
Abstract
Background:
A growing number of mobile applications (apps) target people with chronic illness as the primary user. There is increasing evidence that digital technology can improve health outcomes for users but the sheer number of apps available is likely to overwhelm many potential users.
Objective:
The purpose of this study was to systematically search for apps aimed at people with chronic kidney disease. An important secondary objective was to develop a search strategy that could be used to identify similar apps in the future.
Design:
A systematic review of the scientific and gray literature including app stores, clearinghouses, and Google.
Setting/patients:
The focus of this research was the identification of apps that may be of use to people interested in self-management of chronic kidney disease.
Methods:
Three reviewers independently searched app stores, websites, and databases to identify apps of potential interest and any information related to the function and efficacy of these. Apps that met the inclusion criteria were short-listed, reviewed in more detail, and cross-referenced with other sources such as clearinghouses, Google, and kidney care organizations. A population, intervention, comparison, outcome, and design framework was used to search selected databases.
Results:
Of the 1464 apps purporting to be for chronic kidney disease, only 15 were eligible for inclusion. Searching the 2 major app stores (iOS and Android) appeared to be the most productive way of identifying apps of potential interest. An increasing number of public and private clearinghouses have been established to assist users with finding apps. Privacy and security of user information is a particular and valid concern of health care professionals and organizations.
Limitations:
The breadth and depth of information relating to each app varied and made it difficult to systematize the evaluation of apps. Due to the large number of health care apps and the challenges to searching app stores and websites, it is possible that some apps were missed during our searches. Similarly, while there are many kidney care–related websites that contain useful information, these were not captured by our study.
Conclusion:
There are very few available apps aimed specifically at people with chronic kidney disease; those that are available are best identified by manually searching the 2 major app stores. Privacy and confidentiality of user information when using the apps is a concern among health care providers in particular.
What was known before
Mobile health is a burgeoning industry with tremendous potential to improve self-management in people with chronic kidney disease (CKD). Identifying apps that may be of interest to this patient population is challenging. This is partly due to the huge number of apps available, and also because, in many instances, it is not possible to assess the function, quality, and usability of the app from the limited information available from the developers. In addition, at present, there is no requirement for health apps to be scientifically based, certified, or regulated. This poses a risk that consumers may choose apps that are clinically unsuitable and potentially harmful.
What this adds
This study provides a qualitative description of the challenges to identifying apps that may be of interest to patients with CKD. It confirms that information, such as the scientific basis, the provenance, usability, and efficacy of the apps available, is largely absent. This study includes suggestions of how busy professionals can search for apps efficiently and identifies some of the barriers to providers adopting or endorsing apps that could benefit patients as well as their organization. It concludes with suggestions of how health care providers and information technology (IT) companies could work together to reduce some of the barriers to the adoption of app technology.
Introduction
Mobile health (mHealth) in the form of applications (apps) designed to be used on devices such as smartphones and tablets is a vast and growing industry, with more than 318 000 apps available globally in 2017. 1 Although most of these apps relate to general well-being such as diet and fitness, an increasing number now focus on chronic disease management. 1 There is high demand for app technology that reflects a wider, general end-user interest in apps-as-services. Given the complexities associated with delivering effective health care, patients are likely to benefit from the personalized, real-time, interactive, and geo-located technology associated with some of these apps. However, with so many health apps available, choosing those that are most useful can be overwhelming for consumers. 2
Provider interest in the use of apps to promote patient engagement and positive health outcomes is increasing, but several pertinent barriers to their effective use persist, not least the lack of scientific evidence on the acceptability, usefulness, and impact of these apps.3-5 Similarly, there is no requirement for apps to be scientifically based, registered, or certified. 3 Finally, for many of these apps, there is no information regarding ease of use, efficacy, or value for money. 4 In the absence of any guidance from their health care providers, patients may be at risk of choosing apps that are clinically inappropriate.
