
Abstract
Introduction
In many jurisdictions internationally, distributed networks of clinical care have emerged as a planning principle to meet the needs of rural communities. Such networks rely on productive relationships between small rural sites and larger regional centres as the mechanism for training and backup and as the pathways for transfer when triage to a higher level of care is required. This paper explores the impact of the Rural Surgical Obstetrical Network (RSON) initiative on regional relationships between networked sites in order to provide data on the efficacy of networked models of healthcare. Implementation of networked care may ultimately lead to better patient care.
Methods
This qualitative study involved interviews and focus groups over 4 years with 169 rural healthcare workers and hospital administrators at different RSON sites. Data was analysed inductively using thematic analysis.
Results
Findings revealed three primary areas considered in the context of RSON funding: improved relationships (primarily through clinical coaching and the consequent building of reciprocal trust) and increased regional coordination of patient care through more efficient triage pathways and increased involvement of specialists through outreach care in rural communities. Continued lack of engagement with regional specialists was reported by a minority of participants.
Discussion
RSON provided a supportive infrastructure that benefitted both rural and regional services namely through funding for clinical coaching and quality improvement initiatives which enabled overall improved provider relationships between sites. This strengthened a regional approach to optimal patient care that should be supported on an ongoing basis.
Keywords
Introduction
Health planners and decision makers increasingly recognize the need for distributed models of health services to enable care ‘closer to home’ and optimize the health outcomes of rural populations. 1 Additional motivation comes from ensuring patients at risk for poor outcomes receive ‘the right care, in the right place, at the right time.’ 2 (p.1) In response, there is emerging evidence on how to facilitate this decentralization, sometimes described as a ‘hub-and-spoke’ model, 3 (p.25) other times, ‘networks’ of care. 4 (p.22) Qualities of this model include establishing a centralized service that provides specialized care and satellite ‘spokes’ 3 (p.25) for lower acuity, local care. It involves ensuring an appropriate level of care is available to meet smaller site needs and is enabled by efficient transport from the smaller to the centralized sites for higher acuity patients. 5
British Columbia's Rural Surgical and Obstetrical Networks (RSON) initiative is predicated on such a distributed model to support rural surgical and obstetrical care. Through a series of funded system interventions including support for clinical coaching, continuous quality improvement (CQI), remote presence technology and increased scope and volume,
6
the networks aim to stabilize local care through collaborative bi-directional leadership within a regional planning framework. RSON recognizes and supports naturally occurring alliances between the sites, drawing on previous work which suggests, Networks of health service delivery are not a new construct, based as they are on appropriate triage from low-resource levels of care (typically rural) to secondary and tertiary care (typically large urban centre), and the attendant socio-professional relationships involved in such healthcare transitions. Rural communities in Canada have depended on and thrived within these networks.
7
However, the relationship between specialist surgeons and FPESS has been a complicated one. Although FPESS rely on their specialist colleagues for consultation and backup as well as skills training and mentorship, there has historically been concern from specialists regarding FPESS practice, specifically regarding outcomes in low-volume programs and the training and continuing professional development required to provide safe care in such settings. 9 The pressing challenge, then, becomes one of building regional relationships between generalists and specialists based on mutual respect for their respective contribution to the network of care.
The accrued advantage of regional clinical networks does not lie solely with rural physicians, however; from a systems perspective, providing high quality, safe care in rural settings also benefits regional centres by alleviating surgical backlog and allowing specialists to focus on higher complexity cases. 10 This ultimately results in the regional coordination of patient care, reduces the need for patient travel and facilitates more expedient access to specialist care. 3
There is scant evaluation data on the implementation of regional clinical networks, particularly through a rural lens. This study considers the capacity of RSON strategic interventions (explained further below) to support and enhance such networks with particular focus on the effects of the RSON initiative on regional relationships. Documenting these outcomes is an essential part of understanding how to enhance rural-regional clinical relationships, and subsequently, improving the sustainability of rural surgical sites in meeting community needs.
