
Abstract
Background:
During the 30-day period prior to initiating dialysis, there is a 10-fold rise in emergency department visits and hospitalizations related to kidney failure.
Objective:
The Virtual Ward Incorporating Electronic Wearables (VIEWER) trial implemented a home telemonitoring system to track changes in patients’ vitals and assess their adherence and the acceptability of telemonitoring in a chronic kidney disease (CKD) population.
Design:
A pilot prospective clinical trial using a mixed methods approach was performed.
Setting:
The research was conducted in Winnipeg, Manitoba.
Participants:
There were 2 phases: Phase 1 was a 2-week-long pilot trial consisting of 10 participants. Phase 2 was a 3-month-long trial with a total of 26 participants. Patients with an estimated glomerular filtration rate <15 and a >40% risk of beginning dialysis in the next 2 years according to the kidney failure risk equation were eligible to participate in the study.
Methods:
The primary quantitative outcome was adherence, defined as the proportion of daily self-assessments completed using VIEWER over the follow-up period. The usability and acceptability of VIEWER was assessed qualitatively at the end of the trial through structured questionnaires and focus groups.
Results:
Phase 1 participants (n = 10) had a median adherence of 77.17% for the 2-week observation period. Phase 2 participants (n = 26) showed a lower median adherence of 36% for the 3-month period. Focus group participants (n = 11) identified many positive aspects of VIEWER, including increased awareness and empowerment over health, simplicity of the data platform, and the ability to show clinical staff their health trends. Some challenges identified with VIEWER were connectivity issues with the Bluetooth, perceived inconvenience, and negative thoughts toward their health
Limitations:
Limitations of the study include a small sample size, which limited our ability to measure quantitative outcomes. In addition, patients agreeing to participate in any trial are generally more highly motivated and engaged in their care than those declining participation. Therefore, our results may not be generalizable to individuals who are not interested in self-management of their health.
Conclusion:
Our results suggest that home telemonitoring in patients with advanced CKD is feasible using a CKD-specific platform like VIEWER. We anticipate that improved functionality with incorporation of feedback from this study will result in greater long-term adherence. A future randomized clinical trial is planned.
Introduction
Chronic kidney disease (CKD) is a growing epidemic worldwide. Within Canada, the prevalence of CKD is 12.5% and rising, representing approximately 4 million Canadian adults. 1 Chronic kidney disease is a dominant risk factor for kidney failure, heart disease, and other complications. These outcomes are expensive to manage and resource intensive, imposing an ever-growing burden on health care systems. 1
The clinical management of CKD can be roughly separated into 2 phases. In early-stage CKD (stages 1-3, glomerular filtration rate [GFR] >30 mL/min/1.73 m2), identifying underlying pathology and slowing disease progression are the primary concerns. 2 In the later stages of CKD (stages 4-5, GFR <30 mL/min/1.73 m2), the focus shifts progressively to preparing the patient for kidney failure and dialysis.2,3 This latter phase has a highly variable trajectory, making it very difficult to predict precisely when dialysis will be required. As a result, more than 50% of advanced-stage CKD patients will experience a suboptimal initiation of dialysis, defined as an unplanned or emergent start via a temporary hemodialysis catheter. 4 These suboptimal dialysis starts are usually preceded by a rapid onset of severe uremic symptoms and often occur despite close multidisciplinary care. 4 They are associated with poor outcomes, including volume overload or hyperkalemia, higher mortality, increased health care costs, and hospitalizations.5-10 Beyond these direct adverse consequences, suboptimal dialysis starts are also associated with a significant decrease in the proportion of patients ultimately pursuing home dialysis therapies. Thus, preventing suboptimal dialysis starts will likely be of key importance in maximizing uptake of home treatment modalities, a major priority for the renal community.
Telemonitoring and virtual ward technologies (virtual case management) have shown benefit in reducing acute decompensations, readmissions to hospital, and mortality in specific, high-risk disease states such as heart failure. 11 A disease-specific platform, tailored to the nuances of disease-specific management, and supported by specialized teams, appears to be required for efficacy. 11 Although direct evidence in CKD is still lacking, it is reasonable to hypothesize that enhanced monitoring of patients with late-stage CKD using a tailored telemonitoring platform could reduce the rate of suboptimal dialysis starts. Currently, however, CKD-specific home monitoring platforms do not exist, preventing further research on this important question. To address this technology gap, we developed a CKD-specific telemonitoring and virtual case management platform called Virtual Ward Incorporating Electronic Wearables (VIEWER). As part of the development of VIEWER, we sought to understand how individuals with CKD experience VIEWER, how acceptable they find the user interface, and whether any aspects of the daily use experience could be improved. We therefore conducted a pilot, prospective clinical study using a mixed methods approach to assess user experiences with the VIEWER platform in a small cohort of advanced CKD patients.
