
Abstract
Objective
This study investigated the associations between adherence to the Mediterranean Diet and the Eatwell Guide (EWG) and changes in weight and waist circumference in post-menopausal women.
Study Design
Post-hoc analysis of post-menopausal women from the UK Women’s Cohort Study.
Main outcome measures
Changes in weight, waist circumference and the risk of abdominal and general obesity.
Results
4162 post-menopausal women were selected. Higher adherence to both the EWG and the Mediterranean Diet was associated with smaller increases in waist circumference over 4 years (EWG: β −0.47, CI −0.75, −0.20 per 1 tertile increase in score), (Mediterranean Diet: β −0.29, CI −0.58, −0.01 per 1 tertile increase in score); and lower risk of abdominal obesity (EWG: OR 0.55, CI 0.43, 0.70 third versus the first tertile), (Mediterranean Diet: OR 0.60, CI 0.46, 0.76 third versus the first tertile), but was not associated with weight changes (EWG: β 0.14, CI −0.07, 0.36 per 1 tertile increase in score), (Mediterranean Diet: β 0.03, CI −0.19, 0.25 per 1 tertile increase in score) or risk of becoming overweight or obese (EWG: OR 1.09, CI 0.77, 1.52 third versus the first tertile), (Mediterranean Diet: OR 0.91, CI 0.65, 1.27 third versus the first tertile).
Conclusions
The results suggest that adherence to either the Mediterranean Diet or the EWG can help to prevent abdominal obesity in post-menopausal women.
Introduction
Weight gain, particularly abdominal obesity, is prevalent among women in menopause,1,2 and 66–69% of women over 45 in the UK are overweight or obese. 3 Weight gain is considered age- and lifestyle-related; however, the drop in estrogen during menopause influences the fat distribution, particularly in the abdominal area.1,4 Abdominal obesity is associated with adverse metabolic events, including cardiovascular disease, the leading cause of death in post-menopausal women. 1 Poor dietary quality is an important modifiable factor in the prevention of obesity, and improved dietary quality has been associated with a lower risk of overweight or obesity in both men and women.5,6 There are few studies on dietary patterns in post-menopausal women, but the limited evidence suggests that improvements in diet quality are associated with smaller increases in weight and waist circumference (WC); however, the optimum dietary pattern is undecided.7–9 This study examines how adherence to the Mediterranean Diet and the Eatwell Guide (EWG) influences weight and WC in post-menopausal women in a UK cohort.
Experimental methods
Study population
The UK Women’s Cohort Study (UKWCS) was initially established to investigate the relationships between diet and chronic disease, particularly cancer, and this cohort’s complete details have been published. 10 A total of 7859 post-menopausal participants were identified from their answers on the baseline questionnaire, and 4162 were selected after the following exclusions: 1760 had missing (n = 1756) or implausible (n = 4) anthropometric data; 375 had implausible daily energy intake of less than 500 kcals or more than 3500 kcals per day, 11 and a further 1562 had missing confounding variables (n = 1536) or discordant waist measurements (n = 26).
