
Abstract
Purpose of Program:
Our team co-developed My Kidneys My Health, an online platform designed with patients with non-dialysis-dependent chronic kidney disease and care partners to provide tailored education and self-management support. While My Kidneys My Health has seen increased use and positive user feedback since its development and launch in 2021, there are opportunities to improve its cultural relevance, accessibility, and usefulness for diverse populations. In this report, we describe our approach to addressing these elements by adapting My Kidneys My Health content and knowledge mobilization strategies.
Sources of Information:
Patients and care partners in Canada have identified the lack of accessible, person-centered resources as a major barrier to effective self-management for non-dialysis-dependent chronic kidney disease. Digital heath tools can meet this need by delivering consistent, evidence-based education and support in a user-friendly format. Through our program of research with Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease (Can-SOLVE CKD), we have co-developed My Kidneys My Health through a series of patient-oriented research studies.
Methods:
Our program objectives are to (1) understand and address gaps in sexual health support for individuals with non-dialysis-dependent chronic kidney disease; (2) build relationships with Indigenous communities in Alberta to understand and share self-management learnings; and (3) improve accessibility to My Kidneys My Health content for diverse populations. To guide the adaptation and implementation of My Kidneys My Health, our team adopted the following Can-SOLVE CKD phase 2 pillars: (1) Implementation Science and Knowledge Mobilization, (2) Indigenous Cultural Competency, (3) Incorporation of Equity, Diversity, and Inclusion principles in Knowledge Mobilization and Implementation Efforts, and (4) Patient Engagement and Capacity Building. We used the Can-SOLVE CKD Pathway to Implementation and applied the Map2Adapt framework.
Key Findings:
Primary care and nephrology providers expressed readiness to integrate My Kidneys My Health into clinical workflows, and collaborative partnerships with initiatives like Kidney Check enhanced knowledge sharing. We initiated relationship building with the Stoney Nakoda Tsuut’ina Tribal Council Ltd. Health Department (G4 Health), including in-person meetings with the health directors, and co-development of engagement packages and communications designed to reflect our culturally safe methodologies. We addressed accessibility barriers by updating website features and new printable materials on key self-management topics, with French translations. Results from our mixed methods sexual health study underscored the need for tailored, credible resources for people with non-dialysis-dependent chronic kidney disease. Findings from our ongoing environmental scan will inform a sexual health resource inventory for integration into My Kidneys My Health. Patient partners reported meaningful involvement that shaped project priorities, design, and knowledge mobilization.
Limitations:
Significant time and resources are required to support meaningful Indigenous engagement, which contributed to delays in the project timeline. In Alberta, we have had ongoing healthcare restructuring disrupting relationship building with key decision-makers and creating uncertainty around partner roles. Finally, a permanent solution to accommodate and maintain My Kidneys My Health will be needed after the research is completed.
Implications:
Our work exemplifies an integrated, patient-oriented approach that emphasizes implementation science, equity, cultural competency, and capacity-building. As we move forward, our focus will remain on enhancing accessibility, relevance, and sustainability to ensure that all people living with non-dialysis-dependent chronic kidney disease can access trusted, evidence-based support to live well with kidney disease.
Background
Inappropriate management of early-stage chronic kidney disease (CKD), particularly in individuals with multiple chronic conditions, can lead to adverse short- and long-term outcomes, including a higher risk of dialysis initiation and kidney transplantation. 1 These outcomes carry significant personal consequences for patients and place considerable strain on the healthcare system. 2 Self-management strategies can slow chronic disease progression; however, many patients face considerable barriers to engaging in self-management practices. 1
Patients and their care partners across Canada have identified a significant gap in self-management support for individuals living with non-dialysis-dependent CKD, emphasizing the need for resources that are tailored to each person’s unique circumstances, priorities, and preferences.1,3 Evidence-based eHealth tools present a valuable opportunity to address these needs while also reducing the risks associated with inconsistent or nonstandardized health information. The development of these tools aligns closely with the commitment of the Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease (Can-SOLVE CKD) Network, 4 particularly its commitment to person-centered care and meaningful patient partnership.