Methods
Background
The foundational, organizing structure of the RSON initiative is the creation and maintenance of robust clinical and administrative relationships which coalesce into health service delivery networks. Networks in this instance are defined as the intentional collaboration of entities within healthcare delivery (between rural sites and regional and tertiary centres, interprofessional networks within communities and peer networks across communities) working together to achieve the common goal of improved surgical and obstetrical health services. They are predicated on optimizing health outcomes through increased efficiency and enhanced learning and have emerged as a viable health service delivery option. 4
The RSON initiative was predicated on evidence which demonstrated that increased efficiency, enhanced learning, better client services and improved ability to address challenges are effective mechanisms to solve complex social and population health issues.4,11 These strategies are actualized primarily through taking advantage of both increased resources and human capacity. 12 Further, the inherently decentralized nature of networks was deemed congruent with the distributed nature of rural health services 7 and recognized to be an effective structure to stabilize local rural services. This was particularly relevant in the case of local access to maternity care, as in the past two decades, British Columbia, like other jurisdictions in Canada and internationally, has seen an increasing centralization of maternity care in larger communities, 13 despite growing evidence on the maternity care needs of rural families and the desire for care as close to home as possible.14,15 This is built on consolidated evidence regarding the health, psycho-social and cultural consequences of not providing this care.13,16
Alongside the emergence of ‘networks’ as a solution to address decentralized care across or within regions, there has been growing evidence on enablers of network development,17,18 including the role of mentorship and coaching,17,19 the importance of clinical support from regional specialists, 18 and improved regional management of patients. 18 It has been well-established that trust is an essential precursor to the relationships that underscore a robust network infrastructure,7,17 alongside contextual awareness of each practice site 20 and opportunities to work together in-person. 21 Strategies to facilitate relationship development focus on mentorship and coaching 17 and emphasize the importance of clear communication 17 including virtual communication to mitigate geographical distances. 21
There is also growing evidence on the output of clinical network function, including reduced referrals to regional centres and improvements in the quality of referrals, 18 underscored by what Huxham and Vangen refer to as ‘collaborative advantage’ for issues that could not otherwise be addressed in silo. 22 (p.3) Further benefits include resource leveraging, shared risk, increased efficiency, increased potential for innovation, capacity building and shared accountability, among other attributes. 23 Regional networks which enhance connectivity between rural sites and regional referral centres have also been found to optimize the successful recruitment and retention of rural providers. 24 Alongside evidence of network efficacy, however, are indications of known challenges to network development, namely developing trusting relationships, 25 the potential for power imbalances across network sites 26 and challenges of sustainability. 27 Rural-specific literature cites further barriers including lack of understanding of rural context 20 and limited inter-site access to information including difficulty in accessing patient data due to technological incompatibility between sites. 21
The emergence of RSON in British Columbia (BC) provides a valuable opportunity to assess the output of network function against the premise suggested in the growing body of evidence. We specifically focused on changes to regional relationships as these underscore the clinical capacity of small rural sites.
This qualitative study is part of a larger investigation into the efficacy of the RSON initiative. The larger study involved the quantitative analysis of health outcomes, qualitative analysis of process measures, and cost consequence analysis of the intervention to comprehensively determine value. From this broad dataset, regional relationships between specialists and local RSON providers emerged as a meaningful thematic category.
Settings and participants
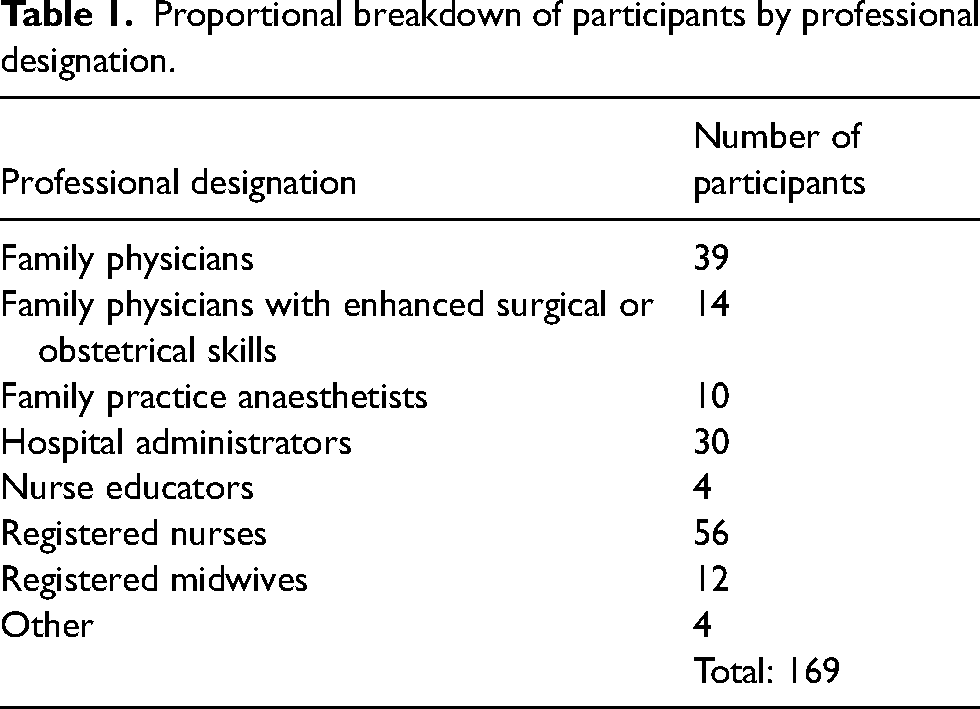