The purpose of this review was to systematically identify apps targeted at people with chronic kidney disease (CKD) including those requiring maintenance dialysis and especially those apps that promote or support self-management. A secondary objective was to describe the search strategy used to identify these apps, which may be used in future by consumers or health care professionals who are seeking to identify potentially relevant apps for people with CKD. Our intention was to include evaluations of identified apps using secondary data from searches of the scientific and gray literature.
Methods
Identifying Apps
Search strategy (See Figure1)

Overview of app screening and selection.
Inclusion criteria
Apps were screened using our eligibility criteria, including the target population, country of origin, language, and function (Table 1).
Population and Intervention-Related Eligibility Criteria for Apps Related to Advanced CKD.

Note. CKD = chronic kidney disease.
Exclusion criteria
We excluded apps that did not primarily focus on CKD and/or its management, and those intended for use by clinicians only (Table 1). Apps that did not provide an English-language user interface were also excluded.
Primary sources
The following sources were searched to identify eligible apps (Supplementary Table 1):
1. App Stores: Google play, iTunes, and Amazon
Two researchers (R.A.L. and C.C.) independently searched Google Play, iTunes, and Amazon using the terms “chronic kidney disease” and/or “dialysis.”
2. Clearinghouses
A number of clearinghouses identified in a previous review 5 were searched using the terms “chronic kidney disease” and/or “dialysis.” An additional number of clearinghouses were identified from our Google search.
3. Kidney care organization websites
R.A.L. searched websites of leading kidney care organizations in Canada, the United States, the United Kingdom, and Australia, for reference to apps.
4. Scientific/academic databases
M.L. searched Medline, OVID, and PubMed Central using keywords and medical subject headings (MeSH) based on the population and intervention.
Additional sources
Two researchers (R.A.L. and C.C.) independently searched Google to identify websites that referenced apps for use by people with CKD. The search term “chronic kidney disease and/or dialysis and app” was used to identify additional apps and clearinghouses not already identified. To keep the search yield manageable, only the first 10 pages of results were reviewed. A “snowballing” process was used to identify further apps, including references of these study reports. Google was also used to cross-reference apps not found in the main app stores.
Describing Apps
Where available, details on the purpose, cost, country of production, year, developer, endorsements, privacy, security, and date of last update were collected from each eligible app.
Results
App Identification
The app sources were searched and included app stores (Supplementary Table 2), clearinghouses (Supplementary Table 4), kidney care organizations (Supplementary Table 4), scientific literature (Supplementary Table 6), and Google (Supplementary Table 5). App names were screened and included or excluded based on the eligibility criteria (Table 1). Apps meeting the criteria were further screened using the developer’s description. This was done through the 2 main apps stores (Table 2) as the other sources searched all referenced either or both of these for download. The Amazon app store listed a small number of apps (n = 9), those relevant were also listed in the 2 main stores. Of the 1464 apps screened at this stage, 360 were available in the app stores. Those not specific to CKD and its management (n = 152) or those intended for provider use only (n = 102) were excluded. Other exclusions included apps not written in English (n = 56), apps not applicable to the patient populations in North America, Western Europe and Australia and duplicates. A short list of 15 apps were identified as possibly of use to people with CKD (Table 3).
Review of Initial Short List From App Stores (iTunes = 16, Google Play = 21, Amazon = 0).