Our team developed My Kidneys My Health (MKMH; https://mykidneysmyhealth.com/), an evidence-informed, co-designed website that delivers tailored education and self-management support for individuals living with CKD and their care partners. The website also serves as a tool for health care providers in their role in providing educational resources. To date, MKMH has reached more than 16 000 users internationally and is widely recognized for enhancing patient self-efficacy and providing positive user experiences. All MKMH content is grounded in current, evidence-based clinical practice guidelines, including those from Kidney Disease Improving Global Outcomes (KDIGO) Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease,
5
Canadian Cardiovascular Society,6,7 Diabetes Canada,
8
and Hypertension Canada9,10:
The website provides valuable tools for patients that are diagnosed [with chronic kidney disease] and offers a safe space and community to those who share this experience. It is a valuable resource of information about the self-management of CKD and making better decisions about lifestyle choices. It is relevant, accessible, and speaks about what I need as a patient with kidney disease. Being a patient with CKD is important to leave a legacy for others.
—Patient Partner (MDe)
In the evolving era of virtual care, MKMH serves as a timely and relevant tool to complement multidisciplinary CKD care. However, to ensure its continued relevance and sustainability, content accessibility and implementation challenges must be addressed. For example, when MKMH was initially developed, there was a lack of evidence and resources on topics such as sexual health. Additionally, the platform could be strengthened by improving its cultural competency, particularly in recognizing and integrating traditional ways of health and well-being. To address these gaps, we are systematically adapting MKMH content and knowledge mobilization strategies. Our goal is to enhance the platform’s accessibility, cultural relevance, and reach. Specifically, our objectives are to
Understand and address gaps to sexual health support for individuals with nondialysis CKD;
Build relationships with Indigenous communities in Alberta to understand and share self-management learnings; and
Improve accessibility to MKMH content for diverse populations.
To guide the adaptation and implementation of MKMH, our team adopted the 4 Can-SOLVE CKD phase 2 pillars: (1) Implementation Science and Knowledge Mobilization; (2) Indigenous Cultural Competency; (3) Incorporation of Equity, Diversity, and Inclusion (EDI) principles in Knowledge Mobilization and Implementation Efforts; and (4) Patient Engagement and Capacity Building. We continuously engage with a diverse team of researchers, program leads, people with lived experience, clinicians, administrators, and our software developer (Tactica Interactive, https://tactica.ca/). In the following sections we outline our approaches and outcomes related to each of these pillars.
Pillar 1: Implementation Science / Knowledge Mobilization
Approach
The initial co-development of MKMH was guided by the Knowledge-to-Action (KTA) Framework 11 and the Can-SOLVE CKD Pathway to Implementation Guide 12 using a person-centered, theory-informed approach. The MKMH was co-created in direct response to a clearly identified patient need for accessible, evidence-informed self-management tools.1,13 -17 Knowledge mobilization has been a central focus throughout the project, led by the Dissemination Working Group, a multidisciplinary group with strong representation from patient partners. This group provides strategic guidance on dissemination activities, including identifying presentation opportunities and developing educational materials. Their work is informed by both their lived experience and user engagement data from Google Analytics, reviewed during meetings held quarterly. To ensure the ongoing accuracy and quality of the website content, our team developed and applied a novel content validation checklist. This tool systematically tracks the validity of information and supports the maintenance of high-quality, evidence-based content. It was created by team members (S.J., S.G., G.C.) and applied annually to identify and update relevant content and functionality.
We have completed steps 1 to 5 of the Can-SOLVE CKD Pathway to Implementation (awareness, readiness, team establishment, launch, and evaluation) during our first phase of funding (phase 1).1,13 -17 Our current focus is on step 6: Planning for Sustainability (Figure 1), with an emphasis on tailoring content to underrepresented groups, expanding reach, and ensuring long-term integration into clinical workflows. The overarching goal was to enhance accessibility, cultural relevance, and long-term sustainability of MKMH by scaling its use across nephrology and primary care and adapting it to meet the diverse needs of patients with non-dialysis-dependent CKD in Canada. We have also aligned our efforts with other Can-SOLVE CKD initiatives, including Kidney Check 18 and APPROACH, 19 to streamline and enhance collaborations with Indigenous communities.