Over the course of the RSON initiative, 169 participants contributed their voices to the evaluation of the RSON project. Initially, the RSON project included eight rural communities across BC, though three additional communities joined the program after the initial start date. Participation in the study was voluntary and open to all members of the hospital team. Participants included local community coordinators, Family Physicians both with and without Enhanced or Obstetrical Surgical Skills (FP-ESS or OSS), Family Practice Anesthetists (FPAs), registered nurses (RNs), health service administrators, medical device reprocessing technicians, operating room managers, midwives and booking clerks. Although we recognize the central role of team-based care in sustaining health services, this manuscript focuses on proceduralist physicians. Participating communities were chosen by Health Authority decision makers based on a need to stabilize local services and the perceived advantage the RSON interventions held for the community.
Data collection
Data was collected through 143 individual interviews and nine focus group interviews (2–3 participants each) over the length of the project (February 2019 to May 2022). A proportionate breakdown of participants’ professional designations is presented in Table 1. Participants could choose between an individual interview or a focus group interview, with both data collection methods occurring simultaneously. Interviews were conducted in person when possible or over Zoom videoconferencing software. Both were facilitated by the principal investigator (JK) in collaboration with a research assistant. Oral or written informed consent was received from all participants prior to the interviews. All participants granted permission for audio recording. Interviews lasted between 30 and 60 minutes, with most extending to 60 minutes. Although we observed data saturation before the end of the study, we continued to interview to ensure we captured nuances and changes over time and between communities. Recordings were transcribed by an external transcription agency and underwent a thorough process of anonymization as well as quality assurance to ensure accuracy. Interviews and focus group transcripts were then moved into aggregate data for analysis, as there was no discernable difference between data gained in each approach. The study was conducted in accordance with the guidelines and regulations of the University of British Columbia's Behavioural Research Ethics Board (Ethics #: H18-01940).
Proportional breakdown of participants by professional designation.
Data analysis
Data analysis was guided by the methodological process of thematic analysis. 28 Researchers achieved familiarization with the data through multiple readings of the interview transcripts, as well as listening to the audio recordings to ensure quality of the transcripts. Through immersion in the data, researchers identified regional relationships as a meaningful thematic topic. Once identified, two members of the research team inductively coded the relevant text using NVIVO 12 software, breaking down ideas and concepts observed in the data into further discrete categories, or ‘codes’ to create a codebook. Each researcher developed an independent coding framework, grouping-related codes together and nesting them into broader overarching categories. 28 Following this step, the two codebooks were then compared; a high level of congruence was found between the two codebooks with only semantic differences between them. The merged codebook was then applied to the entire dataset.
Sub-themes related to ‘regional relationships’ were generated iteratively as the codebook was applied to the transcripts. Further steps included grouping, comparing and connecting how codes relate to others, and searching for overarching ideas and meaning within the dataset concerning regional relationships. The themes were developed directly from the data as opposed to being derived from an external theoretical framework.
Methodological rigour
Given the central role of researchers in generating themes and developing the analysis, researchers engaged in reflexivity, the process of critically reflecting on their own positionality and background so as to mitigate potential bias. Researchers were intentional in their ‘persistent observation’ of the data, repeatedly checking work against the dataset through the analysis to ensure accuracy of interpretations. In addition, researcher triangulation was used during codebook development in order to improve the credibility of the codebook and reduce over or under emphasis on any one theme. Each of these quality strategies was employed to improve the methodological rigour of the qualitative thematic analysis.
