
Abstract
Background:
Life expectancy in patients with end-stage kidney disease treated with hemodialysis (HD) is limited, and as such, the presence of an advanced care directive (ACD) may improve the quality of death as experienced for patients and families. Strategies to discuss and implement ACDs are limited with little being known about the status of Do Not Resuscitate (DNR) orders in the Canadian HD population.
Objectives:
Using data from the Dialysis Outcomes and Practice Patterns Study (DOPPS), we set out to (1) examine the variability in DNR orders across Canada and its largest province, Ontario and (2) identify clinical and functional status measures associated with a DNR order.
Design:
We conducted a retrospective cohort study using data from the DOPPS Canada Phase 4 to 6 from 2009 to 2017.
Setting:
DOPPS facilities in Canada.
Patients:
All adults (>18 years) who initiated chronic HD with a documented ACD were included.
Measurements:
ACD and DNR orders.
Methods:
Descriptive statistics were compared for baseline characteristics (demographics, comorbidities, medications, facility characteristics, and patient functional status) and DNR status. The crude proportion of patients per facility with a DNR order was calculated across Canada and Ontario. Functional status was determined by activities of daily living and components of the Kidney Disease Quality of Life (KDQOL)-validated questionnaire. We used generalized estimating equations (GEEs) to create sequential multivariable models (demographics, comorbidities, and functional status) of variables associated with DNR status.
Results:
A total of 1556 (96% of total) patients treated with HD had a documented ACD and were included. A total of 10% of patients had a DNR order. The crude variation of DNR status differed considerably across facilities within Canada, between Ontario and non-Ontario, and within Ontario (interprovince variation = 6.3%-17.1%, Ontario vs non-Ontario = 8.2% vs 11.7%, intraprovincial variation [Ontario] = 1%-26%). Patients with a DNR order were more commonly older, white, with cardiac comorbidities, with less or shorter predialysis care compared with those without a DNR order. Patients with a DNR order reported lower energy, more difficulty with transfers, meal preparation, household tasks, and financial management. In a multivariate model, age, cardiac disease, stroke, dialysis duration, and intradialytic weight gain were associated with DNR status.
Limitations:
Relatively small number of events or measures in certain categories.
Conclusions:
A large inter- and intraprovincial (Ontario) variation was observed regarding DNR orders across Canada highlighting areas for potential quality improvement. While functional status did not appear to have a bearing on the presence of a DNR order, the presence of various comorbidities was associated with the presence of a DNR order.
Keywords
What was known before
Dialysis may be a terminal treatment for patients and as such, end-of-life planning may lead to improvements in the death process. Strategies to discuss and implement advance care directives (ACDs) are limited with little being known about the status of Do Not Resuscitate (DNR) orders in the Canadian hemodialysis (HD) population.
What this adds
In this analysis of Canadian Dialysis Outcomes and Practice Patterns Study (DOPPS) facilities, we found ACDs were completed in most of the patients with 10% indicating “Do Not Resuscitate (DNR)” as their end-of-life plan and this varied by Province and within Ontario. Factors associated with a DNR order were age, cardiac disease, stroke, dialysis duration, and intradialytic weight gain, whereas functional status measures were not.
Background
Most of the patients with end-stage kidney disease (ESKD) will undergo dialysis as a terminal therapy meaning they will die on or shortly after discontinuing dialysis therapy. 1 In Canada, the mean age of patients with ESKD is 67 years and the prevalence of ESKD among patients >75 years is rising rapidly. 2 The 5-year mortality rate among elderly dialysis patients exceeds 60%, and among patients 80 years or older who begin dialysis, the average survival is 3 years. 3 Over the past decade, the age standardized mortality rate in Canadian hemodialysis (HD) patients remains unchanged. 4 A recent study of dialysis patient’s end of life (EOL) in Ontario demonstrated one-third died in intensive care unit, another one-third died in an acute care hospital or emergency department while few received palliative care. 5 These findings suggest EOL on dialysis may be suboptimal and not consistent with patient wishes.