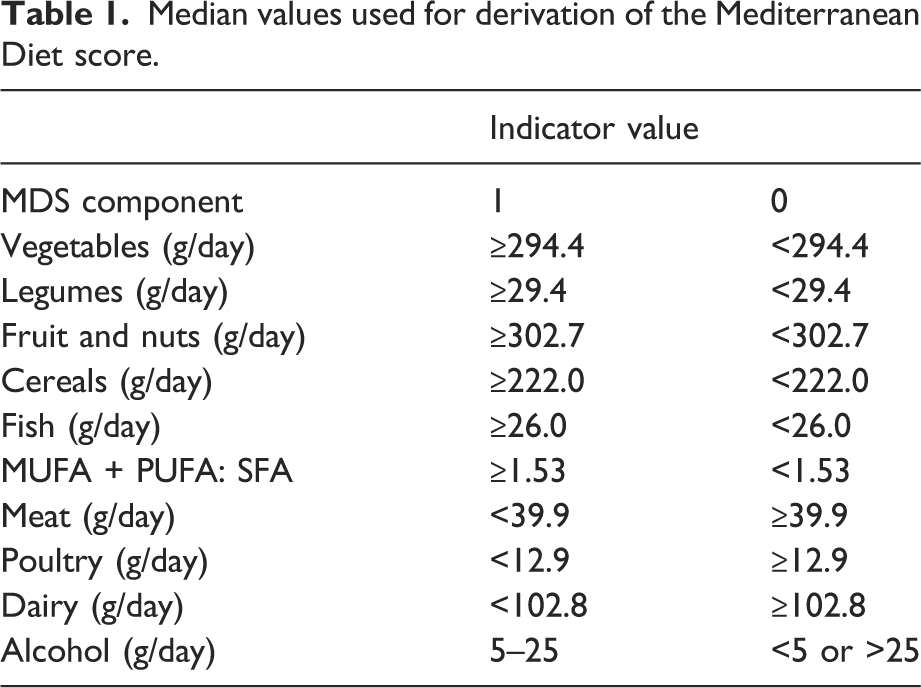
Dietary assessment
Median values used for derivation of the Mediterranean Diet score.
Anthropometric measurements
Anthropometric measurements were recorded from the baseline and Phase 2 questionnaire and were self-reported measurements on WC, height and weight. Participants were categorised into abdominal obesity categories based on their WC, where abdominal obesity was classified as having a WC of ≥88 cm. Participants were also categorised into weight categories based on their BMI, where a BMI over 25 kg/m2 was classified as overweight or obese.
Covariate measurements
Demographic and socioeconomic information was self-reported in the baseline questionnaire. The variables controlled for were age, physical activity, education, smoking and use of Hormone Replacement Therapy (HRT). These were thought to have links between dietary patterns and obesity and have been controlled for in previous studies.17,18 Although ethnicity was identified as a potential confounder, it was not included in this analysis as the majority (99.3%) of the participants selected for this study, who supplied their ethnicity, were white.
Statistical analysis
All statistical analysis was conducted using the Statistical Package for the Social Sciences (SPSS), 19 and statistical significance was reported as <0.05.
Hierarchical multiple linear regression models were used to evaluate the association between the Mediterranean Diet and EWG scores (by tertile of adherence and as a continuous scale) and changes in WC (cm; continuous) from baseline to Phase 2. The first model was minimally adjusted for age (years; continuous) and baseline WC (cm; continuous); the second model included adjustments for total energy intake (kcal; continuous), time from baseline to Phase 2 (year; continuous), physical activity (met the physical activity recommendations Yes/No; dichotomous), smoking (never/current/former; nominal), education (No qualifications, O Levels, A levels, Degree; nominal) and HRT (never/current/former; nominal). Finally, the model was adjusted for changes in BMI (kg/m2 continuous) to understand how weight changes explained any differences. Hierarchical linear regression was then repeated to look at the association between adherence to dietary patterns and changes in weight. All the same adjustments were made, except baseline WC was replaced with baseline BMI in the first model.
For those with a normal (<88 cm) WC at baseline, the relationship between dietary scores and risk of abdominal obesity was assessed using binary logistic regression for each one-point increase in score (continuous) and tertile increase in score (categorical). The first model was minimally adjusted for age, and the second model included adjustments for total energy intake (kcal; continuous), time from baseline to Phase 2 (years; continuous), physical activity (Yes/No; nominal), smoking (never/current/former; nominal), education (none/O level/A level/Degree; nominal) and HRT (never/current/former; nominal). The binary logistic regression was then repeated for those with a BMI of less than 25 kg/m2 to investigate the relationship between adherence to dietary patterns and the risk of becoming overweight or obese.
Results
Characteristics of participants according to tertiles of adherence to the Mediterranean Diet. Continuous variables are presented as the median and interquartile range (IQR) and categorical variables as percentages p-values obtained from the Kruskal–Wallis H test for continuous variables and Chi-squared test for categorical variables.
