
Abstract
The impact of health service access disparities has significant implications for society. The importance of addressing health and social inequities is never more critical than in the early years of a child’s life. Despite advances in healthcare implementation, there is a lack of an evidence-based framework to specifically guide the adaptation of child and family health (CFH) service models for different community contexts. This paper describes the development of a framework for the adaptation of community-based CFH service models. Drawing on the findings of an integrative review and Delphi study, Participatory Action Research was used to test the framework, resulting in the Framework for Collaborative Adaptation of Service Models for Child and Family Health in Diverse Settings (CASCADES). The Framework uses the analogy of a waterfall to represent the iterative process of collecting information to inform each step. The framework supports a collaborative co-design approach to build a comprehensive understanding of the target community to inform the adaptation and evaluation of evidence-based interventions appropriate to the local context. The ultimate aim is to enable the delivery of services that are contextually relevant for local communities and provide greater access to effective, accessible services to support children and their families.
Keywords
Background
The inequities in health outcomes for populations living in less well-resourced communities have been well documented (Commission on Social Determinants of Health, 2008; Nurse et al., 2016). The impact of social determinants of health, and in particular, disparities including access to resources and services for those living in disadvantaged areas, has significant implications for society (Commission on Social Determinants of Health, 2008). Higher levels of vulnerability and exposure to health risks and poorer health outcomes have ramifications for not only individuals, but also for their families and the broader community (Diderichsen et al., 2001).
The importance of addressing inequities in health and social outcomes, while imperative across the lifespan, is never more critical than in the early years of a child’s life (Moore et al., 2017). Research highlights the impact of such inequities on early brain development and the lifelong trajectory of the child into adulthood (Gerlach and Varcoe, 2021; Jeong et al., 2020). Risk factors, vulnerabilities and adverse events experienced in early childhood need to be considered in terms of this critical period of development (Burke Harris, 2019; Commission on Social Determinants of Health, 2008). They have a cumulative effect on the health and wellbeing of the individual across their life course, with implications for intergenerational risk for families, requiring effective support for families and communities to enhance protective factors to prevent or ameliorate such risks (Solar and Irwin, 2010).
Specialist Child and Family Health (CFH) services play a significant role in the provision of stepped-up care through short-term intensive help and support for families experiencing early parenting difficulties (NSW Ministry of Health, 2019). These services build on universal service delivery through comprehensive assessment and service interventions to address complex physical and psychological aspects of wellbeing (Australian Health Minister’s Advisory Council, 2015; Fowler and Stockton, 2021). The services are provided by community-based teams of CFH nurses and allied health professionals, working in a model of partnership with parents to identify child and family-centred goals (Gerlach and Varcoe, 2021), addressing early parenting and psychosocial issues impacting child development, parental mental health and family functioning (Clerke et al., 2017; Fowler and Stockton, 2021).
The World Health Organisation (WHO) has highlighted that effective, evidence-based service models and interventions developed in well-resourced metropolitan settings require adaptation to ensure efficacy for other contextual settings such as rural communities (WHO, 2008). Health researchers and those implementing health service models in differing contexts from which they were developed, have identified the need for contextualisation to inform adaptations responsive to the multifaceted factors which define a local context (Damschroder et al., 2009; Monks, 2016).
Frameworks are often used to support such implementation, as a guide to understanding the ‘why’ and potential ‘how’ of addressing a particular challenge. A framework can be defined as ‘… a graphical or narrative representation of the key factors, concepts or variables to explain the phenomenon of implementation, and… include the steps or strategies for implementation’ (Moullin et al., 2015: 3). They also present an opportunity to enhance our understanding of factors and mechanisms while guiding implementation at a macro level such as policy-making (Solar and Irwin, 2010); and at a micro or local implementation level.
Frameworks collate and enhance understandings of a variety of evidence and learnings at a conceptual level, including influences and factors to be considered when implementing interventions (Moullin et al., 2015). They can also provide guidance on how to assess the fidelity of adapted interventions (Pérez et al., 2015). Some frameworks take the form of toolkits to support practical implementation (Haggarty et al., 2010) while others may focus on elements to guide implementation research and evaluation (Breimaier et al., 2015).
An integrative literature review to examine elements known to strengthen health service systems in rural and remote community-based health services identified the need for community participation in health planning and implementation (Stockton et al., 2021). The findings of the review recognised the opportunities this approach affords in terms of: choosing appropriate interventions for the context (Semansky et al., 2012) and developing innovative contextually appropriate solutions to challenges (Smith et al., 2016). Such an approach can build community capacity and social capital (Chilenski et al., 2014; Smith et al., 2016). Further research is required to understand and guide implementation to enable effective community participation in service design and adaptation (Farmer and Nimegeer, 2014), shifting the power differential to facilitate decision-making by those who best understand their local community (Kenny et al., 2015).
Despite advances in healthcare implementation and implementation science research, there is a lack of evidence-based frameworks to specifically guide the adaptation of service models and interventions for different contextual settings (Movsisyan et al., 2019). The need for such guidance has been identified by the WHO in documents calling for the adaptation of successful service models for implementation in less well-resourced settings (WHO, 2008; WHO, 2007). There is an identified need to develop evidence to provide guidance for effective collaboration in the early childhood field in order to improve systems, services and outcomes for children and families (Chien et al., 2013). This paper describes the development of a framework for the adaptation of community-based CFH service models for implementation in different contextual settings to address this identified need.
Aim
To develop a framework to guide the adaptation of specialist CFH service models for diverse settings.
