
Abstract
Objectives
The COVID-19 pandemic severely disrupted health and social care (HSC) services in many countries, including England. At the same time, it forced systems to respond innovatively to radically changed circumstances and challenges. This study identifies the impacts and emerging legacy of the pandemic for community-based multidisciplinary teams (MDTs) supporting older people with multiple long-term conditions living in their own homes.
Methods
Thirty-eight strategic, operational, and frontline staff involved with MDTs in seven areas in England were interviewed between July 2020 and August 2021, as part of a wider evaluation of the Integrated Care and Support Pioneers programme. Interview transcripts were analysed thematically.
Results
Interviewees described an initial period of pandemic disruption characterised by uncertainty, shifting of priorities and resources within the HSC system towards emergency care, and redeployment of staff away from MDTs. These circumstances required the development of new ways of working with MDT patients/clients and with one another. Remote, mostly virtual, MDT working between professionals was seen by most as a positive adaptation, though some felt that in-person meetings were better for the development of working relationships. Others raised concerns about access to, and quality of, care provided to vulnerable patients remotely, or in person but with a delay. At the local system level, the crisis response lowered barriers to collaboration between organisations, blurred professional roles, increased flexibility in the use of resources, and engendered a stronger sense of local cohesion among a wide range of staff in HSC. Most respondents wished to retain these attributes of the local system permanently.
Conclusions
The pandemic’s legacy seemed to accelerate innovations in health and care provision and increased cohesion and closer working relationships. Remote ways of working were perceived to have improved the efficiency of MDT meetings and facilitated involvement of professionals external to MDTs. The implications for patient/client care were more complex. We suggest that the potential impact on inequalities of remote access to, and provision of, care for people served by MDTs will need to be considered if these changes are to be maintained. The resilience of MDTs and the HSC system may be improved by upskilling staff and creating a more flexible workforce capable of working across organisations during future crises.
Introduction
The COVID-19 pandemic affected health and care systems and populations around the world. Health service use is estimated to have decreased globally by about 37% during the pandemic’s first wave compared to pre-pandemic. 1 In the United Kingdom (UK), primary care consultations, referrals to secondary care and hospital activity fell similarly, with 34% fewer elective inpatient admissions, 21% fewer non-COVID emergency inpatient admissions, and 22% fewer outpatient appointments, compared with the same period the previous year. Simultaneously, the demand for services treating patients with COVID led to the reorganisation of staff and resources within the system. 2 While only approximately 20% of emergency patients had COVID-19 as a primary diagnosis during the first wave of the pandemic, the resources needed to treat these patients have been reported to far exceed those required to treat other emergency patients, putting pressure on hospital capacity, with implications for staff and patients. 2 At the height of the first wave of the pandemic, critical care bed capacity in England increased from 7.4 to 19.6 per 100,000 population, 3 further highlighting the shift in demand for intensive care services. Some of the reported reductions in service use among older and clinically vulnerable people were found to stem from their avoidance of appointments for fear of catching COVID-19 and worrying about being a burden to the National Health Service (NHS). 4 The pandemic put a significant psychological strain on many health and social care (HSC) staff. They had to take care of patients (a term used hereafter to refer to patients, clients and service users) with urgent needs, while managing their own anxieties about spreading the virus, social isolation, stressful working conditions and inadequate supplies of personal protective equipment.5–8 The pandemic placed the most vulnerable people at a higher risk of infection and death, and disrupted HSC services. In the UK, it also exposed weaknesses in the coordination between the NHS and local social care services, leading to calls for further integration of HSC provision and better workforce planning.9,10