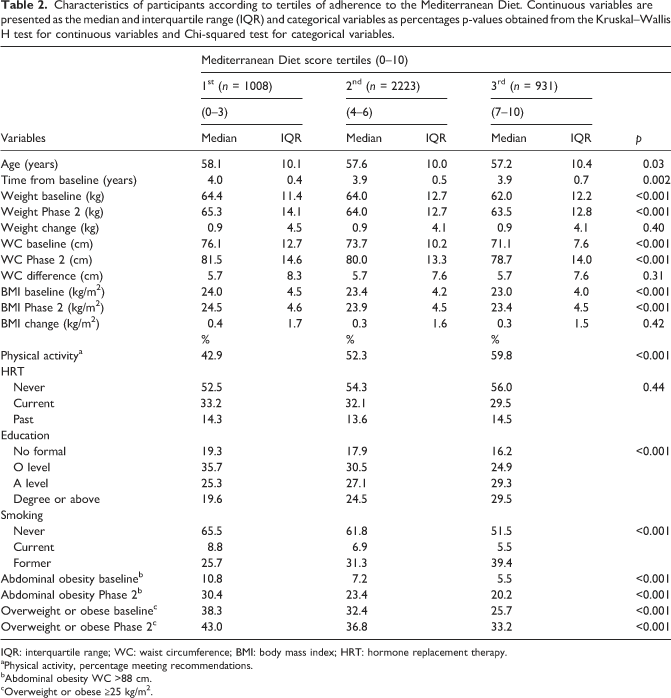
IQR: interquartile range; WC: waist circumference; BMI: body mass index; HRT: hormone replacement therapy.
aPhysical activity, percentage meeting recommendations.
bAbdominal obesity WC >88 cm.
cOverweight or obese ≥25 kg/m2.
Characteristics of participants according to tertials of adherence to the Eatwell Guide. Continuous variables are presented as the median and interquartile range, categorical variables as percentages-p values obtained from the Kruskal–Wallis H test for continuous variables and the Chi-squared test for categorical variables.
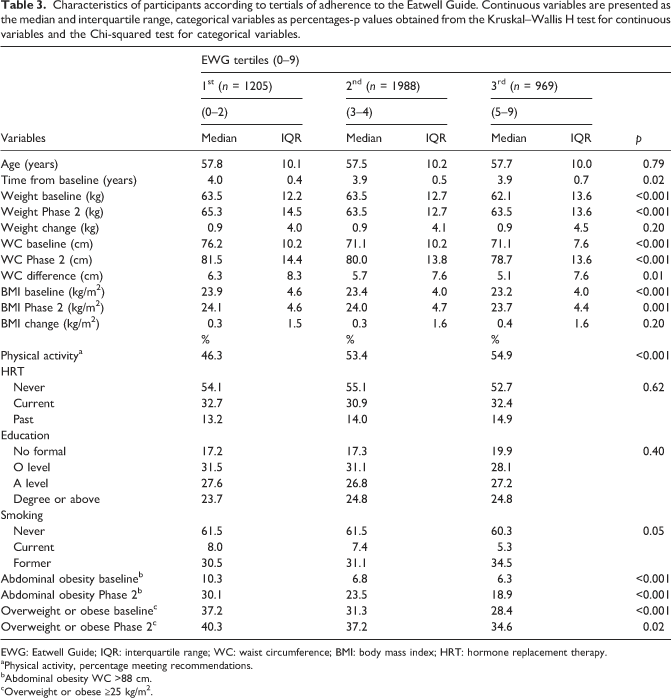
EWG: Eatwell Guide; IQR: interquartile range; WC: waist circumference; BMI: body mass index; HRT: hormone replacement therapy.
aPhysical activity, percentage meeting recommendations.
bAbdominal obesity WC >88 cm.
cOverweight or obese ≥25 kg/m2.
Multiple linear regression models describing the association between an increase in Mediterranean Diet Score or EWG score (continuous variable, per tertile increase) and change in waist circumference between baseline and Phase 2 (β coefficients and 95% confidence intervals).
