
Abstract
Background:
Acute kidney injury (AKI) in critically ill children is associated with increased risk for short- and long-term adverse outcomes. Currently, there is no systematic follow-up for children who develop AKI in intensive care unit (ICU).
Objective:
This study aimed to assess variation regarding management, perceived importance, and follow-up of AKI in the ICU setting within and between healthcare professional (HCP) groups.
Design:
Anonymous, cross-sectional, web-based surveys were administered nationally to Canadian pediatric nephrologists, pediatric intensive care unit (PICU) physicians, and PICU nurses, via professional listservs.
Setting:
All Canadian pediatric nephrologists, PICU physicians, and nurses treating children in the ICU were eligible for the survey.
Patients:
N/A.
Measurements:
Surveys included multiple choice and Likert scale questions on current practice related to AKI management and long-term follow-up, including institutional and personal practice approaches, and perceived importance of AKI severity with different outcomes.
Methods:
Descriptive statistics were performed. Categorical responses were compared using Chi-square or Fisher’s exact tests; Likert scale results were compared using Mann-Whitney and Kruskal-Wallis tests.
Results:
Surveys were completed by 34/64 (53%) pediatric nephrologists, 46/113 (41%) PICU physicians, and 82 PICU nurses (response rate unknown). Over 65% of providers reported hemodialysis to be prescribed by nephrology; a mix of nephrology, ICU, or a shared nephrology-ICU model was reported responsible for peritoneal dialysis and continuous renal replacement therapy (CRRT). Severe hyperkalemia was the most important renal replacement therapy (RRT) indication for both nephrologists and PICU physicians (Likert scale from 0 [not important] to 10 [most important]; median = 10, 10, respectively). Nephrologists reported a lower threshold of AKI for increased mortality risk; 38% believed stage 2 AKI was the minimum compared to 17% of PICU physicians and 14% of nurses. Nephrologists were more likely than PICU physicians and nurses to recommend long-term follow-up for patients who develop any AKI during ICU stay (Likert scale from 0 [none] to 10 [all patients]; mean=6.0, 3.8, 3.7, respectively) (P < .05).
Limitations:
Responses from all eligible HCPs in the country could not obtained. There may be differences in opinions between HCPs that completed the survey compared to those that did not. Additionally, the cross-sectional design of our study may not adequately reflect changes in guidelines and knowledge since survey completion, although no specific guidelines have been released in Canada since survey dissemination.
Conclusions:
Canadian HCP groups have variable perspectives on pediatric AKI management and follow-up. Understanding practice patterns and perspectives will help optimize pediatric AKI follow-up guideline implementation.
Introduction
Understanding of acute kidney injury (AKI) in children has rapidly evolved over the past 10 years. 1 In 2012, the Kidney Disease Improving Global Outcomes (KDIGO) organization unified previous definitions of AKI into a single diagnostic standard for adults and children. 2 The development of a consensus definition for AKI allowed for comparative studies and enhanced our knowledge of incidence, outcomes, and risk factors for AKI in children. 2 AKI is a common complication in hospitalized children 2 and even more common in the pediatric intensive care unit (PICU). Kaddourah et al 3 found that the overall rates of AKI and severe AKI (KDIGO stage 2 or 3) during the first week of PICU admission were 27% and 12%, respectively. AKI is known to be associated with poor hospital outcomes among critically ill children, 4 including increased mortality rate, longer length of stay, and prolonged mechanical ventilation. 5 Acute kidney injury has also been shown to be an independent risk factor for chronic kidney disease (CKD) and kidney replacement therapy (KRT) in adults. 6
The association of pediatric AKI with long-term kidney outcomes is unclear, but current evidence suggests that children admitted to the PICU with stage 2 or worse AKI are at a higher risk for developing CKD or hypertension within 7 years after hospital discharge.7 -11 Collectively, these data suggest that critically ill children who develop AKI, particularly those with more severe AKI, should be monitored for long-term complications. The KDIGO guideline proposes that patients with AKI during a hospitalization should be followed beginning at 3 months after discharge to evaluate for resolution of AKI and potential development of permanent kidney complications.12,13 However, recommendations in children, and the extent to which children with AKI are followed for long-term complication developments remain unclear.