Results
Over the 4 years of the study, a total of 169 participants were interviewed. Study size was based on a convenience sample, with all RSON sites represented.
Findings from participant interviews revealed three outputs of the RSON funding in the context of relationships with regional referral centres: improved relationships, continued lack of engagement and the emergence of strengthened regional coordination of patient care. Although in some study sites all care team members engaged in relationships with their regional colleagues, the focus of this paper is physician proceduralists. The themes noted are explicated below in more detail.
Improved relationships with regional referral centres
Participants identified clinical coaching as the primary mechanism through which they improved relationships with specialists in regional referral centres. This was due primarily to the reciprocal trust that was gained through increased access to clinical coaching opportunities and the consequent increased comfort in reaching out for clinical support.
Clinical coaching
Although the explicit objective of clinical coaching in the RSON initiative was to provide infrastructure support for specialists to aid in skills development for rural surgical and obstetrical providers, a secondary motive was to improve relationships between the provider groups due to increased communication and shared time on task. Most participants noted that relationships ‘improved significantly’ and as trust and confidence in and by each party evolved, the nature of the coaching and skills development deepened. An immediate positive consequence was the increased access to regional specialists by the rural proceduralists (‘[we] can call at any time’, ‘…now when I pick up the phone and talk to them they know who I am’ FP- ESS 001). Another participant described a WhatsApp group being created for physicians in their Health Authority by a regional specialist who ‘made herself available for questions and for discussion and updates’ (FPA 001, Focus Group Interview).
There was additional benefit for those who were not directly coached, either locally or in referral centres, through peer-to-peer sharing of knowledge gained by one practitioner: She comes back and works with us and we do peer coaching in the operating room… none of us are shy about asking for help and whatever expertise she picks up in [referral centre] in terms of techniques and methods, she's able to transfer to us. And so we keep connected that way. (RN 001)
A larger, more pervasive outcome was the incremental improvement in the overall relationship leading to increased acceptance of enhanced surgical skill more generally. As one participant noted, [T]he general surgeons that we…would occasionally send people to maybe didn't agree with GP's doing surgery but they tolerate[d] it… And through the coaching program…our relationship with [the doctors] is much stronger because of it. (FP-ESS 001) He's like do you need any help? I’m like yeah, I need to manage his blood pressure, can you start the ART line? Like just tag teaming type stuff. And I don’t think that would have been possible 10 years ago. Their department is… quite lovely now. I love [doctor]. [They] are hilarious. And [name]'s the one who sent me a one-liner email rejecting my offer to help 5 years ago. And now they all smile, thank me for coming, all the surgeons are quite happy to have me there. Lovely. (FPA 002) I’ve talked to [the specialist] and said ‘I don’t think this patient should be done here’ and they are like ‘that's absolutely no problem’. There's no concerns. I think there's complete support from our surgical colleagues. (FPA 003)
Building trust
Improved relationships based on clinical coaching (‘shoulder-to-shoulder’ or through virtual technology) led to increased trust between FPESS/FPAs and specialist physicians, primarily through the mitigation of specialists’ concerns about the capabilities of FPESS. This was often based on direct observation in learning scenarios (‘[We] went to [the regional referral centre] and did a couple of [cesarean] sections with them and they’re like, “Okay. I see you can do sections. That's excellent”’ FP-OSS 002). The accrued trust was seen by some to be the precursor for increased respect, which many noted to be lacking prior to RSON: The relationships were very poor [in the past] and there was a lot of misunderstanding about roles or some very marked negativity towards us. And that's substantially changed and it's just a matter of hard work and going down there a lot and talking to people. …It's been a huge turnaround in attitudes and acceptance of what we do and what they do and that's a relationship that, again, it's good. It's improving. (FPA 004)
Continued lack of engagement
Although most participants noted improved relationships through clinical coaching, a minority of participants reported experiencing continued resistance to FPESS/FPA practice in rural sites and the attendant lack of availability of referral specialists. Some felt this was rooted in urban-based perceptions of what Family Physicians do – and don’t do – including surgery. This resulted in situations where rural providers ‘[didn’t] feel all that welcome’ in referral centres. Many felt that this requires a ‘shift in Health Authority culture’ to overcome some of the ‘stigma’ that has existed historically. Other participants referred to the historical precedent of having patients travel to bigger centres for care (‘The mindset is still very much “we are the regional centre, this is where the majority of surgery happens”’ Family Physician 003). As one participant said, ‘You know, it's about that shift, you know we are players in the system. We can support the larger system, we are part of the team’ (Site Administrator 001). Some noted that the ‘stubborn pushback’ to this cultural shift has been frustrating, while others noted it will require educating referral specialists about the training of and need for rural FPESS (‘[W]ho else is going to do it, right?’ FP-ESS 004).
