
Abstract
Background:
Many families choose not to consent to organ donation at the time of their loved one’s death. In Ontario, Canada, whether these decisions vary by ethnicity remains unclear.
Objective:
To compare the proportion of families of immigrants who consented for deceased organ donation with families of long-term residents.
Design:
Population-based retrospective cohort study.
Setting:
Potential donors in Ontario, Canada, between November 2008 and March 2013.
Methods:
We used linked administrative databases to study the proportion of families who consented for deceased organ donation.
Results:
Overall, of the 2873 families of potential donors approached, 1912 (67%) provided consent for deceased organ donation. Families of immigrants were less likely to provide consent compared with families of long-term residents (46% [135 of 291] vs 69% [1777 of 2582]; adjusted rate ratio (RR): 0.72; 95% confidence interval [CI]: 0.63-0.81). When examined by the country of birth, families of immigrants from the following regions were less likely to consent to organ donation compared with long-term residents: South Asia (RR: 0.71; 95% CI: 0.55-0.91), East Asia and Pacific (RR: 0.68; 95% CI: 0.53-0.88) and Middle East, North Africa, and sub-Saharan Africa (RR: 0.58; 95% CI: 0.37-0.91).
Limitations:
We could not determine why consent was not obtained. We had a small sample of immigrants. We only had access to the potential donors’ information and not the family member who was approached for consent. Many characteristics that we examined were nonmodifiable (eg, age, sex).
Conclusions:
In Ontario, families of immigrants are less likely to consent to deceased organ donation. There is an opportunity to better understand the reasons for lower consent among certain immigrant groups.
What was known before
Many families choose not to consent to organ donation at the time of their loved one’s death. Families of critically ill ethnic minorities may be less likely to consent on their relative’s behalf.
What this adds
These results suggest that in Ontario, families of immigrants are less likely to consent to deceased organ donation. There is an opportunity to identify and better understand the reasons for lower rate consent among certain immigrant groups.
Background
The ongoing shortage of organs for transplantation demands strategies that maximize the availability of this scarce resource. Several countries are working to increase the proportion of families who consent to deceased organ donation at the time of their relative’s death, which ranges between 40% and 70% across jurisdictions.1-3 Consent rates are undoubtedly a significant factor for increasing transplantation across all ethnicities. Ethnic minorities have been shown to have lower rates of organ donation registration, and families of critically ill ethnic minorities may be less likely to consent on their relative’s behalf.2,4 Therefore, this population may represent an important source of underutilized organs that could be better accessed through culturally sensitive education programs.
Canada has the highest proportion of foreign-born individuals among the 8 leading industrial and developed countries in the world, with the majority of immigrants living in its most populated province, Ontario. 5 The province also houses some of the most comprehensive, large, administrative health care databases in the country, which facilitates population-level health research. Using these resources, we compared the familial consent rates of immigrants with long-term residents in general, and by region of origin. We also identified patients who were already registered donors to see whether registration modified the likelihood of obtaining final consent from families.
Methods
Study Design and Setting
We conducted a population-based retrospective cohort study in the province of Ontario, Canada (population: 13 million) using large administrative health care databases held at the Institute for Clinical Evaluative Sciences (ICES). These datasets were linked using unique encoded identifiers. In Ontario, residents have universal health care coverage. To be an organ donor, the decedent must have suffered a nonrecoverable injury and be mechanically ventilated at the time the provincial organ procurement organization is notified. 6 Each decedent’s eligibility to donate is evaluated on an individual basis. At the time of imminent death or family’s interest in organ donation, a donor coordinator experienced in talking to families about donation will access the decedent’s donor registration information. If the decedent is registered, the coordinator will provide this information to the donor’s family members at an appropriate time. In Ontario, the next-of-kin makes the final decision on proceeding with organ and tissue donation regardless of whether the decedent, prior to death, was registered for organ and tissue donation or not. We did not include decedents who were only referred for tissue-only donation. We conducted this study according to a prespecified protocol that was approved by the research ethics boards at Sunnybrook Health Sciences Centre (Toronto, Canada). We used the RECORD statement to guide the reporting of this study (Supplemental Table 1).
Data Sources
We ascertained demographic information, potential confounders, and outcome information of potential donors from linked administrative databases. The second author (A.A.A) had access to the database population used to create the study population.