Advanced care directives (ACDs), the outlining of specific care protocols in the event of critical illness, are recommended as part of a routine, comprehensive care plan, and may lead to EOL care more in line with patient wishes. 6 Previous studies suggest significant international variation in the completion of ACD and DNR status. 7 To our knowledge, the prevalence of ACDs and DNR has not been documented within the Canadian HD population. The completion of ACD and DNR status is a recommended measure of quality of care for dialysis facilities with evidence demonstrating improvement with standardized methods.8,9 As part of a continuous quality improvement initiative, 50 patients participated in standardized ACD planning, resulting in a change in status from “full code” to “DNR” in 40%. 9 The use of a standardized, educational intervention in a randomized study of 420 dialysis patients reported improvement in EOL decision-making and confidence. 10
Barriers to improve ACD planning include the lack of time required for a full discussion, concerns about invoking hopelessness in patients, lack of training for staff in ACD discussions, limited information on prognostication, and uncertainty when ACD discussions should occur.11-14 To better improve EOL care for patients, we examined the interprovincial and within Ontario variation in DNR orders and identified clinical characteristics (demographic, comorbidities, and functionality) associated with a DNR order.
Methods
Study Cohort and Design
We conducted a retrospective cohort study using data from the Dialysis Outcomes and Practice Patterns Study (DOPPS) Canada data. 15 The DOPPS enrolls dialysis facilities using random sampling and captures patient- and facility-level data including demographics, comorbidities, laboratory values, dialysis prescriptions, and clinical outcomes. Further details on DOPPS data collection protocol and study design have been published elsewhere. 15 Canada has contributed data to DOPPS since DOPPS Phase 2 (2002). All patients captured in DOPPS Canada (chronic HD patients, >18 years of age) with an ACD were included. The date of dialysis initiation was the first day of follow-up (index date).
Covariates
The DOPPS captures variables at both the patient and facility levels. Patient demographics captured include age, sex, race, marital status, and education level. Further clinical variables such as causes of kidney failure, comorbidities (coronary heart disease/coronary artery disease, chronic atrial fibrillation, coronary heart failure, stroke, dementia, and cancer), laboratory values (phosphorus, albumin, hemoglobin, parathyroid hormone, and ferritin levels), vascular access (arteriovenous fistula or graft, temporary or permanent central venous catheter, multiple accesses), predialysis blood pressure (systolic and diastolic), predialysis care, and dialysis treatment characteristics (duration, number of sessions, intradialytic weight loss) are captured at dialysis initiation or during therapy. Activities of daily living (ADLs) and instrumental activities of daily living (iADLs) are assessed by a validated patient self-reported questionnaire and included measures of eating, dressing, bathing, toileting, transferring, use of telephone, traveling, grocery shopping, meal preparation, performing housework, laundry, taking medications, and managing finances. The ADLs/iADLs were captured as “need no help,” “need some help,” and “unable to do at all” and converted to binary categories of “no assistance” or “some or unable to do.” 16 Individual components, the physical and mental health composite of the Kidney Disease Quality of Life (KDQOL 36) tool measuring quality of life (QOL), were included as calculated scale scores with the higher score indicating a higher QOL. 17 Individual dialysis facilities were de-identified within provinces. All provinces were aggregated with the exception of Ontario to maintain facility anonymity. As Ontario has a large number of DOPPS facilities (both academic and community-based), anonymity could be maintained examining the province data.
Outcome
The study outcome was DNR status. From the DOPPS medical questionnaire (collected every 4 months), DNR was defined by an affirmative response to “During this reporting interval, had a decision been made to not resuscitate the patient in the event of a cardiac arrest (DNR)?” The answer options were “0: No, 1: Yes, 2: Unknown.”