Several participants saw the root cause of the lack of acceptance resting in the need for regional procedural volume. Some were told by specialists that if they supported rural surgery, the regional program would ‘collapse’. Nevertheless, other participants noted that over time, concerns over volume scarcity have lessened in light of the recognition that regional referral centres could sustain their own programs alongside support of rural programs. Others pointedly observed that their relationship wasn’t strained, but instead there was ‘a little bit of a disconnect between how we see each other, and what our sort of hopes for the future are’ (Family Physician 003). This led to some participants advocating for a ‘careful, diplomatic approach’ in their relationships to facilitate change over time.
Need for stronger relationships
Participants expressed that the antidote to the challenges with regional specialists experienced by some rested in developing stronger relationships with their regional referral centres which in turn were a necessary precursor for robust backup and consults, as well as coaching opportunities for rural providers. Many thought these relationships were essential to improve the organization and communication between sites and also to obtaining more procedural skills locally to meet community need for services. Mentorship and maintenance of skills was a primary desired output of these relationships.
Regional coordination of patient care
A consequence of improved regional relationships for some RSON sites was increased participation of visiting specialists to expand the scope and volume of local procedural care. In some instances, this involved specialists opening satellite offices in the community, but a more common approach was regularly scheduled bi-weekly or monthly visits by specialists to work in the operating room and do follow-up post-operative care. Although this had occurred prior to the RSON initiative, many participants noted that the availability of additional funding for increased scope and volume facilitated both specialist involvement from diverse communities and enhanced procedural scope.
In many instances, specialist support for increased local care was reciprocated through rural physician assistance when health human resources were compromised in the referral centres: ‘We went to help them through a rough spot there. They didn't have any staff, and so we kept going’ (RN 002). Another participant noted, We've had a couple times where we had patients who were supposed to be labouring or induced or something. [The referral centre] was so busy. They couldn't take them, so we took them. So, there's a little bit of that going on right now. (FP-ESS 004)
Despite the growing inter-site relationships, however, most participants noted the need for increased frequency of visits and an expanded local scope of care. Barriers to achieving this included geography: that is, the distance between sites and sometimes challenging travel conditions in rural British Columbia. As one participant noted, [W]e’ve offered them OR space and tried to recruit people to come up and do outreach programs here. But I think the problem is that it's a long ways away for somebody to want to drive for three and a half hours to come up for an OR day. So I understand that [for] people with families it's a hard sell. I mean, we’re quite isolated here as, as you know, it's geographically a bit of a hard area. (FPA 005)
Other participants perceived that specialist availability was a bigger obstacle than distance. Although there was operating room availability in the rural site, participants recognized how much travel the specialists were already doing: ‘We could offer more. But they can’t travel more. They're really being stretched quite thin’ (FP-ESS 006).
Some participants identified challenges in the coordination of patient booking and referral processes as a barrier to specialist efficiency. Scheduling and balancing specialist slates became a complex task that often fell to over-stretched patient care coordinators at rural sites rather than being an established process at the regional service coordination level. This led to occasional underutilization of specialist time and acted as a barrier to specialist engagement.
For sites more proximal to their referral centres, challenges to increased specialist involvement were rooted more in limited physical and health human resource infrastructure in rural sites, specifically availability of equipment to facilitate surgeries. This was particularly salient for orthopaedic surgeries but extended to laparoscopic equipment as well. As RSON funding became available for sites to update equipment, this problem diminished. Participants reported that access to additional equipment became a significant enabler while challenges with distance and specialist capacity continued to be limiting factors.