As the understanding of pediatric AKI outcomes continues to evolve, it is important to begin translating recent knowledge into practice. Acute kidney injury is a complex disorder mostly affecting patients with non-primary kidney disorders. 14 Critically ill children with AKI are commonly cared for by a broad scope of healthcare providers during the acute phase of illness (e.g., nephrologists, PICU physicians and nurses) whose beliefs and perspectives about AKI are likely to impact how AKI is managed and what type of follow-up, if any, will be instituted. In order to inform on development and implementation of pediatric-specific AKI management and follow-up guidelines, which also consider current entrenched practices and beliefs, it is vital to investigate the current perspectives and knowledge base of the healthcare providers involved.
This study aims to identify evidence-practice gaps in pediatric AKI by surveying Canadian pediatric nephrologists, PICU physicians, and PICU nurses on AKI management, perceived importance of AKI as a long-term risk factor for adverse kidney outcomes, and AKI follow-up recommendations. We hypothesized that significant variation exists in reported AKI management and beliefs, within and between healthcare professional (HCP) groups.
Materials and Methods
Study Design and Survey Development
We distributed a national, cross-sectional, anonymous, web-based survey to 3 provider groups in Canada: (1) pediatric nephrologists, (2) PICU physicians, and (3) PICU nurses. Individuals treating infants, children and adolescents less than 18 years old in an ICU setting were eligible to participate in the survey. Providers who only treat adults or neonates (<1 month old) were not eligible.
Three initial survey drafts (one for each participant group) were developed and then reviewed and edited by members of the Pediatrics Committee of the Can-SOLVE CKD Network (a national nephrology research network). 15 Three PICU physicians, and two PICU nurses additionally provided feedback on face validity. After several rounds of revisions, each survey was piloted by 1 or 2 providers in each target group to evaluate completion time, flow, and ease of administration. Final survey drafts were reviewed and finalized by two study team members. The nephrologist version was developed first and evaluated as above first; as this survey was disseminated and analyzed, the PICU physician and nurse versions were developed and evaluated. Ethics board approval was granted by the SickKids Research Ethics Board. Consent was presumed based on agreement to participate in the survey.
Survey Contents
Surveys included 58 to 77 items (Supplemental Content), depending on the provider-specific version. The survey was broken into 4 sections: (1) demographics (e.g., region of practice; years of practice) and center data (e.g., estimated admissions per year; presence of electronic medical record (EMR) information); (2) questions regarding renal replacement therapy (RRT) and diuretics (AKI management in the PICU setting); (3) perceptions of AKI importance; and (4) AKI follow-up practices. Questions in Section 4 directly asked providers’ opinions on which AKI patients in the PICU should be followed up and which long-term kidney outcomes are most important to ascertain. Within surveys, we utilized KDIGO definitions to stage AKI (e.g., explicitly defining Stage 1 AKI as 50% serum creatinine (SCr) rise from baseline and providing an example [50 μmol/L rising to 75 μmol/L, not requiring dialysis]).
Questions were presented in closed response format, including categorical measurements (yes, no, I don’t know, and “different answer” [for AKI practice and knowledge questions]) or on a 10-point Likert scale (ranging from not important at all to most important; not likely at all to definitely). All 3 versions were designed to be extremely similar in form and content but adapted to provider groups. Surveys contained HCP-specific questions as deemed appropriate (i.e., only PICU physicians and PICU nurses were asked to report the number of yearly ICU admissions at their center). Slight wording differences were based on feedback from the specialty-specific providers described above.
Survey Dissemination
We initially contacted relevant Canadian stakeholder groups to distribute surveys to members. The pediatric nephrology version of the survey was disseminated through the Canadian Association of Pediatric Nephrologists (CAPN) and administered in electronic format via SurveyMonkeyTM, which was the survey platform available and used by our group at the time. The PICU nurse survey version was disseminated through the Canadian Association of Critical Care Nurses (CACCN); hospital site directors were also contacted to assist in dissemination. Pediatric intensive care unit physicians were emailed directly through an existing and updated email list provided by stakeholders. Pediatric intensive care unit physician and nurse versions of the survey were provided electronically via REDCapTM because this platform became easily available to us and was our (and the primary institution’s) preferred survey platform (more versatile for analysis and modification). Two email reminders were sent 2 weeks apart for each survey version. Survey dissemination details are described in supplementary Figure 1.
Statistical Analysis
Categorical responses were compared between groups using Chi-square or Fisher’s exact tests as appropriate. Likert scale interval variables were compared between and within groups using Mann-Whitney and Kruskal-Wallis tests as appropriate. Within-HCP and between-HCP (e.g., PICU vs. nephrology) group responses were evaluated. Analyses were performed using STATA SE statistical software package (15.1, StataCorp LLC, College Station, TX); p-value <0.05 was considered statistically significant.
