
Abstract

Keywords
Introduction
Kidney care, especially dialysis, has a substantial environmental impact through greenhouse emissions and waste generation.1-4 Thus, the Canadian Society of Nephrology implemented a Sustainable Nephrology Action Planning (SNAP) committee to inform best practices in environmentally sustainable kidney care (ESKC). 5 The committee outlined the necessity of ESKC, provided an overview of the existing literature, proposed a planetary health care framework of redesigned kidney care, and developed a toolkit called “Creating a Sustainable Canadian Health System in a Climate Crisis.”6-8
Developing and implementing such a framework and toolkit in low- and middle-income countries (LMICs) requires a better understanding of the challenges faced by these health systems as many have substantially lower health expenditure per capita when compared with Canada. However, resource-limited countries are more vulnerable to the impact of climate change and other disasters despite having lower CO2 emissions per capita when compared with many resource-rich countries.9-13 Also, similar to high-income countries, health care in LMICs is a carbon-intensive activity including kidney care as hemodialysis is the only available or most readily available therapy in many LMICs. 14 As the prevalence of chronic kidney disease (CKD) is rising, the burden of kidney care will likely grow substantially as more countries commit to the UN Sustainable Development Goal 3.8 of increasing access to health care.15-17 Thus, the increasing prevalence of CKD, a commitment to improving access to health care by many nations and hemodialysis being the main option available to those with kidney failure further necessitates the need to implement ESKC practices in LMICs.
This opinion piece synthesizes the perspectives of health care professionals (HCPs) who work in LMICs. These members were identified from the two cohorts of the International Society of Nephrology’s Emerging Leaders Program.2,18 This program brings together and mentors a worldwide network of future leaders in kidney care who work collaboratively on issues relevant to the nephrology community. Those who participated, shared their perspectives narratively on the challenges and solutions to providing ESKC in their respective regions. Two co-authors synthesized these inductively into themes (D.B. and S.S.). Implications were then developed collectively.
Characteristics
Ten participants representing 9 different LMICs provided their narratives. Participants represented 1 upper-middle income country (Brazil), 6 lower-middle countries (Egypt, Ghana, India, Lebanon, Nigeria, Sri Lanka), and 2 low-income countries (Ethiopia, Uganda). Hemodialysis is available as a renal replacement therapy in all countries, whereas peritoneal dialysis and transplantation are available in some but not all (Table 1).
Participants, Their Backgrounds, Available Renal Replacement Therapies, and Health Systems in Their Countries.

Note. AKI = acute kidney injury; CAPD = continuous ambulatory peritoneal dialysis; ESKD = end-stage kidney disease; HD = hemodialysis; PD = peritoneal dialysis; KT = kidney transplantation; CBHI = community-based health insurance; CKD = chronic kidney disease.
The health care expenditure and CO2 emissions per capita for all these 9 countries were substantially lower when compared with Canada. The prevalence of patients on hemodialysis in Brazil and Lebanon (a former upper-middle income country) was at par with Canada and slightly lower in Egypt. The prevalence of patients on peritoneal dialysis was much lower in all countries when compared with Canada (Figure 1).