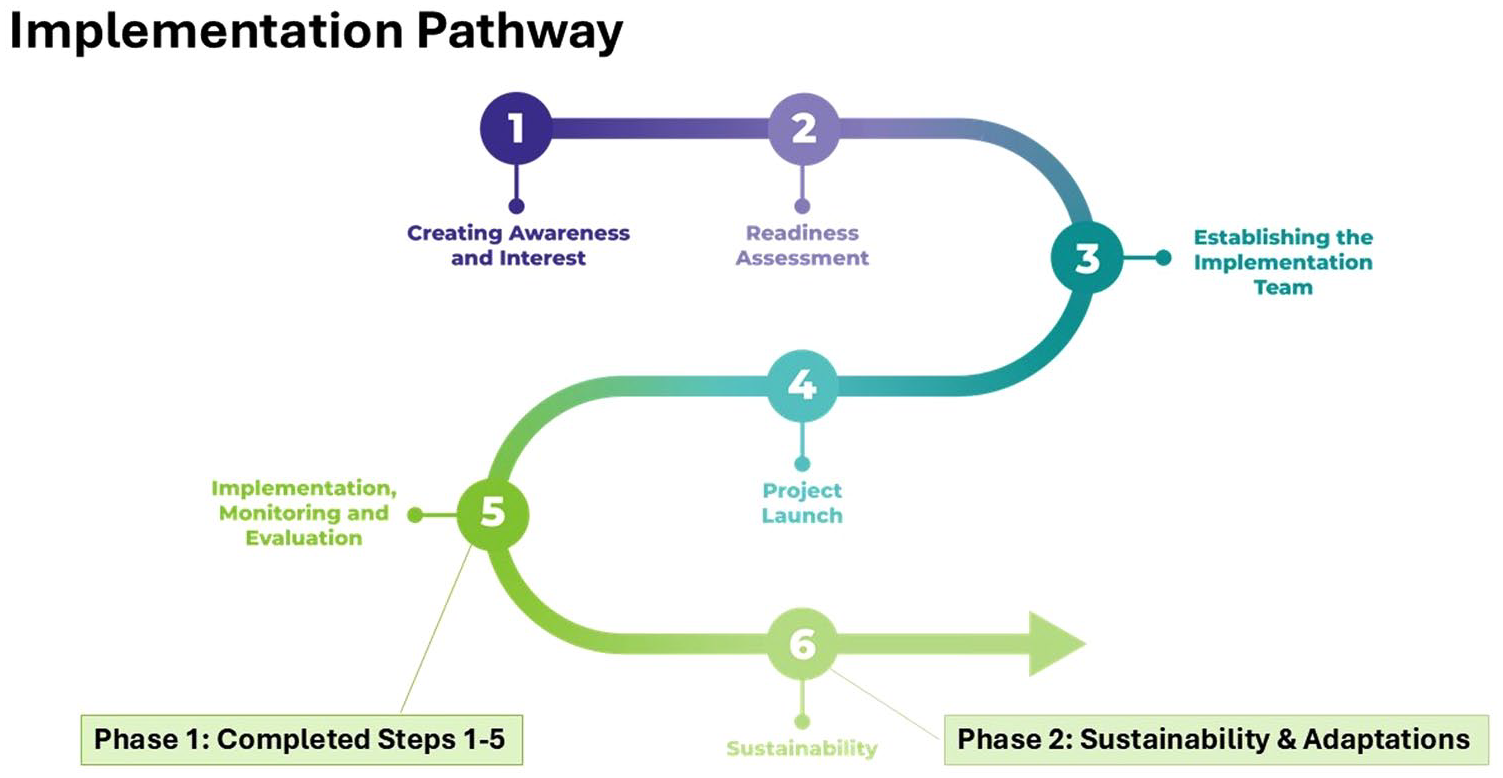
My Kidneys My Health implementation journey using the Can-SOLVE CKD pathway to implementation. 12
We applied the Map2Adapt framework 20 (Figure 2) to systematically guide adaptations of MKMH, connecting to pillars 2 and 3 (Indigenous Cultural Competency and Incorporation of EDI principles in Knowledge Mobilization and Implementation Efforts). To evaluate the perceived value and impact of these adaptations, we will use the Reach, Effectiveness, Adoption, Implementation, and Measurement (RE-AIM) framework. 21 Key partners supporting this work include the Alberta SPOR SUPPORT Unit and the Kidney Foundation of Canada. Target knowledge-user audiences include health care providers, patients, administrators, researchers, charitable and funding organizations (eg, Kidney Foundation of Canada), and the public. To support broad dissemination and uptake, we are developing interactive toolkits and information packages tailored to diverse care settings.

