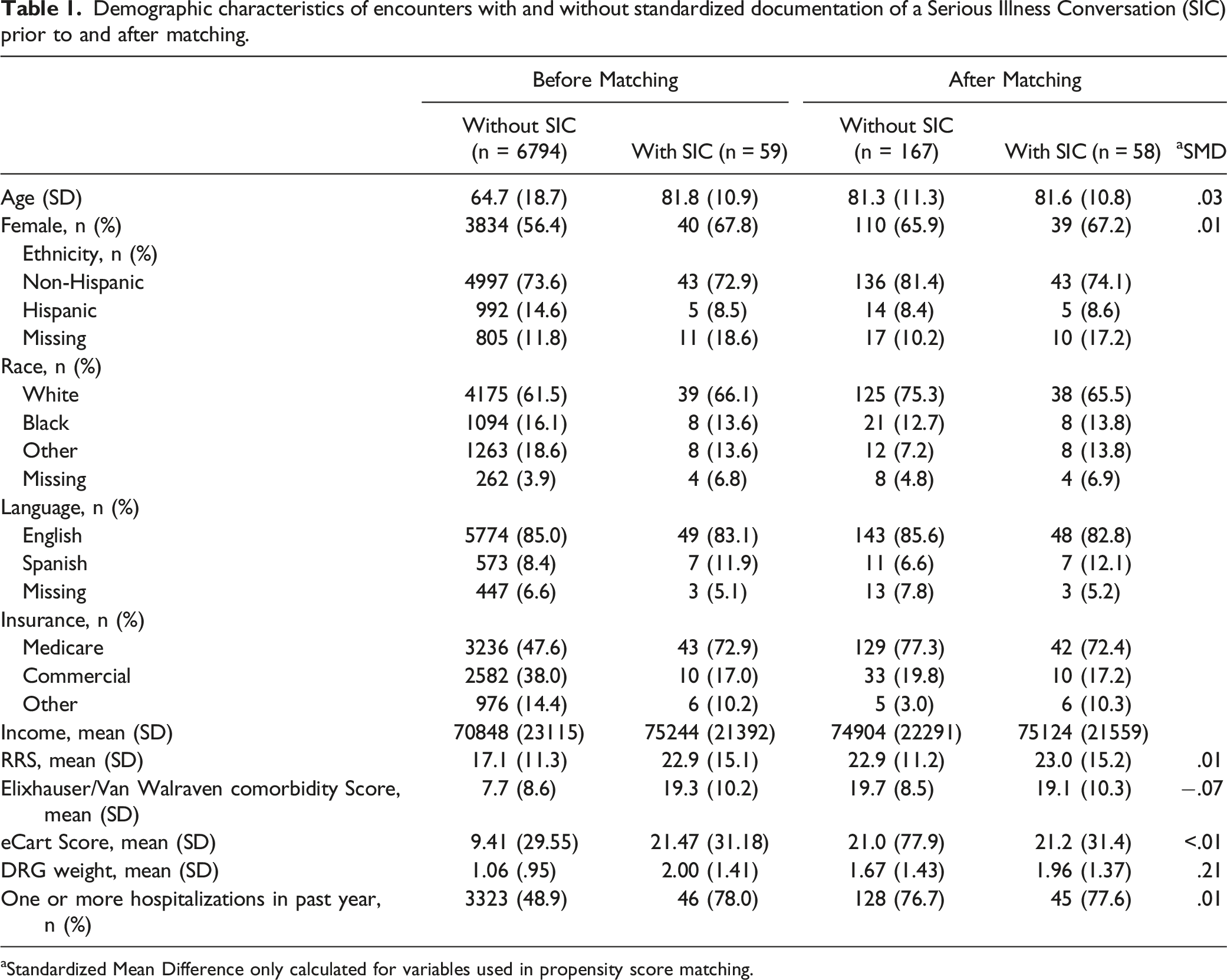
aStandardized Mean Difference only calculated for variables used in propensity score matching.
Propensity score matched cohort analyses of advance care planning (ACP) outcomes in patients with and without standardized documentation of a Serious Illness Conversation (SIC).
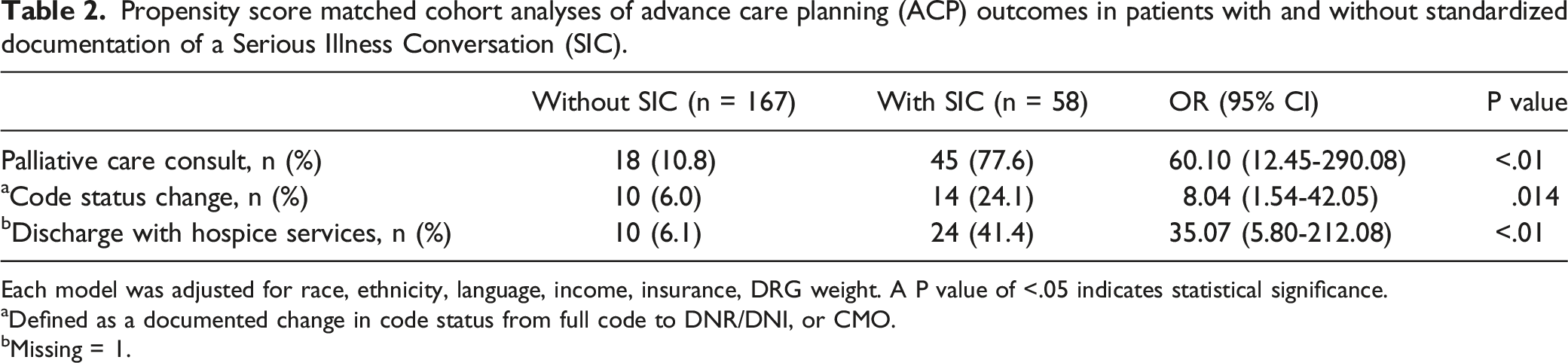
Each model was adjusted for race, ethnicity, language, income, insurance, DRG weight. A P value of <.05 indicates statistical significance.
aDefined as a documented change in code status from full code to DNR/DNI, or CMO.
bMissing = 1.