Better vertical integration within the NHS and stronger horizontal integration of HSC has been a long-standing priority in UK policy, 11 and it has become an even higher priority as the country recovers from COVID-19.12,13 A series of integrated care policy initiatives have been introduced in England in the last 15 years,11,14 including three major national integrated care pilot programmes since 2008: the Integrated Care Pilots (2009–11), the Integrated Care and Support Pioneers (2013-18), and the New Care Model Vanguards (2015–18). 15 The current paper focuses on the Integrated Care and Support Pioneers - 25 areas in England that volunteered to develop and implement innovative integrated care initiatives. The aims of the programme were to deliver better patient-centred care, and to improve patient experience, effectiveness, and cost-effectiveness of care for people with multiple needs, which may be best met when the NHS, local authority social services, the community and voluntary sector, and other public services work in an integrated way. The distinguishing feature of the Pioneers was their focus on horizontal integration of HSC services locally. The Pioneers were evaluated between 2014 and 2022.16–23 Our early evaluation of the programme (2014 to 2015) found that community-based Multi-Disciplinary Teams (MDTs) were one of the most widely reported integration initiatives amongst the 14 first-wave Pioneers. 17 This result was reinforced during our scoping work for the longer-term evaluation (2015-2022), which included 11 second-wave Pioneers, and echoes findings of research on other similar pilot schemes across the UK.11,15
Influenced by these findings, we aimed to undertake a multi-method economic and impact evaluation of 11 community-based MDTs (‘MDT evaluation’) in two contrasting Pioneer areas that volunteered to participate and in which it was feasible to conduct the evaluation. Their caseloads included patients aged 55 and older, with multiple chronic conditions and living at home. We also conducted a survey and an interview study across all 25 Pioneers to explore whether specific types or models of community-based MDTs could be identified (the ‘typology sub-study’) and to provide wider context to the 11 MDTs which were being evaluated in depth. The Pioneer programme, the MDT evaluation design and the two sites that participated in the MDT evaluation are described in detail elsewhere.16,24,25 In brief, site P1 was located in a large conurbation, and the eight MDTs at this site all operated to the same model. P2 was in a mixed urban-rural location and its three MDTs operated to different models.
While the COVID-19 pandemic disrupted the MDT evaluation, leading to a pause in data collection during late spring and summer 2020, it also provided an opportunity to expand our interviews to explore the impact and possible legacy of the pandemic for integrated working through MDTs. Drawing on interviews (March to June 2020) with strategic, operational and frontline staff participating in the MDT evaluation and the typology sub-study, undertaken after the initial COVID-related lockdown, we sought to understand the impact of the pandemic for MDT working. Specifically, we explored how: (1) MDTs were affected by, and responded to, the early stages of the pandemic; and (2) strategic, operational, and frontline staff involved in MDTs viewed the place of MDTs in the future HSC system, as well as their personal post-pandemic roles, ways of working, and inter-professional relationships.
Methods
Design
This was a qualitative interview study involving participants from the MDT evaluation and the typology sub-study, which were part of the larger evaluation of the Integrated Care and Support Pioneers programme.
Procedures
The MDT evaluation fieldwork was already underway when the COVID-19 pandemic began. As we were already conducting strategic and frontline staff interviews at P1 and P2, amendments to original research ethics approvals allowed us to include questions regarding COVID-19 in the interview topic guides (see Supplement D). The development of the original schedules was informed by our overarching research questions about MDTs, as well as the findings of the early evaluation of the Pioneers, reviews of integration policy, literature on MDTs, and our conceptual framework of MDT functioning. 24
Participants and data collection
Summary of study sites and participant information.
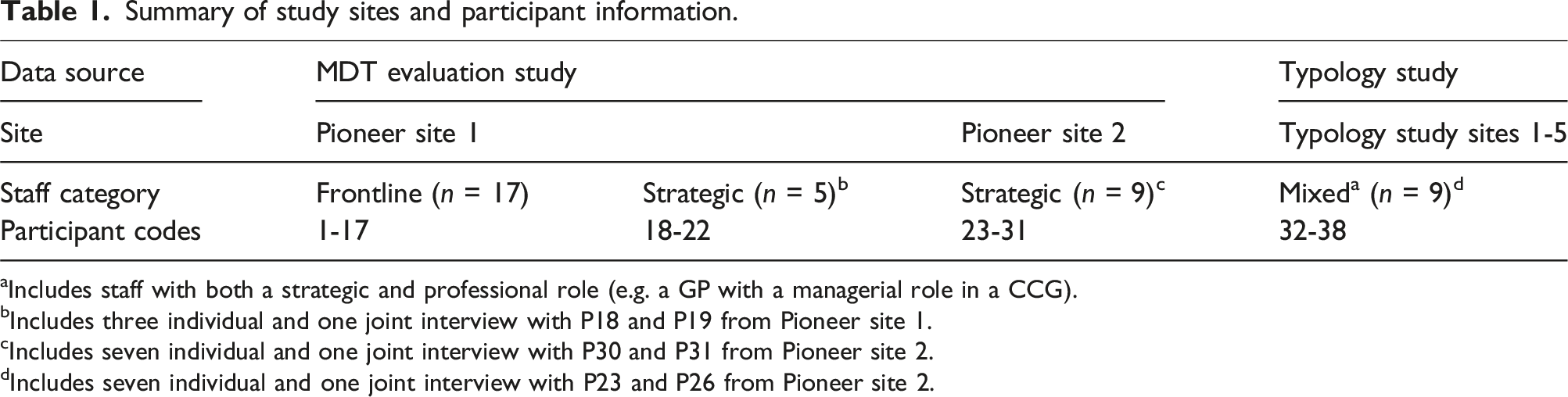
aIncludes staff with both a strategic and professional role (e.g. a GP with a managerial role in a CCG).