Statistical Analysis
We compared demographics, comorbidities, medications, laboratory values, and ADLs/iADLs for patients based on DNR status (yes or no) using χ2 test for categorical data, Student t tests for difference in paired means, and analysis of variance for differences in means across multiple groups. The proportions of patients with an affirmative DNR status between provinces, between Ontario and non-Ontario, and by facility within Ontario were determined. Components of the QOL were compared by DNR status using the Student t test. We used generalized estimating equations (GEEs) to create 3 models that measured the association between sociodemographic variables (model 1), clinical variables (model 2), functional status (model 3), and DNR status. 18 The most parsimonious models were determined using backwards stepwise regression, removing variables until the model with the smallest quasi-likelihood under the independence model criterion (QIC) was identified. 19 Then, a fourth model was created using the variables from previous models to determine the odds of a DNR order. Backwards stepwise regression was performed once again to determine the most parsimonious model with the smallest QIC as the indicator. Generalized estimating equation was used to account for clustering of patients within facilities. P values of <.05 were considered statistically significant. We conducted all analyses with SAS software, SAS Enterprise Guide version 7.1 (SAS Institute Inc., Cary, NC).
Results
During the study period, a total of 26 facilities were enrolled with data from 3786 patients (15 and 1756 in Ontario) of which 1556 (96%) with a documented ACD were included in our study. The proportion of patients with ACD completion decreased over the DOPPS phases (96.1%-90.4%; see Figure 1). A total of 156 (10%) of the study cohorts had a DNR order.
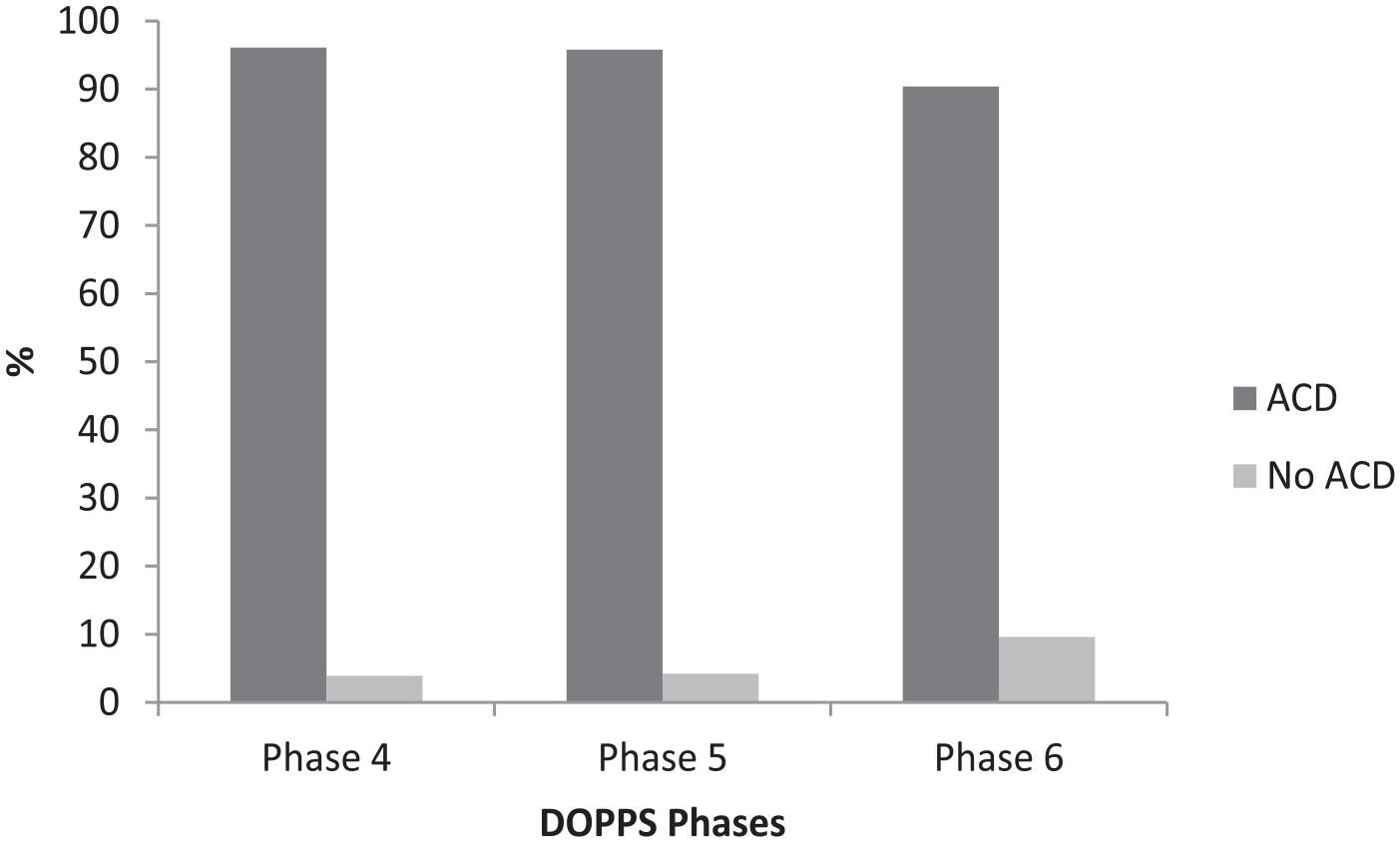
Proportion of Canadian dialysis patients who completed an advanced care directive across DOPPS phases from 2009 to 2017.
Variation Across Regions
Hemodialysis patients with a DNR had a nonstatistically significant variation across provinces with a low of 6.3% (4/63) in Alberta and a high of 17.1% (6/29) in Manitoba (P = .15; Figure 2 and Table 1). As Ontario had the highest number of facilities and patients contributing data (n = 14 facilities, 743 patients), we further compared Ontario versus the remainder of Canadian jurisdictions. Facilities in Ontario reported that 8.2% of patients compared with 11.7% of non-Ontario regions were DNR (P = .02). Within Ontario, facilities reported a range of 0 to 66.7% with a DNR order (P < .0001). Of note, a single outlier center in Quebec reported a DNR order in 66% of patients.
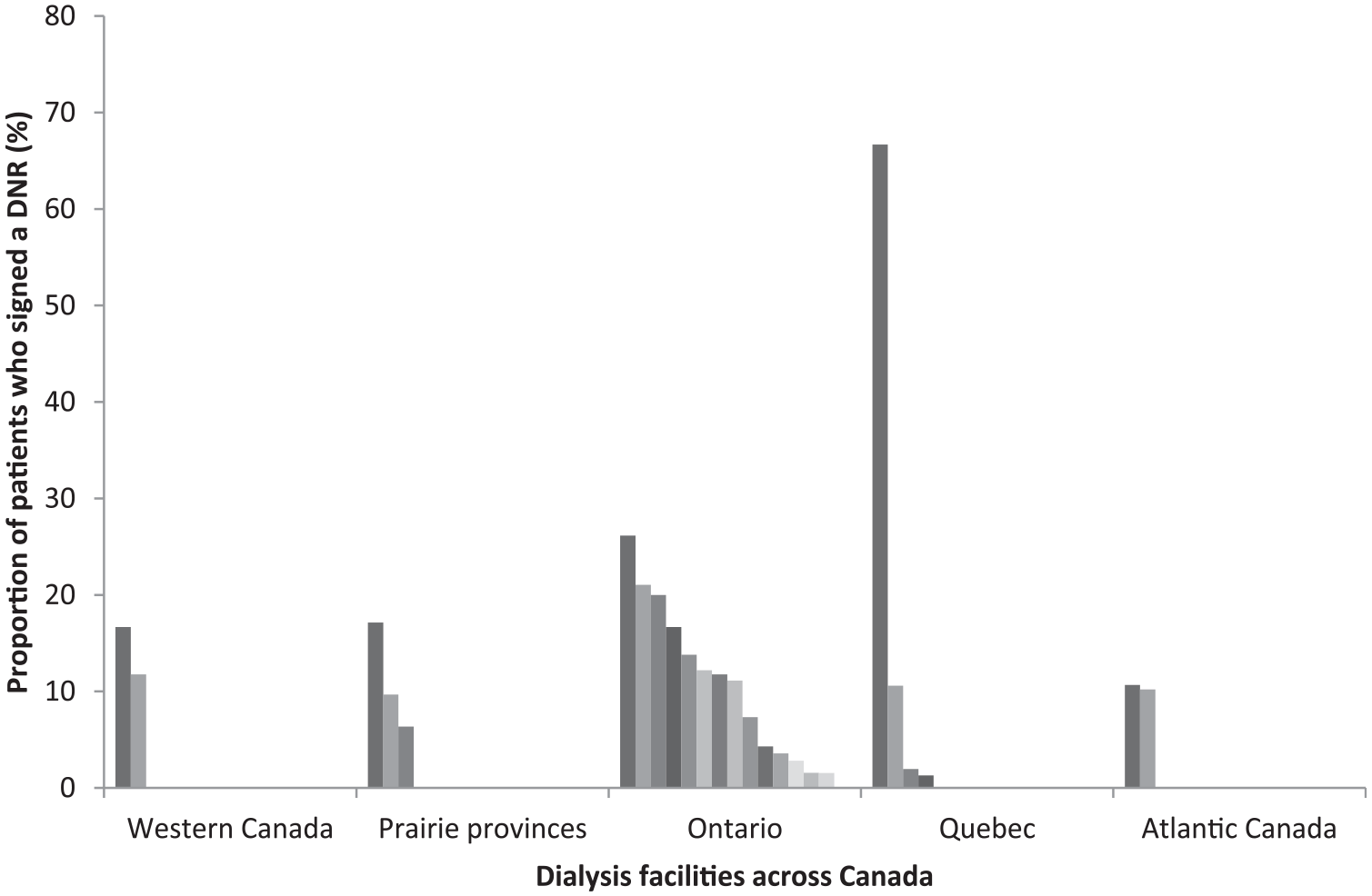
Proportion of DNR patients within dialysis facilities by regions across Canada captured in DOPPS from 2009 to 2017.
Variations in DNR Orders Among Dialysis Facilities Across Canada Captured in DOPPS From 2009 to 2017.

Note. DNR = Do Not Resuscitate; DOPPS = Dialysis Outcomes and Practice Patterns Study. Bold indicates p < 0.05.
Percentages calculated per row; % percentage.