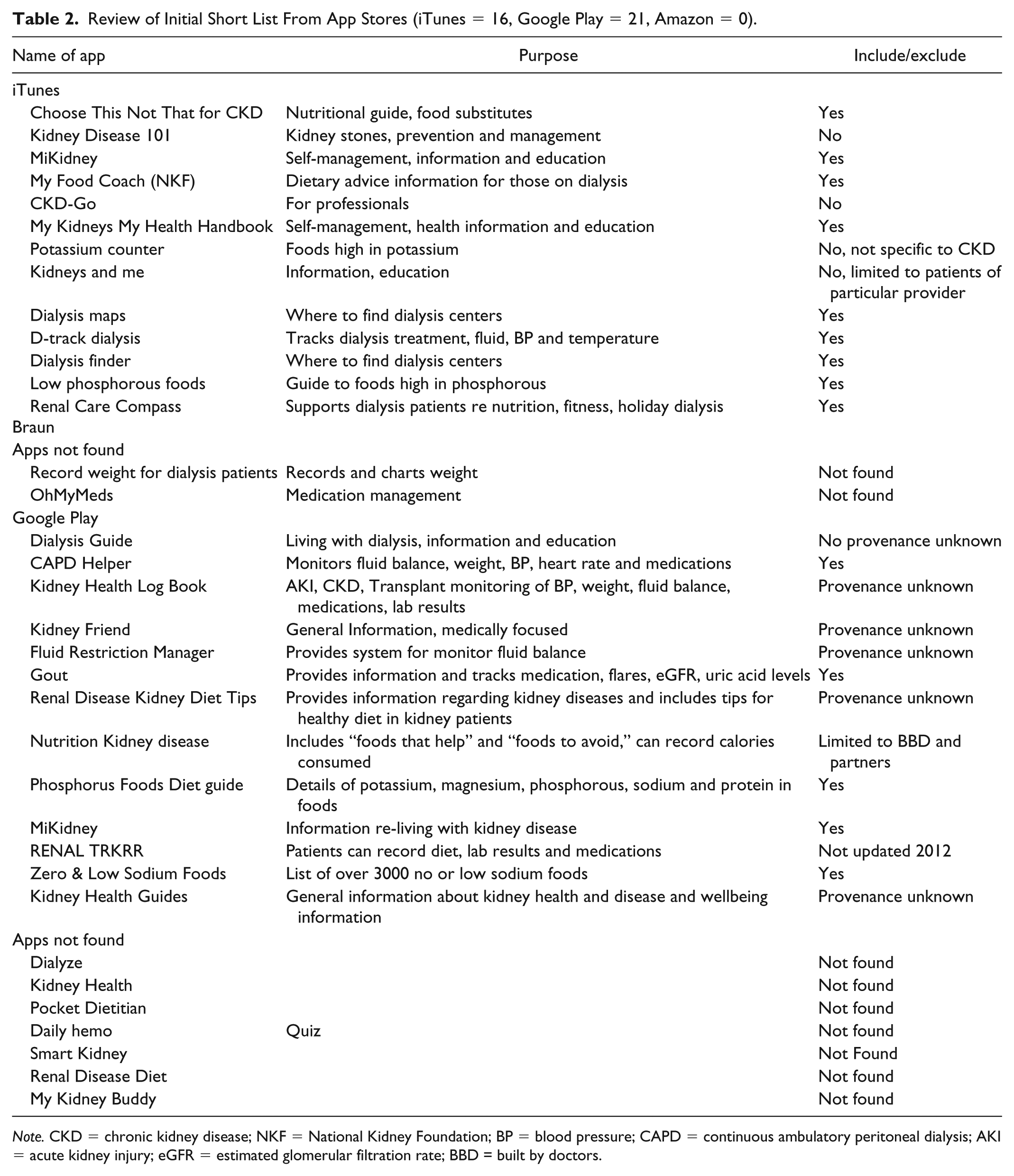
Note. CKD = chronic kidney disease; NKF = National Kidney Foundation; BP = blood pressure; CAPD = continuous ambulatory peritoneal dialysis; AKI = acute kidney injury; eGFR = estimated glomerular filtration rate; BBD = built by doctors.
Final Short List of Apps That May Be of Use to People With CKD (All Sources).