Methods
The iterative approach through the research stages sought to draw on established literature and the insights of consumers and health professionals, to develop a framework which would support the co-design of service model adaptations in collaboration with local community stakeholders. The framework development incorporated three studies (see Figure 1): (i) a Participatory Action Research (PAR) study in a rural setting in NSW, Australia, to review the fit of an established metropolitan CFH service model for the local context; (ii) a Modified e-Delphi Study to identify elements to be considered when adapting CFH service models for rural and other diverse community settings; and (iii) a second PAR study in a different rural community setting to pilot and refine a framework for the adaptation of specialist CFH service models. The research was informed by an integrative review (Stockton et al., 2021) of rural health service literature to identify examples and gaps in relation to the WHO building blocks for strengthening health services (WHO, 2007). Framework development process.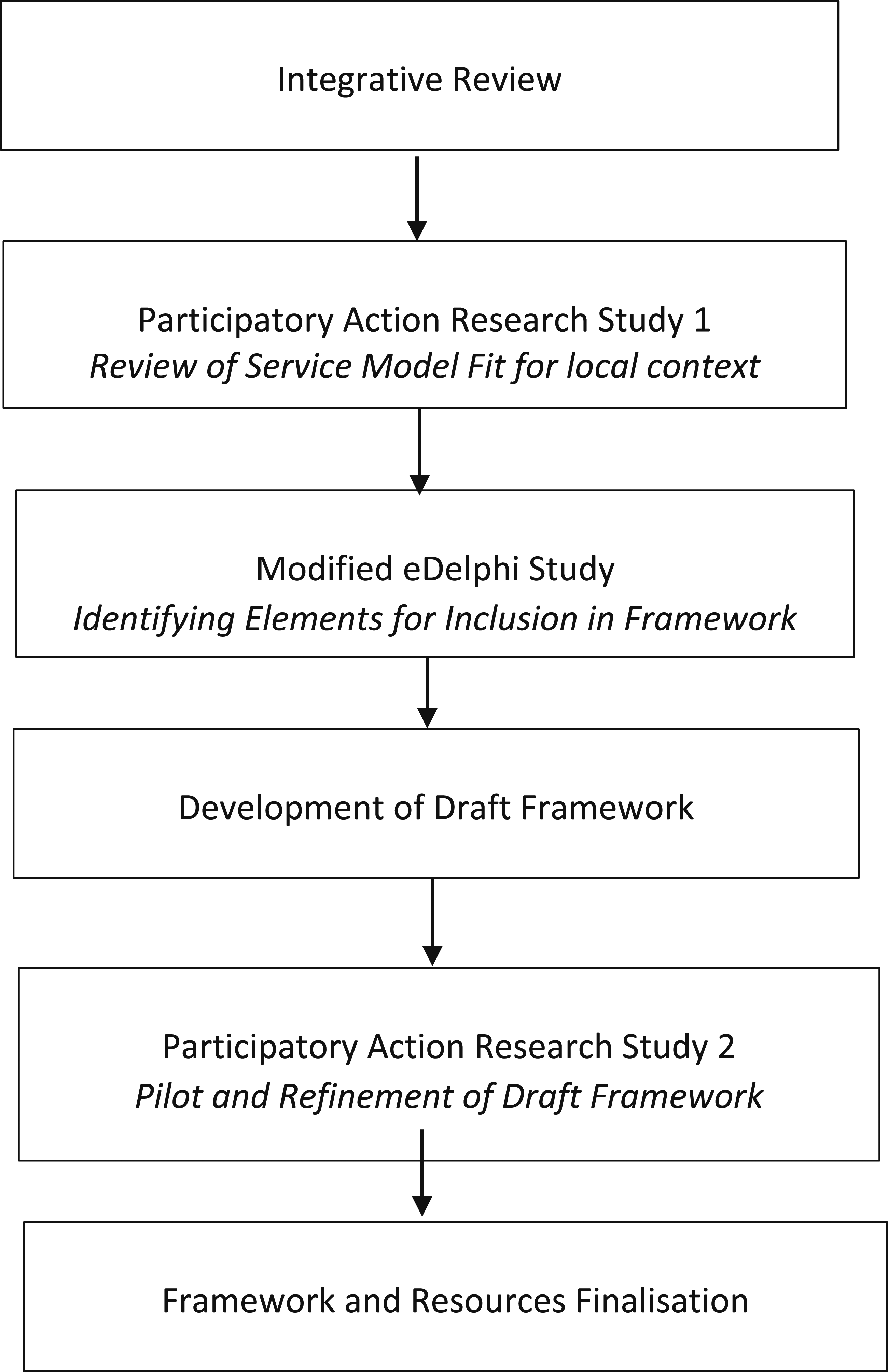
The research was informed by realist evaluation (Pawson and Tilley, 1997), to provide a comprehensive exploration of contextual influences while seeking to understand mechanisms of complex programs, and why they are successful (or not) within particular settings and circumstances (Taylor et al., 2010). The research used to inform the framework development drew upon PAR techniques and a Delphi Study (Rowell et al., 2015).
Participatory action research involves cycles consisting of ‘ask, acquire, appraise, apply and assess’ (Hughes, 2013) to aid the identification of steps of an implementation process (Breimaier et al., 2015). Figure 2 depicts the PAR cycle implemented in Study 1 (centre of figure), noting the addition of the overlay of the draft framework tiers of Context – Outcomes Expected – Mechanism – Evaluation and Reflection (C-O-M-E) piloted with the second PAR group in Study 3. The three workshops conducted to evaluate the framework with the second PAR group were structured as follows: Workshop 1 – Context and Outcomes expected; Workshop 2 – Mechanisms; and Workshop 3 – Evaluate and Reflect. The final workshop included the development of an action plan for a subsequent PAR cycle led by a local health professional to improve access to services for families with young children. The PAR group worked together to identify areas of need and priorities in their community, reach consensus on the outcomes expected of service model implementation, review the proposed service model in light of this information and develop an action plan which incorporated an evaluation strategy. Overlay of draft framework tiers with PAR cycle (Study 3).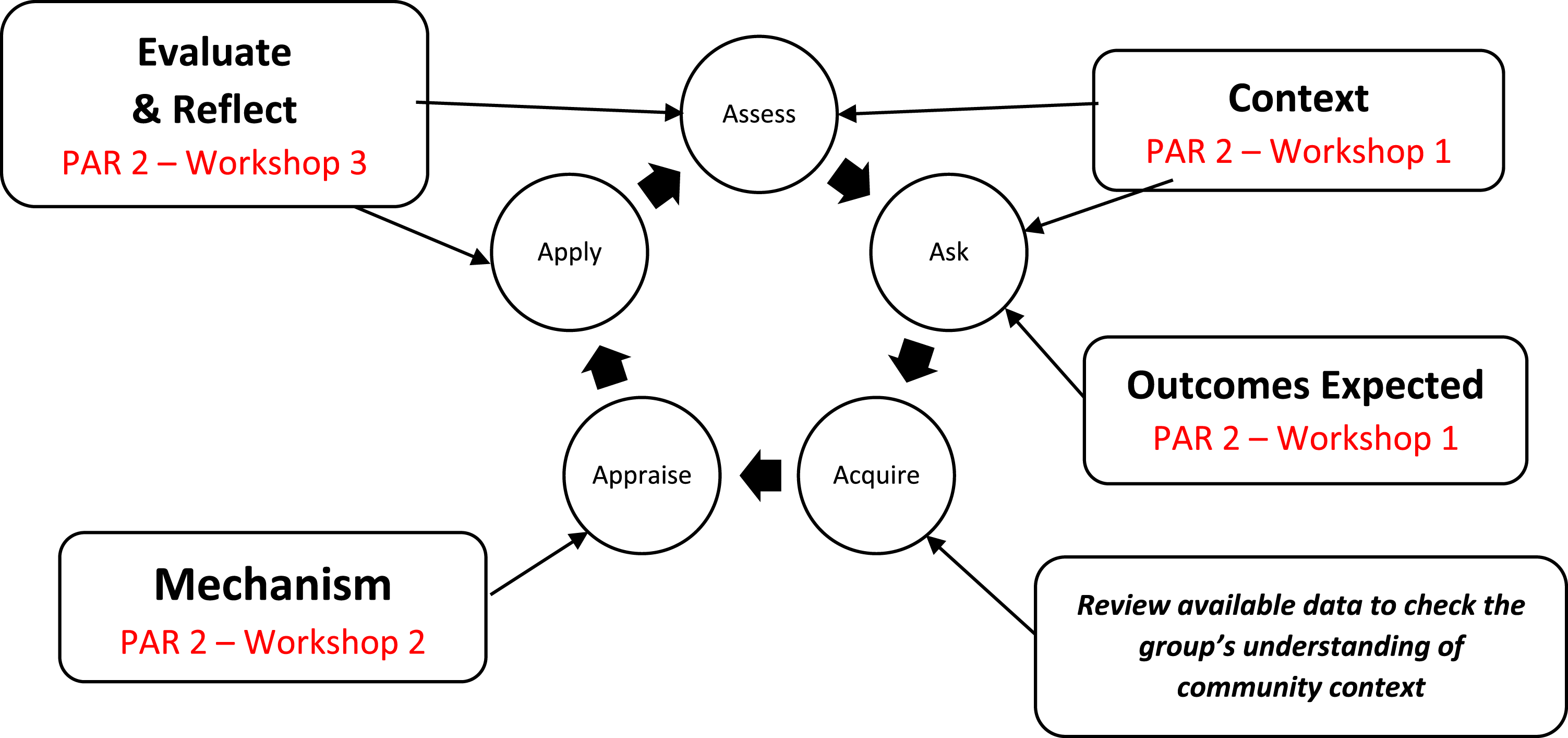
A Delphi study utilises rounds of questionnaires to classify a series of statements in terms of level of consensus among a group, known as an expert panel, who have knowledge and/or experience relevant to the study topic (Hsu and Sandford, 2007). A Modified e-Delphi Study uses two rounds of electronic questionnaires informed by previously obtained data or literature review, rather than three rounds undertaken in traditional Delphi studies (Bryar et al., 2013; Stewart et al., 2017). The definition of consensus used for the Modified e-Delphi Study was a mean score of ≥4 and frequency of scores 4 or 5 of ≥80% for each statement presented to the Expert Panel. A comprehensive description of the design and findings of Study 2 (Modified e-Delphi Study) has been reported in a paper recently accepted for publication (Stockton et al., 2022: in press).