Characteristics of Patients With Completed ACD and Who Chose DNR
Advance care directive completion significantly differed in patients who are single, have cancer, and had intradialytic weight loss (see Table 2). A comparison of patients with and without a DNR order is presented in Table 3. The DNR patients were older (70.9 vs 62.7 years, P < .0001), white (90% vs 78%, P = .003), and had a history of cardiac disease, stroke, or cancer. Regarding marital status, widowed patients were more likely to be DNR, whereas patients who were single, divorced, or separated were not. Serum phosphorous was lower among those with DNR, whereas serum albumin and hemoglobin did not differ. A longer duration of predialysis care was more common with resuscitation. Average dialysis duration was shorter among DNR patients, whereas number of sessions and intradialytic weight loss were not.
Baseline Characteristics of Dialysis Patients With an Advanced Care Directive Captured in DOPPS From 2009 to 2017.

Note. DOPPS = Dialysis Outcomes and Practice Patterns Study; ACD = advanced care directive; N = number; % = frequency; ESKD = end stage kidney disease; CAD = coronary artery disease; CHD = coronary heart disease; PTH = parathyroid hormone; PTFE = polytetrafluoroethylene; BP = blood pressure; DNR = Do Not Resuscitate; PCR = polymerase chain reaction; AV = arteriovenous; mm Hg = millimeters of mercury; CVA = cerebral vascular accident. Bold indicates P < 0.05.
Baseline Characteristics of Dialysis Patients With a DNR order Captured in DOPPS From 2009 to 2017.