First, we obtained data of those who were referred for deceased organ and tissue donation from the Trillium Gift of Life Network. Patients who meet any of the following are referred for potential organ donor consideration: (1) Glasgow Coma Scale score of 3, (2) injured brain or nonrecoverable injury or illness, (3) family initiated discussion of organ donation with the health care team or withdrawal of life-sustaining therapy, and/or (4) planned discussion of therapy limited, de-escalation of treatment, or withdrawal of life-sustaining therapy. All patients referred for organ donation are then evaluated for medical suitability. This dataset also contains information on whether the family was approached for donation and whether consent from their family was obtained. These data are recorded on a real-time basis by a call center. We refer to these patients as potential donors.
Second, we obtained demographics from the Ontario Registered Persons Database. This database has demographic and vital status information on all residents who have ever been issued a health card. We estimated the individual’s income using neighborhood income quintiles.
Third, we used Matheson’s Canadian Marginalization Index to assign marginalization quintiles. 7 This index describes 4 components of marginalization: residential instability, ethnic concentration, dependency, and material deprivation. 7
Fourth, we used the Canadian Institute for Health Information Discharge Abstract Database (CIHI-DAD) to obtain information on hospitalizations to ascertain the patient’s cause of death and to determine whether the admitting hospital of the potential donor had an academic affiliation. We classified cause of death using the International Classification of Diseases Revision 10 codes into traumatic brain injury (S06, S07, S08, S09); subarachnoid and intracranial hemorrhage (I60, I61, I62); other damage to the brain (I63, I64); acute myocardial infarction, cardiac arrest (I21, I22, I23, I46); and all other causes of death.
Finally, we used the Immigration, Refugees and Citizenship Canada’s (IRCC) Permanent Resident Database to ascertain immigration status. This database contains landing records for every permanent legal immigrant who landed in Canada since 1985 onward. All information is captured at the time of immigration application. The overall linkage rate of this dataset to the Registered Persons Database is approximately 86.4%. 8 More details about the linkage and the dataset can be found elsewhere. 8 We generally grouped each immigrant’s country of birth by their world region of origin, according to the World Bank system: (a) South Asia; (b) East Asia and Pacific; (c) Latin America and Caribbean; (d) the United States, Australia, New Zealand, and Western Europe; (e) Middle East, North Africa, and sub-Saharan Africa; and (f) Eastern Europe and Central Asia. 9 We combined Western Europe with the United States, Australia, and New Zealand in one group, as well as sub-Saharan Africa, Middle East, and North Africa in another group because of small sample sizes. This grouping is done because we hypothesized that differences in familial consent are primarily due to cultural awareness and attitudes.
Study Population, Outcomes, and Statistical Analysis
We included all permanent residents of Ontario who were approached for deceased organ and tissue donation with a record of hospitalization from November 1, 2008, to March 31, 2013. For our comparison of immigrants and long-term residents, we classified immigrants as having a record within the IRCC’s Permanent Resident Database. Everyone else without a record in the IRCC database was classified as long-term residents (including immigrants who landed in Canada prior to 1985).
The outcome of interest was obtaining consent from the families of potential donors. We assessed differences in baseline characteristics between immigrants and long-term residents using the chi-square test for categorical variables and the Mann-Whitney U test for continuous variables. We used a modified Poisson regression model with a robust error estimator to compare familial consent rates among immigrants and long-term residents. We used complete-case analysis as the amount of missing data was low (~2%). We also evaluated the association between immigrant status and familial consent in 4 subgroups: age, sex, hospital type, and cause of death. We determined P values for interaction by including the interaction terms in the regression models. We hypothesized that these 4 characteristics affect long-term residents and immigrants similarly. We adjusted for 11 potential confounders: world region of birth, age, sex, residence (urban vs rural), neighborhood income quintile, material deprivation, ethnic concentration, dependency, residential instability, cause of death, and academic hospital affiliation. We conducted analyses using SAS software version 9.4 (SAS Institute Inc, Cary, North Carolina), and a 2-sided P value <.05 was considered to be statistically significant.