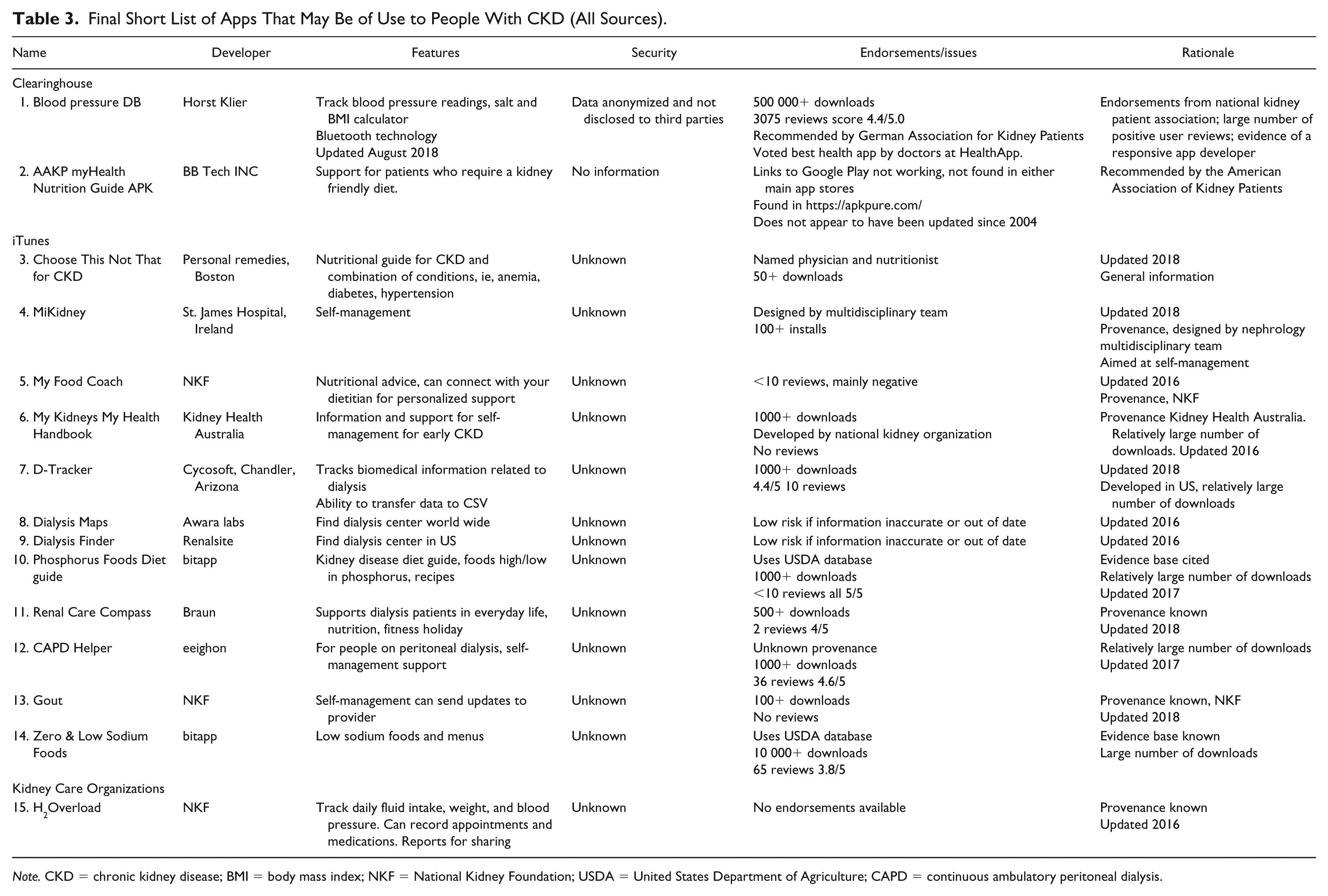
Note. CKD = chronic kidney disease; BMI = body mass index; NKF = National Kidney Foundation; USDA = United States Department of Agriculture; CAPD = continuous ambulatory peritoneal dialysis.
Of the 15 short-listed apps, 4 supported self-management (MiKidney, My Kidneys, My Health Handbook, Renal Care Compass, and CAPD Helper). Two were health trackers, whereby patients could record measures of interest such as fluid intake, blood pressure and weight as well as medications and clinic appointments (D-Tracker and H2Overload). Five apps were aimed at nutritional support; of these, 3 were general dietary guides for people with CKD (Choose This Not That, My Food Coach, and myHealth Nutrition Guide) and 2 focused on common dietary restrictions in CKD, sodium (Zero & Low Sodium Foods) and phosphorous (Phosphorus Foods Diet guide). Two apps were guides to finding dialysis centers away from home, one in the United States (Dialysis Finder) and another worldwide (Dialysis Maps). Two apps aimed to assist patients in managing hypertension (Blood pressure DB) and gout (Gout). Apps not specific to CKD, for instance, “Zero & Low Sodium Foods,” were included if they were endorsed by a kidney care organization.