Materials and Methods
Design and Setting
This prospective clinical trial was conducted in 2 phases, using a mixed methods approach. Phase 1 was a short, 2-week-long “proof of concept” study of 10 participants. The aim of this phase was to identify any “fatal flaws” in the software or component devices and was conducted between November 2017 and March 2018. The second phase consisted of a 3-month prospective observational study which sought to capture long-term use data from participants. Phase 2 included 26 patients recruited between April 2018 and July 2019 (see Figure 1 for participant flow diagram). We have used the consolidated criteria for reporting qualitative research to describe our methods 12 (see Appendix Table A1).
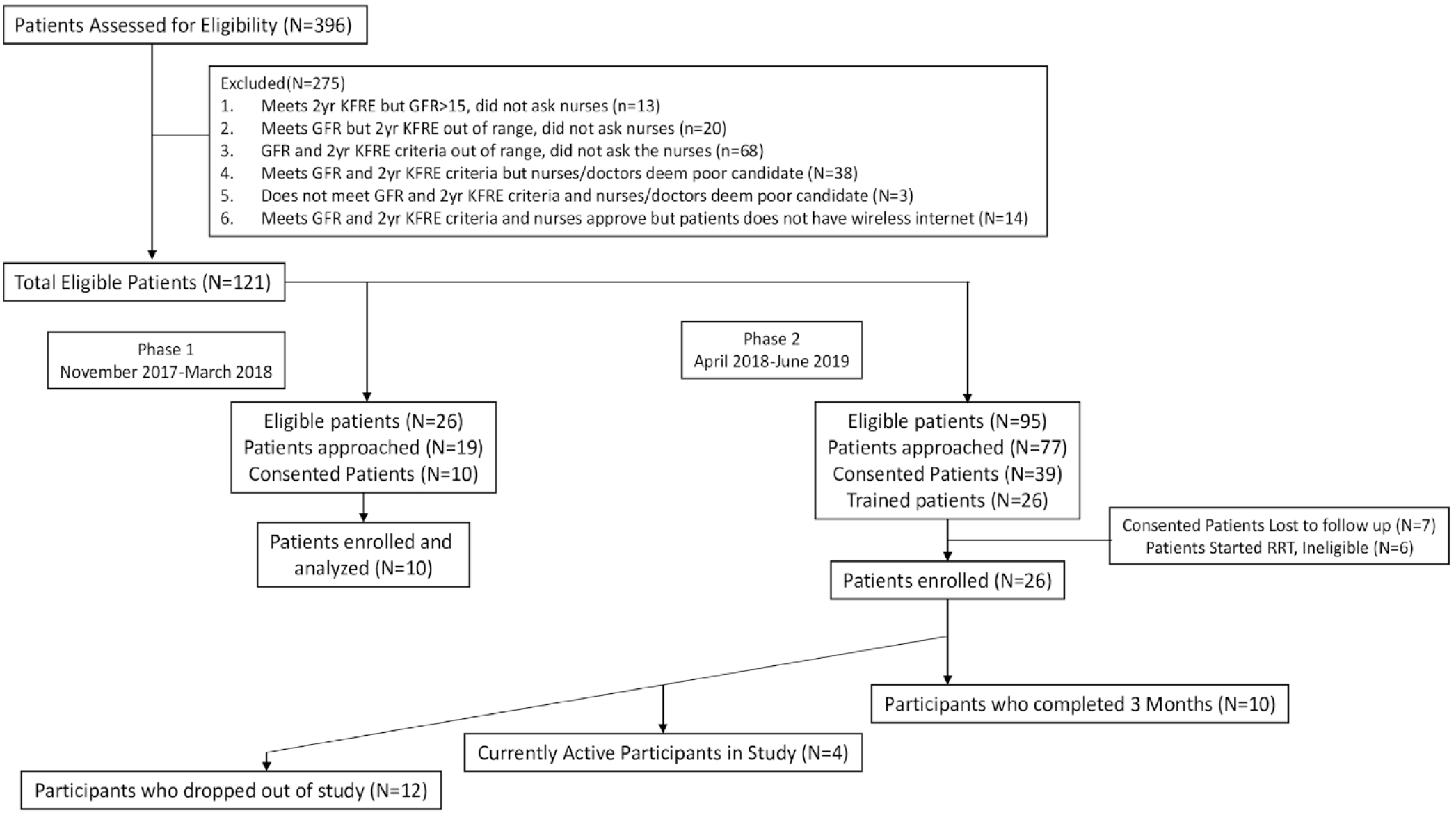
Study flow diagram.