Results
From November 1, 2008, to March 31, 2013, there were 2926 potential donors approached to obtain familial consent (Supplemental Figure 1). Of the 2926 potential donors, 291 were immigrants and 2635 were long-term residents. The median age of immigrants was 54 (interquartile range [IQR]: 42-65) and median age of long-term residents was 57 (IQR: 44-68). The baseline characteristics for the potential donors whose families were approached for consent by immigration status are presented in Table 1. The groups differed on most baseline characteristics; immigrants were more likely to be younger, live in areas with lower income, and demonstrate higher levels of marginalization. Of the 2926 potential donors, no immigrants and 53 long-term residents (2%) had missing data on the marginalization quintiles. Thus, 2873 potential donors were used to determine the rate of familial consent among immigrants and long-term residents.
Baseline Characteristics of Deceased Immigrants and Long-term Residents Whose Families Were Approached for Organ and Tissue Donation.
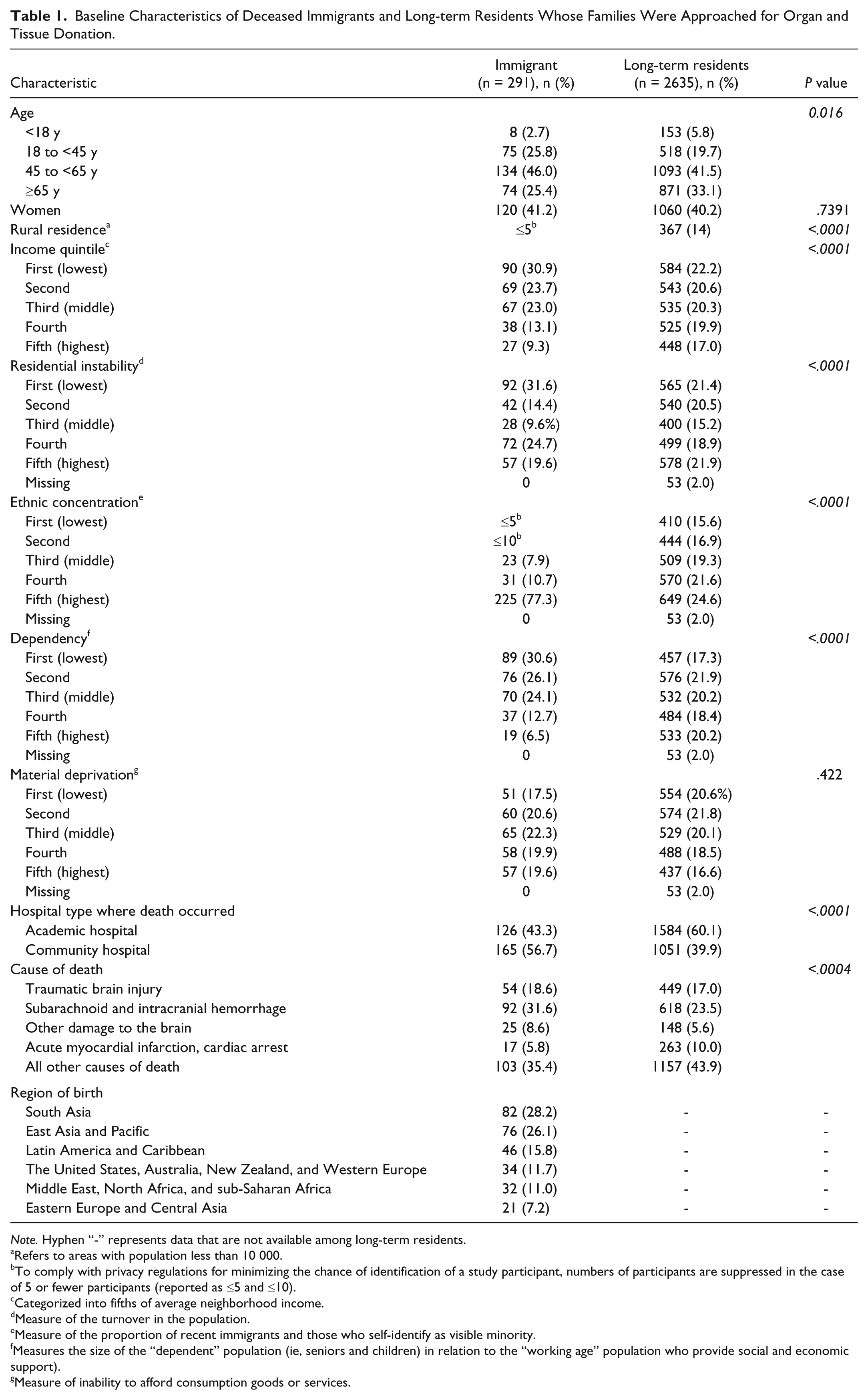
Note. Hyphen “-” represents data that are not available among long-term residents.