bIncludes three individual and one joint interview with P18 and P19 from Pioneer site 1.
cIncludes seven individual and one joint interview with P30 and P31 from Pioneer site 2.
dIncludes seven individual and one joint interview with P23 and P26 from Pioneer site 2.
Lists of names and contact details of frontline staff working in or across the MDTs in P1 and P2 were provided by MDT support staff or managers. Invitations to participate in telephone interviews were sent by email.
Strategic leaders were initially identified by individuals facilitating the study locally at P1 and P2 (in both cases a NHS clinical commissioning group (CCG) manager), followed by snowballing to identify others working in strategic roles. The aim was to interview managers working at a strategic level in a range of relevant organisations – CCGs, local authority social services, primary care, etc. - on local HSC care integration, through MDTs and other local initiatives. Potential participants were invited to take part by email and/or telephone. They were sent study information sheets and consent forms by email. All interviews were conducted by telephone. Seventeen frontline (all in P1), and 14 strategic (five in P1, nine in P2) staff were interviewed after the onset of the pandemic.
Strategic leaders and operational managers for the typology sub-study were identified in two stages. The initial sample was compiled by using contacts from a 2019 key informant survey undertaken as part of the wider evaluation of the Pioneers, 20 and by contacting Pioneer leads and relevant organisations (e.g. CCGs) in each locality. Additional contacts were gathered by asking those completing the survey to nominate other key contacts associated with the MDTs. Contacts were invited by email to participate in telephone interviews after the initial COVID-related lockdown in England. Nine contacts from five study sites (Pioneers) were interviewed between May and August 2021. However, two participants (P23 and P26), who were interviewed jointly for the typology sub-study, had also been interviewed independently for the MDT evaluation study in site P2. Overall, we interviewed thirty-eight participants from seven Pioneer sites. Table 1 summarises the number and category (strategic, frontline or mixed roles) of participants across the study sites.
All interviews were audio-recorded on encrypted recorders. Interviews lasted between 30 and 70 minutes. Interviews were transcribed, and recordings and transcripts stored securely.
Data analysis
The data were analysed inductively, using the process of reflexive thematic analysis to understand patterns across the dataset.26–28 After familiarisation with transcripts, initial descriptive and interpretative codes were given to data relevant to the pandemic and its impacts on HSC integration through MDTs. The codes were clustered into a ‘coding tree’, and further developed through reading, review, and discussions amongst the analysts (AP, LR, MAD). After that, LR, AP and MAD reviewed and refined the codes, primarily using NVivo v.12 software 29 and memos. Themes and sub-themes were developed based on these clusters and organised into a table with illustrative quotes, enabling us to compare the narratives within and between the participant groups. Through an iterative process of continuous review, refinement, discussion, and writing, as outlined by the six phases of the reflexive thematic approach, 28 we constructed the main narrative around the emerging legacy of the COVID-19 pandemic and its implications for the functioning of integrated MDTs post-pandemic. By legacy, we mean lessons learned and changes made to mitigate the impact of the pandemic on the HSC system, including on the functioning of MDTs. While the legacy of the pandemic for MDT working was our focus, beliefs about the COVID-19 legacy were often implicit in participant discussions of the more immediate impacts of COVID-19 on MDTs. We therefore also present participant interpretations of these more immediate impacts.