Note. DOPPS = Dialysis Outcomes and Practice Patterns Study; DNR = Do Not Resuscitate; N = number; % = frequency; ESKD = end-stage kidney disease; CAD = coronary artery disease; PTH = parathyroid hormone; PTFE = polytetrafluoroethylene; BP = blood pressure; AV = arteriovenous; mm Hg = millimeters of mercury. Bold indicates P < 0.05.
ADLs, QOL, and DNR Status
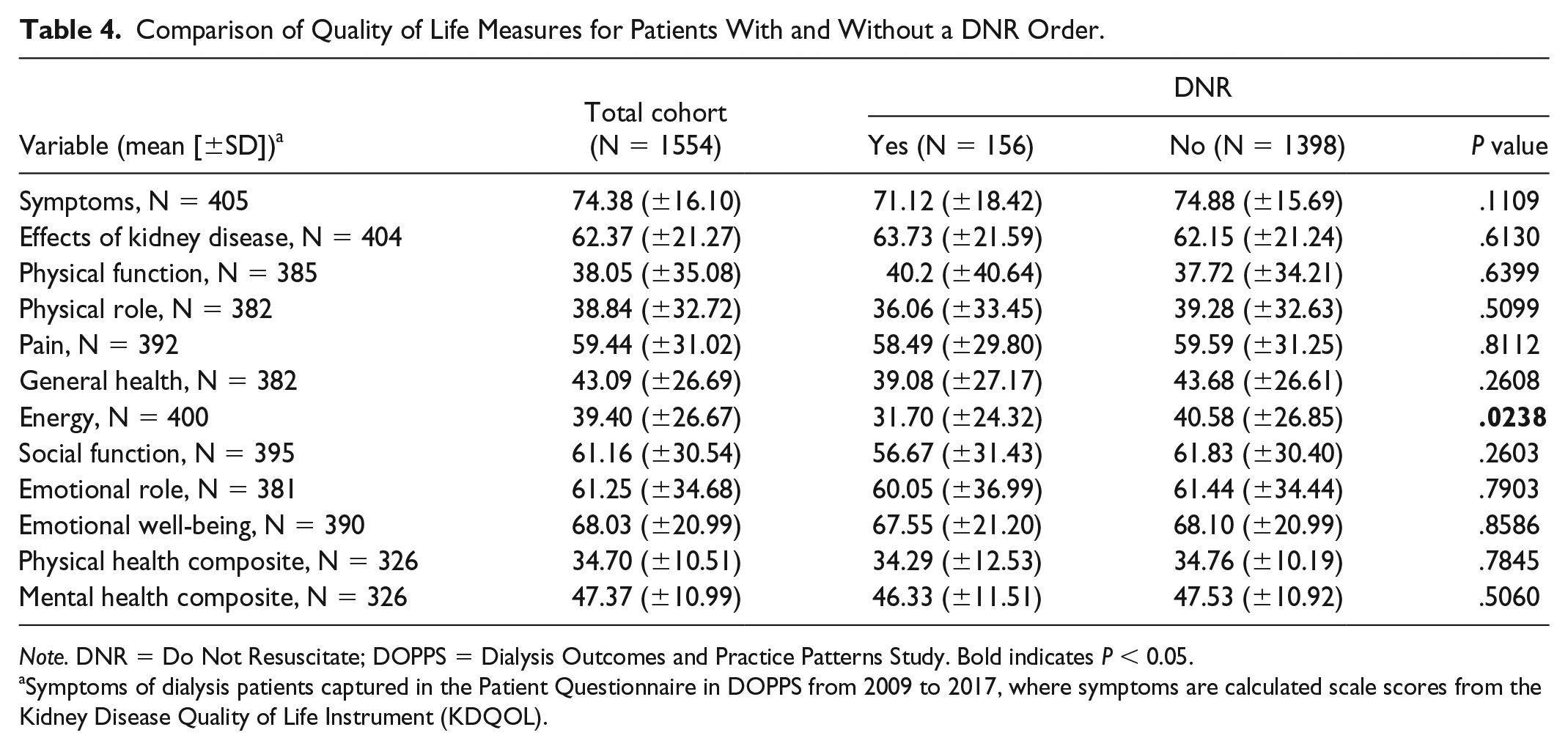
We compared a broad range of ADL and iADLs among patients with DNR orders (Figure 3). A DNR order was associated with needing more aid in meal preparation and doing laundry. Resuscitation was associated with needing more aid to transfer form bed to chair, doing housework, and managing money. Comparing QOL components from the KDQOL (Table 4), only the mean energy level (DNR 31.7 vs no DNR 40.6) differed (P = .02).