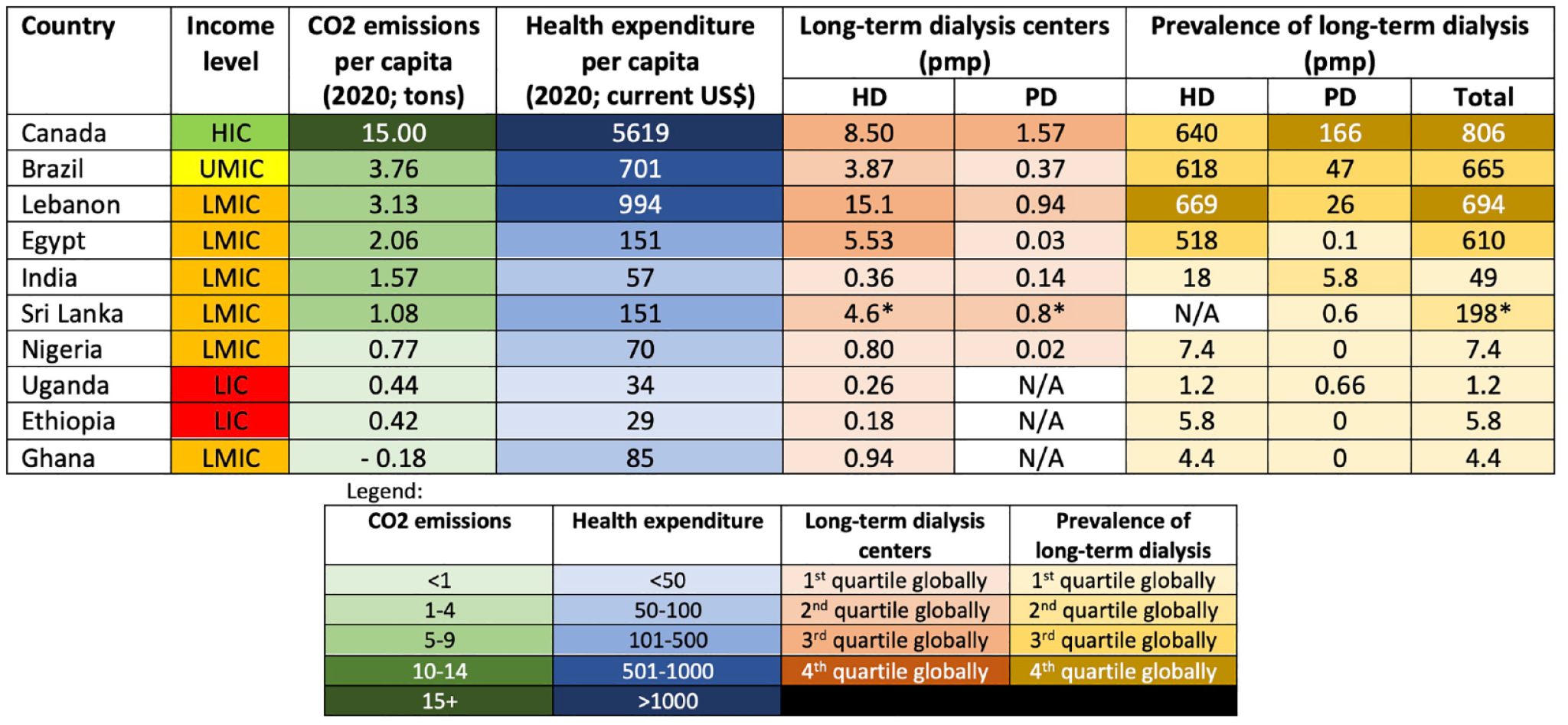
Characteristics of the nine countries whose participants provided narratives compared with Canada organized by the CO2 emissions per capita. 21 Also provided income level, 22 health expenditure per capita (2020; current US$), 23 long-term dialysis centers (pmp), 14 and prevalence of long-term dialysis (pmp). 14
Barriers to Implementing Environmentally Sustainable Kidney Care
A health system comprises several levels,24,25 and we stratified barriers by patient level, provider level, and system level (Figure 2).