Results
Survey Responses
Forty-six of the 64 pediatric nephrologists contacted, responded (supplementary Figure 1); 34 completed the survey (supplementary Figures 1 and 2). Fifty-four of 113 PICU physicians contacted, responded (supplementary Figure 1); 46 completed the survey (supplementary Figures 1 and 2). One hundred thirty-six PICU nurses responded to the survey and 82 completed the survey (supplementary Figures 1 and 2). The response rate for PICU nurses was unknown (supplementary Figure 1).
Provider and Center Characteristics and Practices
Pediatric nephrologist and PICU nurse respondents were represented from 7 of the 10 Canadian provinces; PICU physician respondents were from 8 of 10 provinces. Majority of PICU physicians (70%, 33/47) and PICU nurses (63%, 79/125) reported that their center used an EMR to provide care for ICU patients. No pediatric nephrologists and only 9% (4/47) of PICU physicians reported their unit had an institutional guideline for timing of acute RRT initiation (Table 1). PICU nurse responses on presence of acute RRT initiation guidelines in their unit were 36% (37/102) yes, 29% (30/102) no, and 34% (35/102) reporting they did not know (Table 1).
Provider and Center Characteristics of Survey Respondents.

Note. Abbreviations: PICU = pediatric intensive care unit; ICU = intensive care unit; N/A = not applicable; RRT = renal replacement therapy; AKI = acute kidney injury.
Some respondents did not answer all questions (incomplete), therefore the total number (N) may add up differently depending on the question.
Reported percentages were rounded up, therefore may not total to 100%.
Area of practice categorizes general geographic area of respondents. East includes Manitoba, Ontario, Quebec and Maritime Provinces. West includes British Columbia, Alberta, and Saskatchewan.
N/A refers to not assessed. Those questions were not included in the nephrologist-specific version of the survey.
The majority of pediatric nephrologists (88%, 28/32) and PICU physicians (77%, 34/44) reported that their institution did not have an AKI follow-up guideline or protocol (Table 1). However, 81% (26/32) of pediatric nephrologists reported that their nephrology services had a common practice for arranging post-AKI follow-up of patients in the ICU. Among PICU nurses, 20% (15/76) and 33% (25/76) reported that their ICU did and did not have an AKI follow-up guideline, respectively, and 47% (36/76) reported that they did not know (Table 1).
AKI management
Renal replacement therapy (RRT prescription and type)
Over 65% of all providers reported that only nephrologists were primarily responsible for prescribing and managing acute hemodialysis (HD) (supplementary Figure 3A). The majority of pediatric nephrologists (66%, 23/35) and 42% (41/92) of PICU nurses reported that only nephrologists were primarily responsible for acute peritoneal dialysis (PD) prescription (supplementary Figure 3B). An equal distribution of PICU physicians reported that acute PD was prescribed and managed by the nephrology service (30%, 12/40) vs. the ICU (37.5%, 15/40) vs. both services (32.5%, 31/40) (supplementary Figure 3B).
Regarding continuous renal replacement therapy (CRRT) prescription and management, 43% (15/35) of pediatric nephrologists reported a shared care nephrology-ICU model, but 20% (7/35) reported that the ICU and 34% (12/35) reported the nephrology service were primarily responsible (supplementary Figure 3C). Fifty-nine percent (24/41) of PICU physicians reported that the ICU was primarily responsible; PICU nurses reported that either the ICU (39%, 38/98) or the nephrology service (42%, 41/98) were mostly responsible (supplementary Figure 3C).
Indication for RRT
Severe hyperkalemia (potassium >8 mEq/L) was rated as the most important RRT indication for both nephrologists and PICU physicians (Table 2). Similarly, both nephrology and PICU physicians rated fluid overload, to be more important than severe hypocalcemia with hyperphosphatemia, severe acidosis, or severe protracted oliguria, for RRT initiation decision-making (Table 2). Fluid overload (edema) was significantly more important for decision-making on RRT for pediatric nephrologists compared to PICU physicians (P < .05). Rate of rise in SCr was rated lowest in importance for deciding on acute RRT initiation for both nephrology and PICU physicians (Table 2). Nearly all pediatric nephrologists (97%, 34/35) and PICU physicians (96%, 45/47) indicated that furosemide (Lasix) was their first choice of diuretics for managing fluid overload (edema) or oliguria.
Pediatric Nephrologists’ and PICU Physicians’ Responses Regarding Importance of Various Indications in Decision-Making for Renal Replacement Therapy Initiation Using A 10-Point Likert Scale (0 Being Not Important, 10 Being Most Important).