Comparison of a DNR order versus resuscitation (no DNR) among patients requiring assistance or who are unable to perform activities of daily living.
Comparison of Quality of Life Measures for Patients With and Without a DNR Order.
Note. DNR = Do Not Resuscitate; DOPPS = Dialysis Outcomes and Practice Patterns Study. Bold indicates P < 0.05.
Symptoms of dialysis patients captured in the Patient Questionnaire in DOPPS from 2009 to 2017, where symptoms are calculated scale scores from the Kidney Disease Quality of Life Instrument (KDQOL).
The Association of DNR Status With Clinical and Patients Characteristics
The association of DNR status with patient demographics, comorbidities, and dialysis characteristics and functional status using multivariate models is presented in Figure 4. In a model adjusting for demographics (age, sex, race, and marital status; model A), only age was associated with a DNR order with a 5% higher odds per year increase in age. In a model including comorbidities and dialysis characteristics (model B), cardiac disease (odds ratio [OR] = 1.83, 95% confidence interval [CI] = 1.18-2.85), dialysis duration (OR = 0.89, 95% CI = 0.82-0.96 per minute), and intradialytic weight gain (OR = 1.21, 95% CI = 1.02-1.43 per liter) were associated with DNR. In a model including ADLs/iADLs and QOL, no individual components remained significant (model C). In a final model including significant variables from models A and B, age, cardiac disease, stroke, dialysis duration, and intradialytic weight remained associated with DNR status (model D).

Multivariate models of the association of patient demographics (model A), comorbidities and dialysis characteristics (model B), activities of daily living and quality of life (model C), and statistically significant variables from models B and C (model D) and a DNR order.
Discussion
In the Canadian national study of DOPPS participating facilities, we found ACD completion was high among DOPPS facilities with10% having a DNR order in place. The DNR status differed considerably across facilities within Canada, between Ontario and non-Ontario, and within Ontario. Patients with a DNR order were more commonly older, white, with cardiac comorbidities, with less or shorter predialysis care compared with those with resuscitation. Patients who were DNR reported lower energy, more difficulty with transfers, meal preparation, household tasks, and financial management. In a multivariate model, we identified age, cardiac disease, stroke, dialysis duration, and intradialytic weight gain as being associated with a DNR order.
To our knowledge, the current study is the first to report DNR status in a Canadian HD population. Previous studies report a wide variation in the completion of ACD orders and DNR status.7,9,20,21 A single-center report from the United States reported ACD completion in 49% with noncompletion associated with younger age, men, and non-white race. In the general Canadian population, Teixeira et al using an online survey methodology reported that 20% had an ACD. 22 Chen et al in a single-center study reported that an acute illness, such as an acute coronary syndrome, is associated with a DNR order in 49% of patients with advanced kidney disease. 20 An international study of 8615 patients from the DOPPS HD cohort from 2005 reported the presence of a DNR order in 3.8% with a wide variation among countries (0% in Italy, 7.5% in United States, Canada excluded). 7 The higher observed proportion of DNR orders we observed may be based on cultural differences (countries may have differing values based on patient autonomy) or an era effect as awareness of the importance of ACDs on EOL care may be improving. 23 Although high, the prevalence of ACD orders among chronic HD patients could be further improved and may represent an actionable quality of care measure. It remains unclear whether the high proportion of ACD completion is limited to DOPPS facilities in Canada and future studies should specifically target non-DOPPS facilities.