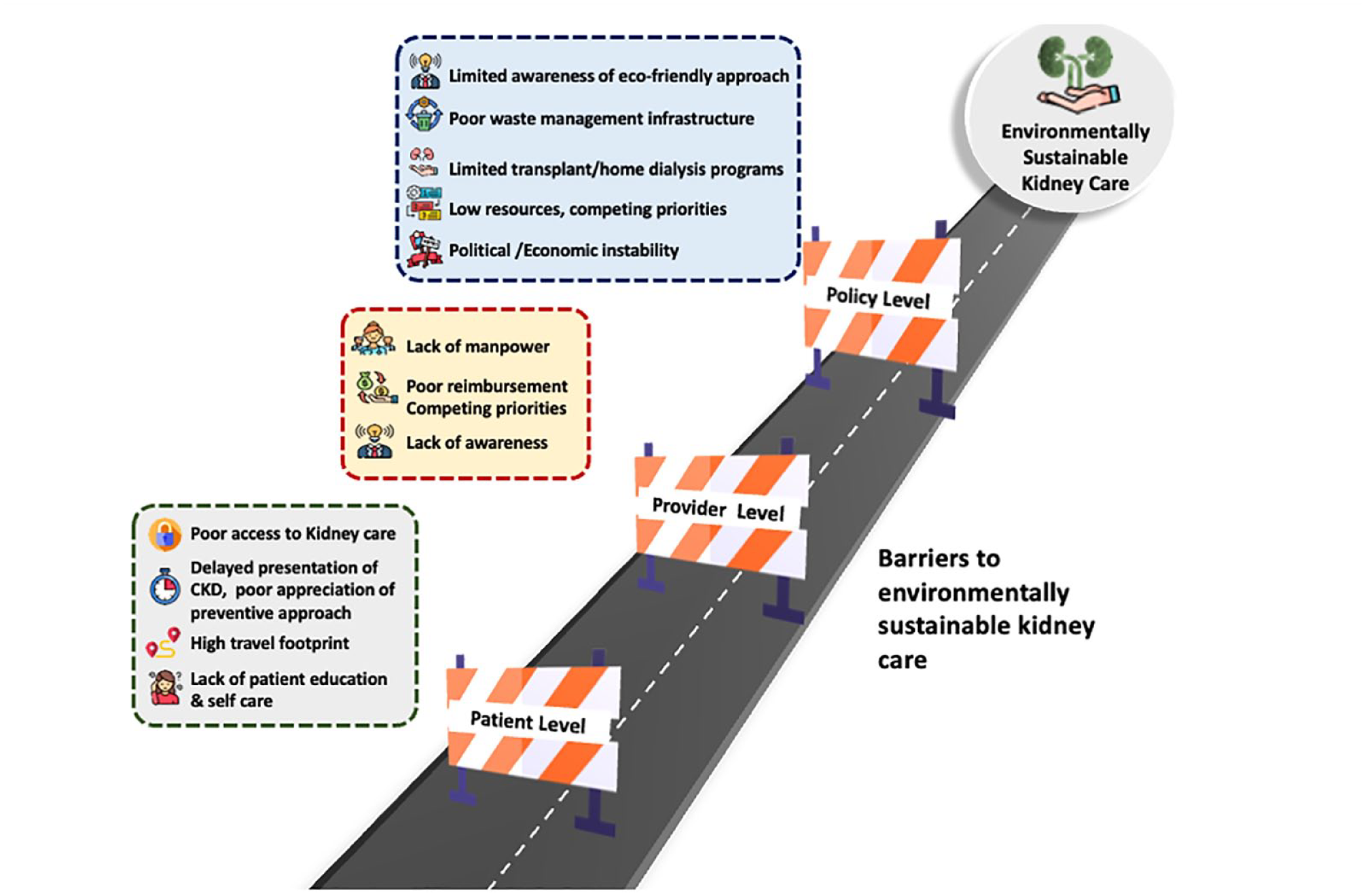
Patient-level, provider-level, and system-level barriers to implementing environmentally sustainable kidney care.
Patient-Level Barriers
Poor and inequitable access to health care
All participants report the lack of universal health care as the most critical barrier to implementing ESKC. Sustainability is not a priority for patients when most cannot afford medications, transplantation, or dialysis, such as in Uganda, where 90% of patients in need of kidney replacement therapy cannot afford it. 26 In addition, access to care is inequitable as most dialysis and transplant programs are located in urban centers,14,20 and many patients incur substantial out-of-pocket expenses (Table 1).