Results
We developed two main themes relating to the pandemic’s emerging legacy for HSC. These are discussed below.
Theme 1: Changed ways of working as an immediate response to the pandemic
Regardless of their role in relation to MDTs, most interviewees perceived the pandemic as having had a sudden impact on a HSC system that was largely unprepared for it. Described as ‘a blow to the system’ (Interviewee 29, Strategic staff, P2), the initial response to the pandemic was perceived as ‘amazingly chaotic’ (Interviewees 18 & 19, joint interview, both Strategic staff, P1). Frontline and strategic interviewees reported a shifting of priorities and resources towards emergency care, moving patients out of the acute hospital to make space for COVID-19 patients, and redeploying staff to support care homes, all of which they said had an impact on staff availability, workload, and care provided through MDTs.
While MDTs would have previously drawn on relationships with a wider group of people working in HSC organisations, these were reported to have been redeployed to meet the increased demand created by the pandemic. The change of priorities to COVID-19-related activities was said to have resulted in MDTs’ workloads initially reducing (P2) or MDTs temporarily stopping meeting (P1). Most interviewees perceived this as necessary to accommodate the changed needs of the system during the crisis: Because things were changing on a daily/weekly basis I think my feeling is that it was the right thing to suspend the MDT, or the MDT meetings, for that period of time because all our energy needed to go back into crisis management in our own organisations, and once we had achieved some sort of system or stability, there with this new normal, even though that was a continually changing process. Only then could we reconvene and start to rebuild a new MDT based on the needs at the time. (Interviewee 11, Frontline staff, P1)
However, some regarded the changing priorities as counterproductive: The meetings stopped, which was very short-sighted because, actually, the patients who we were discussing needed our services more, not less, when COVID started. (Interviewee 12, Frontline staff, P1)
Interviewees observed that fewer patients (other than those with COVID-19) were seeking health services, which they attributed to patients’ fear of becoming infected with the virus: Patients were scared to visit services, or they were not sure if they can, and they were not presenting themselves to the surgeries or to other services. (Interviewee 3, Frontline staff, P1)
With the guidelines at the time recommending social distancing and shielding for the most vulnerable people, interviewees often voiced concerns about a deterioration in patients’ health due to patients not being seen: A lot of patients who are frail in the community have deconditioned. We haven’t had the physiotherapy, our physiotherapists have just been focusing on urgent care. (Interviewee 37, Strategic staff, T4)
As a result of MDT staff being recalled to their separate HSC services and patients’ healthcare-seeking behaviour changing, there was a perceived need to develop alternative ways of working that would enable caseload review, and maintenance of MDT inter-professional relationships and activities while the pandemic was continuing. The transition to remote working (including virtual and telephone contact) was perceived as one of the most significant changes forming the response to the pandemic: Technology improved because of COVID - the NHS came into the 21st century a bit. (Interviewee 23, Strategic staff, P2)
Remote MDT working enabled staff to continue to plan patient care, by meeting virtually or in hybrid meetings. Most interviewees viewed remote working and meetings as a useful innovation helping the teams to adapt to the pandemic, and a positive experience that had reduced boundaries between people and organisations. The perceived benefits included increased convenience (less travelling), meetings becoming more structured and efficient, and increased attendance by MDT members (who previously might not have attended due to the time required for travel): [MDT staff] don’t have to travel … They can switch a computer on. So, they come to the meetings instead of sometimes not turning up for weeks on end, which often happened before. (Interviewee 24, Strategic staff, P2)
Some found it easier to fill in for colleagues who could not attend remote meetings: It’s easier for us as a navigation team to cover for each other when we are on leave or absent, for sickness, because we don’t have to drop everything and travel to a particular site. (Interviewee 7, Frontline staff, P1)
Online MDT meetings also enabled flexible participation of staff whose input was not needed at every meeting, or for every patient discussed.
The disadvantages of remote working included having to become familiar with new technology, problems with document signing and sharing, maintaining focus and engagement in online meetings, less opportunity for informal learning from colleagues, and difficulties developing deeper working relationships with colleagues. Some interviewees suggested that while remote working might work well in established MDTs, it was uncertain whether effective working relationships could be developed online to the same extent with new colleagues who had joined during the pandemic.