Telemonitoring Hardware and Software (VIEWER Kit)
The Virtual Ward Incorporating Electronic Wearables is a suite of hardware and software components specifically designed to monitor CKD patients. It was developed jointly by the Chronic Disease Innovation Centre (CDIC), and a Canadian health technology company (Enhancing Quality of Life [eQOL]) based in Toronto, Canada (https://eqol.ca/). As the literature of CKD telemonitoring is sparse, the selection of devices and measurements to be tracked by the kit was based on data from heart failure models 11 plus input from practicing nephrologists regarding key metrics to follow. The VIEWER kit includes an Apple iPad mini with the VIEWER app preinstalled, a wrist-based motion detector (similar to a Fitbit), a blood pressure (BP) monitor, pulse oximeter, and a weigh scale (see Figure 2). Data from these peripheral devices (movement [step count], BP, weight, and oxygen saturation) are uploaded wirelessly via Bluetooth to the VIEWER app running on the iPad. The VIEWER app also prompts patients to perform a weekly CKD symptom survey using the modified Edmonton Symptom Assessment Scale (mESAS) (see Appendix Table A2). 13 The VIEWER app was developed only for iOS as iOS mobile app development performs very well, is fast, reliable, and with few bugs remaining in the final build of an app compared with other operating systems. 14 All patient data are encrypted and securely uploaded to Health Insurance Portability and Accountability Act (HIPAA)/ Personal Health Information Act (PHIA) -compliant servers. This information is made available to the research team (research coordinator and principal investigator). The research-facing component is based on Web technologies. As such, patient information collected through VIEWER is available to the research team through an Internet Web browser after securely logging in. The VIEWER app via eQOL is fully compliant with the security, privacy, and encryption standards set out by the Personal Health Information Protection Act of Ontario and the Personal Information Protection and Electronic Documents Act of Canada.

VIEWER kit components.
Participants and Training
Participants were recruited from the multidisciplinary Kidney Health Clinic at Seven Oaks General Hospital, located in Winnipeg, Manitoba. The clinic currently follows approximately 1500 patients with advanced CKD (2-year kidney failure risk >20%, 5-year risk >50%). Patients were eligible for inclusion if they were over the age of 18 years; had CKD stage 5 (estimated glomerular filtration rate <15) and an estimated risk of kidney failure >60% in 2 years (calculated using the 4-variable kidney failure risk equation); 15 were able to provide written informed consent; were able to read and understand English; and were cognitively and physically capable of using a tablet computer and performing self-measurements (eg, weight). We excluded patients who did not desire renal replacement therapy (ie, palliative management of end-stage renal disease). To improve recruitment, the kidney failure risk criterion of >60% risk of requiring dialysis in 2 years was relaxed to >40% for phase 2.
Each study participant was given a 1-on-1 structured training session on how to use the VIEWER kit. At this training session, coordinators provided each patient with a secure, password-protected VIEWER application login. Patients were shown how to operate the app, pair the peripheral devices, and were instructed to use their peripherals to perform self-assessments at least once daily. Patients were shown how to fill in the mESAS symptom survey and were instructed to do so weekly. Daily monitoring was encouraged as previous studies on telemonitoring in patients with heart failure showed that daily reporting of weight and symptoms in patients with advanced heart failure would reduce rehospitalizations.16-18
Each participant was given as much time as needed to practice these simple procedures and demonstrate competency. Simple troubleshooting materials in the form of a visual flip chart were provided. A contact number for the study coordinator was provided and patients were encouraged to call if any difficulties with equipment arose.
Measurements
Adherence
Our primary outcome was adherence, measured as the percentage of daily self-assessments successfully performed over the follow-up period. Successful completion of a daily self-assessment was defined as uploading at least 3 out of the 4 self-assessment components (BP, weight, step count, and oxygen saturation). Adherence with the symptom survey was assessed separately as the percentage of weekly symptom surveys completed over the follow-up period. Secondary analyses measured adherence with each individual monitoring component.