Map2Adapt framework. 20
To address the gap in evaluating the effectiveness of self-management interventions in CKD, the CKD Self-Management (CKD-SM) Questionnaire was developed during the platform’s co-design activities (phase 1). This tool underwent initial psychometric testing, and a graduate trainee is currently leading further validation efforts. This work will support future research into the impact of MKMH and other interventions on self-management outcomes.
Outcomes
Initial testing of MKMH has demonstrated that the website is feasible, relevant, and adds value to CKD self-management, showing support for patient self-efficacy and improved care experiences (approved by the University of Calgary’s Conjoint Health Research Ethics Board [CHREB], REB20-0152).
3
Furthermore, health care providers in primary care and nephrology spaces expressed readiness to incorporate MKMH into clinical practice in our implementation study (approved by CHREB, REB21-0930).
22
Collaborating with other Can-SOLVE CKD projects, such as Kidney Check, enhances the knowledge dissemination of MKMH with diverse populations and Indigenous communities to expand its reach and impact: My Kidneys My Health is a significant milestone that has already been achieved. I see all the projects under Can-SOLVE as one. The goal is the same, that’s the reason why I’m looking forward to working together. We have some communities that we are planning to engage, we should partner whenever we go into these communities—we go together. Kidney Check screens for kidney disease and now this information on how you live with kidney disease is a huge opportunity. The degree of alignment between the two activities is great. I think we should leverage it. —Nephrologist-Researcher: Kidney Check (A.B.)
Barriers to implementation of MKMH included awareness, memory, time, motivation, and digital accessibility. 22 In response, we piloted implementation strategies to address these barriers, which were highly utilized by health care providers and received positive feedback. Based on these results and the 4 Can-SOLVE CKD pillars, we entered phase 2 with a focus on the sustainability of MKMH. This phase has involved identifying opportunities for adaptations both to the MKMH website and our broader implementation approach. This has supported our transition into step 6: Planning for Sustainability of the Can-SOLVE CKD Pathway to Implementation. 12
Pillar 2: Indigenous Cultural Competency
Approach
To support the culturally safe adaptation and implementation of MKMH, we embraced a relational and reciprocal approach grounded in the 6Rs Framework (Respect, Relevance, Reciprocity, Responsibility, Reflection, Relationships) to foster meaningful engagement with Indigenous communities. 23 This approach was further informed by Indigenous Research Methodologies, 24 prioritizing community leadership, trust-building, and mutual benefit.
We have established relationships with several key partners who brought valuable perspectives and expertise. These include community partners such as Alberta Health Services’ Indigenous Wellness Core and local health directors, research experts from the University of Calgary’s Indigenous Research Support Team (IRST), and engagement liaisons from the Can-SOLVE CKD Indigenous Peoples’ Engagement and Research Council (IPERC). 25 These collaborators supported our team in co-creating a respectful, community-informed engagement strategy rooted in trust, reciprocity, and cultural safety.
We built a culturally grounded team by welcoming an Indigenous patient partner (M.L.) and a Knowledge Keeper (V.M.) as co-leads in the engagement planning process, and an Indigenous Liaison Manager to support the process (C.T.). Together, we co-developed a research protocol titled Establishing authentic engagement with Indigenous communities in Alberta to explore perspectives on kidney wellness: relationship building and co-development of a research protocol (approved by CHREB, REB22-1794). Our team also engaged in ongoing cultural safety education, including San’yas Indigenous Cultural Safety training, OCAP training and continued mentorship from the Can-SOLVE CKD Indigenous Engagement team: We promote respect and empowerment for Indigenous people and ways of knowing by strengthening our sacred ways of being. We’re building relationships with clinicians, doctors, and settlers and teaching proper protocol in relation to learning from and with indigenous patient partners. Rather than the matters of the disease consuming my health, CKD has become the connection and change that has allowed me to share the facts with my family and all my relations throughout Turtle Island. —Patient Partner (M.L.)