Remote working was therefore a mostly welcome change that enabled more efficient functioning of MDT meetings, though perhaps at the cost of more informal ways of building better quality relationships with colleagues in person: Whether you could start online for a new team that doesn't know anybody, I don’t know. But we didn’t have to do that, we weren’t in that position. (Interviewee 38, Strategic staff, T5)
A small number of interviewees emphasised the continuing importance of face-to-face contacts: I think with COVID everyone’s suddenly realised that they really do need other people in person, no matter how many phone calls or Zoom calls. And I think we’re missing something human by not meeting up. (Interviewee 10, Frontline staff, P1)
Some interviewees suggested that providing services remotely increased access to care and services for patients (e.g. social prescribing, mental health support). However, this only applied to patients who were able to adapt to the new ways of accessing support. Interviewees noted that people without phones or computers might have been excluded from accessing appropriate care during the peak of the pandemic.
Other participants had concerns about having to rely on patients’ self-reports when providing care remotely instead of doing an in-person assessment: One of the things when you're doing an assessment with a client is that, yes, you can talk to them and get their verbal overview of their situation, but when you're actually at their home you can get an idea about how they’re living, the things that they’re struggling with. You can see the physical environment, especially if they’re struggling with hoarding or issues at home. You can make suggestions and approach certain subjects that they might not actually tell you over the phone. (Interviewee 7, Frontline staff, P1)
Some of these difficulties were overcome by involving carers or family members in remote consultations.
Despite the perceived challenges in both professional-to-professional and professional-to-patient contact, most interviewees thought that there was a place for remote team working and remote patient contact after the pandemic, as long as there was capacity for face-to-face interactions with those patients who need them. Having realised the benefits of remote working, most narratives from the first 12 months of the pandemic conveyed a sense of interviewees not wanting to return to previous ways of working. They could see clear opportunities to better tailor patient consultations and MDT meetings to patient and staff needs in the future, contributing to better person-centred care: Being able to text message patients direct from the clinical system, doing video consultations, doing meetings via Teams rather than MDT face-to-face … all of that happened very, very quickly, within the space of a few weeks. I have to say, I think that’s been amazing and really positive, and we’ve really managed to still provide a very good service to our patients that way. These changes we will continue once the pandemic dies down and it is safe to see patients face-to-face, because a lot of the new systems are working so well, and it isn’t necessary to bring patients in. (Interviewee 13, Frontline staff, P1)
Theme 2: Pandemic disruption as a driver of increased cohesion in HSC
Some frontline staff interviewees suggested that the disruption of the MDTs’ ways of working during the early period of the pandemic had led to increased recognition of MDTs’ value in the local HSC system. One participant reflected on feedback they had had from GPs: After wave one there was loads of feedback from GPs saying, ‘We need this back. This is an integral part of how we work now. We need this meeting in order to work effectively with social care, with [site name], with mental health. So, when can we have it back?’ And we just started getting that feedback from across our practice network, so that was really welcome. (Interviewee 32, Strategic staff, T1)
It seemed that even though the pandemic disrupted the MDTs and, in some cases, led to a temporary suspension of meetings, there was a general desire to resume MDT meetings sooner rather than later: When they [the MDT meetings] stopped, then I think people realised actually how useful they were. So, that was an advantage. It took that to make people realise actually that there were things that are too difficult to achieve without an MDT. That joined-up thinking is much easier if we all meet once a week. (Interviewee 12, Frontline staff, P1)
Most interviewees saw the pandemic as a stimulus to closer multidisciplinary working practices. Strategic leaders in P2 spoke of faster pooling of budgets (including loosening of the criteria restricting uses of budgets), removal of unnecessary bureaucracy, and closer collaboration between organisations: I think that’s what COVID has done to organisations - it has brought us together and has said to us in a way, ‘Forget about the bureaucracy and get on with it.’ I think that’s the part we've liked, with not having to get into the financial arguments … There’s one pot of money and get on with it and share your resources, and it's been fabulous, that side of it. None of us want that to go, but we know it's not going to be here forever, so we’ll have to think on how do you maybe pool all your budgets and how do you work differently so we don’t end up having to go back to all that bureaucracy. (Interviewees 30 & 31, joint interview, both Strategic staff, P2)