A key barrier to ACD discussion is the limited ability for caregivers to accurately estimate prognosis.13,14,24 We specifically examined characteristics associated with DNR status to identify emerging risk factors that may trigger ACD discussions. We identified 2 functional measures (inability or requiring aid for meal preparation, laundry) that were more common with a DNR order. Conversely, the ability to manage finances, transfer, and do housework was more common with resuscitation. Interestingly, despite the multiple detailed measures recorded in the validated KDQOL questionnaire, only lower reported mean energy levels was more common in DNR patients. Based on our findings, simple measures of ADL/iADLs may provide more meaningful information than the KDQOL survey. Ultimately, in adjusted models, no functional status measures remained significant, whereas only a shorter dialysis duration and higher intradialytic weight gain were identified as potentially modifiable factors. Whether the identified dialysis-related factors are modifiable remains to be determined as the shorter dialysis time/higher weight gains may be related to worsening cardiovascular or nutritional status as opposed to being causative. As cardiovascular factors and age were strongly associated with a DNR order, it can be inferred that at a minimum ACD should be discussed among patients with an advanced age, existing, or new onset cardiovascular disease.
A large degree of variability in DNR status was noted across provinces and within the province of Ontario. This was surprising as many EOL values would be anticipated to be homogeneous and consistent across Canada. The observed variability across centers in Ontario could be attributed to differences in patient’s characteristics such as demographics (age, race), comorbidities (the prevalence of cardiac disease), practice patterns among facilities, or the era of data collection. We previously demonstrated that patient and facility characteristics are responsible for variability in the initiation of dialysis and choice of dialysis modality.25,26 Both provincial and nation-wide variability could be affected by whether patients are cared for at academic or community hospitals. Residents—especially early in their training—are uncomfortable with and may avoid addressing DNR status. 27 Therefore, patients cared for at academic centers may not have had the opportunity to discuss ACDs and EOL care. This discomfort extends to nephrology trainees who recognize the importance of training in matters of EOL care but are less likely to receive it than teaching on the management of distal renal tubular acidosis. 28 Furthermore, individual jurisdictions may have local champions/expertise, formal working groups or policy-driven, continuous quality initiatives targeting EOL care, and documentation as a quality metric.6,23 The introduction of provincial or ideally, national EOL care plans for dialysis patients could ensure standardization of care and the development of specific tools. Innovative means of education, such as tablet devices, could overcome potential barriers. 29
Some noteworthy limitations were present in our study. Despite including all DOPPS facilities in Canada and multiple phases of the DOPPS study, there were relatively small numbers of DNR orders, especially between provinces, limiting our multivariable modeling. We lacked information on race, a key characteristic previously demonstrated to affect ACD conversations. 21 Although we captured DNR status, it may not have been dialysis-specific, ie, we were not able to discern whether the (dis)continuation was included in the ACD discussion. Patient characteristics, clinical information, and functional status measures were captured cross-sectionally and as such may not reflect the patient’s state at actual completion of the ACD. We used an automated variable reduction technique (step-wise regression) for our adjusted models as opposed to an a priori covariate selection strategy based on clinical relevance. As ADLs are not routinely captured in non-DOPPS facilities, generalizability may be limited. As this was an observational study, we were unable to determine causality.
In conclusion, in participating DOPPS facilities in Canada, over 90% had an ACD in place with 10.0% being DNR. Advanced age and cardiovascular disease were associated with being DNR and should serve as prompts for ACD discussion to take place. Standardization may lead to reductions in the large degree of observed variability among dialysis facilities.
Footnotes
Ethics Approval and Consent to Participate
This project has been approved by the Research Ethics Board at The Ottawa Hospital, Ottawa, Canada.
Consent for Publication
All authors have given their consent for publication of this article.
Availability of Data and Materials
The data and materials are not available for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ontario Renal Network/Cancer Care Ontario.