Patient Satisfaction and Usability
Patient satisfaction with VIEWER was measured using a structured questionnaire administered as part of an exit interview (see Appendix Table A3). The survey was developed with input from initial beta-testers and an expert in human-computer interaction (O.T.S.) and consisted of Likert scale and open-ended questions. The Likert scale questions were rated on a scale of 1 to 5, 1 being strongly agree and 5 being strongly disagree. The questions were divided into the following themes: training experience; enjoyment/satisfaction; clarity/ease of use; ease of fit into a daily schedule; perceived benefits; and desired future modifications to VIEWER. Figure 3 summarizes 7 central close-ended statements from the survey. Participant open-ended question responses are summarized below in terms of advantages and disadvantages of VIEWER.

Participant’s responses to 7 central close-ended statements.
Qualitative Measures
Our primary qualitative objective was to gain a holistic understanding of patient experiences and perceptions of VIEWER. We approached this in 2 ways. First, we conducted an exit interview with all patients, and asked open-ended questions about their experiences using VIEWER. These responses were recorded for subsequent thematic analysis. The exit interview was held at the clinic, usually following a regularly scheduled clinic visit, but was done over the phone in some cases for participant convenience. Second, we conducted 2 focus groups, held on October 2018 and June 2019, with patients who completed the follow-up period. Study participants and their spouses/partners/caregivers were invited to participate. Focus group sizes were kept to 5 to 10 individuals, which is considered optimal for balanced group discussion. 19 Focus groups lasted 60 to 90 minutes and were held at the CDIC located at Seven Oaks General Hospital.
Focus groups were conducted using standard methodology and were moderated by research coordinators (D.P. and L.B.). 20 We used convenience sampling for the focus groups. The focus groups were conducted in a face-to-face manner and were led by members of the research team (L.B. and D.P.). Each group had a primary interviewer with the other interviewers taking detailed handwritten notes. At the start of each discussion, the moderator explained the purpose of the focus group to the participants, as well as ground rules for participation that would allow all persons to share opinions in a safe environment. All participants consented to participate in the focus groups and audio-recording of the session. All sensitive information was deidentified upon transcription for the purpose of analysis. A focus group guide was prepared prior to the sessions to be used as needed to redirect the discussion and make sure multiple dimensions of the patient experience were addressed. The transcripts were coded independently and in duplicate using NVivo qualitative analysis software (https://www.qsrinternational.com/nvivo/home) by 2 reviewers (L.B. and D.P.). The open and axial codes were then categorized into themes, which are described below in the “Results” section.
Ethical Approval
The study protocol was approved by the Health Research Ethics Board (HREB) at the University of Manitoba (HREB#: H2016:256 [HS19867]).
Results
Patient Population
In total, 36 patients were enrolled in the 2 study phases. Participants were mostly male and had a mean age of 57 years (32-81 years; SD ± 12). Seventy-two percent of participants (n = 26) lived in urban areas, and 28% (n = 10) lived in rural areas (see Table 1).
Demographics of all Participants in the Study, N = 36.

Note. eGFR = estimated glomerular filtration rate; ED = emergency department.
A flow diagram outlining patient enrolment and inclusion/exclusion criteria is shown in Figure 1. In phase 1, 19 patients were approached, and a total of 10 patients were enrolled in the study. During phase 2, which began in the spring 2018, a total of 77 patients were approached, out of which 26 patients enrolled and 10 completed the study. Because of the limited number of study kits, the group of patients in phase 2 were recruited separately but consecutively over a 1-year period. The reasons patients gave for dropping out in phase 2 were (1) it reminded the participant of the disease (1 patient), (2) the kit was hard to carry around when traveling by plane (1 patient), and (3) participants found inconvenient to complete the daily monitoring (10 patients).
Quantitative Outcomes
Patient Adherence
We tracked participant uploads of data as a measure of adherence in accordance with the study protocol. Phase 1 participants (n = 10) had a median adherence of 77.17% for the 2-week observation period. Phase 2 participants (n = 26) showed a lower median adherence of 36% for the 3-month period. The adherence distribution was bimodal. Patients who completed the full trial period had a median adherence of 72.47%. In contrast, patients who dropped out early had a median adherence of 18.36%. Adherence to checking BP was highest, with a mean daily measurement of 83%. The lowest adherence was the completion of the weekly symptom survey and measurement of step count, which was a mean of 64% and 66%, respectively.