Both PAR and Delphi approaches seek to address power differentials and foster inclusivity (Fletcher and Marchildon, 2014), with PAR participants situated as research partners. Similarly, the Delphi panel participants were from a broad cross section of backgrounds. The PAR groups and the Delphi Expert Panel consisted of consumers, health professionals, health service managers and non-government community-based workers with representation of rural and remote parents and First Nations peoples. This enabled a broad set of experiences and perspectives (Rowell et al., 2015) to generate the framework for application across a range of diverse contexts.
The iterative nature of the PAR cycles (Baum et al., 2006) and Delphi rounds (Toma and Picioreanu, 2016) were reflected throughout the framework process, with each research stage informing the next. The WHO building blocks for strengthening health service systems (WHO, 2007) were utilised as a frame for the PAR and Modified e-Delphi studies, providing a consistent lens through which to identify the key elements required for the adaptation of specialist CFH service models.
Thematic analysis (Braun and Clarke, 2006) of the transcripts of the PAR studies was undertaken. The themes from the first PAR study were collated with the findings of the integrative review (Stockton et al., 2021) to produce a list of potential elements to be considered when adapting CFH services for different contextual settings. The list was formatted into statements and presented to the Delphi Expert Panel. Analysis of the core set of elements identified in the Modified e-Delphi Study was undertaken drawing on the Context-Mechanism-Outcome (CMO) frame (Mitchell et al., 2013). Each element was categorised to inform the logical flow and structure of the framework to provide a robust platform. This approach is consistent with the understanding that CMO refinement can be utilised to ‘… contribute to further cycles of inquiry and, therefore, to ongoing theoretical development’ (Salter and Kothari, 2014: 2).
The draft framework was tested through a second PAR study (Study 3) in a different location, moving from an inland community to a coastal area of NSW. The process provided an opportunity to pilot the framework in a real-life application, while further refining the structure, flow and supporting resources to facilitate utilisation of the framework in various geographic and socio-economic contextual settings.
Results
The first PAR study (Study 1), undertaken with seven participants representing consumers and health professionals, identified six themes when considering the fit of a CFH service model for a specific community context. The themes were (i) ‘what parents want’ which emphasised the need to consider expected outcomes early in the adaptation process; (ii) ‘breaking down barriers’ (to access); (iii) ‘being flexible and responsive’; (iv) ‘real life is messy’ highlighting the need for service models to be reflective of contextual realities; (v) ‘building capacity by working together’ including interagency collaboration and trust; and (vi) ‘service enablers’, including funding to support sustainable service implementation, evaluation and sustainability.
The findings from Study 1 and the integrative review were collated to develop a list of 107 potential elements for consideration when planning to adapt an established CFH service model for a different contextual setting. In the first round of the Modified e-Delphi Study (Study 2), the 12-member Expert Panel identified 80 elements for inclusion in the framework. In the second round, the participants were provided individualised information on the elements which had not reached consensus for inclusion. This included the score the panel member attributed to each statement together with the aggregated results from the group. This review process identified an additional 17 elements to be retained, resulting in 97 elements for inclusion in the draft framework with high rates of consensus reached across all retained elements (SD < 1.0) (Stockton et al., 2022: in press).