A number of strategies6-9 have been suggested for evaluating the quality of health-related apps. However, the information relating to individual apps is largely limited to the descriptions offered in the app stores and is generally insufficient to execute the suggested evaluation strategies. Although information regarding the function, aesthetics, and usability of the app can be obtained from using the app, details related to the accuracy of information, the provenance of the supporting evidence base, and the security and privacy of the apps are generally absent. Consequently, in choosing apps to include in our final list, it was necessary to compromise on some aspects of the evaluation criteria for individual apps and to use a combination of proxy measures of eligibility where possible (Table 3). These included the number of downloads and positive reviews (Google Play only), those endorsed by or developed with care providers or kidney care organizations, and those that referenced credible evidence sources. Most of the apps were typically inexpensive (<$10) or free, although some included advertisements and in-app purchases, which some users found annoying.
Developing a Search Strategy
Identifying potentially relevant apps proved challenging, largely due to the arbitrary cataloging of apps in the 2 main app stores and the absence of mechanisms to allow for more targeted searches. Apps are often listed due to popularity with the indexing determined by developers who, keen to attract consumers from a broad interest base, use a number of general descriptors such as “kidney” which can encompass a large range of apps unrelated to CKD. Searches using more specific terms, such as “chronic disease management,” did not significantly reduce the number of apps unrelated to our purpose, and in some instances, excluded them. Similarly, knowing the exact name of an app did not necessarily locate it in the stores. Other search problems included not being able to use a computer (but only an iOS device) to search iTunes and the limited information contained in the developers’ descriptions on which to evaluate the apps. iTunes does not publish the number of downloads and often cites a lack of ratings and reviews to be able to provide a summary. This was the case in the iTunes listing of the Blood Pressure BD app. In contrast, Google Play cited more than 3000 reviews for the same app.
Clearinghouses
Clearinghouses (Supplementary Table 3) were identified from the literature, 5 from searching Google and from reviewing information technology (IT) health media publications such as Health IT (https://hitconsultant.net/), mobilehealthnews (https://www.mobihealthnews.com/), and Healthcare Informatics (https://www.healthcare-informatics.com/). Although generally an efficient way for potential users to access app summaries and systematic evaluations, the quality of the information is dependent upon the methods used by the clearinghouses and these are not always readily available or transparent.
Some clearinghouses such as appcrawlr (http://appcrawlr.com) provide the number of user reviews and compare these with those of other apps they consider similar; in practice, these comparisons are not always accurate or helpful. In their evaluation of the “Kidney Diet” app (136 reviews), the comparators included a “Calorie counter by FatSecret” app (220 000 reviews) and “Lose Weight without Dieting” app. In contrast, AppScript (https://www.iqvia.com/) scores apps according to functionality, peer and patient reviews, certifications, and their potential to improve care outcomes and/or reduce health care costs. 1 Across these 6 dimensions, 70 metrics are weighted and aggregated providing a score of 1 to 100. What constitutes a good score can vary according to the condition, the patient, and the discretion of the health care provider. At the time of writing, there were no apps for CKD listed in AppScript. Other websites, such as imedicalapps (https://www.imedicalapps.com/), are limited to health care professionals and did not include any relevant apps.
Some health care providers, usually in collaboration with an IT company, are developing their own clearinghouses. RxUniverse (http://www.rxuniverse.com/) is a multiplatform application developed in partnership with Mount Sinai hospital in New York. It allows health care providers to prescribe apps from a curated formulary and can deliver digital health to their patients’ smartphone during their consult (http://www.rxuniverse.com/). Although this is likely to be a prototype, on the basis of their initial success, they have partnered with a start-up company to license other health care systems to use their platform. In many instances, access to the information on these sites is proprietary. Other academic, nonprofit, and government organizations such as the National Health Service (https://apps.beta.nhs.uk/), the Federal Drug Administration (https://www.fda.gov/medicaldevices/digitalhealth/), and the University of Florida (https://diabetes.ufl.edu/) also provide information and endorsements on a number of health-related apps. The identification of apps through the clearinghouses was limited; this was presumed to be because of the smaller target population in relation to more prevalent conditions such as mental health and behavioral problems, diabetes, and heart and circulatory systems.