Edmonton Symptom Assessment Scale
In the ESAS, the symptoms reported as most severe were pain (mean 4.14 [±2.90]), well-being (mean 4.50 [±2.46]), and tiredness (mean 2.48 [±2.53]) among participants in the phase 2. The participants during phase 2 responded a median of 8 questionnaires during their study time.
Qualitative Outcomes
Exit interview survey
Perceived advantages of VIEWER:
Most participants identified increased awareness and empowerment over their health as a major benefit of VIEWER. Participants enjoyed the ability to collect vitals and plot trends, which they found helpful in managing their health.
VIEWER made me more aware of my condition. We were able to check blood pressure right at home instead of going to doctor or ER, which was nice. [Study participant 0036]
Most patients also found VIEWER easy to use and intuitive.
“Very easy and comfortable to use!” I would highly recommend [VIEWER] to all CKD patients. You don’t have to be computer-literate to use [VIEWER]. [Study participant 0026]
Finally, patients liked being able to refer to their trends in weight, BP, and other vitals during clinic visits with the health care team. The ability to see trends in BP was of particular interest to many participants and was the most commonly cited positive aspect of the kit.
Perceived disadvantages of VIEWER:
Some patients experienced challenges when using the kits. When devices failed to connect automatically by Bluetooth, participants found these issues frustrating, especially those less comfortable with technology.
The weight scale didn’t always connect via Bluetooth and took a long time to measure the weight. [Study participant 0022]
In addition to general connectivity issues, participants also described problems with the activity tracker included in the kits. There were several concerns, including short battery life, difficulty navigating functions, and discomfort with wrist wearing.
Focus Groups Findings
In the first focus group, a total of 5 participants (3 males and 2 females) attended. The second focus group consisted of 2 males and 2 females, plus, 2 patient spouses, making a total of 6 participants. The following results are presented according to 3 themes identified in the focus groups: (1) perceived strengths of VIEWER, (2) perceived challenges with VIEWER, and (3) desired future state for VIEWER.
Perceived Strengths of VIEWER
Ease of use and daily integration
Most participants had little trouble completing the daily self-assessments operating the app and the kit devices. The user interface was found to be reasonably intuitive and allowed participants to easily progress through measurement of their vitals. Participants mentioned that conducting the self-assessments quickly became routine. Most patients found it easiest to complete the assessments either when waking up or prior to heading to bed (see Table 2). Patients also stated that having a specific place in their home where they could set up the equipment was helpful, because having it visible to them served as a reminder and made it easier for them to comply with daily assessments (see Table 2).