Note. Abbreviations: PICU = pediatric intensive care unit; mEq/L = milliequivalents per liter.
25th to 75th percentile shown in brackets beside median value. Median responses were calculated and analyzed using Mann Whitney test. A P value <.05 was considered statistically significant and indicated with an asterisk (*). Above questions were not included in the PICU nurse version of the survey.
Importance of acute kidney injury
Nephrology consultation for AKI
Perceived indications for nephrology consultation for AKI varied within and between HCP groups. Forty-three percent of nephrologists (15/35) reported that their ICU requests nephrology consultation if the ICU suspects a need for RRT within the next few days (supplementary Figure 4A). Thirty percent of PICU physicians (14/46) reported that they never consult nephrology for AKI (supplementary Figure 4A). Pediatric intensive care unit nurses responses varied: 18% (15/82) believed they consult nephrology when SCr doubles, 25% (20/82) believed they consult nephrology if they suspect that the patient may require RRT in the next few days, and 34% (28/82) responded they did not know (supplementary Figure 4A). Supplementary Figure 4B contrasts beliefs and what was reported to be done, in terms of nephrology consultation. Nephrologists believed their ICU should consider consultation with nephrology at earlier stages of AKI (supplementary Figure 4B). The majority of pediatric nephrologists (24/34, 71%) believed that by the time they receive a consultation request for AKI from the ICU, there are some patients on whom they should have been consulted earlier.
AKI association with hospital outcomes
There was discordance and variation regarding the minimum AKI severity threshold which contributes to increased risk of poor hospital outcomes. The majority of PICU physicians (26/46, 57%) and PICU nurses (37/82, 45%) believed that severe AKI requiring acute RRT is the minimum AKI threshold for increased risk of PICU mortality (Figure 1A). However, an equal distribution of nephrologists reported believing that the minimum threshold for increased PICU mortality risk was either stage 2 AKI or severe AKI requiring acute RRT (Figure 1A). The majority of nephrologists (18/34, 52%) believed that stage 2 AKI was the minimum threshold for risk of longer PICU stay (Figure 1B); PICU physician responses for this question were distributed across the spectrum of AKI severity (Figure 1B). PICU nurse responses on minimum AKI threshold association with longer PICU stay were skewed toward more severe AKI, but a large proportion reported uncertainty (do not know) (Figure 1B). Pediatric nephrologists and PICU physicians believed that more severe AKI (stage 2 or worse) was the minimum AKI severity threshold associated with longer invasive ventilation, with nephrologists’ responses skewing more toward stage 2 AKI, compared to PICU physicians (Figure 1C). PICU nurses believed that more severe AKI requiring RRT was most strongly associated with prolonged invasive ventilation; again many were uncertain (responding do not know) (Figure 1C).

Pediatric nephrologists,’ PICU physicians’ and PICU nurses’ beliefs regarding the minimum acute kidney injury (AKI) severity that independently contributes to increased risk for (A) PICU mortality, (B) longer PICU stay, and (C) prolonged invasive mechanical ventilation.
Acute kidney injury follow-up
Perceptions on need for AKI follow-up
HCP beliefs on who should be followed up for possible long-term kidney dysfunction varied within and between groups, especially for patients with early-stage AKI (Figure 2). Most HCPs reported believing that patients with stage 1 AKI do not require follow-up for long-term kidney dysfunction (Figure 2A). However, the proportion of PICU nurses (26%, 20/76) believing that patients with stage 1 AKI require follow-up was significantly higher compared to PICU physicians (7%, 3/44) (Figure 2A, P < .05). Majority of pediatric nephrologists and PICU nurses believed that patients with stage 2 AKI require long-term follow-up; PICU physicians’ beliefs were equally distributed between for and against need for follow-up of stage 2 AKI (Figure 2B). The majority of HCPs believed that patients with stage 3 AKI should be followed up for long-term kidney dysfunction (Figure 2C); nearly all HCPs believed that patients requiring RRT should be followed up (Figure 2D).