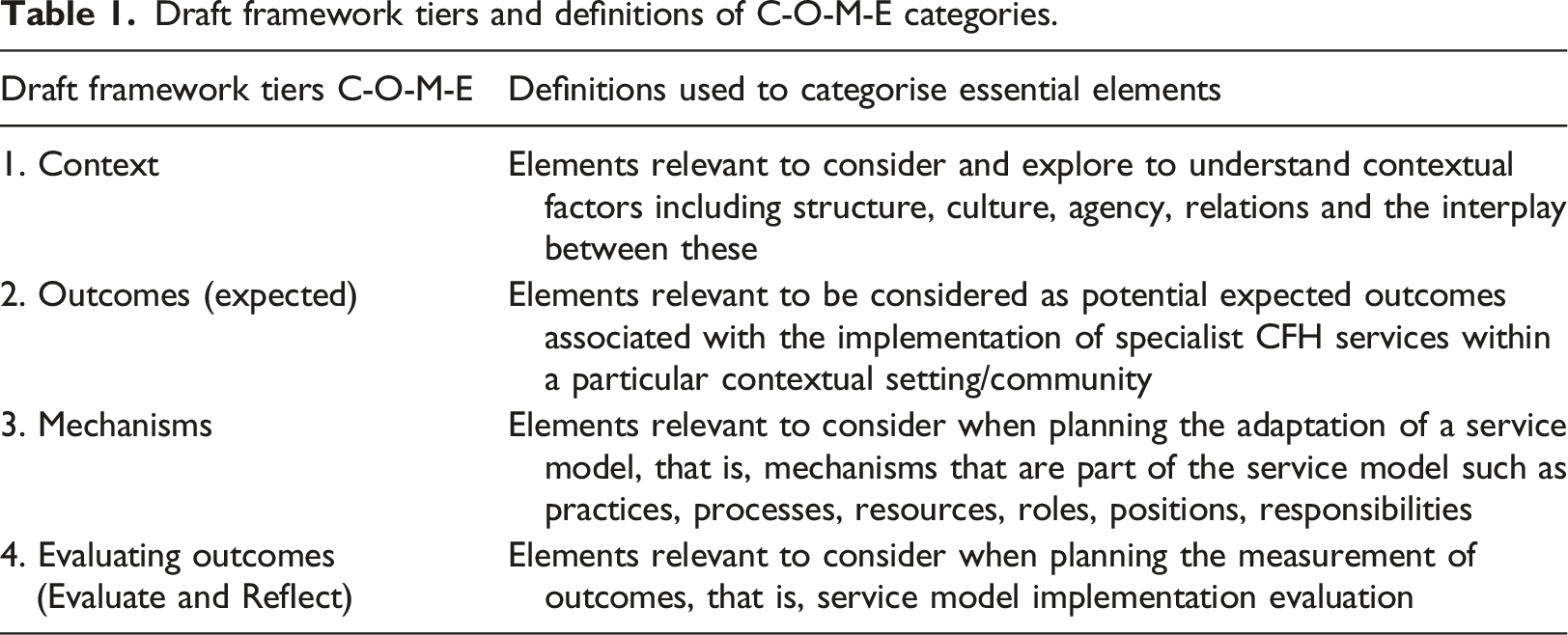
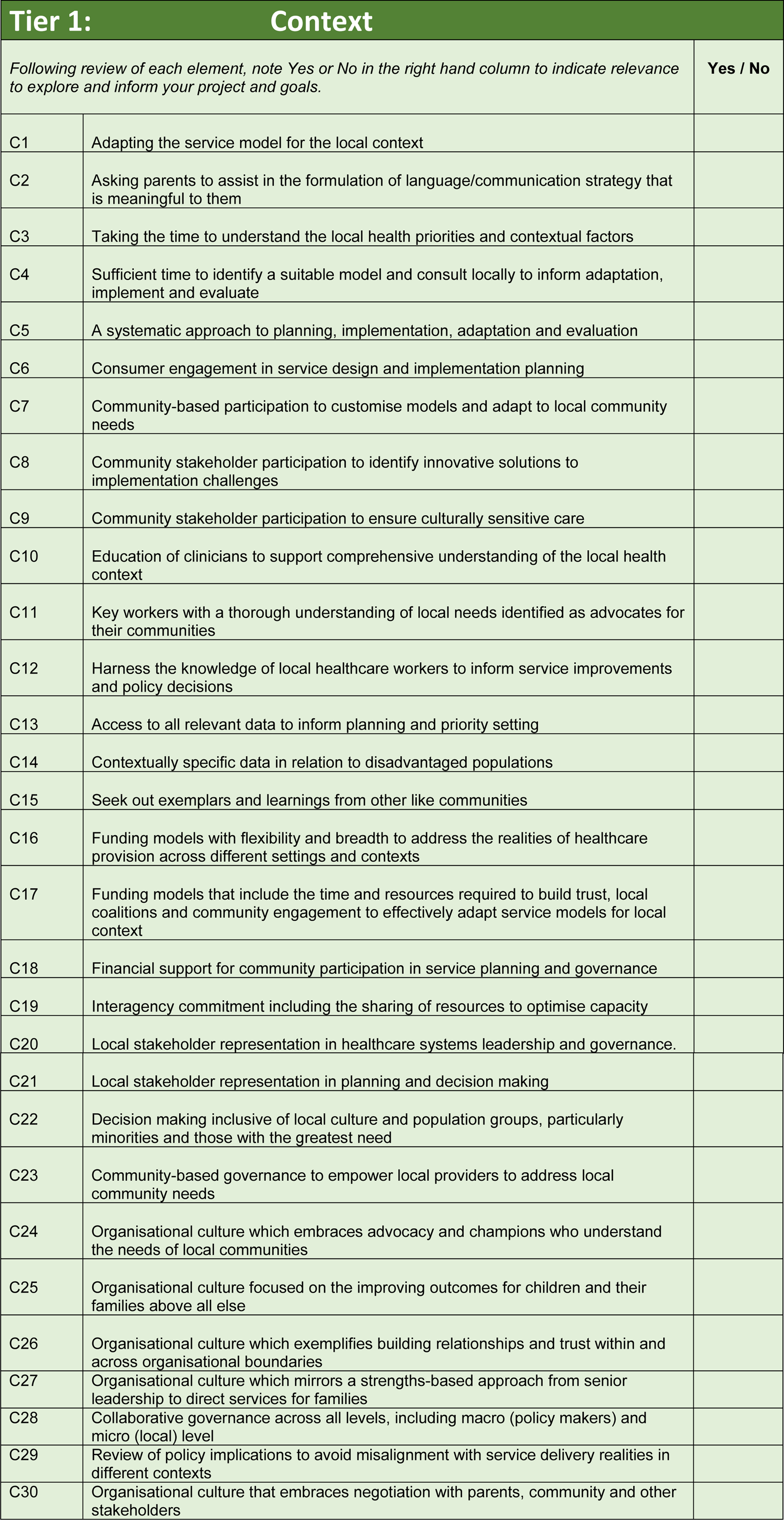
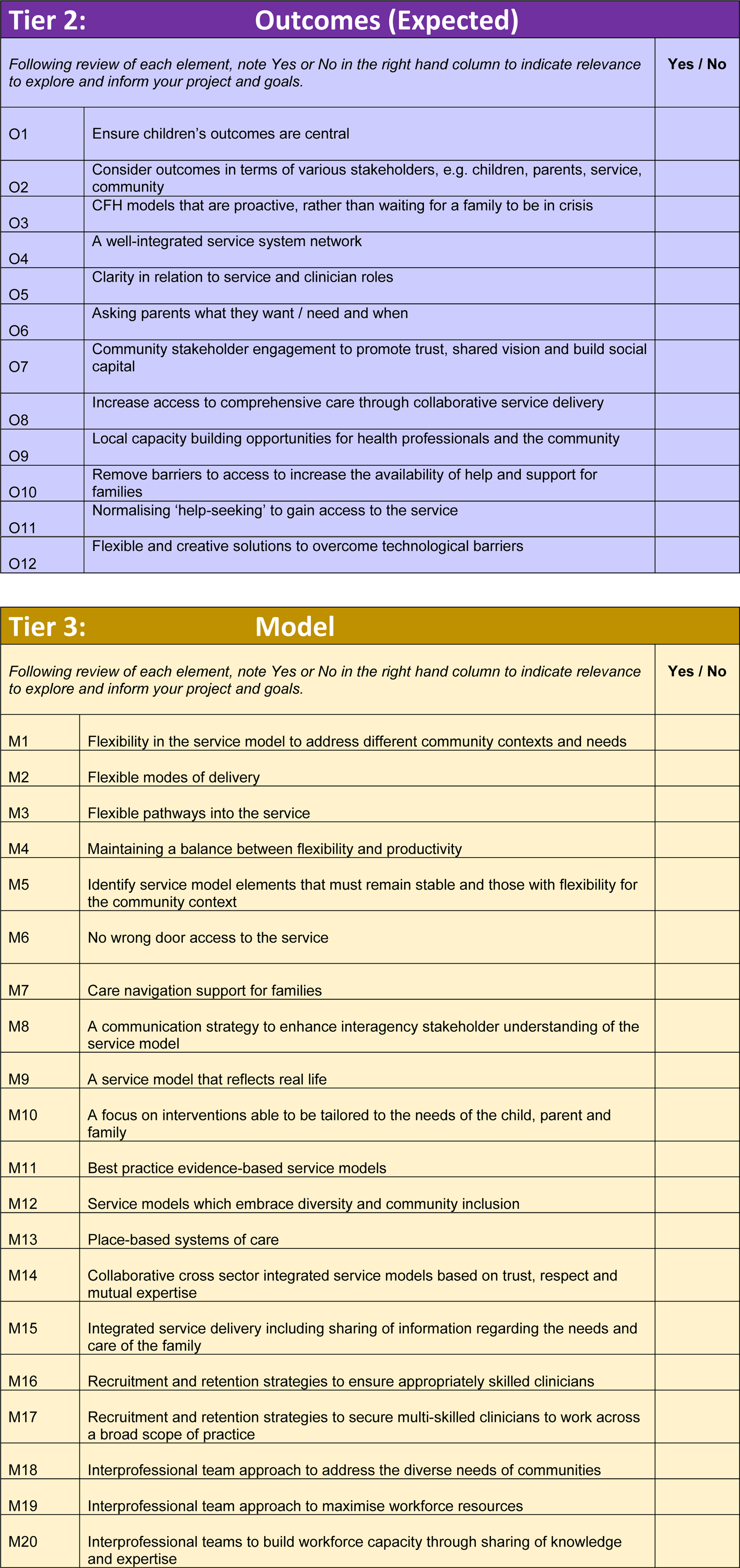
Draft framework tiers and definitions of C-O-M-E categories.
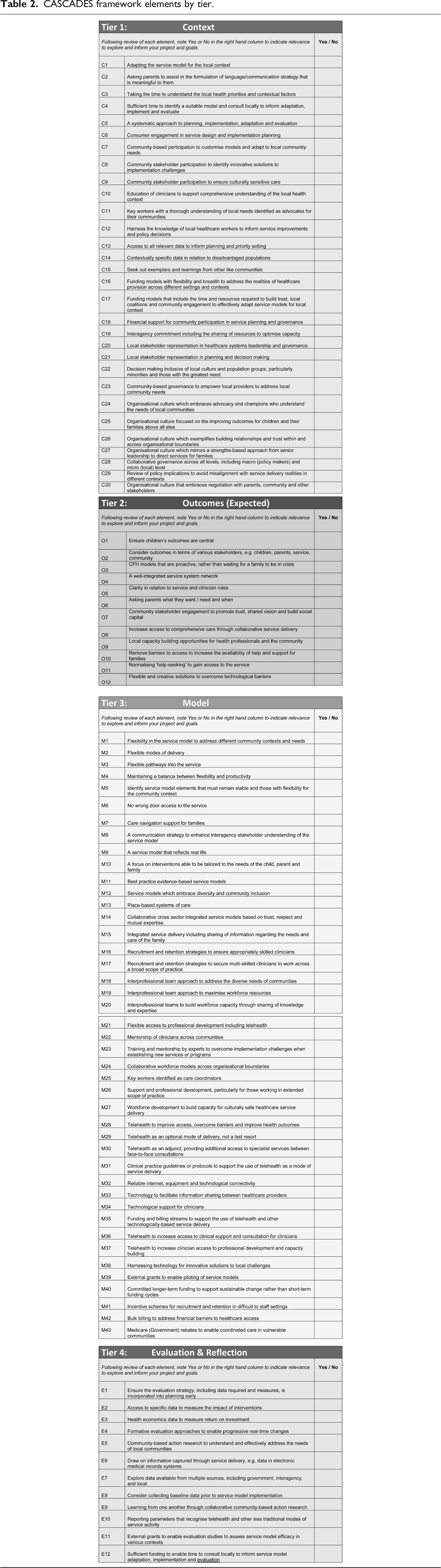
CASCADES framework elements by tier.
In the draft version of the CASCADES Framework, the ‘Outcome’ category was divided into two: (i) expected outcomes and (ii) evaluating outcomes. This approach was in response to a key finding in the first PAR study, which highlighted the need to consider from the outset the outcomes expected or hoped for before considering service model adaptations required for the local context. Specifically, the first PAR group recommended CFH service model implementation groups consider whose lives or experiences will be improved and whether the expected outcomes articulated in an established service model are meaningful for the target population. In light of this, the draft framework was structured to enable focused exploration of the expected outcomes from CFH service implementation once a shared understanding of the community context had been developed. The resulting configuration was represented as Context – Outcomes expected – Mechanism – Evaluating Outcomes (see Table 1).
A total of 13 participants provided consent to participate in the second PAR group which piloted the CASCADES Framework (Study 3). Of these, four withdrew or did not participate in the workshops due to competing professional and personal demands. The nine remaining participants represented stakeholder categories of local clinicians (n = 3), health service manager (n = 1), consumer (n = 1), Aboriginal Health Worker (n = 1), non-government organisation (NGO) community service worker (n = 2) and non-health government department manager (n = 1). Two of the participants (one NGO community service worker and one non-health government department representative) withdrew due to competing professional demands prior to the final workshop after having participated in workshops one and two.