Strengths of VIEWER—Patient Quotes.
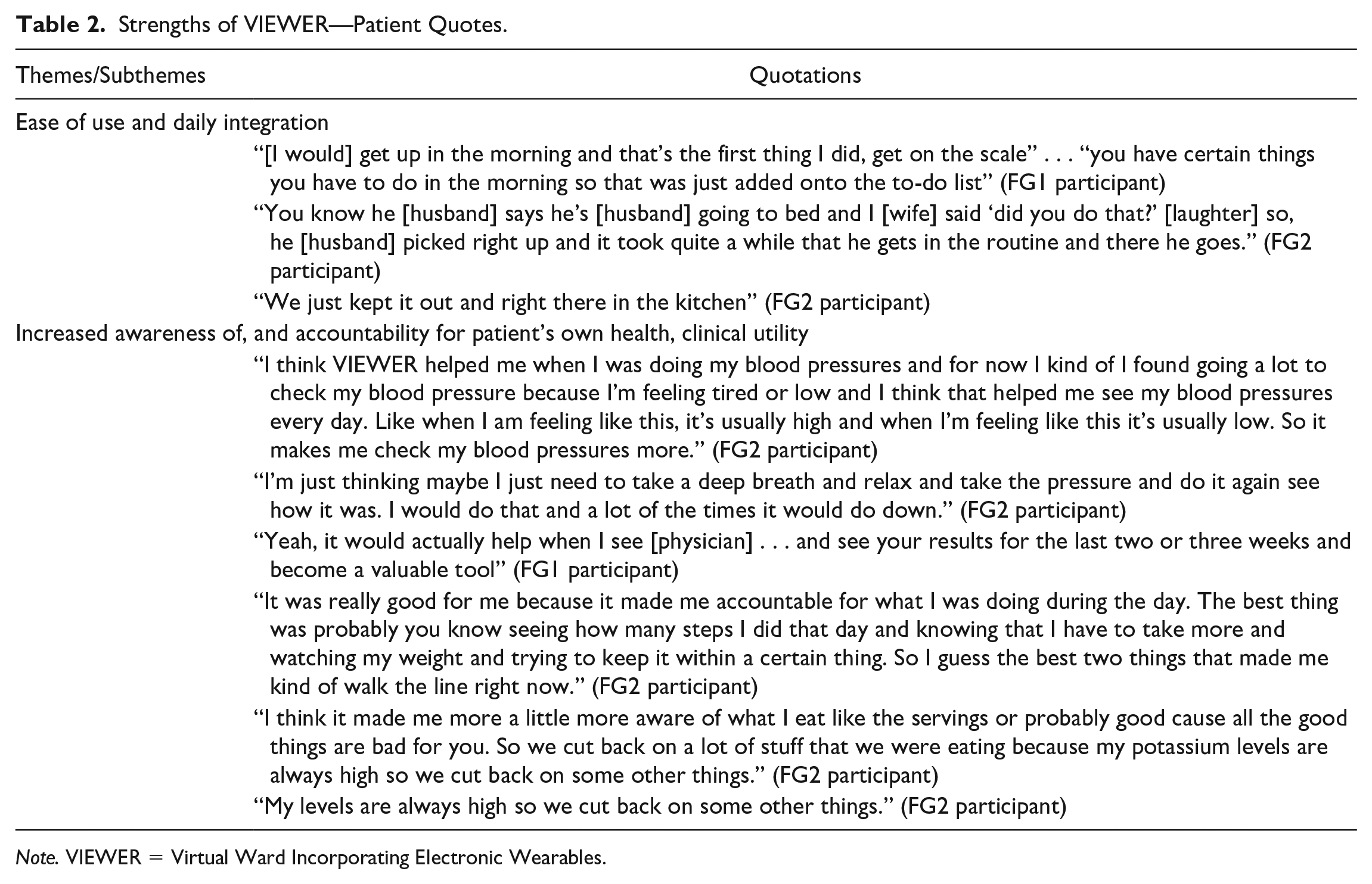
Note. VIEWER = Virtual Ward Incorporating Electronic Wearables.
Increased awareness of, and accountability for patient’s own health, clinical utility
Most patients felt monitoring trends in a simple, digital format with VIEWER increased their sense of autonomy and health awareness. In some cases, these positives were so significant that participants continued self-monitoring of weight and BP on their own without VIEWER after the study was completed (see Table 2). Overall, patients valued having the ability to show their health care team past trends and current values during clinic visits. The Virtual Ward Incorporating Electronic Wearables provided patients with a way to show providers the effort they were making toward bettering their health and empowered them to express concerns to their health care providers (see Table 2). The activity tracker in particular encouraged participants to engage in more activity to reach a higher step count (see Table 2).
An increased sense of autonomy and ability to self-manage was seen in both patients who were new to self-monitoring (ie, had not been self-monitoring at home) and those who had previously self-monitored. Most participants did not routinely self-monitor prior to participation in the study, and found that by incorporating VIEWER into their routine, they developed a greater sense of engagement, awareness, and control over their own health (see Table 2). For patients who did practice self-monitoring prior to participating in the study, VIEWER provided a useful and integrated way to store and present trends and changes in their health. Several patients noted that they would never have been able to afford devices with similar functionality on their own. Indeed, the cost of commercially available devices was cited as a “barrier to entry” for those interested in monitoring on their own. One patient noted he could not afford a home BP monitor and would use BP machines in pharmacies and stores to monitor BP outside of clinic (see Table 2).
Perceived Challenges With VIEWER
Connectivity and peripheral device problems
A number of technical problems were faced by several patients, including connectivity issues (eg, devices failing to pair with iPad, Wi-Fi connectivity issues) as well as general difficulties using the equipment, such as changing or charging batteries (see Table 3). The activity tracker proved to be especially problematic. Besides troubles with connecting the activity tracker to the iPad, users also found it uncomfortable to wear, citing that the band material made the wrist sweaty and uncomfortable. In addition, it was difficult to navigate through the different functions of the device (see Table 3). Further problems cited were difficulty viewing data on the activity tracker and attaching the wristband to the wrist, especially in patients with impaired manual dexterity. Patients also felt that the battery life was too short, as it required daily charging, which was seen as burdensome and discouraged daily use.