Outcomes
Through sustained collaboration with our Indigenous Patient Partner (M.L.), Knowledge Keeper (V.M.), and local First Nation’s Health Manager, we initiated relationship-building with the Stoney Nakoda Tsuut’ina Tribal Council Ltd. Health Department (G4 Health) for the G4 Nations (Bearspaw, Chiniki, Goodstoney & Tsuut’ina). This included 2 in-person meetings with health directors, the co-development of engagement packages, and tailored communications (eg, speaker notes, team biographies, 1-pagers) designed to reflect the 6Rs of Indigenous engagement.
We have also aligned our efforts with other Can-SOLVE CKD initiatives, including Kidney Check and APPROACH, to ensure our work complements and supports other Indigenous-led Can-SOLVE CKD projects. Our team presented its engagement approach at the NorthWest SPOR Collaborative Forum alongside C.T., M.L., and V.M., highlighting the importance of cultural safety and sustained relationship-building. To illustrate and keep record of our continued Indigenous engagement connections, we created an Indigenous Network Map, shown in a simplified version in Figure 3.
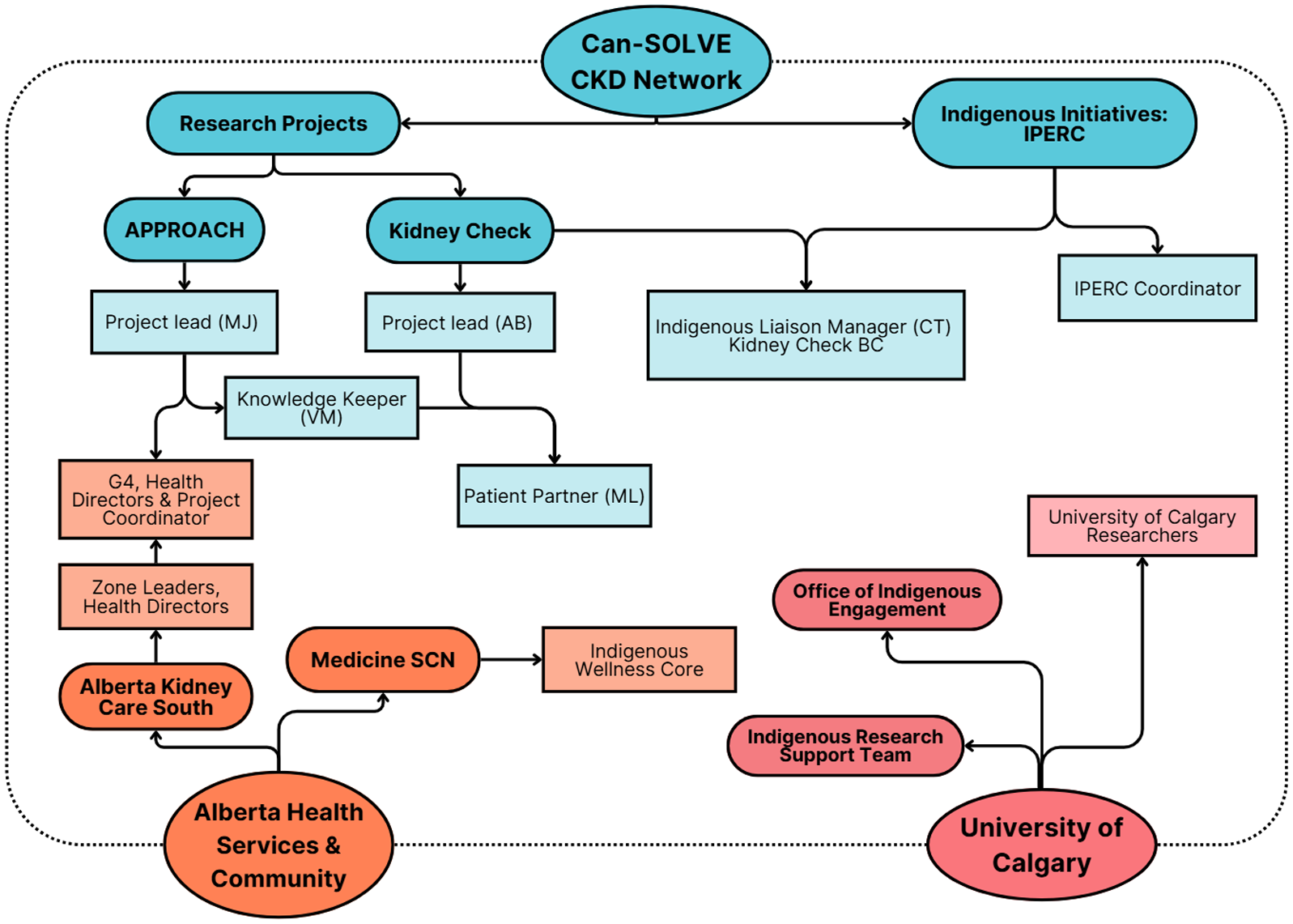
Indigenous engagement network map.