All participants were residents of the target community. As such, health professionals within the group were invited to contribute both their personal insights as a community member and consumer of local health services, and their professional perspectives of living and serving in the target community (Kilpatrick et al., 2009). Participants were asked to flag which perspective they were sharing when contributing information and insights. Quantitative and qualitative data were collected as to the ‘usefulness’ of the CASCADES Framework. When asked to evaluate the draft CASCADES Framework in terms of helpfulness in assisting the review of the service model fit for their community (on a scale of 1–10), 72% of participants scored ≥8, while 28% scored <5 (median score = 8.0).
Participants were asked to provide suggestions for improving the CASCADES Framework (note that pseudonyms have been used to maintain participant confidentiality). Some responses suggested that no improvements were necessary, with participants stating, ‘I loved that… that was neat actually. Yeah, I did [find the framework helpful], it was interesting to look at it like that. I liked that more than just a table. It certainly made it more interesting’ (Sam) ‘Yeah. I wasn't sure. I mean, I could have easily pushed that up to 10, it was so very effective, but I just didn't have any extra ideas (of what to add). I wasn't sure what was missing, if anything at all’ (Alex)
Some participants commented on the visual representation of the waterfall as an analogy for the framework. Participants indicated the diagram had assisted their frame of reference as to the focus of discussions for each workshop. ‘None [suggestions]. It is clear and I like the visual’ (Sam) ‘The visual works well ...and the mechanism broken into what works well and what needs to change is also helpful’ (Jo) ‘And because there was a picture, you were referring to it throughout the workshops. And so, we knew what you were talking about rather than those collection of words we can think of, the waterfall’ (Alex)
Participants provided insights into how the framework had assisted their thinking throughout the PAR cycle. One participant identified flexibility in the framework and its application. Another recognised the framework as assisting in narrowing the focus of discussions from broad issues to targeted action. ‘… It's a fluid way of looking at quality of change and service delivery. It's a working framework allowing for scope and change’ (Jackie) ‘I thought it provided a good framework for our discussion, it started broad and narrowed down. Yeah. It's the same with the broad context and then now, I mean, to problems and actions. I like it and there's a visual representation’ (Alex)
Most respondents indicated they had understood the labels of the tiers of Context-Outcomes-Expected-Mechanisms-Evaluate and Reflect. One participant expressed some confusion with particular terms: ‘I find the headings confusing. I do not get an immediate picture in my mind of what they represent’ (Mary)
The participant elaborated that they had found the term ‘mechanism’ difficult to relate to. Given the focus of the CASCADES Framework on the adaptation of service models, the term ‘mechanism’ was replaced with ‘model’, to clearly delineate the third tier of the framework as an opportunity to review and assess a prospective service model in terms of its fit for the community context. The language used to describe the tiers in the final version of the framework therefore became Context – Outcomes expected – Model – Evaluation and Reflection. The initials of the tiers of COME represent an invitation to community stakeholders and health professionals to ‘come’ together as a collaborative group to share their insights, experiences and information to inform the identification and implementation of context appropriate CFH service models to meet the needs of children and their families.
Discussion
The CASCADES Framework has been developed and piloted through the three phases of research as described. The framework provides both evidence-based guidance and a toolkit of resources to support community-based adaptation to CFH service models for local contextually appropriate implementation. The framework can be applied in conjunction with PAR, to facilitate the inclusive co-design approach required when working with communities. The framework provides guidance for health professionals and service managers to build a comprehensive understanding of the target community in which a CFH service model is to be implemented. The process and resources included in the framework support planning and decision-making when identifying, adapting and evaluating interventions which are appropriate to the local context, in a manner acceptable and accessible for families.