Challenges With VIEWER—Patient Quotes.

Perceived inconvenience
Beyond the technical difficulties encountered when using VIEWER, some participants found it difficult to remember to conduct the daily measurements and weekly surveys. They suggested incorporating reminders within the application to complete the surveys and daily measurements (see Table 3). However, most participants found that with time, VIEWER became part of their daily routine. Participants did note that the perceived burden of using the kit varied with the state of their health. When participants felt ill, due to declining kidney health or other illness, daily reporting decreased dramatically (see Table 3).
Effect on perception of health
Some participants felt discouraged when they observed adverse trends in measurements (eg, rising BP or weight). These negative trends reminded patients that they had a chronic progressive illness (see Table 3). These feelings were noted primarily by participants who progressed to dialysis during their time using VIEWER.
Desired Future State of VIEWER
Increased ease of use
An activity tracker with improved battery life, better user interface, and a more ergonomic wristband was deemed a top priority by patients. Participants also desired a more portable case for VIEWER as many patients traveled and would have taken VIEWER along, but the current kit was too bulky and difficult to carry. Finally, reminders of when to complete the self-assessment and surveys were desired by some participants (see Table 4). Patients suggested adding the ability to set up push reminders to cell phones.
Recommendations for VIEWER—Patient Quotes.

Increased comprehensiveness of health management
Participants valued the ability to plot values and track trends in their vitals. Many participants would like to see a more comprehensive list of health metrics to track, in particular, the ability to track blood sugars in diabetic patients, or the ability to enter and track key blood test results (see Table 4). Patients also requested the ability to record symptoms they are experiencing in free text, in addition to the structured weekly symptom survey. They felt that incorporating this additional information into the application would increase the perceived value in using it and would encourage use.
Increased support and education for patients
In the focus groups, it became evident that each participant had unique experiences in their health care journey. Some felt fully prepared for dialysis, while others felt left in the dark. One key function that patients felt should be added was a confidential messaging system whereby patients could ask simple, nonurgent questions to health care staff (or to support staff for the technical aspects of the kit) (see Table 4). Patients felt that with a messaging system in place to address minor complaints, they could reserve hospital and clinic visits for more serious issues, and worry less about minor symptoms, thereby improving quality of life. Patients also expressed that their motivation to use the system would increase if they knew the data they were tracking were being regularly reviewed by health care staff, and had a direct impact on their clinical management.
Discussion
Our results suggest that home telemonitoring in patients with advanced CKD is feasible using VIEWER and is likely to be well accepted by many high-risk CKD patients. Our results also suggest that a randomized clinical trial of the utility of VIEWER, amended and improved according to patient feedback received in this study, is justified.
While evidence for the feasibility, acceptability, and efficacy of remote monitoring is sparse for patients with CKD, 21 data are more abundant in other chronic diseases such as heart failure, and to a more limited extent, chronic obstructive pulmonary disease. Previous work has shown that home telemonitoring strategies reduce hospital readmissions in individuals with heart failure. 20 Few studies have examined telemonitoring use in CKD and most of these have been very limited in scope (eg, home BP monitoring alone). A systematic review found that electronic health (eHealth) self-management interventions in patients with CKD have the potential to improve CKD patients’ management and health outcomes. 21 However, to our knowledge, none have addressed clinically important outcomes such as prevention of suboptimal dialysis starts in patients with advanced CKD. This may in part be due to the lack of readily available CKD-specific platforms for telemonitoring, an issue directly addressed by our results. 22 Furthermore, it is unknown whether changes in specific vital signs (ie, BP and physical activity/step counts) might reliably predict an impending dialysis start. 23
As a short-term pilot and feasibility study of a new telemonitoring platform, we could not meaningfully measure major clinical outcomes. It was encouraging to note, however, that many patients described improvements in their sense of empowerment over their health, with greater sense of insight, autonomy, and control over their illness.
It is important to acknowledge that VIEWER is associated with some challenges in addition to benefits. A few patients were discouraged by the decline in “good” readings, as this was a daily reminder of their affliction with a chronic progressive disease. These patients felt less motivated and experienced more negative feelings toward daily monitoring, a finding noted in other studies. 24 In future iterations of VIEWER, it may be possible to mitigate these negative effects with appropriate integration of education and health team communication resources. 25 Indeed, identification of “worsening” trends, in the appropriate setting, may stimulate learning, improve control, or at the very least, permit honest and objective discussion about the need to start dialysis preemptively.