Poor appreciation of preventative approaches and delay in seeking care
Lack of awareness of CKD and delay in seeking care is another critical barrier. In Nigeria, for instance, patients either live in denial of disease even with overt symptoms or consider it as “the will of God” and thus resort to faith-based healing practices or use of herbal concoctions. Thus, many present with uremic symptoms limiting opportunities to initiate early treatments to prevent CKD progression. It is well recognized that the carbon footprint of kidney care increases with increasing CKD stages.3,6 Also, patients are largely unaware of the risk factors for CKD, such as diabetes. Similarly, India is called the diabetes capital of the world. 27 Increasing obesity, sedentary lifestyle, cost of healthy food choices, and increased consumption of cheaper high-carbohydrate diets contribute to the burden of diabetes and CKD.28,29
Lack of patient education and empowerment
Most patients are not fully aware of the environmental impact of kidney care and unaware of practices in ESKC. They are not empowered to engage in self-care and home-based practices, such as through home monitoring of blood pressure, blood glucose, and proteinuria detection. These simple interventions could lower the travel footprint of kidney care and help with early CKD detection and management.
Low uptake of sustainable treatments
In some regions, the uptake of kidney transplantation and home dialysis is low either due to lack of availability (Table 1) or significant cultural and religious barriers. 30 In Lebanon, deceased organ donation is commonly refused because of unfamiliarity with the concept of brain death, denial, and the expectation of a miracle. In some regions, conservative kidney care management is not pursued as it is perceived to be a pathway of abandonment.
High travel footprint
Care delivery tends to be concentrated in urban centers contributing to a significant travel footprint. 20 In India, up to 60% of patients must travel >50 km to access hemodialysis. 27 In Uganda, dialysis facilities are present in 4 districts that cater to the country, as well as to the Eastern Democratic Republic of Congo and South Sudan. In Ethiopia, most hemodialysis centers are situated in the capital. Furthermore, patients often prefer taking individual transportation, such as a fuel-inefficient but cheap ride called a Tuk-tuk in Sri Lanka (Figure 3) rather than public transportation. In other regions, such as Lebanon, public transportation is quasi-inexistent or unreliable.

A Tuk-tuk, a fuel-inefficient cheap ride taken by many patients when accessing kidney care in Sri Lanka. This was one of the many sources of the high travel footprint of kidney care (Picture credit: Eranga Wijewickrama).
Provider-Level Barriers
Lack of education
The greatest barrier is a lack of awareness of ESKC. Some consider it to be a relatively new concept with limited evidence to support practices. Thus, many HCPs struggle to adopt them and advocate for them. In addition, changing behaviors and practices can be met with resistance by institutions and some fear professional repercussions depending on the political climate. Access to relevant educational resources and opportunities to engage in ESKC are also barriers. Some are not well trained or prepared to discuss conservative options in kidney care.
Lack of adequately trained manpower
The lack of medical doctors and pharmacists has been identified as a key barrier to sustainability in Mpumalanga, South Africa; 31 this resonated with all participants. They described an increased burden of undertaking primary care and other care facets due to the lack of adequately trained ancillary staff, such as nutritionists and social workers. Many participants are one of the few specialists in their countries and have a huge patient load to care for (Table 1). This limits the time HCPs can invest in ESKC.
Poor remuneration
In general, many felt that HCPs with the knowledge to deliver dialysis efficiently are inadequately renumerated and relocate to other regions for economic and security reasons. This is well described as the Japa syndrome in Nigeria and further fuels manpower shortage. 32 Moreover, the lack of adequate physician and center reimbursement for home therapies incentivizes the use of a more lucrative option, ie, in-center hemodialysis.
Competing priorities
Chronic kidney disease care is complex and combined with all the factors described above, many HCPs find themselves prioritizing acute patient needs over ESKC practices, such as deprescribing or incremental dialysis. Other low-value aspects were identified, such as maintaining health records on paper (instead of digital), which leads to duplication of work and increases carbon footprint. However, engagement needs organizational support.