The final version of the framework is structured in terms of the key tiers, each drawing on information from the one before to inform the next. The information and insights gained are represented by water flowing down a waterfall, spilling from one tier of a cascade to the one below (see Figure 3: CASCADES Framework illustration). The momentum from the tier before enables the information to flow in a similar fashion to the water flowing downstream, filling the next level and ultimately landing at the bottom of the cascade. In the same way that water slows when reaching the pool at the bottom of a cascade, community stakeholder groups are encouraged to take time to pause after finalising their action plan and evaluation strategy, to reflect on their experience of the collaborative process. Just as the water then moves on down the river, the group will work to implement the agreed service model or intervention, heading towards their end goals of improving outcomes for families in their community. In keeping with this analogy, the framework was named the CASCADES Framework, with CASCADES being an acronym for the Collaborative Adaptation of Service Models for Child and Family Health in Diverse Settings. CASCADES framework illustration (Illustration credit: R Spooner).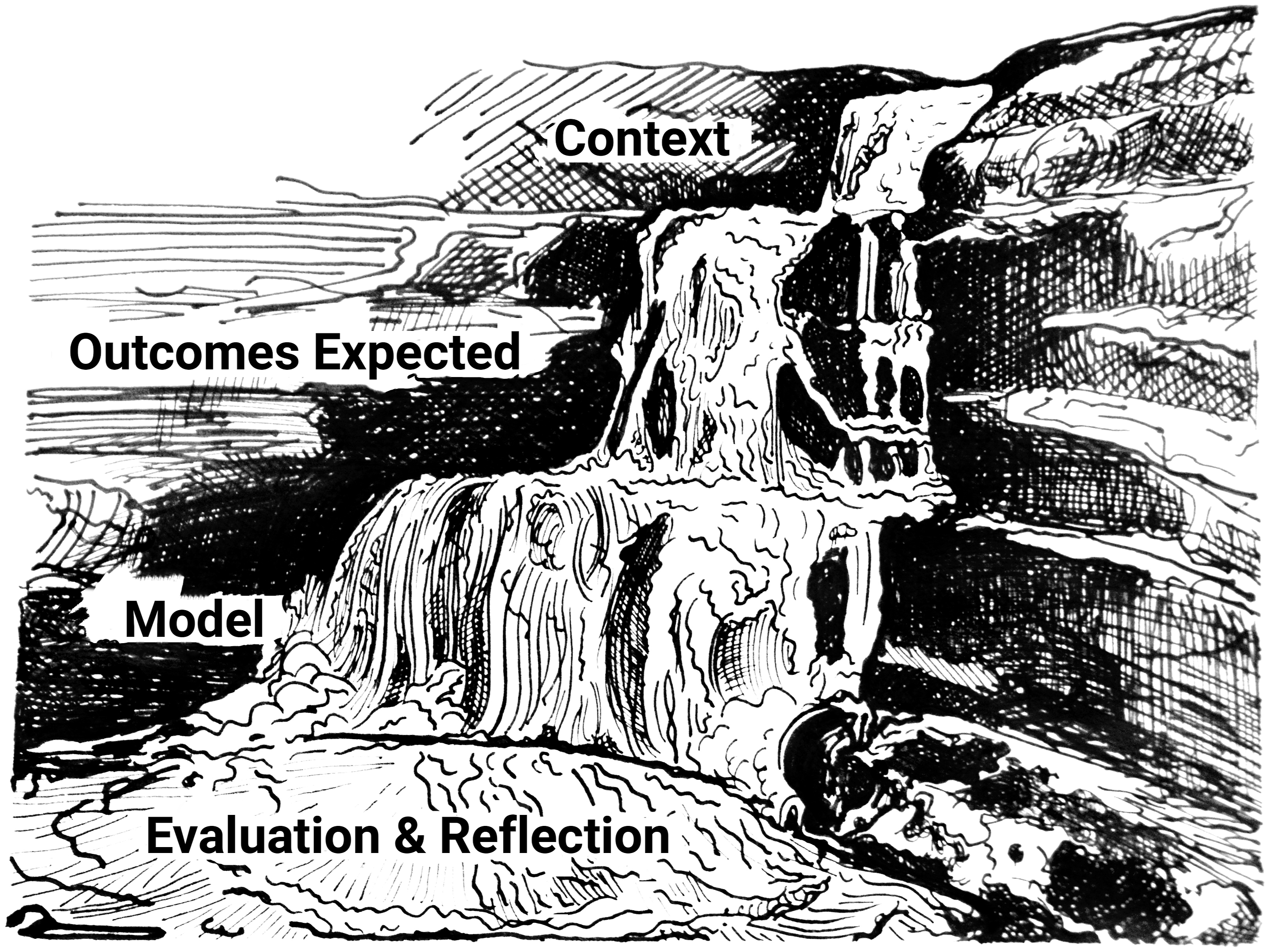
The focus of the CASCADES Framework is aligned with the phase of ‘adoption/assimilation’ in a ‘conceptual model for considering the determinants of diffusion, dissemination, and implementation of innovations in health service delivery and organization’ developed by Greenhalgh and colleagues (2004: 595). The aim is to promote dedicated time and attention on gathering information from multiple sources to develop a comprehensive understanding of the local community context in which a service model is to be implemented. This information then guides decision-making as to the appropriateness of a service model; adaptations which are needed to tailor the service model to the context; and to plan and prepare for implementation and evaluation. This process is similar to the concepts depicted by Moullin et al. (2015) in their description of two sub-stages of the ‘adoption/assimilation’ phase, being: ‘… “exploration” (the innovation-decision process, whereby the end-user(s) appraise the innovation to decide whether to adopt) and “installation” (the course of preparation, prior to use)’ (Moullin et al., 2015: 3).
The CASCADES Framework draws on the pre-existing theoretical knowledge of implementation science through the lens of CFH service provision and service model adaptation. There are synergies between the CASCADES Framework and the five domains described in the Consolidated Framework for Implementation Research (CFIR): (i) intervention characteristics, (ii) outer setting, (iii) inner setting, (iv) characteristics of the individuals involved and (v) the process of implementation (Damschroder et al., 2009). The aim of the CFIR is to ‘… guide formative evaluations and build the implementation knowledge base across multiple studies and settings’ (Damschroder et al., 2009: 1). The CASCADES Framework is aimed specifically at supporting health professionals and local stakeholders when adapting successful CFH service models in different community contexts.
The CASCADES Framework includes a guide to apply the framework, including establishing a working group. A key area of focus is consideration as to whether the collaborative working group is representative of all stakeholders with an interest or who will be impacted by the new service model. The group are asked to consider whether there are others who should be invited to participate to represent the views and voices of others in their community, including consumers and cultural representation, before proceeding. The framework then describes the four tiers of (i) Context, (ii) Outcomes expected, (iii) Model and (iv) Evaluation and reflection in detail. A description is provided of the manner in which a PAR approach (Baum et al., 2006; Hughes, 2013), can be used when working through the CASCADES Framework, in a similar manner to the process utilised during the second PAR study which informed the framework itself (see Figure 2).
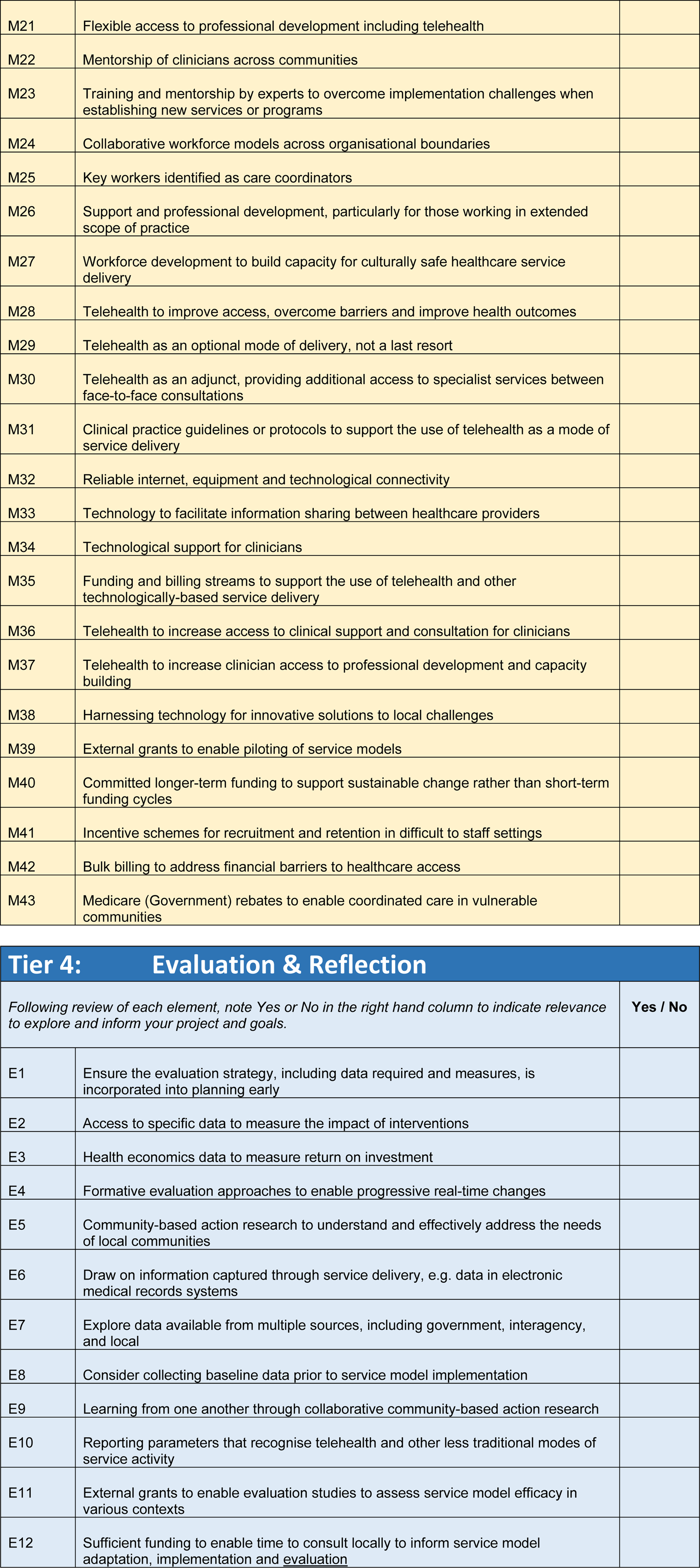
The framework includes the full list of elements to be considered when adapting a CFH service model, aligned with each tier (Table 2). Groups or facilitators may choose to review the list and identify the elements which are most meaningful and useful for their context. Alternatively, community-based groups may choose to utilise the range of optional tools and resources provided to support exploration and information gathering for each of the tiers. These include focus questions for Tiers One and Two (Context and Outcomes expected), and a checklist to support the review of a service model fit for community context for Tier Three (Model). Conversation starters are provided for Tier Four: Evaluation and Reflection, which is divided into two sections: (a) establishing our evaluation strategy and action plan, and (b) reflections of our working together. The resources for Tier Four provide options for guided facilitation, supporting the group to reflect on the information gathered; the connections made through the collaboration; and finalise the evaluation strategy for the implementation of service model and planned adaptations.