Thirty-one percent vs 18.0% of encounters with and without standardized documentation of a SIC were associated with death within six months of discharge, respectively (P = .04). Decedents with standardized documentation of a SIC were statistically more likely to have a palliative care consult (15 [83.3%] vs 4 (13.3%) encounters, P < .01) and discharge with hospice services (10 [55.6%] vs 3 [10.0%] encounters, P < .01) than decedents without a SIC. Compared with decedents without standardized documentation of a SIC, decedents with standardized documentation of a SIC had a non-significantly higher percentage of a code status of DNR/DNI or CMO on discharge (15 [83.3%] vs 17 [56.7%] encounters, P = .07).
Discussion
We conducted propensity score matched analyses to explore if standardized documentation of a SIC in a structured EHR module during encounters of general medicine patients was associated with palliative care consultation, change in code status, discharge with hospice services, and 90-day readmissions among general medicine patients with similarly elevated comorbidity burden and healthcare utilization. Our population had low rates of standardized documentation of SICs in the EHR module. Nevertheless, encounters with standardized documentation of a SIC had significantly greater odds of a palliative care consultation, documented code status change to DNR/DNI or CMO, and discharge with hospice services compared to encounters without standardized documentation of a SIC. There was no statistically significant difference in 90-day readmissions possibly due to the increased comorbidity and complex medical needs of this patient population. We also found that a significantly greater proportion of decedents with standardized documentation of a SIC had a palliative care consult and discharge with hospice services.
The low rate of standardized documentation of SICs in our population was disappointing but consistent with national trends.6,7 The observed association between standardized documentation of SICs with our study outcomes may be explained by the high rate of palliative care consultations and attention to shared decision making and patient/family engagement in SICs among these patients. At our study site, as in many institutions, palliative care is limited to inpatient consultations on weekdays with referrals to home-based palliative care and hospice services in the community where appropriate. Though inpatient palliative care consultation is typically reserved for patients with the highest mortality risk,30,31 our ability to successfully propensity match in a ratio of 1:3 suggests that other high-risk patients may have unmet palliative care and end-of-life needs that were not formally elicited and addressed during the hospital encounter. A variety of barriers to conducting SICs and to using the structured EHR module to document the conversation during the hospital encounter may explain this gap, including limited availability of palliative care consultants, 32 lack of standardized indications for palliative care consultation, 33 difficulty with prognostication,28,34 limited clinician time, suboptimal training or discomfort with leading these conversations and documenting them in the institutionally-approved manner. 1
Achieving a healthcare system that values and prioritizes patient-centeredness requires that hospital-based clinicians have tools, training and resources to identify patients with elevated mortality risk, conduct these conversations and document these conversations so they can readily be carried forward in the medical record. 1 Initiatives to improve rates of SICs35-37 or ACP38,39 in the inpatient setting have found higher rates of SIC or ACP completion and improved patient and caregiver satisfaction.37,38 Clinicians also agree that SICs enhance clinical care and can be provided in an appropriate amount of time. 37 Interventions aimed at encouraging SICs in the inpatient, general medicine setting described in the studies above35-37 are diverse and include methods aimed to alleviate the significant time burden of hospital practice by means such as identifying hospitalized patients with unmet palliative care needs (including by age and number of prior hospitalizations), training in use of the SIC guide, standardized documentation of conversations, and additional professional roles to help facilitate SICs in the inpatient setting and coach providers. 22
Limitations of our study include the low number of encounters with standardized SIC documentation and small sample size. SICs that were documented outside the EHR module we described were not studied. It is possible that controls in our cohort had a SIC documented within a progress note or other note type within the EHR. We were also limited by unmeasured confounding by certain indications, such as frailty and failure to thrive, which were not accounted for in the propensity score. Additional limitations include the possibility of reverse causality (i.e., clinicians who initiate a SIC because they intend to recommend a change in code status or referral to hospice). Lastly, we were unable to assess quality of care or health status outcomes, which may be affected by SICs earlier than healthcare utilization outcomes such as 90-day readmission. 4
In conclusion, we conducted a retrospective, propensity matched study and observed that standardized documentation of a SIC during hospitalization, while infrequent in our cohort, is associated with greater odds of palliative care consultation, code status change to DNR/DNI or CMO, and hospice enrollment for patients with high comorbidity burden and elevated mortality risk. Future prospective studies focused on increasing SICs during hospitalization are needed to demonstrate and measure their benefits more clearly.
Supplemental Material
Supplemental Material - The Association of Standardized Documentation of Serious Illness Conversations With Healthcare Utilization in Hospitalized Patients: A Propensity Score Matched Cohort Analysis
Supplemental Material for The Association of Standardized Documentation of Serious Illness Conversations With Healthcare Utilization in Hospitalized Patients: A Propensity Score Matched Cohort Analysis by Myrna K. Serna, Catherine Yoon, Julie Fiskio, Joshua R. Lakin, Jeffrey L. Schnipper, and Anuj K. Dalal in American Journal of Hospice and Palliative Medicine®
Footnotes
Author’s Note
Please direct any questions and requests for data and/or models to the first author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Controlled Risk Insurance Company (CRICO). CRICO had no role in the design or conduct of the study, the collection, analysis, or interpretation of data, or preparation or review of the manuscript. The conclusions in this report are those of the authors and do not necessarily represent the official position of AHR.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.