System-Level Barriers
Limited resources and competing priorities
All participants unanimously mentioned this as the biggest barrier to implementing ESKC. Many countries at baseline have fragile health care systems and lack the infrastructure to diagnose and treat lower CKD stages. In Nigeria, the budgetary allocation to health was only 5.75% in 2023, far below the 15% target proposed by the WHO. 33 The focus is on communicable and other non-communicable diseases (NCDs); kidney disease is rarely a priority. When it is prioritized, the focus is on accessibility and affordability, not sustainability. In Sri Lanka, eg, when the Ministry of Health makes bulk purchases for tubing and dialysis solutions, cost, quality and immediate delivery are prioritized. Biodegradability or recyclability is generally not a consideration.
Poor recognition of kidney disease as a public health problem
Like patients and HCPs, many administrators, policymakers, and other governmental personnel are largely unaware of the environmental impact of kidney care and the benefits of ESKC. Chronic kidney disease is a neglected NCD in many African regions.34,35 Thus, there is minimal support and low governmental investment in the early detection of CKD and the implementation of preventative measures to delay progression. 36
Political and economic instability
In many regions, unstable governments, ongoing conflicts, and economic crises also contribute. Lebanon, for instance, has been without a president and a lasting government for more than a year. The lack of stable governments challenges any investment toward ESKC. Also, there are significant issues related to inflation and increasing costs that not only impact accessibility and affordability of kidney care but also implementing preventative care, such as healthy diets that are generally more expensive than high fat, sugar and/or salt foods with little or no nutritional value.
Disincentivizing Environmentally Sustainable Kidney Care
Another major barrier is that currently there are no incentives to generate the infrastructure toward ESKC. Many instead reported disincentives due to corruption, bureaucratic interference, and privatization that have led to the prioritization of short-term profits. In many countries, renewable energy sources can be easily implemented; however, high startup costs, lack of enthusiasm, and lucrative commissions for administrators from the fossil fuel sector are significant disincentives. For example, the Nigerian economy is largely dependent on crude oil exportation hindering any efforts to invest in alternative sources of energy.
Poor waste management infrastructure
Many reported a lack of proper waste management practices and policies. Where policies exist, they are often not enforced or strictly implemented due to a lack of resources or ineffective regulatory bodies. Most dialysis units generate enormous waste (Figure 4) and do not have any clear measures for decreasing waste or recycling it.

Pictures demonstrating the amount of waste generated following dialysis sessions in Nigeria (Picture credit: Onu Ugochi Chika).
In some regions, there is no recycling infrastructure, and incineration is the mainstay of waste management. Industrial waste products, poor management of the wetlands, increased urbanization, poor disposal mechanisms, and loose regulations contribute to significant environmental pollution (Figure 5). This directly impacts the risk of acute kidney injury and indirectly the costs associated with kidney care. For instance, removing high levels of arsenic and other compounds from water sources used to generate dialysate in Uganda adds to the cost of delivering dialysis. 37 All these factors contribute to the high costs of dialysis curbing any effort to pursue ESKC.

Pictures demonstrating the poor waste management infrastructure in Uganda (Picture credit: Robert Kalyesubula).
Lack of access to home dialysis therapies and transplantation
In some countries, kidney transplantation is not available, not widely available, or unaffordable. Patient who can afford it, embark on medical tourism, and have to travel to other countries to obtain a transplant. Peritoneal dialysis is also not widely available due to infrastructural and logistical inconsistencies. Thus, patients have access to hemodialysis only, the less sustainable therapy (Table 1).
Poor investments or lack of enthusiasm in research and development
There is limited infrastructure to implement telehealth and telemedicine approaches to minimize the footprint associated with travel in many regions. Before the COVID-19 pandemic, teleconsultations were considered illegal in India, and there were legal repercussions for physicians who pursued them.
In addition, the major worldwide footprint of the health sector is primarily derived from the supply chain through the production, transport, and disposal of goods and services. 38 The industrial infrastructure to manufacture medications and dialysis supplies locally are generally lacking. Thus, kidney care relies on carbon-intensive imports. Of concern was also that the economic instability in some regions has led many multinational drug companies to shut down local manufacturing, worsening the situation.