Study limitations
A limitation of the study is the small cohort in the community-based PAR group who participated in the framework pilot (Study 3). This is mitigated to some extent by the input of the participants of the first PAR study (Study 1) and the Delphi Expert Panel (Study 2), who combined to provide a broad range of knowledge, experience and perspectives in the development of the key elements and guiding principles of the framework. It is also acknowledged that the framework testing has been limited to an Australian rural community context, and is yet to be tested in international and other settings. Data will be gathered through feedback from those who request a copy of the framework, to build upon learnings from other situated research and collaborative community working groups to inform framework enhancements, continuing the iterative approach undertaken through all phases of the framework’s development.
Implications for practice
A recurring theme identified in the integrative review and both PAR studies was that of barriers to accessing specialist CFH services for families in rural (and less well-resourced) communities. In light of this, a key thread running through the framework is a focus on health service access: the contextual barriers and enablers at an individual level, the community level and broader policy level. Health service managers, policy makers and local service providers need to consider strategies to overcome service access barriers. These may range from a lack of community awareness of services or the stigma attached to help-seeking, the tyranny of distance and geographic isolation, to policy and health service structures impacting on resourcing and interagency collaboration.
The framework emphasises the need to take the time necessary to develop a thorough understanding of the local community context by drawing on multiple perspectives and sources (Fitzpatrick et al., 2017). Health service planners, managers and funding bodies need to provide sufficient funding to enable collaborative community co-design, including the time to build trust and engage with representative community stakeholders. The building of trust is a complex matter, influenced by a range of factors including fear or stigma which may be associated with speaking with those new to the community (Hastie, 2021), emphasising the need to work with those who have strong, established relationships who understand the community context (Ridgway et al., 2021).
The guiding principles for the utilisation of the CASCADES Framework are centred on a collaborative community-based process. This is consistent with the relationship and strengths-based approaches which underpin contemporary CFH service delivery (Clerke et al., 2017; Ridgway et al., 2021), enabling CFH clinicians and parents to collaborate in the co-production of new knowledge and skills (Fowler et al., 2012). A strengths-based approach enables the group to value all contributions and build trust while gathering information as to not only the needs of the community, but also the strengths and resources they hold (Pelletier et al., 2020). This is based on the premise that the group aims to be inclusive of a broad range of community stakeholders who best understand their local context and can identify innovative solutions to current or anticipated challenges (Kenny et al., 2015). The additional gains of this approach include the strengthening of inter-service and community relationships, enabling collaboration to address identified community priorities while building social capital through the collaborative consultation and design process (Chilenski et al., 2014).
Conclusion
The CASCADES Framework has been developed following three phases of research, including pilot testing of the framework with a PAR group in a community setting. The CASCADES Framework was demonstrated to provide a useful structure for guiding stakeholder groups when seeking to adapt an established CFH service model in a different contextual setting. The analogy of the water flowing down and over the cascades of a waterfall, from one tier to the next was reported as being helpful for participants. The framework provides guidance through the steps of gaining a thorough understanding of the local community context and developing shared expected outcomes of the implementation of a service model. The insights gained then support the identification of the key components of the service model relevant to the needs of the local community while noting those requiring adaptation, and taking the time to reflect and plan the evaluation strategy.
The themes of the vital role of community co-design and taking the necessary time to come to a comprehensive, collective understanding of the local context and the priority areas of need for children and their families in the community were identified throughout the three phases of the research. These have been embedded as underpinning principles within the Framework. The CASCADES Framework at its core seeks to support greater access to evidence-based specialist CFH services for families and communities in diverse and often less well-resourced settings. The Framework guides stakeholders to adapt CFH service models, to enable the delivery of services that are contextually relevant for local communities; providing effective support and interventions so children and families can reach their own aspirational goals and thrive.
Footnotes
Acknowledgements
We would like to acknowledge the support of Tresillian Family Care Centres in providing the Tresillian Standardised Service Model for use in this research; and the Local Health Districts within which this research was situated.
We would like to thank Rhianna Spooner for providing the illustration of the waterfall depicting the tiers of the framework. We would like to thank the Participatory Action Research groups and Delphi Expert Panel members for giving so generously of their time and insights which made this research possible.
Authors’ contributions
DS designed the study, undertook the project management of the study including participant recruitment, collected and curated the data, undertook data analysis, completed the development of the framework and associated resources and prepared the manuscript. JT, CF and DD were involved in study design, review and refinement of data collection tools, provided advice on recruitment, assisted with ethical approval and contributed to the manuscript preparation. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research is supported through an Australian Government Research Training Program Scholarship, supporting the doctoral research undertaken by DS.
Author’s Note
This study forms part of the doctoral research undertaken by DS. Co-authors JT, CF and DD were employed by University of Technology Sydney and completed their contributions to this paper in their roles as doctoral supervisors of DS.
Ethics approval and consent to participate
This study was approved by Sydney Local Health District Human Research Ethics Committee (RPAH Zone) – Protocol No X18-0358 & HREC/18/RPAH/504; and the University of Technology Sydney Human Research Ethics Committee (Ref: ETH19-3496). All participants were provided with a Participant Information Sheet and provided informed written consent.
Consent for publication
The data in this study has been de-identified. All participants in this study were provided with a Participant Information Sheet including reference to the publication of study results, and signed a consent form.
All authors have read and approved the final version of the manuscript. Deborah Stockton had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
Data availability statement
The authors confirm that the data supporting the findings of this study are as represented within the article and the framework can be made available on request to the primary author.
Transparency Statement
Deborah Stockton affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.