Pillar 3: Incorporation of EDI principles in Knowledge Mobilization and Implementation Efforts
Approach
To improve the relevance, accessibility, and sustainability of MKMH, we intentionally integrated EDI principles throughout our implementation planning and knowledge mobilization efforts. These efforts focused on addressing the needs of underserved populations—particularly Indigenous communities, those facing accessibility barriers, and individuals with sexual health concerns. Our goal is to reduce inequities in self-management support and ensure that all individuals with non-dialysis-dependent CKD can benefit from MKMH.
To address accessibility, we reviewed MKMH content and dissemination strategies, identifying areas for improvement. Feedback from our implementation study revealed challenges to integrating the website into practice, such as limited access to computers, time constraints, lack of translated resources, and navigation barriers. 22 In response, the Dissemination Working Group identified and are addressing the following: underutilized areas of the website, plain language revisions, content to be printable, and translation of priority topics into other languages. For example, we are developing printable materials that summarize key self-management topics and translating these resources into French.
To understand the patient-identified priority of sexual health, we conducted a sequential mixed methods study (approved by CHREB, REB23-0272), including a national provider survey and qualitative interviews to explore barriers and opportunities for integrating sexual health into nondialysis CKD care. Our sexual health study incorporated equity, diversity, inclusion, and accessibility into various research activities, including recruitment, wording, inclusivity of survey questions, and demographic categories. In collaboration with experts in this area (S.D., C.M.), and patient partners (K.A., D.S.), we also analyzed data to understand how provider perspectives varied across sex and professional identity. In addition, we are conducting an environmental scan of online sexual health resources available for patients and health care providers to identify relevant resources and evaluate their quality, accessibility, and content.
Outcomes
In terms of improving accessibility, based on results from our implementation study and Google Analytics data, we have made several key updates to the MKMH platform to enhance its usability for diverse users, including patients, care partners, and health care providers. These include targeted updates to improve accessibility and usability of the MKMH website (https://mykidneysmyhealth.com/), such as a redesign of the My Questions List feature to enhance functionality and user experience, as well as the creation of a new Resources page to improve content visibility and navigation. In response to feedback from patients and health care providers about technology access and information retention, we also co-developed printable 1-page summaries on key self-management topics such as sodium intake and medications. French translations are currently underway to further improve accessibility.
Our mixed methods study revealed a clear disconnect between the recognized importance of sexual health discussions in kidney care and its limited integration into clinical practice, with barriers including time constraints, lack of training, and provider discomfort. This work underscored the need for accessible, credible sexual health tools tailored to CKD care. 19 As previously mentioned, we are completing an environmental scan to identify and evaluate the credibility of online resources for patients and health care providers. Our findings will contribute to a resource inventory for patients and health care providers to access as part of CKD care, and this inventory will inform future content development and integration into MKMH.
In addition to content improvements, we conducted a comprehensive review of the website for clinical and design updates in collaboration with Tactica and the Dissemination Working Group. From April 1, 2024, to March 31, 2025, MKMH had approximately 6000 unique users and 21 051 page views, with most users located in Alberta and increased uptake in Ontario, British Columbia, Quebec, and Nova Scotia. Tool usage has also increased, with higher engagement with interactive features such as the My Questions List, PDF downloads, and dietary planning tools.