Working together with a common purpose during the crisis overrode individual organisational goals and boundaries: The pandemic, I think, has accelerated the need for systems to really understand how we can effectively work better together - accelerated the glue, if you like, between the interfaces of organisations. So, now, if you think about what the impact of COVID has had, we’re now absolutely beginning to think through how we cement that integration using digital enablers. We’re finally in the place where we’re able to do some of that … it’s changing the mindset of health professionals. (Interviewee 15, Frontline staff, P1)
Some frontline and strategic interviewees noted that the pandemic strengthened existing relationships between different organisations and facilitated initiatives to respond to the pandemic, such as setting up local pop-up vaccination centres: It’s really enabled a phenomenally integrated response - how we’ve pooled resources together to do that, how we’ve pooled staff in primary care, how we use novel venues to administer the vaccine. So, fantastic administration of pop-up vaccines, based at a local mosque, which was a combined effort. So, lots of really integrated and fantastic work that I think had the seeds laid a very long time ago, so that it wasn’t so difficult to do stuff better together. (Interviewee 15, Frontline staff, P1)
The pandemic placed a significant physical and mental strain on interviewees. Many interviewees spoke of ‘change fatigue’ – the exhaustion caused by changes in working practices and disruption of routines, the ongoing waves of the pandemic, and the need for continuous learning (e.g. IT systems, COVID-19-related government guidelines). Other factors that contributed to this feeling were staff shortages, and increasingly negative public attitudes towards frontline staff between the first and the second wave of the pandemic (due to the public’s increased frustration about reduced access to services). In addition, many frontline interviewees reported working without adequate personal protective equipment, which exposed them to the virus and led to some of them being infected and absent from work.
Yet, many interviewees reported a sense of resilience and positivity in the HSC workforce as a result of their ability to adapt to the challenging situation: At the beginning I felt ready to throw in the towel … It felt horrible, but it’s been a massive learning curve for everybody, no matter who you are and what level you are, and now I feel like we’re in a much better place than we were. (Interviewee 26, Strategic staff, P2).
The boundaries between professional roles seemed to have become more blurred, which likely helped overcome the reported staff shortages. A small number of frontline and strategic interviewees in P1 and P2 noted the additional training provided to frontline staff to enable them to move into related areas of competence or cover for colleagues, as appropriate: We do have a lot of training, mainly on managing PPE [personal protective equipment], donning and doffing PPE, screening for COVID, so those are the things that are fairly new to what we did before. (Interviewee 2, Frontline staff, P1)
The blending of professional boundaries seemed to have contributed to interviewees’ sense of empowerment and unity despite their experiences of exhaustion: As a peer-coaching team, we ended up moving into lots of areas. We started working in crisis services to help people make soft landings out of crisis. We worked with the recovery and rehab teams, the mental health teams, to help people who were then struggling with their teams if we had capacity. We helped with some of the discharges. So, in some ways within the social services we kind of blurred boundaries a lot about what was delivered during the COVID time as well. (Interviewee 1, Frontline staff, P1)
Most interviewees expressed the hope that the closer working relationships between different professions would continue beyond the pandemic as part of the evolution of integrated care.
Discussion
Participants involved in organising integrated health and care for older people living in their own homes during the early stages of the COVID-19 pandemic described an initial period of disruption followed by developing new ways of working with patients and with one another. Remote MDT working was seen by most as a positive development overall in terms of team working, especially in enabling ‘guest’ staff to contribute to case coordination and management at specific MDT meetings where their skills were needed. At the same time, interviewees recognised the potential for deterioration in the health of people who had not been seen in person, or whose care was delayed due to the prioritisation of COVID-19-related care.
At the same time, the pandemic had highlighted the gaps in HSC, especially the need to increase the involvement of mental health workers, benefits advisers and housing staff in MDTs, and the development and training of a more flexible workforce.
We found that the pandemic highlighted the need for improved integration to not only carry out the usual MDT functions during the crisis, but also to allow for more pandemic-specific integrated responses. At the local system level, the crisis response lowered the barriers to collaboration between organisations, blurred professional roles, increased flexibility in the use of resources and engendered a stronger sense of local cohesion among a wide range of different staff in HSC. Interviewees wished to retain these attributes of the local system more permanently.