Refers to areas with population less than 10 000.
To comply with privacy regulations for minimizing the chance of identification of a study participant, numbers of participants are suppressed in the case of 5 or fewer participants (reported as ≤5 and ≤10).
Categorized into fifths of average neighborhood income.
Measure of the turnover in the population.
Measure of the proportion of recent immigrants and those who self-identify as visible minority.
Measures the size of the “dependent” population (ie, seniors and children) in relation to the “working age” population who provide social and economic support).
Measure of inability to afford consumption goods or services.
Outcomes
All potential donors
Of 2873 potential donors, 1912 families provided consent (66.6%). Families of immigrants were less likely to provide consent compared with families of long-term residents (46.4% [135 of 291] vs 68.8% [1777 of 2582]; adjusted rate ratio (RR): 0.72; 95% confidence interval [CI]: 0.63-0.81; Table 2). When examined by the region of origin, families of immigrants from different regions were less likely to consent to organ and tissue donation compared with long-term residents: South Asia (RR: 0.71; 95% CI: 0.55-0.91), East Asia and Pacific (RR: 0.68; 95% CI: 0.53-0.88) and Middle East, North Africa, and sub-Saharan Africa (RR: 0.58; 95% CI: 0.37-0.91).
Rate of Familial Consent Among Immigrants and Long-term Residents (n = 2873).
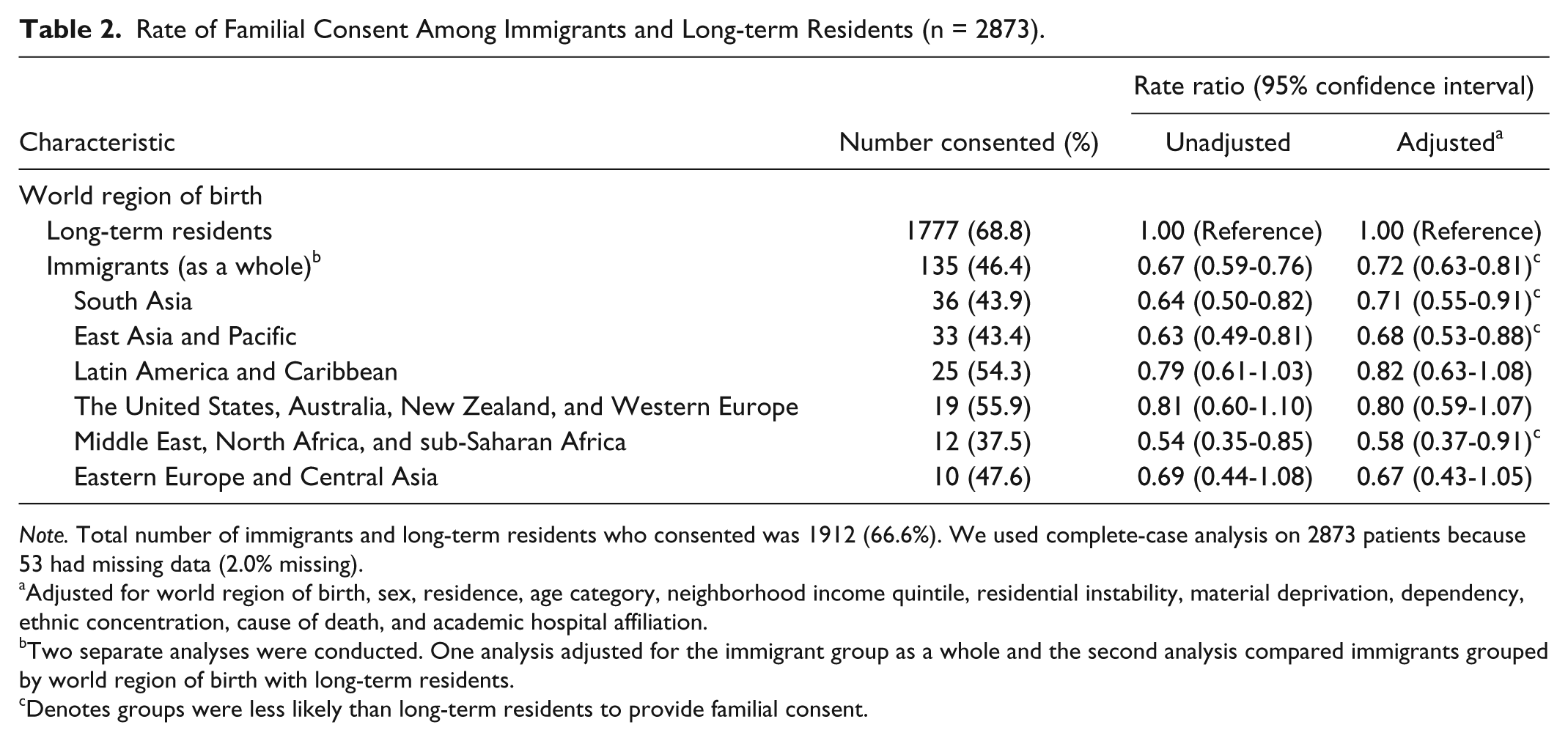
Note. Total number of immigrants and long-term residents who consented was 1912 (66.6%). We used complete-case analysis on 2873 patients because 53 had missing data (2.0% missing).
Adjusted for world region of birth, sex, residence, age category, neighborhood income quintile, residential instability, material deprivation, dependency, ethnic concentration, cause of death, and academic hospital affiliation.
Two separate analyses were conducted. One analysis adjusted for the immigrant group as a whole and the second analysis compared immigrants grouped by world region of birth with long-term residents.
Denotes groups were less likely than long-term residents to provide familial consent.
Registered potential donors
Among the 2926 potential donors, 606 (20.7%) had previously registered for deceased organ and tissue donation. Among these potential donors, we found no statistically significant difference in consent rates among registered immigrants and long-term residents. Of these registered potential donors, 83.8% (31 of 37; 95% CI: 68.9%-92.7%) of immigrant families provided consent compared with 89.3% (508 of 569; 95% CI: 86.5%-91.6%) of registered long-term residents.