Many mentioned that the lack of evidence demonstrating the benefits of ESKC significantly hinders advocacy efforts. Poor funding in health research is a major barrier to initiating research projects. For the system to champion ESKC, effective implementation strategies and evidence-based data are required. Without support for research, this cannot be generated. Thus, there is a lack of policy and guidelines on the subject matter.
Policy and Practice Implications
Although large-scale projects have been implemented in some countries, such as the Benban Solar Park project in Egypt to increase renewable energy sources, there have been minimal efforts to adopt such technologies in the health care sector. At the grassroots level, some initiatives were reported. For example, a dialysis center in Uganda utilizes its large open window design to minimize the use of electricity for light and air conditioning (Figure 6). However, participants described the need for system-wide efforts and investments rather than microlevel interventions to effectively promote and adopt ESKC. 39 Many mentioned that global cooperation is required as increasing access to health care must be prioritized in LMICs. We propose implications stratified by scope of relevance (Figure 7).

A local initiative in energy conservation at a dialysis unit in Uganda. Large and open windows in dialysis unit minimize the need for air conditioning and electricity (Picture credit: Peace Bagasha).

A visual representation of proposed practice and policy implications.
Implications at a Global Level
Recognizing kidney disease as an important NCD
A key recommendation is the global recognition of CKD as an important NCD to increase investment in early detection and preventative care. Kidney health has traditionally received far less attention than some other NCDs. The global burden of CKD is enormous and rising. 29 Recognition of CKD as an important NCD will increase investment and promote practices in preventative nephrology and ESKC.
Education of all stakeholders
Educating leaders, politicians, patients, HCPs, and other stakeholders on the environmental burden of kidney care and measures to address them is important. Chronic kidney disease awareness is a cost-effective approach to preventive nephrology as lack of awareness was identified as a key barrier at the patient level, provider level, and system level.
Research and development
There is a need to invest in research and innovation in ESKC. Lack of evidence can significantly hinder the uptake of practices by relevant stakeholders. The development of newer technologies and treatment methods that are both effective and eco-friendly while being cost-effective will increase enthusiasm for ESKC. Health care professionals can then champion developing and implementing such technologies and treatment methods at regional levels.
Implications at a Regional Level
Health care accessibility
Although aspirational, one of the strongest recommendations by all was the implementation of universal, accessible, equitable, and affordable health care. Given the most significant barrier to ESKC pertains to costs associated with kidney care, improving access to home-based dialysis and transplant will prove both cost-effective and more sustainable over in-center hemodialysis. Also, improved health care access that particularly strengthens primary care access may promote early CKD detection allowing interventions to decrease the risk of progression to kidney failure.
Cultivating local expertise
To implement ESKC practices requires local expertise who understand the barriers and are more equipped to develop implementation strategies. Many participants mentioned the disheartening experiences that increased the “brain drain” in their regions. Support mechanisms that promote and nurture the creation and retention of HCPs and implementing appropriate remuneration were key suggestions. Training surgeons in transplantation will contribute to building or strengthening transplant programs.
Investing in preventative measures
As the carbon footprint of kidney care increases with increasing CKD stages, another recommendation was to invest in early detection and prevention of CKD as the best waste is the one which is never generated. Thus, preventive nephrology practices and timely detection and management of risk factors are key strategies toward ESKC.