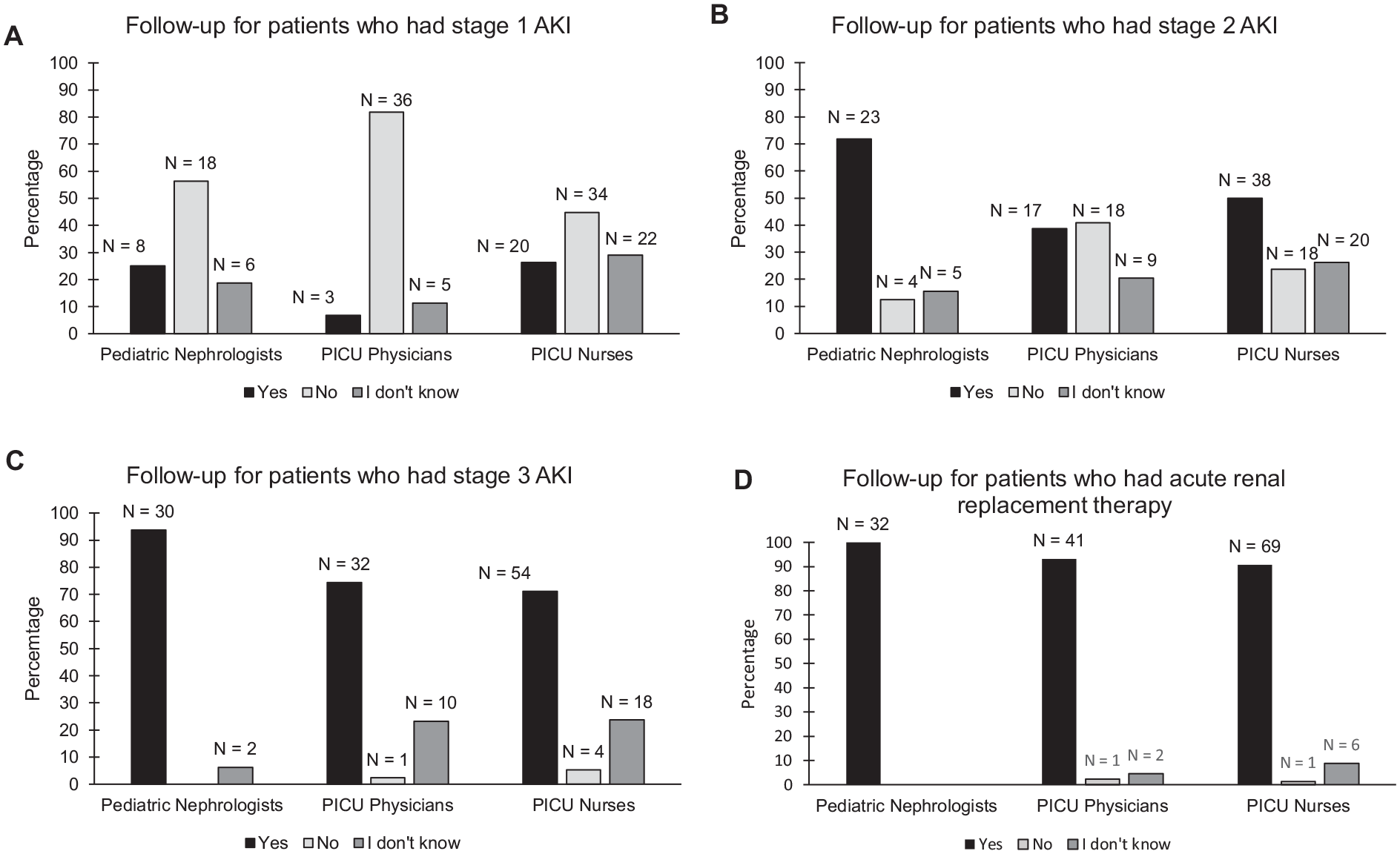
Pediatric nephrologists,’ PICU physicians,’ and PICU nurses’ acute kidney injury (AKI) follow-up beliefs for patients who had (A) stage 1 acute AKI, (B) stage 2 AKI, (C) stage 3 AKI, and (D) acute renal replacement therapy (dialysis).
Organizing and performing AKI follow-up
Pediatric nephrologists’ beliefs on who would be most effective at organizing post-AKI follow-up of kidney function after discharge varied; 31% (10/32), 50% (16/32), and 16% (5/32) believed the ICU, the nephrology service or other HCPs, respectively, would be most effective (supplementary Figure 5). Most PICU physicians (82%, 36/44) and PICU nurses (70%, 53/76), believed that the nephrology service would be most effective at organizing long-term follow-up after AKI (supplementary Figure 5).