Access to tertiary centres
Despite usual referral patterns to regional referral centres for most cases, some participants noted preferential access directly to tertiary centres, particularly when they had a pre-existing relationship due to previous education and training with that centre. So like with the trauma example, if you phone Vancouver General Hospital because you have a bad trauma case and someone that… you've been doing sim education with for the last two years picks up the phone, it's amazing… So we are actually in networks with them. (FPA 006)
Out of town patients
Several participants noted that regional networks of care involved not only specialists coming from larger centres to smaller rural sites but also their patients travelling for more expedient care than available in their home communities. One participant described their site as …being the overflow for the smaller procedures that are bugging up the OR for other bigger procedures or, or more serious procedures that need to be attended to right away. We kind of are that overflow site so with all the other surgeons coming in, it's been really great. (Administrator 002)
In these instances, visiting specialists not only provided care to the local population, but also patients with them. This has the added advantage of increasing procedural volume at rural sites which further stabilizes the rural operating room by providing more experience for the OR team. This balance was noted by several respondents as essential to optimizing functioning services.
Discussion
This study set out to understand the capacity of the RSON system interventions to support and enhance regional networks of care, with the assumption that these networks will enable optimal patient care as close to home as possible. 1 Findings revealed the efficacy of the RSON framework in fostering stronger regional clinical networks, namely through funding for clinical coaching, which led to building trust among providers through the longitudinal relationships that were supported. The downstream effect of this, according to study participants, was improved regional coordination of care; that is, ensuring the right patient, provider and place for procedural care. The benefits accrued reflect existing literature on the advantages of rural health service networks, including the capacity for the optimization of regional planning across sites. This happened most directly in this study through regional discussions on scope of practice and triage, which is reflected in previous work. 17 In addition, the rural exposure of visiting specialists ensured they gained a more fulsome understanding of rural contexts, and ‘mutual awareness of one another's potential.’ 29 (p.30)
Participants in this study overwhelmingly identified improved relationships with regional centres as a key output of the RSON initiative. This led to increased comfort in reaching out for clinical support and increased access to specialists and nurses which resulted in downstream benefits to patient care. Most participants also pointed out increased support for FPESS as clinical trust increased between the provider groups. This reflects findings from other clinical network evaluations. 2 The accrued advantage of regional clinical networks does not lie solely with rural physicians, however; from a systems perspective, providing high quality, safe care in rural settings also benefits regional centres by alleviating surgical backlog and allowing specialists to focus on higher complexity cases. 10 This ultimately results in the regional coordination of patient care (as noted by respondents in this study), reduces the need for patient travel and facilitates more expedient access to specialist care. 3
Ultimately, the vision of solving the challenge of rural access to surgical services depends on shifting thinking about service provision ‘from a series of isolated problems to the realm of collective responsibility’. 30 (p.104) This not only creates the theoretical underpinnings for clinical networks of care across rural geographies, but also opens the door to a more expansive understanding of departments of surgery or obstetrics in regional centres to include adjacent rural sites. Many benefits are associated with supportive relationships between rural and referral hospitals, for example, mobile health human resources from rural sites that can contribute to staff shortfalls at larger centres. This was recognized as an unanticipated advantage of RSON by participants in this study. This geographically fluid approach allows for more agility and flexibility in dynamically meeting local needs, but must be predicated on autonomy in decision-making for both sites, underscored by robust relationships between healthcare providers.
This study allowed us to dig deeper into the stressors on regional relationships, stressors that if unresolved, will pose significant challenges. We heard from participants about instances of challenging relationships between rural FPESS providers and regional specialists, due in part to what participants described as the regional need for procedural volume and the attendant belief by specialists that care in rural sites diminished this potential. When unaddressed, other jurisdictions have reported that these challenges resulted in fragmentation of care. 31 The current study revealed that over the course of the RSON initiative, concerns over volume scarcity had lessened based on observations that regional centre volume had not diminished despite the increase in rural procedures. It was also noted that even when relationships were productive and based on a shared commitment to best patient care, the reality of outreach care was challenging for some due to travel distances and conditions (particularly in winter months) and the lack of availability of specialists due to clinical commitments in the regional centres and other rural sites.
An additional contribution to the current literature is recognition of the importance of a funded position for CQI. Beyond clinical coaching, a half-time CQI position at each site and funding to complete locally identified CQI projects supported quality improvement and the robust evaluation of health outcomes during the RSON initiative. This indirectly contributed to relationship building through addressing known concerns. Additionally, CQI-related opportunities for building regional relationships between providers also led to the development of informal and highly beneficial quality improvement networks between sites. Often spearheaded by local maternity and surgical nurses, informal bridges contributed to distributed knowledge surrounding innovative QI projects across sites. Successful regional collaboration was demonstrated through joint projects such as the multi-site development of a maternity skills comfort assessment tool, designed to meet an identified need at rural maternity sites.