Scientific literature
A search of selected databases using our Patient/Population/Problem, Intervention Comparison and Outcome (PICO) framework (Table 1) produced 61 articles. Four articles from other sources were identified. After removing duplicates and reading the titles and abstracts, 10 articles were retrieved for review (Supplementary Table 6), leading to the identification of several apps that may have been of use. None of these were available in the app stores.
Discussion
We aimed to identify apps focusing on people with CKD and to develop a search and evaluation strategy that would assist consumers and health care professionals in finding such apps in future. Although we successfully identified a limited number of potentially useful apps, we encountered several challenges, including the relatively low number of apps for people with CKD, how apps are cataloged and listed in the app stores, determining the provenance of some apps, and locating the evidence base. In addition, while the initial intention was to evaluate the identified apps using published data, it was not possible to do this systematically or comprehensively as the information available was typically limited and varied between different apps and operating systems. While there is increasing recognition that mHealth can potentially benefit patients and care organizations, 10 some apps may be clinically unsuitable and possibly unsafe. In addition, major barriers to the use of apps persist, namely, the lack of interoperability with existing patient data systems and the privacy and security of user information. 11 In response to these barriers, an increasing number of hospitals and health care organizations are adopting or developing their own digital platforms.
Challenges to the Identification of Apps
In 2017, there were 325 000 health care apps available, 12 the volume alone makes identifying apps that are clinically relevant a challenge to those in practice. 13 In the area of clinically specific apps, CKD accounts for only 1% of the total number of available apps. This contrasts with apps for use in mental health and behavioral disorders (28%), which have the highest proportion of clinically related apps. 1 Irrespective of the therapeutic area of interest, the cataloging and indexing of apps in the stores makes it difficult to identify less popular apps 5 even using specific terms such as the app’s title. Potential users are required to trawl through several hundred apps, many of which are not relevant. Although time-consuming, and probably not feasible for busy clinicians, at present, this seems to be the best way to initially identify apps. IQVIA’s AppScript 1 is probably the most evidence-based clearinghouse publicly available. However, at the time of this study, we did not identify any eligible apps focused on CKD in the AppScript clearinghouse.
In general, traditional methods of searching the academic literature were time-consuming and not an effective method for identifying apps focused on CKD. Although these searches did identify a small number of apps that may have been of interest, none were available in the app stores. Searching academic databases was useful in identifying research and reviews of digital health, and although many of these were unrelated to CKD, they provided useful insights into strategies for reviewing and evaluating health-related apps. A more productive method of sourcing mHealth information proved to be via a growing number of digital news platforms including mHealth Intelligence (https://mhealthintelligence.com), med-technews (https://www.med-technews.com), and mobihealthnews (https://www.mobihealthnews.com). These include a wide range of information and news from health care apps and devices to research, regulation, governance, and clinical practice.