Pillar 4: Patient Engagement and Capacity Building
Approach
Patient partnership has been central to every stage of this project, with meaningful contributions from 7 patient partners (B.P., K.A., L.F., M.De., M.L., N.V., V.M.) and 1 patient partner project co-lead (D.S.). These individuals bring diverse perspectives across geography, age, disease stage, ethnicity, and caregiving experiences. Patient partners were intentionally embedded across all project objectives, ensuring that implementation strategies remained grounded in lived experience and fostering long-term capacity for patient-oriented research. All patient partners continue to contribute to the Dissemination Working Group, where they played a key role in advising and shaping the MKMH website content, such as the My Questions List and Resources page, and in guiding dissemination strategies. They also regularly participate in Self-Management Project Team Meetings, where they offer feedback on project directions and deliverables, and support the refinement of protocols, manuscripts, posters, and reports.
Outcomes
This project has involved a high level of patient engagement throughout all stages, from priority setting to knowledge mobilization. As a result, MKMH content was designed to be highly relevant to its primary audience. Patient partners have reported that the trainings they were offered have better equipped them to contribute meaningfully to the research project and have consistently stated that they feel their voices have been heard and played a strong role in guiding this research project. Our work continues to be strengthened by strong patient engagement and empowerment. Several patient partners also took on leadership and specialized roles:
D.S. (co-lead) and N.V. completed formal training in patient-oriented research, including the San’yas Indigenous Cultural Safety course and the TCI Implementation Course.
M.L. and V.M. co-lead Indigenous engagement activities, co-developed outreach materials, liaise with community partners, and presented project learnings at national conferences, including the NorthWest SPOR Collaborative Forum (2023, Edmonton) and the Indigenous Wellness Conference (2024, Calgary).
K.A. contributed to data interpretation for the sexual health care provider survey study.
B.P. and D.S. provide ongoing review and feedback on newsletters and patient-facing resources, helping to refine project communications:
One of the most disheartening aspects of being a patient partner in kidney research is when the role feels symbolic rather than truly meaningful. Fortunately, that was not the case with the My Kidneys, My Health project. The research team went above and beyond to engage patient partners in every stage of the research cycle. From setting project priorities to shaping the website’s content and design, they consistently relied on patient input. My Kidneys, My Health was truly created by patients, for patients. Being part of this project reminded me why patient partnership matters — and what it can achieve when done right. —Patient Partner (D.S.)
Discussion
Supporting people with CKD through better self-management tools can improve decision-making, quality of life, and care experiences, particularly when those tools are tailored to meet the needs of diverse populations. Our effort in phase 2 addresses longstanding gaps in CKD care and sets a precedent for inclusive implementation. Our achievements to date are highlighted in Figure 4. To support widespread dissemination of our project findings, we have shared results at local, national, and international conferences through 33 poster or oral presentations (eg, Canadian Society of Nephrology Annual General Meetings, University of Calgary’s Roy and Vi Baay Chair events, and NorthWest SPOR Collaborative Forums). We have also completed 22 presentations to diverse audiences, including patients, care partners, healthcare providers, and decisions makers.

Summary implementation outcomes for MKMH aligned with the 4 pillars of the Can-SOLVE CKD phase 2 pillars.
In addition to the 10 manuscripts published in phase 1 of our work, we continue to build the knowledge base for self-management through several new publications, including a published scoping review on peer support in the American Journal of Kidney Disease, 26 a multi-methods study on the implementation of MKMH (pre-print), 22 and a mixed methods sexual health study (in submission). 27 Additional publications, including the environmental scan of sexual health resources, are currently in development. Findings from our mixed methods study on sexual health and ongoing environmental scan are directly informing the integration of evidence-based sexual health content into MKMH. These adaptations will be designed to improve patient-provider communication and ensure that sexual health is recognized as a critical component of patient wellbeing and chronic disease care.
Team and Partner Engagement
Our team’s approach to respectful engagement with Indigenous communities, guided by Indigenous Research Methodologies and co-developed ethics protocols, offers a model for culturally safe health research. These approaches demonstrate that time, reciprocity, and shared leadership are essential for building authentic and sustainable partnerships.