Pediatric nephrologists’ perspectives on which HCP types should perform follow-up for long-term kidney dysfunction varied with AKI severity (supplementary Figure 6A). For patients with stage 1 AKI, 60% (6/10) and 40% (4/10) believed nephrologists and general practitioners, respectively, should follow these patients long-term (supplementary Figure 6A). All nephrologists agreed that patients requiring RRT should be followed up by a nephrologist (supplementary Figure 6A). There was substantial variation in nephrologists’ perspectives on the duration of long-term follow-up required for patients with AKI (supplementary Figure 6B). Most nephrologists believed that patients with severe AKI (stage 3 or requiring RRT) should be followed up for life (supplementary Figure 6B).
Regarding follow-up of patients whose kidney function returns to normal by hospital discharge, all nephrologists agreed that some of these patients require long-term follow-up. However, 41% (18/44) of PICU physicians and 51% (39/76) of PICU nurses believed that these patients do not need specific follow-up.
AKI associations with long-term kidney outcomes
In general, nephrologists and PICU physicians agreed on the potential long-term kidney outcomes or CKD measures which were important to detect (Table 3). Both HCP groups ranked in increasing order of importance estimated glomerular filtration rate (eGFR) <90 mL/min/1.73 m2 (least important to detect), followed by mild proteinuria/microalbuminuria, eGFR <60 mL/min/1.73 m2, long-term hypertension, and chronic dialysis (Table 3). On average, nephrologists rated all outcomes, except for chronic dialysis, to be more important to detect, compared to PICU physicians (P < .05, Table 3).
Pediatric Nephrologists’ and PICU Physicians’ Responses Regarding Importance of Monitoring and Detecting Potential Long-Term Kidney Outcomes or Measures of Chronic Kidney Disease Using A 10-Point Likert Scale (0 Being Not Important, 10 Being Most Important).

Note. Abbreviations: PICU = ediatric intensive care unit; eGFR = estimated glomerular filtration rate; mL = milliliter; min = minute; m2 = square metre.
25th to 75th percentile shown in brackets beside median value. Median responses are calculated and analyzed using Mann Whitney test. A P value <.05 was considered statistically significant and indicated with an asterisk (*). Above questions were not included in the PICU nurse version of the survey.
Regarding what to inform families of children with AKI, nephrologists reported that they are more likely to inform families that post-AKI long-term follow-up is required for all levels of AKI severity, compared to PICU physicians and PICU nurses (P < .05, Table 4). Pediatric intensive care unit physicians indicated they were more likely to inform families of need for follow-up than PICU nurses, for almost all levels of AKI severity (P < .05, Table 4). Pediatric nephrologists were significantly more likely to report informing patients of need for long-term follow-up, if they required RRT, compared to PICU physicians (P < .05, Table 4).
Pediatric Nephrologists,’ PICU Physicians, and PICU Nurses’ Responses Regarding Likelihood in Current Practice to Inform A Family That They Should Have Follow-Up of Their Long-Term Renal Function Using A 10-Point Likert Scale (0 Being Not Likely at All, 10 Being Definitely).

Note. Abbreviations: PICU =ediatric intensive care unit; AKI = acute kidney injury; RRT = renal replacement therapy.
25th to 75th percentile shown in brackets beside median value. Median responses are calculated and analyzed using Kruskal Wallis equality of populations rank test. A P value <.05 was considered statistically significant and indicated with an asterisk (*).
Discussion
To our knowledge, this is the first study utilizing a national survey to assess the multi-dimensional perspectives of different healthcare providers that commonly treat children with AKI in the PICU. Overall, our survey demonstrated widespread variation in RRT initiation indication, perceived importance of AKI as it relates to long term complications, and recommended AKI follow-up.
We found differences in opinions regarding relevant factors for deciding on RRT initiation between nephrologists and PICU physicians that could be explained by the lack of institutional guidelines for timing of acute RRT. Both HCP groups agreed that severe hyperkalemia was the most important indication. However, nephrologists rated hyperkalemia, severe hyperkalemia, and fluid overload higher in terms of importance in decision-making than PICU physicians. Standardized RRT guidelines may be beneficial to begin evaluating the role of early RRT initiation on impacting outcomes in critically ill children, particularly with severe sepsis or multiorgan dysfunction early in PICU admission.16,17 Future research and implementation science should attempt to harmonize fluid and RRT management of AKI across healthcare provider stakeholders with a goal of optimizing outcomes and unifying care processes.