Not surprisingly, adherence with VIEWER was higher in the short term than over the long term. In phase 1, median data collection adherence was moderately high in all participants. In phase 2, adherence was bimodal: Patients seemed to self-select into consistent users versus nonusers of the kit. The dichotomy between consistent users versus nonusers likely reflects the burden of sustained self-monitoring and highlights the importance of making the mechanics of self-monitoring as streamlined as possible. Blood pressure monitoring had the highest patient adherence. This finding was not surprising, as patients are encouraged to check their BP at home in routine clinical practice. In contrast, adherence was poorest with the weekly symptom survey. This could be attributed to forgetfulness and may be amended by the addition of reminders within the application. Moreover, the survey is only conducted once per week, making this portion of the platform less habitual. In regard to poor adherence with the activity tracker, participants stated it was difficult to use, had poor battery life, and was uncomfortable to wear. In later studies, we hope to improve this by substituting a new activity tracker, as well as refining the user interface to improve survey completion.
Our study has several strengths. Patients were recruited and followed up prospectively for up to 3 months. We used multiple qualitative research methods (interviews, surveys with open-ended questions, focus groups) to address patient perceptions of VIEWER. To our knowledge, this study is novel and represents the first report of the feasibility, usability, and patient acceptability of a CKD-specific home telemonitoring tool. The VIEWER kit is a powerful tool that affords patients greater autonomy, awareness, and provides them direct feedback for greater accountability.
Our study also has acknowledged limitations. In this study, we did not aim to achieve data saturation as this was beyond the scope of this initial work. Recall bias is possible because focus groups were conducted some months after study participation. Our sample size was small, limiting our ability to measure quantitative outcomes. Patients agreeing to participate in any trial are generally more highly motivated and engaged in their care than those declining participation. Our results may therefore not be generalizable to individuals who are not interested in self-management of their health. Furthermore, our sampled population did not represent the full cultural spectrum of high-risk CKD patients. These limitations are inherent to the current platform, which, at this early stage of development, is limited to the English language, and requires wireless Internet, a resource that may be unavailable in rural and remote communities. These issues will need to be addressed in future iterations. Despite these limitations, we believe our results justify further development of VIEWER, especially as it has the potential to provide medical monitoring to a vulnerable and at-risk chronic disease population.26,27
Conclusion
Late-stage CKD is a high-risk disease state that leaves many patients vulnerable to rapid decomposition and often results in suboptimal dialysis starts and poor outcomes. To our knowledge, VIEWER is the first telemonitoring platform tailored to monitor this patient population. Our results suggest that such a platform may encourage patients to be more involved in managing their health and provide welcomed context when discussing concerns with health care teams. A large, mixed methods randomized controlled trial across several sites in a larger patient population is needed to further test the efficacy of VIEWER.
Footnotes
Appendix
Exit Interview Survey.
For each of the following statements, please mark 1 box that best describes your reactions to VIEWER today.

| Strongly disagree | Strongly agree | ||||
|---|---|---|---|---|---|
| 1. I think that I would like to use VIEWER frequently. | 1 | 2 | 3 | 4 | 5 |
| 2. I found VIEWER unnecessarily complex. | 1 | 2 | 3 | 4 | 5 |
| 3. I thought VIEWER was easy to use. | 1 | 2 | 3 | 4 | 5 |
| 4. I think that I would need support of a technical person to be able to use VIEWER. | 1 | 2 | 3 | 4 | 5 |
| 5. I found the varios functions in VIEWER were well integrated. | 1 | 2 | 3 | 4 | 5 |
| 6. I thought there was too much inconsistency in VIEWER. | 1 | 2 | 3 | 4 | 5 |
| 7. I would imagine that most people would learn to use VIEWER very quickly. | 1 | 2 | 3 | 4 | 5 |
| 8. I found VIEWER very cumbersome (awkward) to use. | 1 | 2 | 3 | 4 | 5 |
| 9 I felt very confident using VIEWER. | 1 | 2 | 3 | 4 | 5 |
| 10. I needed to learn a lot of things before I could get going with VIEWER. | 1 | 2 | 3 | 4 | 5 |
VIEWER = Virtual Ward Incorporating Electronic Wearables.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support was provided by affiliates at the Chronic Disease Innovation Centre and partners at Enhancing Quality of Life.