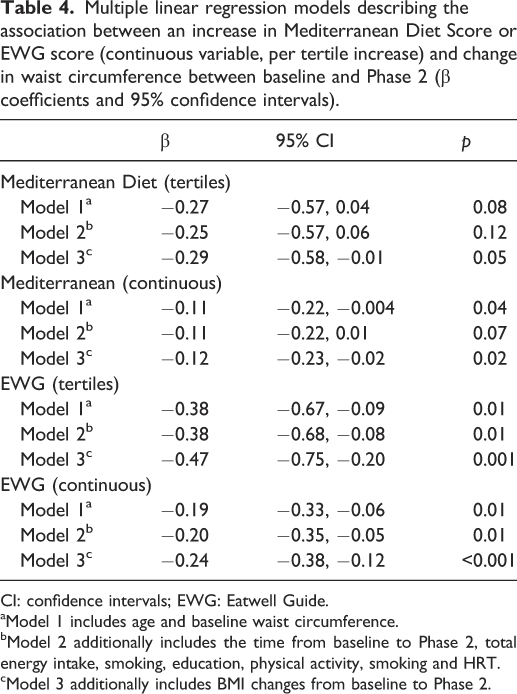
CI: confidence intervals; EWG: Eatwell Guide.
aModel 1 includes age and baseline waist circumference.
bModel 2 additionally includes the time from baseline to Phase 2, total energy intake, smoking, education, physical activity, smoking and HRT.
cModel 3 additionally includes BMI changes from baseline to Phase 2.
Multiple linear regression models describing the association between an increase in Mediterranean Diet Score or Eatwell Guide score (continuous variable, per tertile increase) and change in weight between baseline and Phase 2 (β coefficients and 95% confidence intervals).
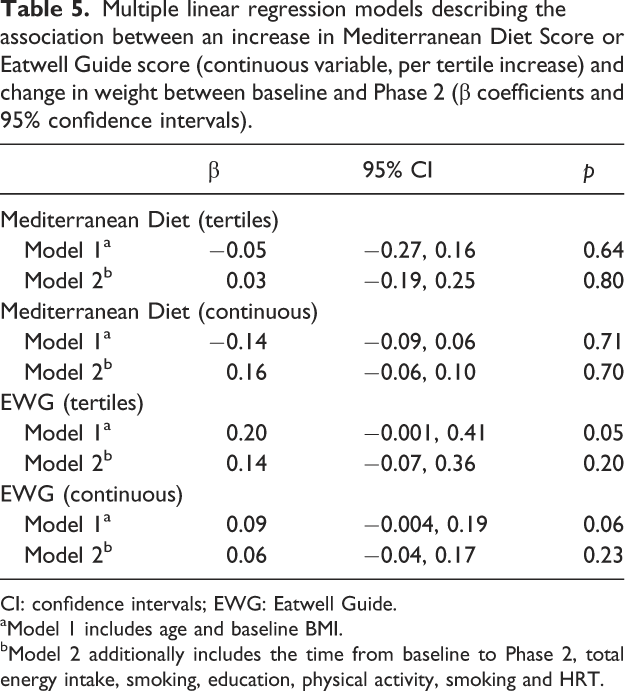
CI: confidence intervals; EWG: Eatwell Guide.
aModel 1 includes age and baseline BMI.
bModel 2 additionally includes the time from baseline to Phase 2, total energy intake, smoking, education, physical activity, smoking and HRT.
Binomial logistic regression models describing the relationship between adherence to the Mediterranean Diet and Eatwell Guide and becoming abdominally obese in participants with a waist circumference of less than 88 cm at baseline. (Odds ratio and 95% confidence intervals).