Our survey identified contrasting beliefs concerning nephrology consultation for AKI. Most PICU physicians reported that they either never consulted nephrology for AKI or only consulted if they believed the patient required RRT soon. A significant number of PICU nurses also reported that they did not know when nephrology should be consulted for AKI. However, majority of nephrologists reported that some of the ICU consults they received for AKI in the past should have been conducted earlier, highlighting the need to further consolidate AKI management between HCP groups. Early consults with nephrology have shown potential benefit by lowering risk of progression to AKI stage 3 through interventions such as early fluid adjustment. 18 Hospitals may consider implementing an AKI alert system using existing EMR infrastructure to generate automated consultations with the nephrology division, which has shown to be associated with improved rate of recovery from AKI. 19 Ultimately, these findings also suggested that the role of the nephrologist in assisting in the care of children with AKI when RRT is not required, is unclear to other healthcare providers. Future research should study this, together with evaluation of care bundles or clinical pathways in patients developing varying levels of AKI severity.
HCPs differed in their beliefs about the association between AKI and the hospital outcomes we queried, taken directly from the literature. In general, nephrologists believed the association between AKI (especially early-stage AKI) and hospital outcomes was stronger than PICU physicians and nurses. A significant proportion of PICU nurses reported they did not know if there was an association between AKI and hospital outcomes despite existing literature identifying AKI as an independent risk factor for PICU mortality, longer length of stay, and prolonged mechanical ventilation in critically ill children.4,5 AKI in children admitted to the PICU has been shown to be associated with a two-fold longer PICU stay, and a mortality rate tenfold higher in AKI than non-AKI patients. 20 In order to improve interdisciplinary care, future knowledge translation efforts should focus on raising awareness and educating PICU providers on adverse outcomes associated with AKI.
The study also revealed significant differences in AKI follow-up beliefs between providers. Almost all agreed that patients with severe AKI (stage 3 or requiring RRT) needed to be followed up. However, respondent answers varied for patients with early-stage AKI (stage 1 or 2), highlighting existing knowledge gaps regarding the long-term outcomes of these patients. Our survey revealed opposing AKI follow-up perspectives in patients whose kidney function returns to normal at ICU discharge. Nephrologists believed that patients with AKI, but with normal kidney function at discharge, should still be followed up, whereas many PICU practitioners disagree. This discrepancy highlights the need for future research to examine whether these patients are truly at risk for long-term kidney dysfunction in order to propose evidence-based guidelines to aid in decision- making. Moreover, more detailed study on which degree of AKI severity is most likely to be associated with later kidney or other outcomes, followed by knowledge translation of these findings, should be performed. Such data will provide HCP the data needed to make decisions for their own patients and for institutions/systems to justify resources required to ensure appropriate long-term AKI follow-up.
Our study has several limitations. The use of different survey platforms for the nephrologist vs. the two PICU versions of the survey might have potentially affected how responses were provided, simply by having a different visual appearance. However, we believe that this issue had a minor effect as most questions required only a selection and both platforms allowed for completion on computer or phone. We had a lower response rate from PICU physicians and were unable to calculate a response rate for PICU nurses; the number of PICU nurses notified and eligible for our survey was unknown. However, the respondents spanned at least 7 of the 10 provinces in Canada. Therefore, we believe our respondents are representative of the spectrum of healthcare providers we were interested in surveying as there are no pediatric nephrology departments in New Brunswick, PEI, and Newfoundland and Labrador. Additionally, information from all eligible HCPs in the country was not obtained; there may be differences in opinions on AKI between providers that completed the survey and those that did not. We chose to not obtain data on the specific healthcare facility of practice to maintain anonymity of responses and encourage healthcare providers to feel comfortable responding to the survey. This led to a lack of ability to understand within-center variation in responses which could potentially provide insight on the validity of center-specific responses regarding practice. However, even if within-center responses differed across individuals, we do not feel that this substantially changes our main findings which suggest important areas of practice variation. Finally, the cross-sectional design of our study may not adequately reflect changes in guidelines and knowledge since survey completion; however, no specific guidelines or overt implementation strategies have been performed in our country since these survey disseminations. We were unable to determine the impact of the difference in perceptions on patient outcomes. However, other than commentaries on existing adult AKI guidelines,21,22 no concrete pediatric AKI follow-up guidelines have been published in the literature.