Provider Perspectives
Patients are increasingly turning to providers to recommend potentially useful apps—and although health care professionals are generally supportive of digital health, adoption into their practice is low. IQVIA’s research suggests that only 26% of clinicians currently recommend patient engagement apps and these are typically limited to general well-being and prevention. 1 In their study of health care professionals’ reluctance to engage with technology, concerns about data overload, quality, and reliability were identified. 14 At present, there are also a number of practical considerations related to poor interoperability with existing patient data systems. A number of the apps identified during this research cited an ability to share information with providers. In practice, the format of app data is often not immediately compatible with existing health care systems and does not always meet provider regulations regarding its transfer and use: “[t]o sift that data and bring it into an EHR, you need infrastructure too big for a small provider . . . in a big hospital, there’s too much red tape, privacy issues and other barriers” (pp. 24-25). 11
The privacy and data security of health-related apps is a potential concern for health care professionals and organizations. 15 In their analysis of the 20 most popular health-related apps, researchers found that the majority of those reviewed did not adhere to accepted privacy and security practices and guidelines, or even the legal requirements included in the data protection regulations. 10 Similarly, in 2017, the Journal of the American Medical Association reviewed the privacy policies of Android apps used in diabetes. Of the 271 apps identified, 211 were included in their sample, the majority of which (81%) had no privacy policy. Of those that did have a privacy policy (n = 24), most (n = 19) had shared user information with a third party. 16 At present, there appears to be no federal legislation preventing the disclosure or sale of data from an app to a third party in Canada. In 2016, the European Union (EU) drafted a “Code of Conduct on privacy for mobile health applications,” and the EU has recommended that app developers reference these guidelines to ensure adherence to data protection standards and principles. 10
The Future of mHealth
There is growing interest from clinicians and health care organizations in working with digital companies (and vice versa) to develop and produce customized health-related apps specifically for their clinical staff and patient populations. 17 This is likely to ensure health-related apps are evidence based and more suited to patient and provider needs 11 with appropriate oversight and governance of their uptake, usage privacy, and security. Similarly, health care organizations and networks are adopting their own vetting and curation systems 18 to make it easier for clinicians to identify and recommend apps for their patients. The identification and evaluation of health-related apps for a particular purpose could be a group effort, commissioned through either a service improvement team or a health care system. It is possible that this could be done through existing organizations with a common interest, such as kidney care, whereby the costs and benefits are shared through an electronic repository of curated mhealth resources.
Limitations
Despite the small number of apps available for people with CKD, executing our search required us to review a large volume of information from several sources, much of which was not relevant to our study. Similarly, while we recognized that a number of apps were potentially of use to people with CKD, we did not feel able to fully endorse any individual apps without further qualification. The breadth and depth of information relating to each app varied and made it difficult to systematize the evaluation of apps. A number of clearing houses (notably AppScript) have extensive resources with which to access information on which to base their evaluation of apps, including trial data. While searching the app stores is the most productive way for potential users to identify apps, it is labor-intensive and unlikely to be practical for busy clinicians. In addition, we found the listing of apps varied almost on a day-to-day basis, which made systematizing searches of the app stores difficult. Most of the scientific literature was outdated compared with the rapid pace of technical change and the digital health literature. Due to the large number of websites related to health care apps, it is possible that some apps were missed during our searches. Similarly, while there are many kidney care–related websites that contain useful information, these were not captured by our study.
Further research is required to evaluate the quality, efficacy, and usability of apps that may be of use to people interested in CKD. This would require patients with CKD and specialist providers to download and use the apps and give feedback with reference to the core values in health care. 5
Conclusion
MHealth has tremendous potential to improve outcomes for both patients and health care organizations, but there are valid concerns regarding the identification, efficacy, evidence base, privacy, and security of apps. Partnerships between patients, health care providers, the digital industry, and other stakeholders to develop relevant apps and/or curated registries might help to ensure a pipeline of more patient-centered apps that mitigate some of the identified privacy and security issues.
Supplemental Material
Supplementary_Tables_App_manuscript_05112018 – Supplemental material for Identifying Mobile Applications Aimed at Self-Management in People With Chronic Kidney Disease
Supplemental material, Supplementary_Tables_App_manuscript_05112018 for Identifying Mobile Applications Aimed at Self-Management in People With Chronic Kidney Disease by Rachel A. Lewis, Meaghan Lunney, Christy Chong and Marcello Tonelli in Canadian Journal of Kidney Health and Disease
Footnotes
Ethics Approval and Consent to Participate
This study has been approved by the Conjoint Health Research Ethics Board (CHREB) at the University of Calgary. Informed consent was obtained from all those who participated in this research.
Consent for Publication
All authors consent to the publication of this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: While no external funding was provided for this study, the authors are financially supported by the generosity of the Alberta Kidney Disease Network.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.