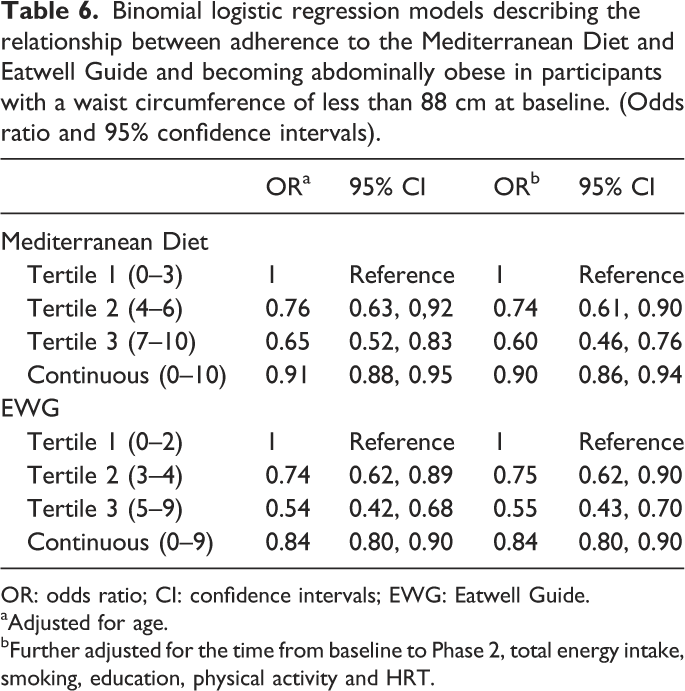
OR: odds ratio; CI: confidence intervals; EWG: Eatwell Guide.
aAdjusted for age.
bFurther adjusted for the time from baseline to Phase 2, total energy intake, smoking, education, physical activity and HRT.
Binomial logistic regression models describing the relationship between adherence to the Mediterranean Diet and Eatwell Guide and becoming overweight or obese in participants with a weight less than 25 kg/m2 at baseline. (Odds ratio and 95% confidence intervals).
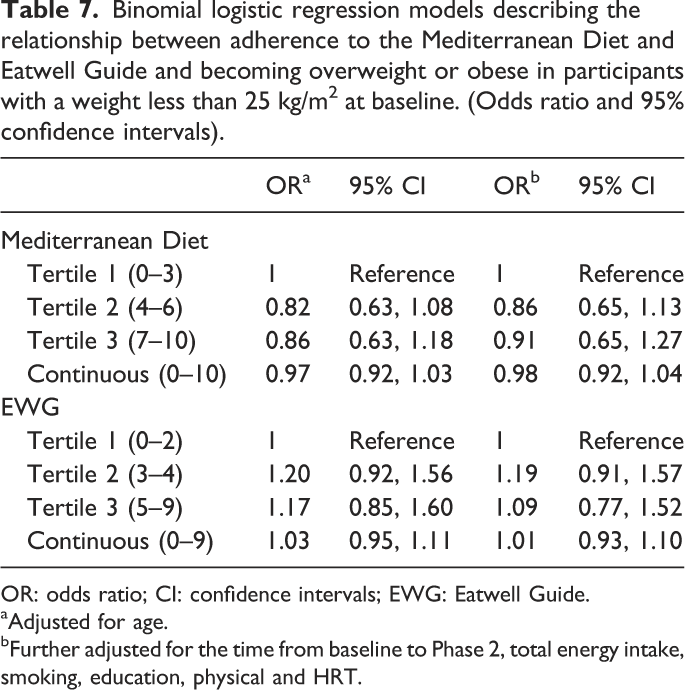
OR: odds ratio; CI: confidence intervals; EWG: Eatwell Guide.
aAdjusted for age.
bFurther adjusted for the time from baseline to Phase 2, total energy intake, smoking, education, physical and HRT.