An undercurrent of network development is ensuring availability of resources to maintain supportive activities which contribute to the valuation of clinicians’ time, that is, to remunerate all those involved in clinical coaching or CQI to ensure no personal loss of clinical income occurred, provide meals at education days and working lunches. RSON participants also noted the benefits of funding to support, for example, expanded operating room days for specialists at the rural sites, additional equipment where necessary and additional nursing lines. 7 This funding allotment was essential to build the regional infrastructure necessary to stabilize and support rural surgical and obstetrical care, but, as Luiza et al. point out, is successfully activated by institutional leadership that engage as ‘agents of change’. 31 RSON champions included local administrative leaders, who facilitated effective working groups and advocated for their local teams on regional committees. Continued RSON successes such as increases in site volumes to address regional backlogs and the stabilization of local services, subsequently allowed administrators to further support their teams at the regional level.
This evaluation revealed significant benefits to the RSON interventions that directly and indirectly resulted in improved patient care due to improved regional coordination. This output was predicated on improved relationships between rural communities and regional referral centres and laid the foundation for a shift to conceptualizing the inter-connected nature of regional procedural care.
This evaluation was carried out over 5 years, which allowed longitudinal engagement with the communities and participants. The funding itself arose from previous engagement by the research team with the communities to thoroughly understand the issues at hand in order to co-create effective and restorative system interventions. Repeated annual fieldwork visits, in addition to the enduring historical relationship and the multidisciplinary nature of the research team (representing rural health services researchers and rural healthcare providers) provided a rigorous foundation for this work. Additionally, internal triangulation was possible due to the participation of discrete communities, which provided richness to the thematic development.
Limitations included the potential for interview fatigue due to the participant burden of the annual interviews, particularly towards the end of the study. This was not evidenced in the number of annual interviews achieved, however, as it remained constant throughout the study. A more significant limitation was the occurrence of the COVID-19 pandemic during the course of the study. These necessitated virtual interviews which, although built on a strong relational foundation, did not allow situational awareness and the reading of body language in the same way face-to-face interviews do. More pertinently, however, was the clinical burden of dealing with the pandemic at the small rural sites, and the emotional toll on the participants. This translated into both less time availability for many individual participants and a focus during the interviews on the impact of the pandemic on site sustainability. However, we worked these data into an understanding of how the interventions could contribute in times of health service delivery stressors.
RSON provided a supportive infrastructure that benefitted both rural and regional services, namely through funding for clinical coaching and quality improvement initiatives which enabled overall improved provider relationships between sites for all members of the healthcare team. Ultimately, this strengthened a regional approach to optimal patient care that should be supported on an ongoing basis by establishing a regional infrastructure and involving all sites providing care, including patients’ home communities, in determining the best location for procedural care on a case-by-case basis. This communication infrastructure would greatly improve organization and planning.
Footnotes
Acknowledgments
The authors gratefully acknowledge funding for this work from British Columbia's Joint Standing Committee on Rural Issues and support and collaboration from the Rural Coordination Centre of BC. We are also grateful to Audrey Cameron and Payal Parti who contributed to background literature and manuscript preparation.
Author contributions
The first author (JK) led all aspects of this work including data collection, analysis and writing. All authors made substantial contributions to the design and analysis. All authors agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tom Skinner is employed by the Rural Coordination Centre of BC (RCCbc) as the Project Manager of the RSON Initiative. The findings reported in this survey are part of the evaluation of RSON. As an employee, his travel to the rural communities was covered because he was supporting hospital teams in implementing the RSON initiative. Dr Sean Ebert received sessional funding from the RCCbc in his role as medical lead for the Quality Improvement Pillar for the RSON initiative. In his capacity as CQI medical lead for the Quality Improvement Pillar, he received funding to travel to the rural RSON communities. Dr Nancy Humber received funding from the RCCbc in her role as a clinical lead for the RSON. In her capacity as a clinical lead, she received funding for travel to the rural RSON communities. All other authors are part of the RSON evaluation team at the University of British Columbia, Canada and have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Joint Standing Committee on Rural Issues (grant number R005415).