Conclusion
Recently, a multi-disciplinary group of pediatric AKI experts convened to publish a commentary on an international AKI quality improvement goals consensus document published for adults (the 22nd Acute Disease Quality Initiative consensus conference). 23 The pediatric commentary highlights “As the impact of AKI in children has become clear, it is critical to focus on strategies that improve the process of care by developing care pathways with defined quality metrics/indicators and by disseminating these tools to optimize AKI care to improve outcomes in children at risk of AKI.” 21 We believe that understanding the HCP beliefs and existing variations in care processes will help optimize the feasibility and success of future educational and implementation endeavors to improve pediatric AKI care. We found that AKI management, perceived importance, and follow-up beliefs vary across HCP groups in Canada. Such variability may adversely impact the ability to develop and implement robust AKI management and follow-up guidelines. Factors associated with variation and motivating factors for current perspectives should be explored, to maximize relevance of guideline development for stakeholders and maximize knowledge translation strategies. Future work should include developing educational tools targeting areas of highest knowledge and practice uncertainty. Findings from this survey study may aid in addressing provider beliefs and developing realistic, feasible, and pragmatic intervention trials for AKI management and follow-up in children.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581231168088 – Supplemental material for Perspectives of Pediatric Nephrologists, Intensivists and Nurses Regarding AKI Management and Expected Outcomes
Supplemental material, sj-docx-1-cjk-10.1177_20543581231168088 for Perspectives of Pediatric Nephrologists, Intensivists and Nurses Regarding AKI Management and Expected Outcomes by Adrian Che, David D’Arienzo, Allison Dart, Cherry Mammen, Susan Samuel, Todd Alexander, Catherine Morgan, Tom Blydt-Hansen, Patricia Fontela, Gonzalo Garcia Guerra, Rahul Chanchlani, Stella Wang, Vedran Cockovski, Natasha Jawa, Jasmine Lee, Sophia Nunes, Stephanie Reynaud and Michael Zappitelli in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-pdf-2-cjk-10.1177_20543581231168088 – Supplemental material for Perspectives of Pediatric Nephrologists, Intensivists and Nurses Regarding AKI Management and Expected Outcomes
Supplemental material, sj-pdf-2-cjk-10.1177_20543581231168088 for Perspectives of Pediatric Nephrologists, Intensivists and Nurses Regarding AKI Management and Expected Outcomes by Adrian Che, David D’Arienzo, Allison Dart, Cherry Mammen, Susan Samuel, Todd Alexander, Catherine Morgan, Tom Blydt-Hansen, Patricia Fontela, Gonzalo Garcia Guerra, Rahul Chanchlani, Stella Wang, Vedran Cockovski, Natasha Jawa, Jasmine Lee, Sophia Nunes, Stephanie Reynaud and Michael Zappitelli in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-pdf-3-cjk-10.1177_20543581231168088 – Supplemental material for Perspectives of Pediatric Nephrologists, Intensivists and Nurses Regarding AKI Management and Expected Outcomes
Supplemental material, sj-pdf-3-cjk-10.1177_20543581231168088 for Perspectives of Pediatric Nephrologists, Intensivists and Nurses Regarding AKI Management and Expected Outcomes by Adrian Che, David D’Arienzo, Allison Dart, Cherry Mammen, Susan Samuel, Todd Alexander, Catherine Morgan, Tom Blydt-Hansen, Patricia Fontela, Gonzalo Garcia Guerra, Rahul Chanchlani, Stella Wang, Vedran Cockovski, Natasha Jawa, Jasmine Lee, Sophia Nunes, Stephanie Reynaud and Michael Zappitelli in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-pdf-4-cjk-10.1177_20543581231168088 – Supplemental material for Perspectives of Pediatric Nephrologists, Intensivists and Nurses Regarding AKI Management and Expected Outcomes
Supplemental material, sj-pdf-4-cjk-10.1177_20543581231168088 for Perspectives of Pediatric Nephrologists, Intensivists and Nurses Regarding AKI Management and Expected Outcomes by Adrian Che, David D’Arienzo, Allison Dart, Cherry Mammen, Susan Samuel, Todd Alexander, Catherine Morgan, Tom Blydt-Hansen, Patricia Fontela, Gonzalo Garcia Guerra, Rahul Chanchlani, Stella Wang, Vedran Cockovski, Natasha Jawa, Jasmine Lee, Sophia Nunes, Stephanie Reynaud and Michael Zappitelli in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
We would like to thank the CAN-SOLVE CKD Network for providing resources to help develop the original survey; stakeholder groups including the Canadian Association of Pediatric Nephrologists (CAPN), Canadian Association of Critical Care Nurses (CACCN), and the C17 Council for helping to provide information for survey dissemination; Sarah Gil for her enormous effort and help to design and disseminate the original survey.
Ethics Approval and Consent to Participate
Ethics approval was stated in the methods section of the article.
Consent for Publication
All authors consent to the publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.