Subgroup Analyses
Age, sex, and cause of death did not modify the relative association between immigrant status and familial consent (Supplemental Table 2). The relative rate of familial consent in immigrants (vs long-term residents) was lower in community hospitals compared with academic hospitals (P value for interaction = .045).
Discussion
We found that families of immigrants in Ontario, Canada, were less likely to consent to deceased organ donation compared with long-term residents. However, among those who were registered for organ and tissue donation, we found no difference in the likelihood of consent.
The 2 largest ethnic groups in Ontario, Canada, are South Asians and Chinese. Similar to our previous findings that families of South Asian and Chinese individuals were less likely to provide consent, 10 we found that families of immigrants born from the East Asia and Pacific region and South Asia were also less likely to consent to deceased organ and tissue donation even after adjustment for multiple characteristics. We also found that families of immigrants born from the Middle East, North Africa, and sub-Saharan Africa region were less likely to consent. This finding is not surprising given lower levels of support for organ donation documented within these groups. 11
The similarity in donation rates that we observed among immigrants and long-term residents who had previously registered for organ donation supports the value of donor registries. Although our findings may have resulted from selection bias, it is also possible that the documented wishes of potential donors helped families concur with their choice to donate. In contrast, a British report found that 25% of Black and Asian families refuse to consent to organ donation even if their loved one was on the donor register compared with 10% for the rest of the population. 12 Researchers have suggested that in situations where an individual has registered for deceased organ donation, the emphasis should be on providing families with the registration information in addition to educative and support services rather than solely focusing on obtaining familial consent. 13 In Ontario, this has been our practice since 2009. Future research that examines differences in the reasoning behind familial refusal among immigrants compared with long-term residents may be useful to support efforts to provide educative and support services.