These findings are similar to those from a key informant survey of all Pioneers looking at the impact of the pandemic on MDTs undertaken in the autumn of 2020, 21 and almost identical to those reporting on responses of HSC systems to the pandemic internationally. 30
Implications for MDT practice
The findings indicate that community-based MDTs supporting older people with multiple long-term conditions may benefit from adopting remote technology. While this technology may not adequately substitute for all the benefits of face-to-face contact with colleagues and patients, its expansion and utility during the pandemic likely facilitated access to, and continuity of care for, people with long-term conditions, who might otherwise not have been able to receive care. 31 Examples of using virtual treatments and digital services during the pandemic include receiving prescriptions on mobile phones via text messages or email, consultations via telephone or video, or using electronic systems to share information. 32
However, engaging with remote consultations may be easier for patients with already established relationships with professionals, and it is unclear whether new patients would benefit from remote contact with MDT staff to the same extent.
The challenge for practitioners, assisted by health services researchers, is to identify which approaches to care and support work best for which purposes and for which types of patients.
Discussions of virtual consultations and eHealth solutions commonly emphasise the risks of inequities arising between patients who can, versus those who cannot, manage computer technology, the internet, or smart phones.33,34 In its pre-pandemic guidance for general practice providers and commissioners, NHS England outlined ideas to improve patient access to general practices. These included expanding access via new consultation types (online, telephone, group consultations). 35 The initial phases of the pandemic saw a substantial change in the ratio of face-to-face versus telephone and electronic/video consultations.36,37 While there were approximately 30% of telephone consultations before the pandemic in April 2019, this changed progressively to almost 90% in April 2020. GPs and nurses were reported to have carried out three and five times more remote consultations, respectively, between April and July 2020, compared with the same period the previous year, while face-to-face consultations with GPs and nurses dropped to 16% and 50% of the previous year, respectively. 37 Other sources cite a 468% increase in remote appointments overall. 2 An analysis based on almost four million consultations between February and May 2020 reported that people with the highest frailty and risk of polypharmacy attended several-fold more face-to-face and telephone appointments compared with people without frailty and polypharmacy, 36 suggesting increased needs in these people, their preferred mode of communication, and potentially the prioritisation of their needs during the pandemic. Limited other evidence suggests that people over the age of 85 are more likely to use telephone consultations than younger people, and that women may be slightly more likely to use remote consultations compared to face-to-face ones and compared to men in general. 38 Evidence of the effect of socioeconomic position and ethnicity on the use of technology-enabled consultations currently seems somewhat mixed, although indicative of unequal access for people of non-white ethnicity and those living in more socially deprived areas, highlighting the need for flexibility in remote care provision. 39
In our study, interviewees in MDTs where direct contact with patients was part of the MDT’s remit reported adopting approaches to remote consultation that attempted to reduce the risk of patients being excluded from accessing services, by involving patients’ informal carers, who might be able to assist in remote consultations. Using telephone consultations also proved useful and possibly reduced the risk of digital exclusion. Three quality considerations that may facilitate the transition to remote consultations for patients are ensuring privacy and confidentiality (e.g. by having a dedicated telehealth room), building trust through continuity of care (seeing the same clinician over time), and establishing empathetic and person-centred communication online, likely requiring additional staff training. 40
From the perspective of MDTs, remote meetings were reported to widen and deepen the involvement of relevant, but more peripheral, specialised MDT members in planning the care and support of patients with multiple needs, possibly contributing to more efficient and tailored care. Our observations of MDT meetings before the pandemic showed that there is a strong case for engaging a wider range of professionals in regular MDT meetings, especially those knowledgeable about housing matters, employment and benefits, and mental health. 16
Community pharmacists are another group of professionals increasingly identified as having a significant role in these types of MDTs. 41 Our interviewees did not mention community pharmacists. This was surprising given the vital role community pharmacists played during the pandemic, ranging from dispensing medications and providing telehealth services, to delivering vaccinations, while also adapting ways of working to be able to provide these essential services.42,43 The National Pharmacy Association reported a 25% increase in medication dispensing and a 300% increase in home deliveries during the first lockdown in 2020. 44 It is possible that community pharmacists were either not perceived as missing from the MDT team because they had already been involved in the pandemic response via local Primary Care Networks, or they were still not seen as core members of the MDTs.