Patient partners have been embedded throughout every phase of the project. From identifying priorities and shaping MKMH content, to guiding implementation and sustainability efforts, they have rooted the project in lived experience. Their leadership and insight have profoundly shaped the direction, tone, and impact of this work. They have enabled continued progress of the project, with the aim of improving the experience of patients and care partners at the center of each step. They have strengthened the quality of our work and continue to provide direction and leadership on how to continue to improve and sustain MKMH: Being a patient partner in the My Kidneys My Health website development project has been and continues to be very rewarding. The team dynamic has always been respectful, inclusive and collegial and everyone’s contributions have been recognized and appreciated. I would highly recommend that anyone interested in “making a difference” to the health of Canadians, consider becoming a patient partner. —Patient Partner (BP)
Regular team engagement is maintained through biannual newsletters, full-team meetings, Dissemination Working Group meetings, and periodic email check-ins to share updates and maintain momentum. Collaborations with experts in sexual health and kidney disease (C.M.), and Indigenous liaisons (S.B.), have further strengthened the cultural safety and relevance of our work. These partnerships contributed to the relevance, depth, and cultural safety of our approach.
Challenges
One of the primary challenges is the significant time and resources required to support meaningful Indigenous engagement, which contributed to delays in the project timeline. To address this, we revised the scope of engagement through collaborative discussions with community leads, extended our timelines, and intentionally involved patient partners in planning activities. We also re-engaged with collaborators from aligned Can-SOLVE CKD projects such as Kidney Check and APPROACH to ensure coordinated efforts and resource sharing.
Ongoing healthcare restructuring in Alberta posed another obstacle, disrupting relationship-building with key decision-makers and creating uncertainty around partner roles. Despite this, we maintained communication with the health authority and adapted our plans as organizational roles evolved to preserve continuity and momentum.
Finally, our focus is ensuring the sustainability and longevity of MKMH to ensure relevant and credible content is easily accessible to patients, care partners, and healthcare providers. As such, we are currently exploring alternative website hosting platforms and are conscious of the need for a permanent solution to accommodate MKMH.
Conclusion
The ongoing adaptation and implementation of MKMH reinforces the importance of long-term, collaborative partnerships to support sustainable change in CKD self-management. Continued engagement with patient partners, Indigenous communities, and national organizations such as the Kidney Foundation of Canada will be critical to enhancing the website and integrating it into clinical and community settings. Guided by the Can-SOLVE CKD 4 pillars, our work exemplifies an integrated, patient-oriented approach that emphasizes implementation science, equity, cultural competency, and capacity-building. As we move forward, our focus remains on enhancing accessibility, relevance, and sustainability to ensure that all people living with nondialysis CKD can access trusted, evidence-based support to live well with kidney disease.
Supplemental Material
sj-pdf-1-cjk-10.1177_20543581251370922 – Supplemental material for Adapting a Self-Management Tool (My Kidneys My Health) to Meet the Needs of Diverse Canadian Populations: Program Report
Supplemental material, sj-pdf-1-cjk-10.1177_20543581251370922 for Adapting a Self-Management Tool (My Kidneys My Health) to Meet the Needs of Diverse Canadian Populations: Program Report by Maoliosa Donald, Sabrina Jassemi, Shannan Love, Gillian Crysdale, Dwight Sparkes, Maria Delgado, Laurinda Ferreira, Betty Pearson, Nancy Verdin, Kaitlin Ahrenholz, Violet March, Maureena Loth, Sarah Gil, Heather Beanlands, Aminu Bello, Sandra Dumanski, Janine Farragher, Lori Harwood, Allison Jaure, Joanne Kappel, Ellen Novak, Sharon Straus, Catherine Turner, Clare McKeaveney, Brenda R. Hemmelgarn and Meghan J. Elliott in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
University of Calgary’s Institutional Indigenous Engagement Office, Roy and Vi Baay Chair, Nephrology Research Group, Alberta SPOR SUPPORT Unit, CKD Clinic Network, Kidney Foundation of Canada, Alberta’s Medicine Strategic Clinical Network, and Tactica Interactive.
We thank the patients, care partners, and health care providers who participated in our research studies.
Ethics Approval and Consent to Participate
The University of Calgary’s Conjoint Health Research Ethics Board (CHREB) provided approval for this series of studies discussed in the manuscript (Ethics IDs: REB20-0152, REB21-0930, REB22-1794, REB23-0272).
Consent for Publication
The authors have consented to the publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is a project of the Canadians Seeking Solutions and Innovations to Overcome; Chronic Kidney Disease (Can-SOLVE CKD) Network, funded by the Canadian Institutes of Health Research (CIHR) under Canada’s SPOR grant (KMI-18189). The funding organizations had no role in the design and conduct of the study; data collection, analysis, and interpretation; or preparation, review, or approval of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.