Our study has some limitations. First, our study was designed to measure differences in donation consent rates, and although our databases provided highly accurate information on that, we could not determine the reasons for failing to obtain familial consent for deceased organ donation. This information would be important for the design of strategies to increase consent rates and will be the subject of future work. Second, although our findings seem to support the value of organ donation registries, our analysis was limited by our small sample of immigrants and registered potential donors. Estimates from small sample sizes are imprecise, and these results should be interpreted with caution. Furthermore, while it is tempting to assume that the potential donor’s registration status helped encourage family members to provide consent, our findings may have been the result of high levels of support for organ donation throughout the families of registered potential donors. Third, our analysis of family consent among immigrants and long-term residents by world region of birth is limited by the small number of cases which yielded wide confidence intervals produced in the multivariable analysis. These estimates should be interpreted with caution given the uncertainty in the confidence intervals due to the low number of cases within the subgroup analysis. Fourth, we only had access to the potential donors’ information and not the family member who was approached for consent. It may have been possible that there are important distinguishing characteristics of families that provide (vs do not provide) consent. Fifth, many of the characteristics we examined were nonmodifiable, and this limits the number of interventions that could arise from our findings. Simpkin et al found that modifiable characteristics such as the skills of the requestor and the timing of the conversation may have a significant impact on consent rates. 14 Sixth, an important limitation of the immigration dataset is that we classified immigrants who arrived prior to 1985 as “long-term residents” because we do not have any immigration records for immigrants prior to this date. However, as Benchimol et al mentioned, this group would have been residing in Canada for more than 10 years and their health service patterns would be more similar to nonimmigrants. 15
Overall, our findings show that a significant number of potentially life-saving organs are going unused among all potential donors, but particularly among those of ethnic minorities. This provides an important starting point for improving the availability of organ from these subpopulations. Further research will be targeted at defining specific factors responsible for this disparity and strategies for overcoming them, including the role for expanding organ donor registration.
Footnotes
Ethics Approval and Consent to Participate
This study was approved by the Sunnybrook Health Sciences Centre Research Ethics Board in Toronto, Ontario. Participant consent for this study was waived.
Consent for Publication
Not applicable
Availability of Data and Materials
The dataset for this study is held securely in coded form at the Institute for Clinical Evaluative Sciences (ICES). While data sharing agreements prohibit ICES from making the dataset publicly available, access can be granted to those who meet prespecified criteria for confidential access, available at ![]() .
.
Author Contributions
AHL and AXG contributed substantially to conception and design; AAA, JM, AHL, and AXG contributed to acquisition of data, or analysis; AHL and AXG agreed to act as guarantor of the work (ensuring that questions related to any part of the work are appropriately investigated and resolved). All authors involved in interpretation of data, drafted the article or revised it critically for important intellectual content, and gave final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Amit X. Garg received an investigator-initiated grant from Astellas and Roche to support a Canadian Institutes of Health Research study in living kidney donors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible by infrastructure support from the Lilibeth Caberto Kidney Clinical Research Unit. This study was supported by the Institute for Clinical Evaluative Sciences (ICES) Western site. ICES is funded by an annual grant from the Ontario Ministry of Health and Long-term Care (MOHLTC). Core funding for ICES Western is provided by the Academic Medical Organization of Southwestern Ontario (AMOSO), the Schulich school of Medicine and Dentistry (SSMD), Western University, and the Lawson Health Research Institute (LHRI). The research was conducted by members of the ICES Kidney, Dialysis, and Transplantation team, at the ICES Western Facility, who are supported by a grant from the Canadian Institute for Health Research (CIHR). The MOHLTC is the provider of large administrative datasets to which the Trillium Gift of Life Network dataset is linked. The opinions, results, and conclusions are those of the authors and are independent from the funding sources. No endorsement by ICES, AMOSO, SSMD, LHRI, CIHR, or the MOHLTC is intended or should be inferred. Parts of this material are based on data and/or information compiled and provided by Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed in the material are those of the author(s) and not necessarily those of CIHI. Ngan N. Lam was supported by a KRESCENT New Investigator Award. Amit X. Garg was supported by the Dr. Adam Linton Chair in Kidney Health Analytics. Alvin Ho-ting Li was supported by a CIHR doctoral scholarship.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.