Discussion
This study has found that higher adherence to the EWG and the Mediterranean Diet is associated with lower gains in WC and a reduced risk of abdominal obesity in post-menopausal women. Cespedes Feliciano, Tinker 7 found similar results in their prospective cohort study of post-menopausal women. They examined four different dietary indices, including those based on the American Healthy Eating Guidelines adapted to incorporate more foods predictive of preventing disease (AHEI-2010) and the Alternate Mediterranean Diet Score (AMDS). They found that each 10% increase in dietary quality score was associated with between 0.10 cm (AMDS) and 0.20 cm (AHEI-2010) smaller increases in WC. A prospective cohort study of 32,119 men and women in Italy also observed that increased adherence to the Italian Mediterranean Diet was significantly associated with negative changes in WC and a reduced risk of becoming abdominally obese. 18
Similarly, in Spain, increased adherence to the Mediterranean Diet was associated with smaller WC increases after 10 years. In addition, they also saw a decreased incidence of abdominal obesity, but this did not reach significance. 20 Cross-sectional studies have also observed an association with adherence to the Mediterranean Diet and lower WCs17,21 and a reduced risk of abdominal obesity with higher adherence to the Healthy Eating Index in America 22 ; however, in a study of Mexican Americans, the improvements in diet quality were associated with a lower risk of abdominal obesity in men but not in women. 23
No significant associations were seen between adherence to the Mediterranean Diet or the EWG and weight changes or the risk of becoming overweight or obese in those with a BMI of less than 25 kg/m2 at baseline. Similar results for weight gain have been seen previously in post-menopausal women where adherence to the Mediterranean Diet was not significantly associated with weight gain in fully adjusted models, and adherence to AHEI-2010 was associated with a higher risk of gaining weight. 8 An increase in adherence to the Mediterranean Diet was also not significantly associated with changes in weight over 5 years in an extensive study of both men and women in Italy. However, when the results were stratified by BMI, a significant weight reduction was seen in those with a BMI less than 25 kg/m2 18 . Cross-sectional studies have also not found a significant association between healthy eating patterns and BMI.17,21
In contrast to this study, some other studies have shown that adherence to the Mediterranean Diet is associated with reduced weight gain 24 and a reduced likelihood of becoming overweight or obese.18,24 However, in the multicentre, prospective study, significant heterogeneity was seen between countries, and one study in the UK saw a non-significant increase in weight gain. 24 These conflicting results are a possible indication that there may be variations in the diet in the UK compared to Mediterranean regions, and a similar lack of association between adherence to the Mediterranean Diet and weight was seen in a younger population in Sweden. 25 Differences in results with the Mediterranean Diet may also be linked to differences in the scores. This study’s score was based on median values specific to the population, so results are not directly comparable between studies. 26
The strength of this study is the availability of baseline and follow-up data from a large prospective cohort, the use of validated questionnaires for the dietary intake alongside the collection of additional data on potential confounders used in the regression models. This study, however, does have several limitations. The anthropometric measurements were self-reported, and the FFQ was administered only on a single occasion at baseline. In addition, the cohort’s population is generally healthier, 27 and the study is limited to those who returned the Phase 2 questionnaire and those who had complete and plausible data.
The results of this study add to the paucity of evidence in this area and suggest that adhering to dietary guidelines can help prevent abdominal adiposity in post-menopausal women. Adherence to guidelines in the UK is currently very low. For higher adherence, women need to consume more fibre, fruit, vegetables and oily fish and less free sugars and saturated fats. 28 Current recommendations are that public health interventions should routinely include diet and lifestyle advice alongside appropriate HRT prescribing at perimenopause. Doing this could limit the adverse health implications seen in post-menopausal women and reduce the levels of avoidable health issues in the female population.29,30
Footnotes
Acknowledgements
The authors would like to acknowledge the participants and data collection team members of the UK Women’s Cohort Study. The data for this research have been provided by the Consumer Data Research Centre, an ESRC Data Investment, under project ID CDRC LEEDS006_EXT, ES/L011840/1; ES/L011891/1.
Contributorship
NB contributed to the study conception and design, data analysis, interpretation of findings and manuscript writing. OF provided oversight and guidance at all stages of the project. All authors edited and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Manchester Metropolitan University granted ethical approval for this study. The original ethical permission for the UKWCS was granted from 174 local ethics committees, and participants consented to the use of information collected for research purposes providing confidentiality of the participants was maintained.
Guarantor
OF.