We also found that virtual meetings facilitated communication between different professional groups and with the voluntary sector. It remains an open question as to how far this way of working can be sustained post–COVID-19, though we observed that there was a hope among the participants that this particular advantage of remote meetings would be sustained in the longer-term.
Implications for local health and care systems
Our findings suggest that MDT members’ experiences of more flexible ways of working, with less emphasis on strict role demarcations between professions and organisations, were not only helpful for system resilience during the immediate crisis, but pointed to potential gains from more flexibility in working arrangements in the future. This suggests that there is scope to train and develop a more flexible workforce equipped with generic and transferable skills and competencies - for example, through multidisciplinary teaching and training programmes. 45
The majority of interviewees saw the pandemic as a stimulus to closer multidisciplinary working in the future. This accords with the results of our key informant survey of all the Pioneer sites undertaken in the autumn of 2020 on the impact of COVID-19 on integration activities, where only a few participants raised concerns about organisations retreating to siloed working after the pandemic. 21
Limitations
There were two main limitations to this part of the Pioneer MDT evaluation. First, the COVID-19 pandemic had a significant impact on our ability to collect data from HSC staff during the first year, as interviewees were redeployed across the system and in high demand. The timing of interviews also varied depending on when the participating sites considered it appropriate to resume research not directly related to COVID-19. As a result, it was difficult to compare participant reports between the different sites.
Second, as the data collection period lasted from the second half of 2020 to well into 2021, some participants had experienced several COVID-19 waves and lockdowns by the time they were interviewed and thus may have altered their views over time. On the other hand, interviewing participants over time may have provided us with reflections that might not have been available to staff interviewed immediately after the first lockdown.
Conclusions
In England, the emerging legacy of the early stages of the COVID-19 pandemic for community-based MDTs involved in the care of older people living in their own homes, appears to have been generally positive. Remote ways of working were perceived to have improved efficiency of MDT meetings and encouraged the involvement of valuable colleagues external to MDTs.
The implications for workforce planning include potential upskilling of staff in tasks that can be done remotely, and the development of transferrable skills that can be used in situations of emergency redeployment across HSC organisations. The implications for patient care are more complex, including the potential for more tailored care, by using hybrid ways of working, but also concerns about access to care and its quality for people unable to adapt to the new ways of working.
Supplemental Material
Supplemental Material - The impact and legacy of COVID-19 on community-based multidisciplinary teams organising integrated health and social care for older people with long-term conditions: Findings from the evaluation of the integrated care and support Pioneers
Supplemental Material for The impact and legacy of COVID-19 on community-based multidisciplinary teams organising integrated health and social care for older people with long-term conditions: Findings from the evaluation of the integrated care and support Pioneers by Lucia Rehackova, Mary Alison Durand, Agata Pacho, Gerald Wistow, Lavanya Thana, Mustafa Al-Haboubi and Nicholas Mays in Journal of Health Services Research & Policy.
Footnotes
Acknowledgments
We wish to thank all of those - patients, informal carers and staff - who participated in the MDT evaluation, and staff at the Pioneer sites who helped to facilitate its implementation. We also acknowledge the contributions of our former colleagues Nick Douglas, Ties Hoomans and Tommaso Manacorda to the development of our conceptual model of MDT functioning.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is an independent evaluation funded by the NIHR Policy Research Programme (Evaluation of the Integrated Care and Support Pioneers Programme in the context of new funding arrangements for integrated care in England (2015–2022), PR-R10-0514-25001). NIHR played no role in the conduct of the research or preparation of this manuscript. The views expressed are those of the authors and are not necessarily those of the NIHR or the Department of Health and Social Care.
Ethical statement
ORCID iDs
Data availability statement
The datasets generated and analysed during the current study are not publicly available because they contain information that would identify the research sites, individuals, and/or case-material and it would not be feasible to redact or otherwise anonymise them. The data custodian is Professor Nicholas Mays, London School of Hygiene & Tropical Medicine.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.