Creating satellite units and optimizing telemedicine and telehealth practices
Mobile and Internet connectivity is growing in LMICs with half of the population using mobile Internet. 40 Promoting telemedicine and virtual consultation and ensuring appropriate compensation of HCPs will encourage optimal implementation of preventative care, decrease the transportation-related costs, and environmental burden associated with patient and HCP travel. Many respondents emphasized the need to spread available dialysis services to remote areas that can be virtually managed. This can also help implement telehealth geared toward educating the public and patients on CKD and risk factors. Patients can be empowered on self-management and self-monitoring. Smartphone technology with health-based apps can help track health parameters and generate prompts for implementing automated educational resources or a virtual visit with an HCP. Countries like India, with over two thirds of the population using smartphones, can quickly implement such measures. 41
Waste management
Another big recommendation was to invest in not just reducing waste generation, but toward improving waste management, particularly the recycling infrastructure. This was acutely described by some participants from Africa where incineration is a major method of discarding waste. Varied mechanisms are needed depending on the type of waste generated as has been detailed by the World Health Organization. 42 Practices monitoring waste in dialysis units are also needed to inform measures toward ESKC. This may increase governmental investment in it and help plan a clear strategy to address it. At a regional level, in Brazil, some facilities have implemented initiatives to become more sustainable, but national policies would encourage more uptake.
“Make local, buy local.”
Local manufacturing can significantly decrease the costs of supplies and medications which are major contributors to the carbon footprint of kidney care. This may encourage low-carbon innovations and motivate pharmaceutical companies and other manufacturers to compete in finding such solutions. The “Atmanirbhar Bharat movement” and the “Buy Uganda Build Uganda” policy were cited as examples of governmental initiatives to make India and Uganda self-reliant by increasing the local production of goods. This will in turn reduce the carbon footprint of importing drugs and devices.
Implications for the Nephrology Community
Implementing best practices toward environmentally sustainable kidney care
Deprescribing, the process of tapering, stopping, discontinuing, or withdrawing drugs that are not indicated or have poor evidence of efficacy can also make a significant difference by decreasing the environmental burden associated with manufacturing, supply chain, and disposal of drugs.43-45 Approaches to incremental dialysis can also help reduce waste generation.46,47 Cultivating local expertise and generating guidelines to inform other HCPs can help champion ESKC.
“Transplant first” initiatives
Initiatives in increasing kidney transplantation are relevant because it is the better treatment option and generally believed to have a lower ecological burden than dialysis. Implementing this requires significant grassroots efforts in advocacy and education to overcome cultural and religious barriers in some regions and increase both living and deceased organ donation.
Inclusion and representation
Local HCPs with practical knowledge are better equipped to know the barriers and facilitators to implement practices in ESKC in their respective regions. Their inclusion and involvement are extremely important to advocacy efforts. Initiatives from global organizations such as the International Society of Nephrology that support training opportunities for nephrology workforce and increase local expertise and manpower were recommended.48,49
Conclusions
In this opinion piece, we summarized the perspectives of HCPs from 9 different LMICs. Several patient-level, provider-level, and system-level barriers to ESKC were summarized of which lack of education and awareness of all stakeholders are easily modifiable. The lack of universal health care and the high costs of delivering kidney care that prioritizes accessibility over sustainability were unanimously reported as barriers to ESKC. Investment and promotion of lower-cost therapeutic options such as transplantation and dignified conservative care among eligible patients would also decrease the environmental burden of delivering kidney care as they generally have a lower ecological footprint than hemodialysis. Effective development of ESKC and regional implementation requires global collaborative efforts and system-level changes with representation and inclusion of HCPs from LMICs. The implications proposed may help develop an implementation framework for ESKC in resource-poor settings.
Footnotes
Acknowledgements
Drs S.S. and I.E. are supported by the Chercheur boursier clinicien—Junior 1 award from the Fonds de recherche du Québec—Santé. Dr R.K. is supported by a grant from the Mulago Foundation as the Rainer Anhold Fellow.
List of Abbreviations
CKD, chronic kidney disease; ESKC, environmentally sustainable kidney care; HCP, health care provider; LMIC, low- and middle-income country; NCD, non-communicable disease.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr S.K. is a scientific consultant for George Clinical. Dr V.C.-S. is a speaker and consultant from Baxter Brazil. Dr S.S. has received an education grant from Amgen Canada. The rest of the authors have no relevant disclosures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
No new data generated.